
Abstract
Background:
Value of information analysis has been proposed as an alternative to the standard hypothesis testing approach, which is based on type I and type II errors, in determining sample sizes for randomized clinical trials. However, in addition to sample size calculation, value of information analysis can optimize other aspects of research design such as possible comparator arms and alternative follow-up times, by considering trial designs that maximize the expected net benefit of research, which is the difference between the expected cost of the trial and the expected value of additional information.
Purpose:
To apply value of information methods to the results of a pilot study on catheter securement devices to determine the optimal design of a future larger clinical trial.
Methods:
An economic evaluation was performed using data from a multi-arm randomized controlled pilot study comparing the efficacy of four types of catheter securement devices: standard polyurethane, tissue adhesive, bordered polyurethane and sutureless securement device. Probabilistic Monte Carlo simulation was used to characterize uncertainty surrounding the study results and to calculate the expected value of additional information. To guide the optimal future trial design, the expected costs and benefits of the alternative trial designs were estimated and compared.
Results:
Analysis of the value of further information indicated that a randomized controlled trial on catheter securement devices is potentially worthwhile. Among the possible designs for the future trial, a four-arm study with 220 patients/arm would provide the highest expected net benefit corresponding to 130% return-on-investment. The initially considered design of 388 patients/arm, based on hypothesis testing calculations, would provide lower net benefit with return-on-investment of 79%.
Limitations:
Cost-effectiveness and value of information analyses were based on the data from a single pilot trial which might affect the accuracy of our uncertainty estimation. Another limitation was that different follow-up durations for the larger trial were not evaluated.
Conclusion:
The value of information approach allows efficient trial design by maximizing the expected net benefit of additional research. This approach should be considered early in the design of randomized clinical trials.
Introduction
Peripheral venous and arterial catheters are widely used around the world. Up to 70% of patients in acute care hospitals need a peripheral catheter; about 330 million are sold each year in the United States alone. 1 Effective securement of peripheral catheters to the skin is necessary to ensure that the device does not dislodge and move out of its place. 2 Additionally, adequate catheter securement minimizes the chance for common catheter-related complications such as catheter site irritation, catheter occlusion and catheter-related bloodstream infections.2,3 Despite the use of dressings to secure catheters, up to 92% of catheters still fail.2,4 Catheter failure requires removal and reinsertion of a new device, which consumes health-care resources in terms of equipment and staff time, and causes discomfort to patients. Because most failures are likely to be preventable with effective catheter securement, there is a need to improve current catheter securement techniques. Unfortunately, this topic has received little research attention, and there is a paucity of evidence to support practice improvement.2,5 A pilot study was conducted to assess the feasibility of a clinical trial to compare the efficacy of different devices in securing peripheral arterial catheters in the operating theater and the intensive care unit (ICU). Typically, and based on the results of a pilot study, a larger clinical trial will be designed to more definitively answer the research question.
Sample sizes of clinical trials are usually calculated based on type I and type II errors and the minimum clinically important difference. The smallest sample size to identify the minimum clinically important difference is usually most efficient due to the costs of running large clinical trials. However, an alternative to calculating sample size based on hypothesis testing is the value of information (VOI) approach. This is based on the notion that errors are costly and information is valuable since it reduces the risk of making wrong judgments. VOI analysis quantifies the uncertainty surrounding trial results, estimates the expected benefits (i.e. value) of reducing this uncertainty with additional research, and subsequently informs optimal future trial design.6–8 Based on this approach, if the expected benefit of an intended clinical trial outweighs its expected cost, then the study is potentially worthwhile. Beyond sample size determination, VOI analysis can optimize additional aspects of research design such as possible comparator arms and alternative follow-up periods, by considering trial designs that optimize the expected benefits of research.6,9 In recent years, the application of the VOI analytic framework in health-care interventions has grown. However, a limited number of applied papers have reported the use of this approach in informing optimal trial design.10–12 Most applications have been restricted to the estimation of optimal sample size, and the majority were in two-arm, randomized trials.13–15
The aim of this article is to apply VOI analysis to the results of a pilot study in order to determine the optimal trial design of a larger clinical trial on arterial catheter securement devices from the perspective of the State Health Department, Queensland Health, Australia.
Material and methods
The general approach to achieve the aim of this article was to conduct an economic evaluation to compare different types of arterial catheter securement devices, using the results from the pilot study. After that, probabilistic Monte Carlo simulation was performed to characterize uncertainty surrounding the analysis results and to calculate relevant VOI measures. To guide the optimal trial design, expected costs and benefits of the alternative trial designs were estimated and compared.
The pilot study
A single-center, four-arm randomized controlled, non-blinded pilot study was conducted from November 2012 to February 2013, in Queensland, Australia. The included subjects were adult surgical patients admitted post-operatively to the ICU who had a peripheral arterial catheter inserted. The study was approved by the health authority and the University Human Research Ethics Committees (Trial ID: ACTRN12611000769987). A centralized web-based randomization service allocated patients in a 1:1:1:1 ratio to the control product of standard polyurethane dressing, or to the experimental arms of tissue adhesive, bordered polyurethane dressing, or a sutureless securement device. The primary endpoint was catheter failure defined as any early removal of the catheter due to dislodgement, occlusion, phlebitis, local infection or catheter-related bloodstream infection. Additionally, health-care resource utilization data were collected alongside the clinical trial. Resources captured included the equipment and staff time required for insertion and removal of arterial catheters and both initial and any replacement dressings required while in the ICU. Data were analyzed by intention-to-treat analysis. A total of 123 participants were randomized, and all received the allocated intervention. There were no differences in demographic or clinical risk factors between groups at enrolment. Catheter failure was lowest in the tissue adhesive group (2/32, 6.3%) and highest in standard polyurethane (6/30, 20%), with sutureless securement device (5/31, 16.1%) and bordered polyurethane (4/30, 13.3%) in the mid-range, but these differences were not statistically significant (p = 0.43). Based on a significance level of 0.05, 95% power and at least 10% absolute reduction in catheter failure from the control value, the projected sample size for a larger, four-arm, clinical trial was estimated at 388 patients in each arm.
Economic evaluation
A decision tree was used to describe the research question (Figure 1). Clinical outcomes and cost data collected from the pilot study were used to populate the decision tree. Because the primary outcome of the trial was catheter failure probability, which is an adverse event, the effect outcome chosen for this cost-effectiveness analysis was the probability of catheter success (i.e. 1 − failure probability). Resources collected alongside the clinical trial were valued from the perspective of the State Health Department, Queensland Health, Australia, at 2012 prices and wages. Due to the acute nature of the evaluated interventions, it was difficult to measure the effect of each dressing on the quality of life of the hospitalized patients and conduct a cost utility analysis. The net monetary benefit approach was used for the cost-effectiveness analysis; the net benefit is the difference between the clinical effect valued at a given willingness-to-pay threshold and cost: net benefit = willingness-to-pay × effect − cost. 16 The willingness-to-pay threshold was set at AUD100/catheter success. The net benefit was estimated for the four catheter securing devices, the preferred option being the one with the maximum average net benefit. 16 To characterize the uncertainty in the cost-effectiveness analysis, cost and effect parameters were characterized by probability distributions (Table 1). For this analysis, the probability of a catheter being successful was assigned a beta distribution. Thus, Success ∼ Beta (a0,b0), where a0 is the number of successful catheters and b0 is the number of failed catheters in the initial clinical trial of sample size n0 for each intervention. Conditional on the outcome being 1 or 0 (i.e. successful or failed catheter), cost of success (CostS) and cost of failure (CostF) were assigned lognormal distributions; thus, the natural log of the cost is approximately normally distributed


where VS and VF are the respective mean log costs for success and failure, and τS(n0) and τF(n0) are the respective standard deviations of the log costs of success and failure in the initial trial. The mean intervention cost is a weighted average of the means of the lognormal distributions of success and failure costs 17

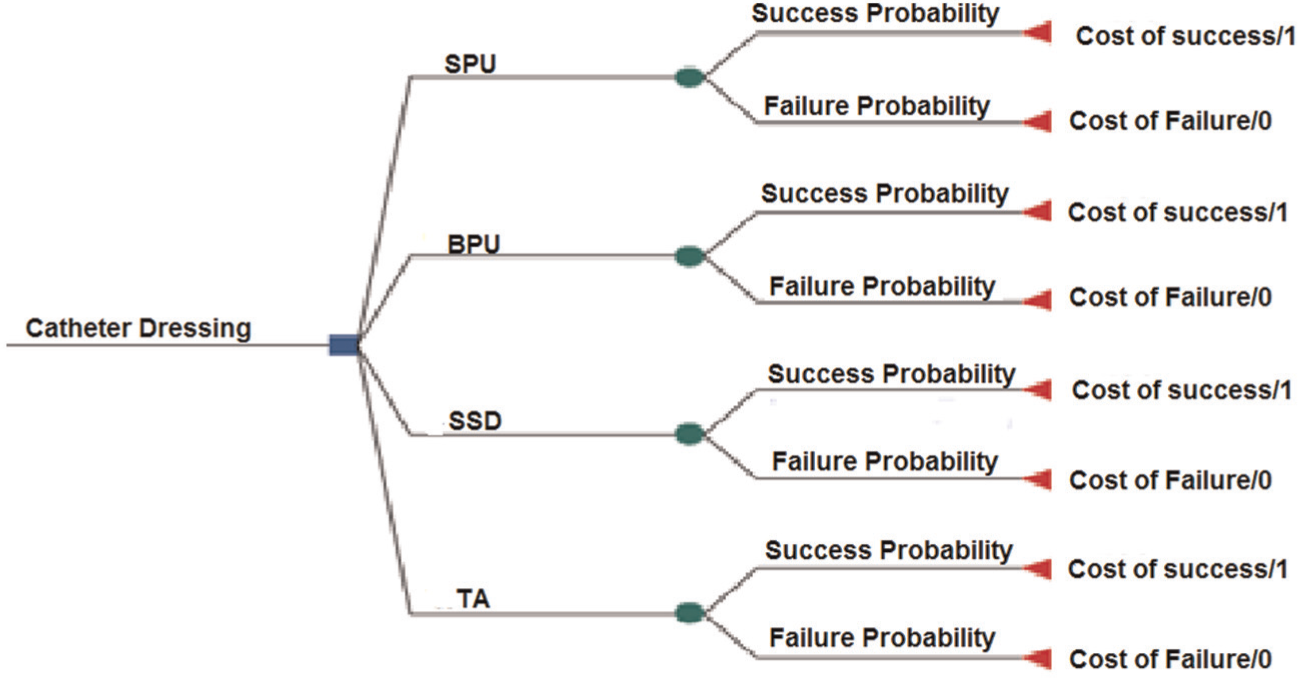
A decision tree based on the clinical trial.
Parameters used in the value of information analysis.
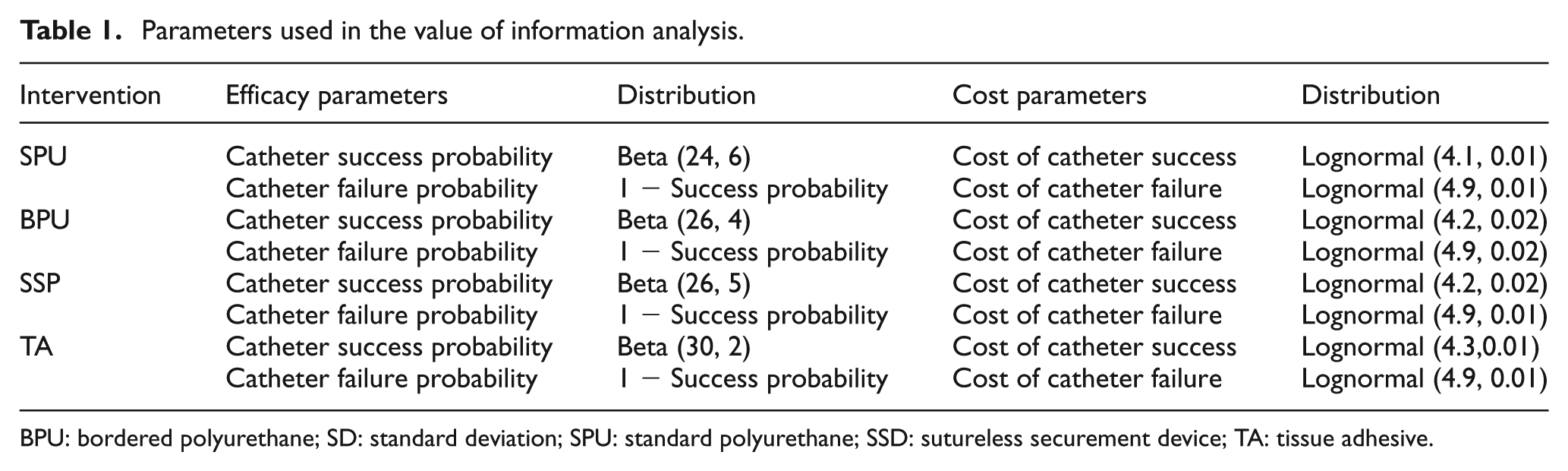
BPU: bordered polyurethane; SD: standard deviation; SPU: standard polyurethane; SSD: sutureless securement device; TA: tissue adhesive.
VOI analysis
Three measures of VOI were calculated: (1) the expected value of perfect information, (2) the expected value of sample information, and (3) the expected net benefit of sampling.
The first step in the VOI analysis was to calculate the expected value of perfect information. This measure represents the value of the total uncertainty surrounding a research result. 18 In other words, the expected value of perfect information is the maximum value expected to be gained from resolving uncertainty by conducting additional research, hypothetically with infinite sample size. 8 This is the first hurdle before deciding whether additional research to resolve uncertainty is worthwhile. If the expected value of perfect information is small, then there would be very little decision uncertainty and consequently low value for additional research. Conversely, if the expected value of perfect information is high, then the next step is to calculate the expected value of sample information to determine the VOI from additional trial with a specific design (e.g. sample size). 8 Finally, the expected net benefit of sampling is the difference between the expected value of sample information and the total cost of the intended trial for that sample size. The total cost of a future trial should include fixed costs (e.g. salaries), variable costs (i.e. per patient recruited), and opportunity costs (i.e. benefits forgone) incurred by patients who receive the inferior intervention while the trial is performed.6,19 The total cost for a future study was estimated to be AUD120,000 of fixed costs and AUD150/patient in variable cost. To decide on the optimal future trial design in terms of the number of arms and optimal sample size, the expected value of sample information and the expected net benefit of sampling were calculated for the alternative possible designs (i.e. two-arm, three-arm, four-arm) across distinct sample sizes. The optimal trial design is the design with the maximum expected net benefit of sampling. Designs of priority are those that provide the maximum return-on-investment (i.e. maximum expected net benefit of sampling per additional dollar spent on research).7,8
Methods to calculate these VOI measures are described in detail elsewhere.19–22 In general, our VOI analysis was a continuation of the above probabilistic sensitivity analysis and included the steps below:19,20
Sampling repeatedly (100,000 iterations) random values from the effect and cost parametric distributions;
Calculating the overall average net benefit for each intervention to determine the intervention with the highest net benefit (i.e. the preferred intervention);
Calculating the net benefit for each intervention at each simulation (i.e. iteration) to identify the intervention with the maximum net benefit at that iteration;
Averaging the maximum net benefits from all iterations (Step 3) and subtracting from this the net benefit of the preferred intervention (Step 2) to give the per-patient expected value of perfect information.
The expected value of sample information for a future study of n patients/arm was calculated using the following algorithm assuming the net benefit is linear on effect and cost parameters: 19
1. Sampling effect and cost parameter values from their prior probability distributions.



2. Sampling from the predictive distribution of the sufficient statistics arising from the new study size n, given the sampled values in Step 1.



3. Combining prior and predicted data to estimate the posterior expectations for the cost and effect parameters for each intervention. 19



The posterior expected cost of the intervention (Costposterior) as a function of the posterior expectations for the cost and effect parameters can be expressed as

4. Calculating the posterior net benefit for each intervention, using the posterior expectations above.
5. Identifying the intervention that has the expected maximum posterior net benefit.
6. Repeating Steps 1–5 (100,000 times) and averaging the posterior net benefits from Step 5.
7. The per-patient expected value of sample information for a new study with n patients/arm is the difference between the average net benefit in Step 6 and the net benefit of the preferred intervention calculated in Step 2 of the expected value of perfect information algorithm.
The VOI measures estimated from these simulations are for the individual patient. However, to calculate VOI at the population level, the per-individual measures were multiplied by the number of patients expected to benefit from the evaluated devices over a given time period. The expected population for the State of Queensland was estimated at 125,000 ICU patients over the coming 5 years.
Results
Cost-effectiveness
Clinical outcomes and costs for the four catheter securement devices are summarized in Table 2. At a willingness-to-pay threshold of AUD100/catheter success, the average net benefit was the highest for tissue adhesive (AUD14.1), indicating that tissue adhesive was the preferred intervention. The probability of tissue adhesive being the dressing with the highest net benefit was 35%.
Cost-effectiveness analysis results.
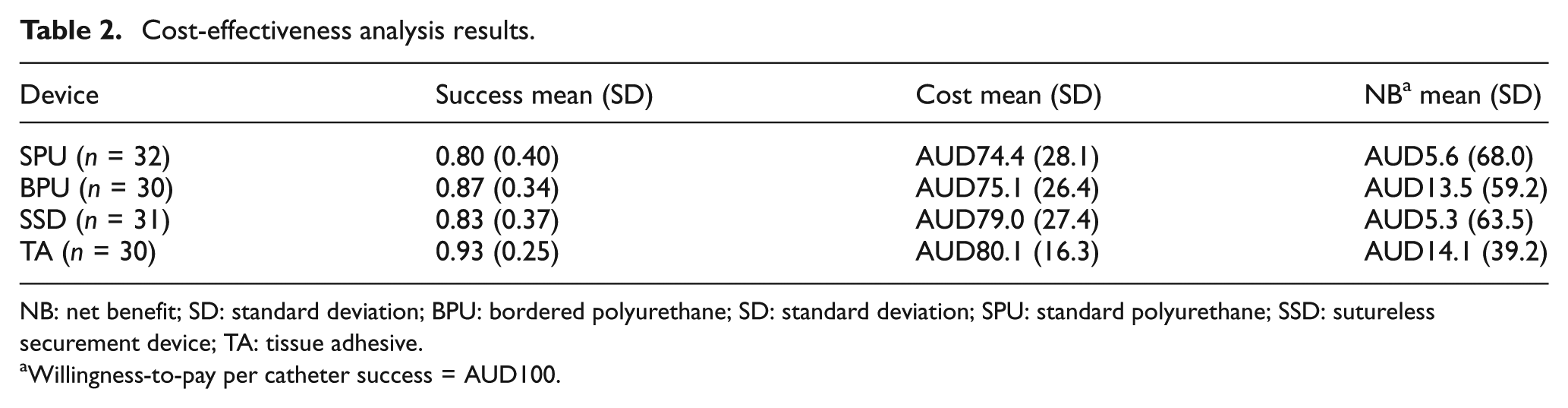
NB: net benefit; SD: standard deviation; BPU: bordered polyurethane; SD: standard deviation; SPU: standard polyurethane; SSD: sutureless securement device; TA: tissue adhesive.
Willingness-to-pay per catheter success = AUD100.
VOI measures
The estimated expected value of perfect information from the pilot study was AUD6.8/patient at the willingness-to-pay threshold of AUD100/catheter success. This amounted to a population expected value of perfect information of AUD850,000 (125,000 patients × AUD6.8). Such value indicated high level of uncertainty in the pilot study results, suggesting that additional research might be potentially worthwhile. As the sample size increased and more uncertainty is resolved, the calculated expected value of sample information converged to the expected value of perfect information (Figure 2). The highest expected value of sample information was associated with the four-arm trial design followed by the three-arm designs of (standard polyurethane, bordered polyurethane and tissue adhesive) and (standard polyurethane, bordered polyurethane, and sutureless securement device); however, the three-arm design of (standard polyurethane, sutureless securement device, and tissue adhesive) provided lower expected value of sample information compared to the two-arm trial (standard polyurethane, bordered polyurethane). Subtracting the associated total research cost from the four designs with the highest expected value of sample information values generated the expected net benefit of sampling curves (Figure 3).
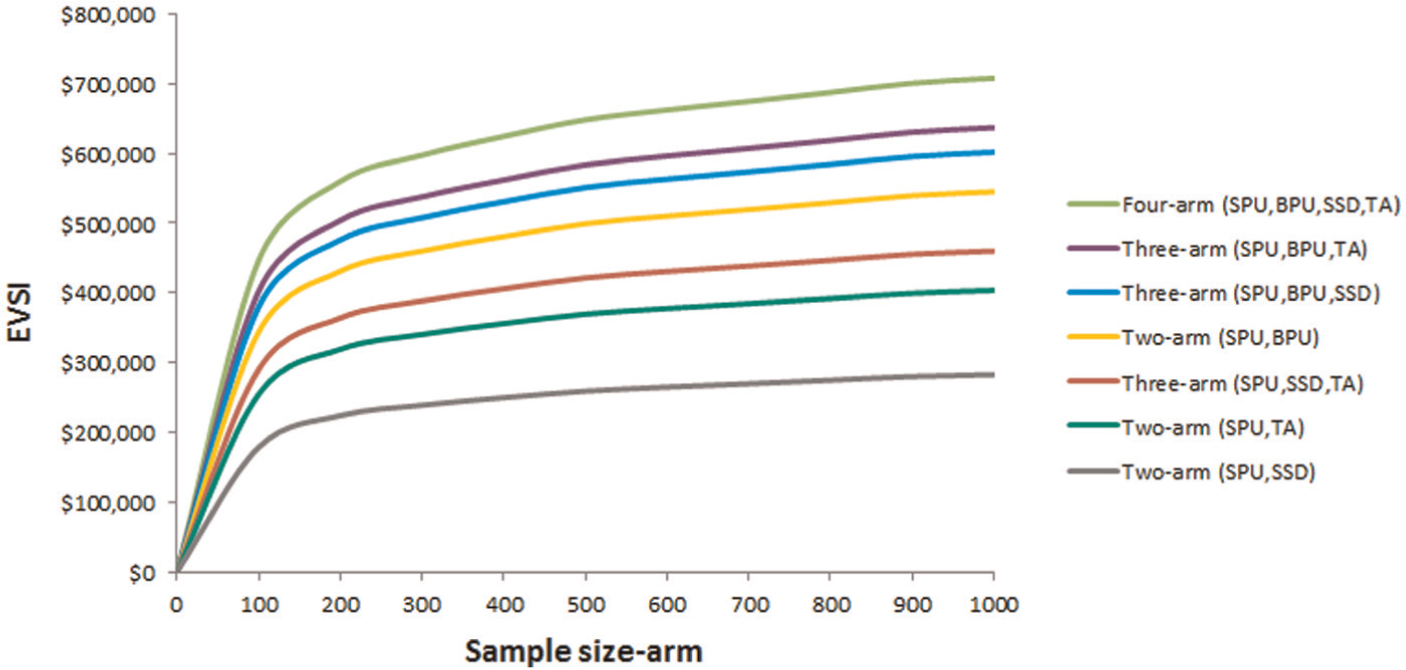
EVSI for the alternative future trial designs.
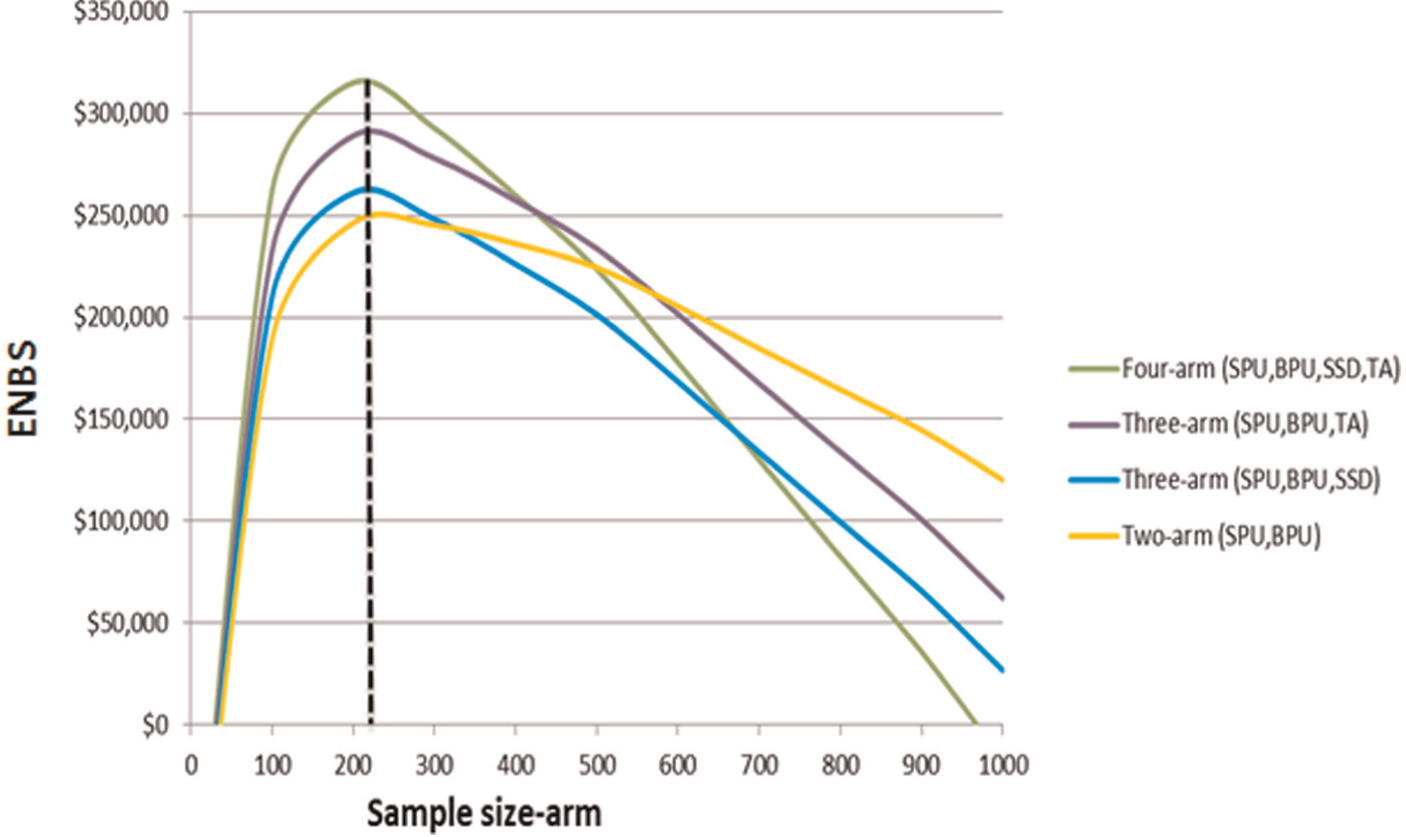
ENBS for the alternative future trial designs.
The expected net benefit of sampling was positive, that is, the expected research benefits exceeded expected costs, for sample sizes from 50 to 980 in each arm for all future trial designs. However, the expected net benefit of sampling was the highest in the four-arm design with 220 patients in each arm with AUD325,324 at a total cost of AUD250,000, providing a return-on-investment of 130%. However, the return-on-investment for the three-arm design (standard polyurethane, bordered polyurethane and tissue adhesive) was the highest with 132% although it had lower expected net benefit of sampling compared to the four-arm design (Table 3). Finally, the expected net benefit of sampling from the initially calculated sample size of 388 patients/arm was AUD282,200 at a cost of AUD357,800, providing a return-on-investment of 79%. In a sensitivity analysis, the optimal design remained with four arms and a sample size between 220 and 250/arm when the lifetime of the technology was increased to 10 years, and a sample size between 190 and 220/arm when the willingness-to-pay varied between AUD50 and AUD400 for catheter success.
Calculated value of information measures for the alternative future trial designs.
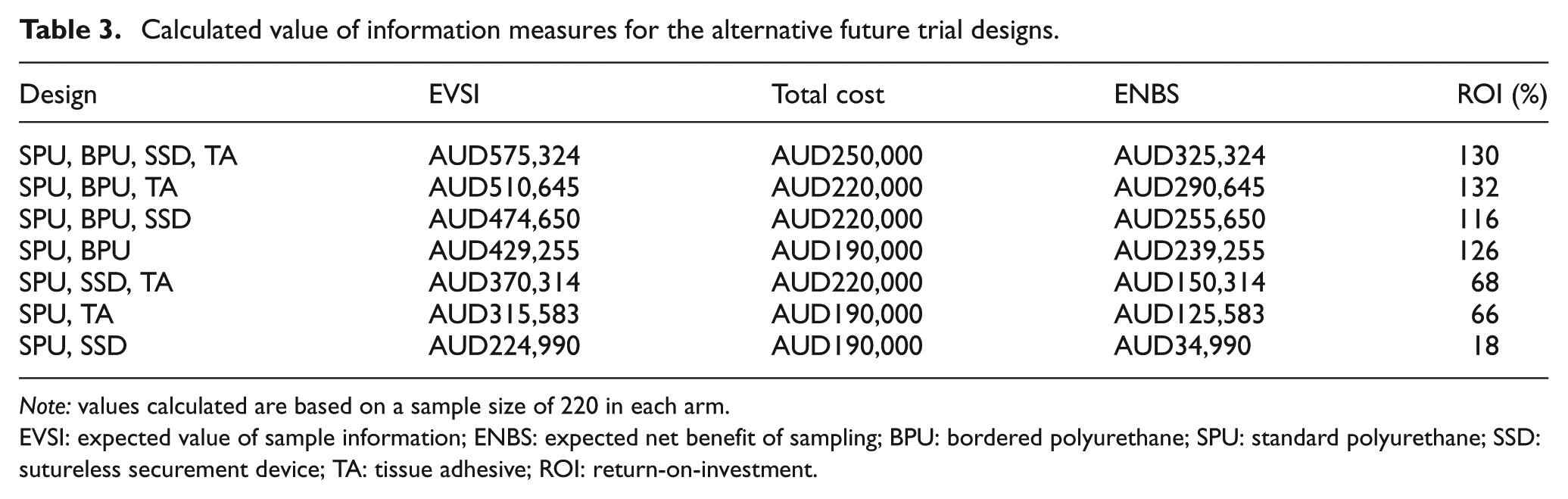
Note: values calculated are based on a sample size of 220 in each arm.
EVSI: expected value of sample information; ENBS: expected net benefit of sampling; BPU: bordered polyurethane; SPU: standard polyurethane; SSD: sutureless securement device; TA: tissue adhesive; ROI: return-on-investment.
Discussion
This article presents an application of VOI analysis to inform the optimal trial design for a clinical trial based on the results of a pilot study on arterial catheter securement devices. The pilot study showed that newer devices such as tissue adhesive and bordered polyurethane were more effective than the conventional standard polyurethane dressing. However, when considering the costs of the evaluated devices, the tissue adhesive appeared to be more cost-effective compared to the other options. This finding was not certain because the probability of tissue adhesive being cost-effective was only 35%. Applying VOI methods to the results of the pilot study indicated that the value of this uncertainty is sufficient to justify further research.
VOI analysis compared alternative future trial designs and suggested the optimal design that maximizes research benefits in terms of the number of arms and sample size. In this example, the four-arm trial design with 220 patients provided the highest expected net benefit of sampling. In addition, calculating the expected net benefit of sampling and return-on-investment enabled a quantitative prioritization of the proposed designs. 6 Interestingly, the design with the highest expected net benefit of sampling may not necessarily provide the highest return-on-investment, as evidenced by the results from the expected net benefit of sampling and the return-on-investment for the four-arm design and the three-arm design (standard polyurethane, bordered polyurethane and tissue adhesive). Because the objective of health-care systems is to maximize health benefits, research proposals should be prioritized based on their expected net benefits.6,8 Return on research investment is a useful indicator to compare the efficiency (i.e. how favorable the investment gains are compared to cost) of the competing research proposals, particularly when two or more proposals provide the same net benefit.
Another important feature of this analysis is that the VOI-based sample size (i.e. 220 patients/arm) was more economical than the sample size initially calculated based on type I and II errors and the smallest clinically significant difference. It has been argued that the VOI framework can provide an alternative to the standard hypothesis testing approach which relies on arbitrary chosen error probabilities where type I and type II errors receive the same weight (e.g. 5% and 20%, respectively) regardless of the consequences of making an error.7,8 In optimizing trial design, the VOI approach takes several factors into consideration. Such factors include the relative benefits and costs of the evaluated interventions, the lifetime of the technology, the population expected to benefit from research findings, the trial follow-up time, level of intervention implementation, and the associated research costs. Selecting the appropriate values for these factors is challenging and has been explored in several recent papers on VOI analysis informing multi-stage trial design, between-study variation, imperfect research implementation, and optimal trial design across jurisdictions.23–26 In this article, the calculated VOI measures were mainly driven by the level of uncertainty from the pilot study, the expected population in the State of Queensland that would benefit from the evaluated interventions over a given time period and the willingness-to-pay threshold per catheter success. However, a sensitivity analysis was performed to explore the effect of varying the willingness-to-pay threshold and the time horizon of the technology on our VOI estimates.
A limitation of our work is that the cost-effectiveness and VOI analyses were based on data from a single pilot study. It is possible that we have underestimated parameter uncertainty.13,27 Ideally, different sources of information should be sought to inform the analyses. However, the evidence in the field of catheter devices is scarce, and we could not identify relevant studies despite an extensive systematic search of literature. Accordingly, we had to make certain assumptions about the prior distributions such as that the pilot study population was assumed the same as the population that would be included in the full trial and also the same as the population for which we would make treatment decisions. Moreover, the design and conduct of pilot studies are not as rigorous as large randomized controlled trials which may result in biased results. 27 Another limitation of this analysis is that different follow-up durations were not evaluated in informing the optimal trial design. Due to the acute nature of the interventions, it was assumed that the outcomes would be readily available after the end of the proposed trial. With chronic diseases, a longer follow-up period provides more information to resolve uncertainty. However, this comes with increased research costs as well as an opportunity cost (i.e. benefit foregone) from delaying the use of a beneficial intervention awaiting the results from a clinical trial.
Unfortunately, despite the benefits of VOI analysis, the application of this approach in informing optimal trial design remains limited for two main reasons.12–15,28 First, it is commonly believed that estimating VOI measures, particularly the expected value of sample information, is computationally challenging. 10 Nevertheless, in recent years, there has been a progressive evolution and simplification of VOI methods.21,27,29–32 For instance, closed-form solutions are available to enable simpler calculation of VOI measures including the expected value of sample information.6,7,30 Second, optimizing research designs using VOI methods is relatively new. There is a need to create more awareness about the usefulness of this approach among researchers and research organizations using applied real-world examples.
In conclusion, the results in this article indicated that a larger clinical trial on catheter securement devices is potentially worthwhile. Based on VOI analysis, a future trial design of four arms with 220 patients in each arm is more economical than a design with the sample size calculated by hypothesis testing. The VOI approach should be considered early in the design of costly large clinical trials.
Footnotes
Acknowledgements
The authors would like to thank Mr Gabor Mihala for research assistance with data collection and management.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
Haitham Tuffaha is supported by a National Health and Medical Research Council PhD scholarship through the Centre for Research Excellence in Nursing Interventions for Hospital Patients. A National Health and Medical Research Council Project grant funded the clinical trial.