
Abstract
Objectives
To evaluate efficacy and safety of percutaneous-endovascular aneurysm repair (p-EVAR) where large-bore access puncture holes were closed with a suture mediated closure device (SMCD) in all eligible patients.
Methods
A single-center cohort of prospectively collected data in an Internal Quality Control Registry (IQCR). An “All Comers” cohort of 368 patients with 736 access groins was assessed. All abdominal aortic aneurysm (AAA) patients eligible for p-EVAR after CTA evaluation were included. Patients with stenosis and occlusions requiring vascular Interventions during EVAR were excluded. The groins were stratified into two groups: low-profile (12Fr – 16Fr) and high-profile introducers (18Fr - 20Fr). PerClose ProGlide (Abbott Cardiovascular, IL, USA) and later the newer version PerClose ProStyle (Abbott Cardiovascular, IL, USA) SMCD devices were assessed. Primary endpoints were: Primary ProGlide technical success and Primary assisted percutaneous and non-invasive technical success. Secondary cutdown was an exclusions criterion. Safety endpoints were Freedom from early peri-operative and late 30-day groin access complications requiring vascular surgical intervention.
Results
Primary technical success was achieved in 66.4 % (473/712) groins. Primary assisted percutaneous and non-invasive technical success was achieved in 32.2 % (229/712) groins. Continuous hemorrhage in 1.4 % (10/712) groins required a cutdown. 98.6 % (712/736) of the groins were successfully closed percutaneously. Median age was 76 years (IQR 71, 80). 78.8 % were male. 92 % (330/368) of the p-EVAR were elective. Median AAA diameter was 57mm (IQR 53, 63). Few groins required surgical intervention. No statically significant differences were found between the PerClose ProGlide and the ProStyle (p < .05).
Conclusions
Percutaneous closure is efficient and safe. Low-profile introducers and EVAR components (12Fr – 16Fr) had slightly better primary technical and assisted technical success. 83.5 % of the patient groins were treated with low-profile introducers reflecting the drive in the vascular field toward lower-profile devices. No statistical difference between groups was observed for primary technical success and complication rate.
Introduction
The closure of large-bore puncture holes in the common femoral artery (CFA) using (12Fr − 20Fr) introducers during Endovascular Aneurysm Repair (EVAR) was first facilitated by open surgical access. A cutdown gave visual view of the CFA allowing for correction of vessel wall pathologies such as atherosclerotic stenosis, occlusion, or aneurysmatic dilation prior to access. 1 Scar tissue from prior groin procedures or radiation treatment could also be addressed, and a visually guided suture of the puncture hole gave hemostasis after completion of the EVAR. The downside of open surgical access was complications as postoperative pain, seromas, postoperative wound infections, scar tissue formation, and prolonged hospitalization with higher cost.2,3
Percutaneous-endovascular aneurysm repair (p-EVAR) with a suture mediated closure device (SMCD) was introduced as a minimally invasive alternative to closure of arteriotomies, with a reduction of the complications associated with open surgical access, and subsequent reduced costs.3–6
Lønn et al. suggested that a percutaneous femoral approach should initially be considered for all endovascular aortic procedures, but with a low threshold to convert to traditional cutdown technique when complications arise such as bleeding, stenosis, ischemia or femoral artery injury. The patient’s unique anatomy dictates the optimal choice of procedure. 1
The aim of this study is to evaluate the evolution of this technique, including the introduction of the PerClose ProStyle SMCD (Abbott Cardiovascular, IL, USA).
Methods
This is a single-center cohort of prospectively collected data in our Internal Quality Control Registry (IQCR). An “All Comers” cohort of 368 patients (736 groins) were recruited with abdominal aortic aneurysms (AAA) eligible for treatment with p-EVAR. A computer tomography angiography (CT-A) with focus on calcification and degree of stenosis of the CFA and Iliac arteries was performed prior to endovascular treatment in all patients. Two groups were analyzed: stratification group 1 (12Fr – 16Fr) and stratification group 2 (18Fr – 20Fr). 74 % (527/712) of the groins were closed with PerClose ProGlide (Abbott Cardiovascular, IL, USA) and in April 2022 the remaining 26 % (185/712) groins were closed with PerClose ProStyle (Abbott Cardiovascular, IL, USA).
Exclusions
Groins with introducers smaller than 12Fr were excluded. Additionally, access sites with occluded Iliac arteries, groins requiring primary cutdown due to excessive atherosclerotic disease necessitating open surgical revascularization (bypass or thrombendarterectomy), and patient death before completion of EVAR (in case of ruptured AAA) were excluded.
Additional techniques
Percutaneous
All SMCD were placed with Ultrasound guidance using Seldinger technique, in accordance with the ESVS guidelines.7,8 One SMCD PerClose ProGlide 6F was placed medially and one laterally in the percutaneous puncture hole according to the manufacturer’s Instructions for Use (IFU).
In groins without adequate hemostasis and pulsatile or continuous bleeding despite the SMDC, a 6Fr or 8Fr Angio-Seal (Terumo International Systems, Tokyo, Japan) was used to seal the puncture hole. The Angio-Seal system contains an anchor deployed on the luminal side of the vessel wall, a collagen plug designed to conform to the arteriotomy and a suture, all components are bioabsorbable within 60-90 days. 9 The Angio-Seal is placed over a guidewire and so is only an alternative if the guidewire is still in place after knotting the SMDC.
Non-invasive
A HemCon® Patch (Pro-tricol Biomedicals, OR, USA) is an alternative for smaller bleedings, after removal of the guidewire. It is placed extra-corporal, over the puncture hole and is made of collagen. If the ProGlide suture failed to achieve hemostasis the suture ends are retained, and a slit is made in the patch, and a vascular clamp is tightened on the suture ends. 60-120 minutes later the clamp is released, and the suture ends cut.
Manual compression: In case of inadequate hemostasis with the prior alternatives, or a small bleed, manual compression is an option and attempted with external compression for 15 minutes.
As an alternative to manual compression, a FemoStop ™ II Plus (St Jude Medicals, Mn, USA) band could be placed around the patient’s waist and with an inflatable transparent dome mounted on a ridge platform. A manometer is then used to control the pressure which is successively reduced over 30 minutes.
Surgical cutdown
Surgical Cutdown is a standard open surgical procedure with exposure of the CFA.
In patients with massive bleeding, proximal control over the inguinal ligament with a retroperitoneal approach is preferred. After access to the CFA sutures the puncture hole are sutured. The Fascia Suture Technique (FST) was omitted in this study due to higher incidence of reoperations. The FST could also be used as a “Bailout” procedure if percutaneous technique failed, with fewer access wound complications as compared to open access to the CFA. 10
Endpoints
Primary ProGlide technical success was defined as hemostasis without any additional percutaneous and/or non-invasive technical assistance or assisted open surgical cutdown. Primary assisted percutaneous and non-invasive technical success was implemented if Primary Technical Success was not attained. Secondary surgical cutdown was an exclusion criterion.
Safety endpoints were defined as Freedom from early peri-operative and late 30-day groin access complications requiring surgical treatment.
30-day and 1 year mortality were recorded. All EVAR patients were controlled with a CT-A at 1 month, 6 months and annually. Late complications were obtained from both the CT-A and clinical follow up appointments in the out-patient clinic at 30-days.
Ethics
Regional Ethics Committees (REC) University Hospital Oslo has approved our internal Quality Control Registry (IQCR) (Ref. nr.13410/2015) and our Hospital Ethics Committee has also approved our IQCR (PVO nr. 35158/2018). Furthermore the Regional Ethics Committees (REC) University Hospital Oslo evaluated this project where only de-identified data was to be used and did not require patient consent and delegated the approval to our Local Hospital REC. (Ref. nr. 151845/2020). The Local Hospital REC known as the Data Protection Officer (DPO) at our hospital has approved this study (Ref. nr. 132655/2021) and was amended (Ref. nr. 30460563/2024). Patient consent was not required on the de-identified data.
Statistics
Continuous variables were expressed as means ± SD when symmetric distribution or median and Inter Quartile Range (IQR) if skewed/asymmetric. Categorical variables were expressed as numbers and percentages. Comparison between two groups was calculated using Chi-square test for categorical outcomes or Student t-test/Mann-Whitney U for continuous variables. SPSS software (version 29.0) was used for statistical analysis. Statistical significance was set to p < .05.
Data
The study database is in the hospital server with patient sensitive information and therefore not accessible.
Results
Patient demography.
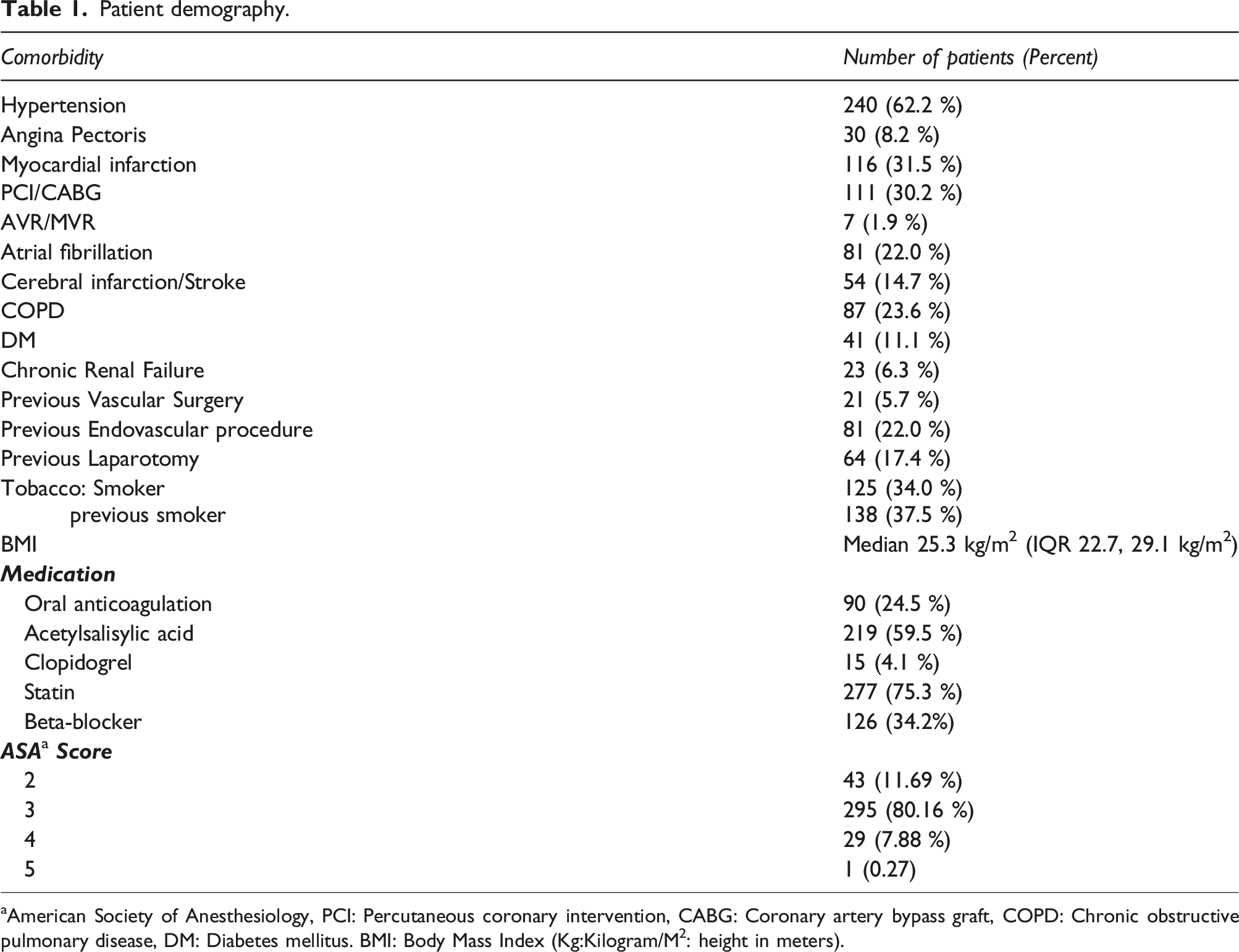
aAmerican Society of Anesthesiology, PCI: Percutaneous coronary intervention, CABG: Coronary artery bypass graft, COPD: Chronic obstructive pulmonary disease, DM: Diabetes mellitus. BMI: Body Mass Index (Kg:Kilogram/M2: height in meters).
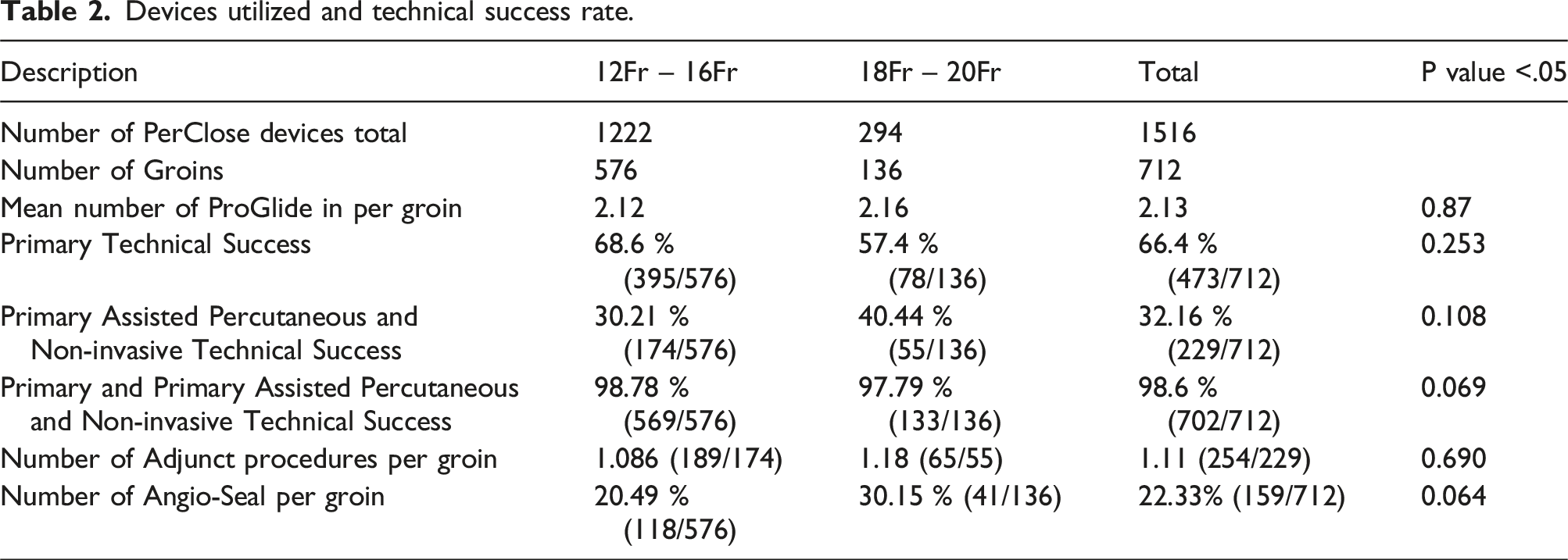
Primary technical success with SMCD was achieved in 66.4 % (473/712) of the groins. Primary assisted percutaneous and non-invasive technical success was achieved in an additional 32.2 % (229/712) of the groins. Due to continual hemorrhage 1.4 % (10/712) groins required a secondary surgical cutdown (Figure 1). 98.6 % (712/736) of the groins were successfully closed with ProGlide in combination with percutaneous devices 64.4 % (159/229) or other non-invasive technique 44.1 % (101/229). (Table 2). Patient Flowchart showing flow through the access closure procedure. Devices utilized and technical success rate.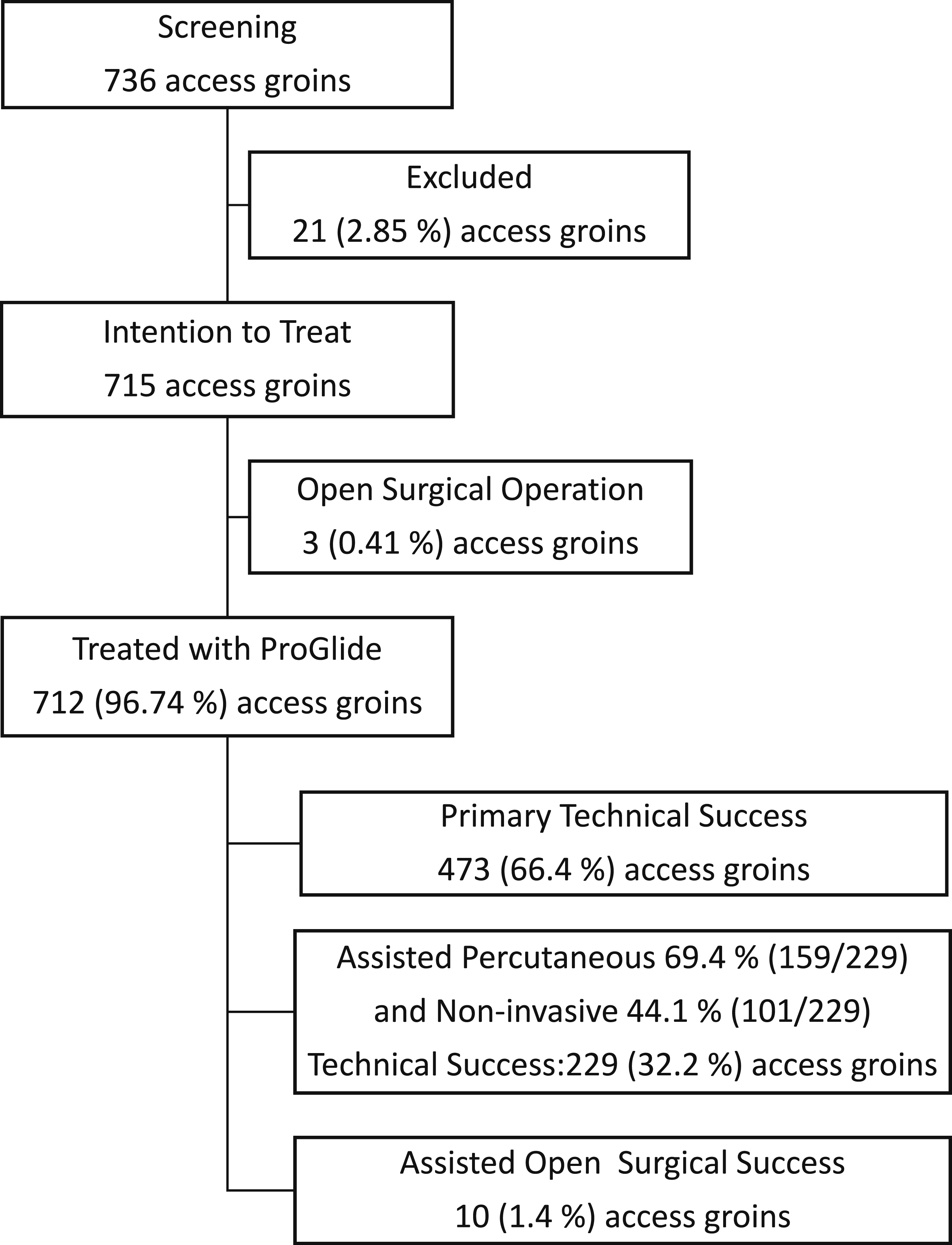
Patient recruitment/selection resulted in 21 exclusions: 4 > 12Fr, 5 occlusions, 9 primary cutdowns, 2 groins rAAA death on table, and one aorto-unifemoral stent graft requiring Fem-Fem crossover bypass due to contra-lateral ischemia and three open surgical conversions to cutdown were also excluded during the procedure at the operators discretion, due to acute ischemia: two with contra-lateral common iliac artery (CIA) occlusion that required a Femoral-Femoral Crossover Bypass and one due to thromboembolic complications in a patient with rAAA that was treated with an EVAR that kept on hemorrhaging due to a high volume endoleak II (EL II) that required an open surgical conversion. These exclusions were not ProGlide device related.
During closure of the access groins nine groins had hemorrhaging requiring a cutdown, one groin was treated with a thrombendarterectomy due to a dissection with stenosis and bleeding.
Of the 712 groins (98.6%) with a primary, or primary assisted technical success a mean of 2.1 (1516/712) ProGlide devices were deployed per groin. In the low-profile stratification group (12Fr – 16Fr), a mean of 2.1 (1222/576) devices where deployed, and in the high-profile stratification group 2.2 (294/136) devices where deployed (p = .87) (Table 2).
ProGlide failure occurred in three groins during p-EVAR and required an open surgical procedure. 32.2 % (229/712) groins required an assisted percutaneous or non-invasive adjuvant procedure. 1.4 % (10/712) required an open surgical cutdown.
Of the 239 groins without primary technical success, 10 groins needed open surgical cutdown due to hemorrhage. In 217 groins one adjunct device was placed, two devices were placed in 8 groins and in 4 groins 3 devices were placed.
The mean number of adjunctive devices deployed per groin was 1.1 (189/174) in group 1(12 Fr – 16Fr), 1.2 (65/55) in group 2 (18Fr – 20Fr) and in the entire cohort 1.1 (254/229). In 22.3 % (159/712) of the groins an additional percutaneous Angio-Seal was deployed. Angio-Seal 6Fr was deployed in 88.7 % (141/159) and Angio-Seal 8Fr in 11.3 % (18/159) (Table 2).
There was no statistically significant difference in Primary technical success between the two stratification groups (p = .25) and the same was found for Primary assisted percutaneous and non-invasive technical success (p = .069). Neither did statistical analysis of the two stratification groups yield significance for Primary and Primary assisted percutaneous and non-invasive technical success (p = .069). (Table 2).
Length of stay on the intensive care unit was median 0 days (IQR 0, 0) and in hospital stay was median 3 days (IQR 2, 4). The 10 patients that required an open cutdown had a median time on the intensive care unit of 0 days (IQR 0, 1 days) and length of stay of a median of 4 days (IQR 3, 5 days).
Endoprosthesis
Two different EVAR stent grafts were used in the study: 62 % (228/368) Medtronic Endurant II (Medtronic, Minneapolis, MN, USA, and 38 % (140/368) Gore Excluder (W.L. Gore & Associates, Flagstaff, AZ, USA) with access bore-hole size 12Fr – 20Fr.
Complications occurred in 69 groins in 61 patients. Early (peri-operative) complications occurred in 46 groins and late (30-day) complications were found in 23 groins. Eight patients had two complications where six of these patients had a postoperative hematoma following by a 30-day CT-A verified pseudoaneurysm. Two patients had bilateral groin hematomas postoperatively. Most of the complications were minor hematomas and small pseudoaneurysms that did not require additional treatment. However, 1.83 % (13/712) of groins peri-operatively and 0.14 % (1/712) groins at 30-days required treatment (Table 3).
Access site complications.
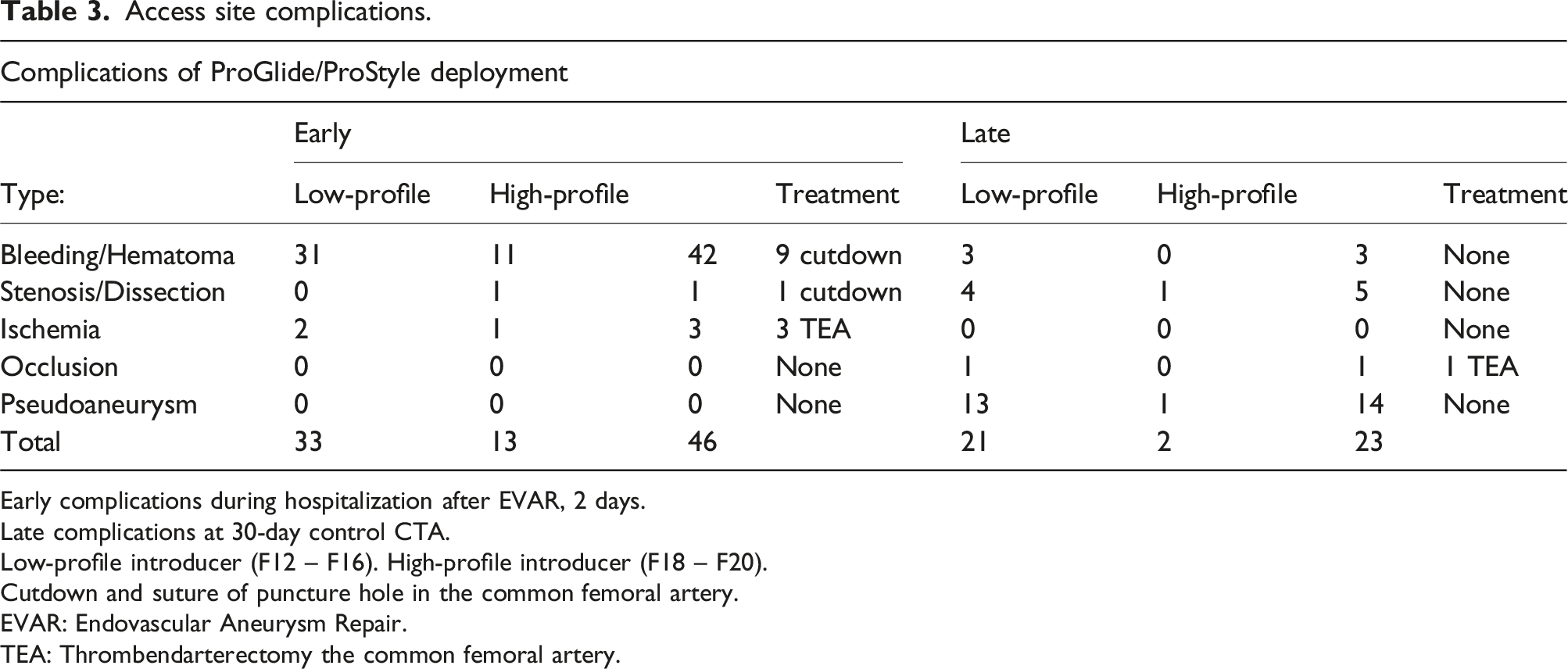
Early complications during hospitalization after EVAR, 2 days.
Late complications at 30-day control CTA.
Low-profile introducer (F12 – F16). High-profile introducer (F18 – F20).
Cutdown and suture of puncture hole in the common femoral artery.
EVAR: Endovascular Aneurysm Repair.
TEA: Thrombendarterectomy the common femoral artery.
ProGlide vs. ProStyle
Comparison of two different Suture Mediated Closure Devices: PerClose ProGlide Device vs. PerClose ProStyle Device.
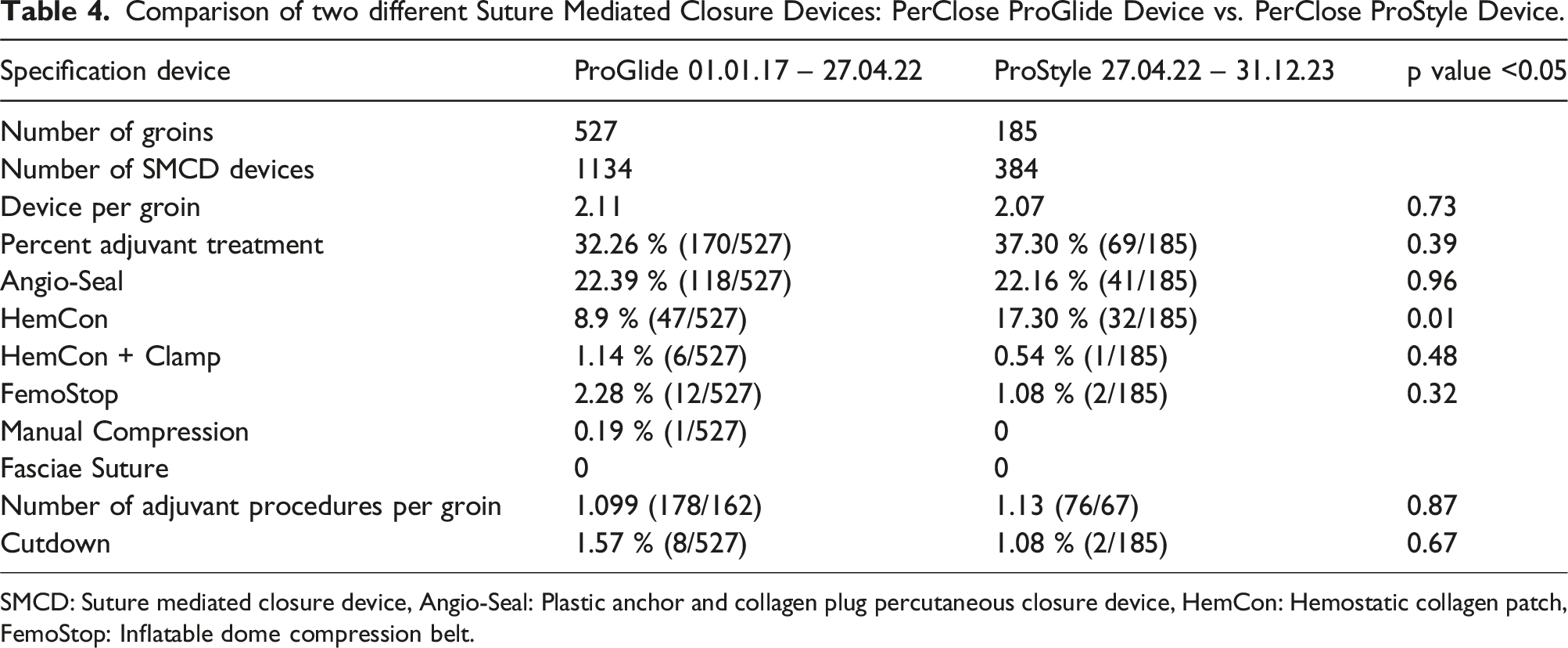
SMCD: Suture mediated closure device, Angio-Seal: Plastic anchor and collagen plug percutaneous closure device, HemCon: Hemostatic collagen patch, FemoStop: Inflatable dome compression belt.
Discussion
This study demonstrates that hemostasis was safely and effectively achieved in 98.6 % of the p-EVAR procedures with the combination of primary and primary assisted technical success. Success rates of more than 95 % have been described earlier in selected studies. 11
In this study, 56% (396/712) of the groins were accessed with (12Fr-16Fr) (low-profile introducer), The primary technical success combined with primary assisted technical success was 98.6 % in this study. The trend toward increased use of low-profile devices is evident and is reflected in the Endovascular device Industries push toward lower-profile devices.
ProGlide failure
Earlier ProGlide studies have described various factors associated with SMCD failure. Chen et al. Investigated 602 access sites in 458 patients treated endovascularly for AAA, thoracoabdominal aortic aneurysms or B dissection and found failure to achieves hemostasis in 7.3 % (44/602) of the access sites leading to a cutdown. Factors that predisposed for ProGlide failure were a sheath size >19 Fr in addition to a history of PAD, presence of calcified arteries, depth of skin puncture ≥33 mm and BMI ≥28.7 kg/m2. 12 In our study we compared the median BMI of the whole cohort which was 25.3 kg/m2 (IQR 22.7, 29.1) and those patients that had a high-profile introducer with a median of 26.3 kg/m2 (IQR 23.1, 29.0). 62.5 % (227/363) patients had low-profile introducers in both groins. 28.7 % (104/363) had a high-profile introducer in the right groin and a low-profile introducer in the left groin, 8.5 % (31/363) had the opposite and only one patient had a high-profile introducer in both groins. Consequently, comparing these two stratification groups is difficult.
Malkawi et al. found in a meta-analysis of 22 publications with p-EVAR where PerClose ProStar and ProGlide (Abbott Cardiovascular, Il, USA) was used that 92 % (95% CI 90.1 – 93.9%) were successfully closed. However, seven of the studies excluded calcification, five scar tissue in the groin and three for common femoral artery aneurysms. 11 This contrasts with this study where we accepted “All Comer s” prior to exclusion.
Manunga et al. found that calcification of over 50 % of the anterior CFA predicted failure regardless of sheath size (12Fr – 24Fr) or patient BMI. 13 Whereas Smith et al. compared open surgical cutdown to Percutaneous ProGlide Closure with automated 3-D CT reconstructions of before and after CT imaging. They demonstrated that patients with obesity or severely calcified femoral arteries could be safely treated with p-EVAR with less complications then open surgical cutdown. 14
Mousa et al. reported that the learning curve and operator experience was a good predictor of percutaneous access failure. They also found that calcification in addition to age and female sex also were detrimental to success. Vessel diameter and device profile did not show any significant difference in outcome. 15
Ultrasound guided puncture
Ultrasound guided vessel puncture to avoid calcification in the anterior vessel wall is now standard procedure at our institution. Oikonomou et al. stated that ultrasound guided puncture as well as intraoperative and postoperative monitoring of the access sites to minimize the complication rate and to allow immediate revision of complications is mandatory, which is also corroborated by Bensley et al.16,17 The ESVS guidelines also recommend the use of ultrasound guided puncture. 8
Learning curve/predictors of success
Gao et al. showed that 36 – 40 deployments of ProGlide were necessary to achieve a target failure rate of 5 %. 18 Mousa et al. found that predictors of ProGlide success were learning curve and operator experience. 15 Others are more optimistic and set proficiency levels after 30 ProGlide deployments. 3 Our center has performed over 960 EVAR for AAA and the procedures are performed by five vascular surgeons and four interventional radiologists. All procedures done by the junior staff are accompanied by experienced mentors.
Efficacy and safety
In this study, by combining both primary technical success and primary assisted percutaneous and non-invasive technical success, 98.6 % of the groins were successfully closed with ProGlide. Despite our more liberal use of ProGlide, the number of serious adverse events was small. Complications requiring treatment was less than 1.97 % (14/712) in this study. Our primary technical success of 67 % is lower than others have reported where success rates have varied from 63 to 100 %. 19 Patel had a primary patency of 75.4 % with 20.5 % adjunct Angio-Seal giving an overall success of 95.1 %. 20 Whereas Lee et al. reported 94.4 % primary patency. 21
Previous investigators have obtained up to 100 % primary technical success, we have reached 68.2 %. Different definitions of technical success in previous publications and the fact that we have included and treated “ALL COMER” patients with factors associated with failure may explain our poorer results.
If two ProGlides were not sufficient, we had additional adjunct non-invasive procedures. HemCon, HemCon with clamp in 60 – 120 minutes, FemoStop with pressure successively released over 30 – 60 minutes or manual compression for 15 minutes. This resulted in an additional hemostasis in the current study with a Primary and primary assisted technical success of 98.6 % (n = 702). Georgiadis et al. found better results with p-EVAR access site closure with ProGlide SMCD with introduces sheath size ≤18 F. 22
In this study 83.5 % (395/473) of the low-profile (12Fr – 16Fr) access introducers resulted in a Primary technical success rate of 68.6 % as opposed to the high-profile introducers where 16.5 % (78/473) (18Fr – 20Fr) resulted in a Primary technical success rate of 57.4 %. This discrepancy is most likely attributed to the smaller diameter introducers used in low-profile stent grafts. Several groups have documented that the ProGlide SMCD attained better patency with introducers ≤18Fr.20,22–24 Though not statistically significant, there was a 10 % absolute reduction in the low-profile primary assisted technical success and a 10 % absolute increase in the Angio-Seal deployment in the high-profile group. Considering the uneven distribution of patients between the low- and high-profile groups (83.5 % vs 16.5 %) this may have introduced some quantitative skewed bias towards the low-profile group.
Adjunct procedures
Other studies have also used adjunct devices in addition to the ProGlide device. Cakal et al. reported adjunct Angio-Seal was feasible and safe in 25 % (46/185) of 185 of their procedures as a Bailout when hemostasis was not attained with ProGlide alone in mostly introducers Fr > 18. 24 Patel et al. looked at 122 p-EVAR with CFA access with a median introducer size of 18F and one Angio-Seal was necessary in 20.5 %. 20 Szpotan et al. reported a series of 384 large-bore access sites having introducers with diameter (12Fr – 22Fr) where 10 % required one additional ProGlide. 25 Lin et al. reported 87.6 % primary technical success with two ProGlide devices. 11.5 % required an additional ProGlide giving a secondary technical success rate of 99 %. 26 In our current study we deployed an extra adjunct Angio-Seal in 22.3 % 159/712 of our access puncture sites to obtain hemostasis. It is apparent that not all large-bore puncture holes can be sealed with only two ProGlide devices. In most studies reported there seems be around 20 % that require an additional Angio-Seal to obtain hemostasis.
FST - Fascia Suture Technique
Larzon et al. reported that the Fascia Suture Technique is feasible for closure of CFA puncture holes after p-EVAR in both elective and acute procedures. Failure can be managed easily with a cutdown. 10 Complication rates after p-EVAR are also rare. 27
ProGlide can be used in a ruptured AAA setting if the patient is hemodynamically stable, but in an emergency setting with a hemodynamically unstable patient it is often not practical or ethical to take time to place two ProGlide percutaneous sutures in each groin before and an emergency EVAR for a ruptured AAA. Then a cutdown or a quick Fascia Suture can be advantages.
Cost effective
Several studies have shown that a percutaneous closure is more cost effective than an open cutdown due to shorter length of stay and reduced risk of postoperative groin infections.3–5 Procedure time is also reduced compared to an open cutdown. Uhlmann et al. showed in a prospective randomized trial that successful percutaneous access for endovascular aneurysm repair was significantly cheaper than femoral Cutdown. 28
In our hands closure of CFA puncture holes after EVAR with ProGlide and if necessary assisted secondary percutaneous and non-invasive technique is efficient and safe. Over 95 % hemostatic percutaneous with non-invasive adjunct procedures is a very acceptable result. Especially with so few complications and the reduced number of access groins that have required a surgical procedure to obtain hemostasis.
Limitations
Anatomical measures of the Common Femoral Artery and degree of calcification has not been registered in this study. Patients with obvious significant stenosis on preoperative CT-A imaging were treated with open surgical technique with thrombendarterectomy prior to EVAR. Cost–benefit of ProGlide, Angio-Seal and Non-invasive devices has not been registered nor calculated. We have calculated the BMI (kg/m2) but have not measured depth/length of the puncture from skin to vessel wall in this study. Uneven distribution of study groins in the low- and high-profile groups (83.5 % vs 16.5 %) may have introduced a quantitative skewed bias toward the low-profile group.
Conclusions
Percutaneous closure is efficient and safe. Low-profile introducers and EVAR components (12Fr-16Fr) had slightly better primary technical and assisted technical success. 83.5 % of the patient groins were closed with low-profile introducers reflecting the drive in the vascular field toward lower-profile devices. No statistical difference between groups was observed for primary technical success and complication rate.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.