
Abstract
Keywords
Introduction
In the last three decades, coronary mortality in Western Europe and the USA was reduced by 50%. 1 Regrettably, the beneficial effect of improved resuscitation management, optimized revascularisation strategies, and secondary prevention of coronary heart disease (CHD) is at least partially contradicted by the rapidly increasing prevalence of obesity and the subsequent onset of type 2 diabetes mellitus (T2DM). According to data from the Multiple Risk Factor Intervention Trial (MRFIT) 2 and to a well-established Danish registry, 3 diabetes is considered to be a ‘CHD equivalent’.
Although target value achievement for blood pressure and lipid profiles has markedly improved in the last few years, there is still a need for the optimization of secondary prevention in diabetic patients with CHD. 4
The extent to which patients with T2DM receive secondary prevention according to these stringent treatment goals in clinical practice or the short-term prognosis of patients after cardiac rehabilitation (CR) have not been investigated in larger populations. Therefore, we aimed: (1) to study patients participating in CR after acute coronary syndrome (ACS) in order to assess the proportions and characteristics of three subgroups with different glucose metabolism states; (2) to analyse whether glucose metabolism was a predictor of one-year mortality; and (3) to derive predictors for cardiovascular death or revascularization events using the diabetic state and level of target value attainment for conventional risk factors.
Methods
Patients
The Transparency Registry to Objectify Guideline-Oriented Risk Factor Management (TROL) is a nationwide, prospective, observational registry. The present analysis was based on a subgroup of 1614 patients after the first ACS (mean age 55 ± 10 years; 85.9% men) who were hospitalized during an observation period between January 2005 and December 2006 for inpatient cardiological rehabilitation (CR) at four rehabilitation centres in Germany.
All patients underwent a two-dimensional and M-mode echocardiography with a calculation of the left ventricular mass (LVM) using Devereux’s formula and of the biplane left ventricular ejection fraction (LVEF) according to Simpson. All subjects without previously documented diabetes mellitus underwent a 75 g oral glucose tolerance test (OGT). The OGT was performed during the first week of the CR. Plasma glucose levels were measured at baseline and 2 h after the glucose load. The impaired glucose tolerance (IGT) was stated if the OGT 2 h glucose plasma concentration was ≥140 and <200 mg/dl. The T2DM was defined as a previously known diagnosis of diabetes with non-pharmacological (diet and exercise) or pharmacological anti-diabetic treatment, or if the 2 h post-OGT plasma glucose value was ≥ 200 mg/dl. 5 Patients with normal fasting (≤126 mg/dl) and 2 h glucose level were classified as ‘no diabetes’. According to the glucometabolic state, patients were classified into: group 1 – no diabetes (ND); group 2 – impaired glucose tolerance (IGT); and group 3 – manifest diabetes mellitus (T2DM).
To assess the cardiovascular risk profile, blood pressure, smoking status, total low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C), triglycerides, creatinine and HbA1c (in diabetic patients only) were recorded. The resting blood pressure was measured with two measurements spaced by 1–2 min in patients in the seated position after a 5-min resting period using a standard cuff positioned at the heart level. The target BP and LDL-C values were <140/90 mmHg and <100 mg/dl, respectively. Target HDL-C and triglyceride values were ≥40 mg/dl and ≤150 mg/dl for all patients, respectively. T2DM patients were expected to optimally achieve more stringent target values of blood pressure (<130/80 mmHg and <125/75 mmHg in the presence of proteinuria) and LDL-C levels (<70 mg/dl).
All patients underwent a structured rehabilitation program including individualized progressive physical training, education, training programmes for the reduction of cardiovascular risk factors and psychological support.6,7 The medication used was recorded at admission and discharge from rehabilitation. Patients were followed for a mean of 13.4 ± 2.7 months.
The protocol for this study was reviewed and approved by the ethics review board of the Bavarian Physician Chamber in Munich.
Statistics
Discrete variables were calculated as counts and percentages, while continuous variables were calculated as mean ± standard deviation. Changes within a group for discrete characteristics from baseline to the end-of-follow-up were tested with the McNemar test. Univariate between-group comparisons for nominal scaled variables were performed using the Chi-squared test, The Cochrane -Armitage trend test or Jonckheere-Terpstra test were used for ordinal scaled variables, and an analysis of variance (F-test) and polynomial contrast test were used for continuous variables, respectively. For the analysis of follow-up events (death, which was a composite of death and rehospitalization), multivariate logistic regression models were applied. In addition to the three groups (T2D, IGT and ND), the following variables were also considered: gender, age, BMI, history of previous stroke, peripheral arterial disease (PAD), renal failure, cancer, hyperlipidaemia, arterial hypertension, smoking/recently stopped smoking/non-smoking, microalbuminuria, family history of myocardial infarction, exercise capacity, left ventricular hypertrophy (LVH) and LVEF. Since LVH, LVEF and exercise capacity data were missing for 199, 91 and four of the patients, respectively, we analysed our data with multiple imputation. 8 A nominal p-value < 0.05 was considered statistically significant. No adjustment for multiplicity was performed.
Results
Patient characteristics
Baseline parameters, risk factors and end organ damages in different types of glucose metabolism
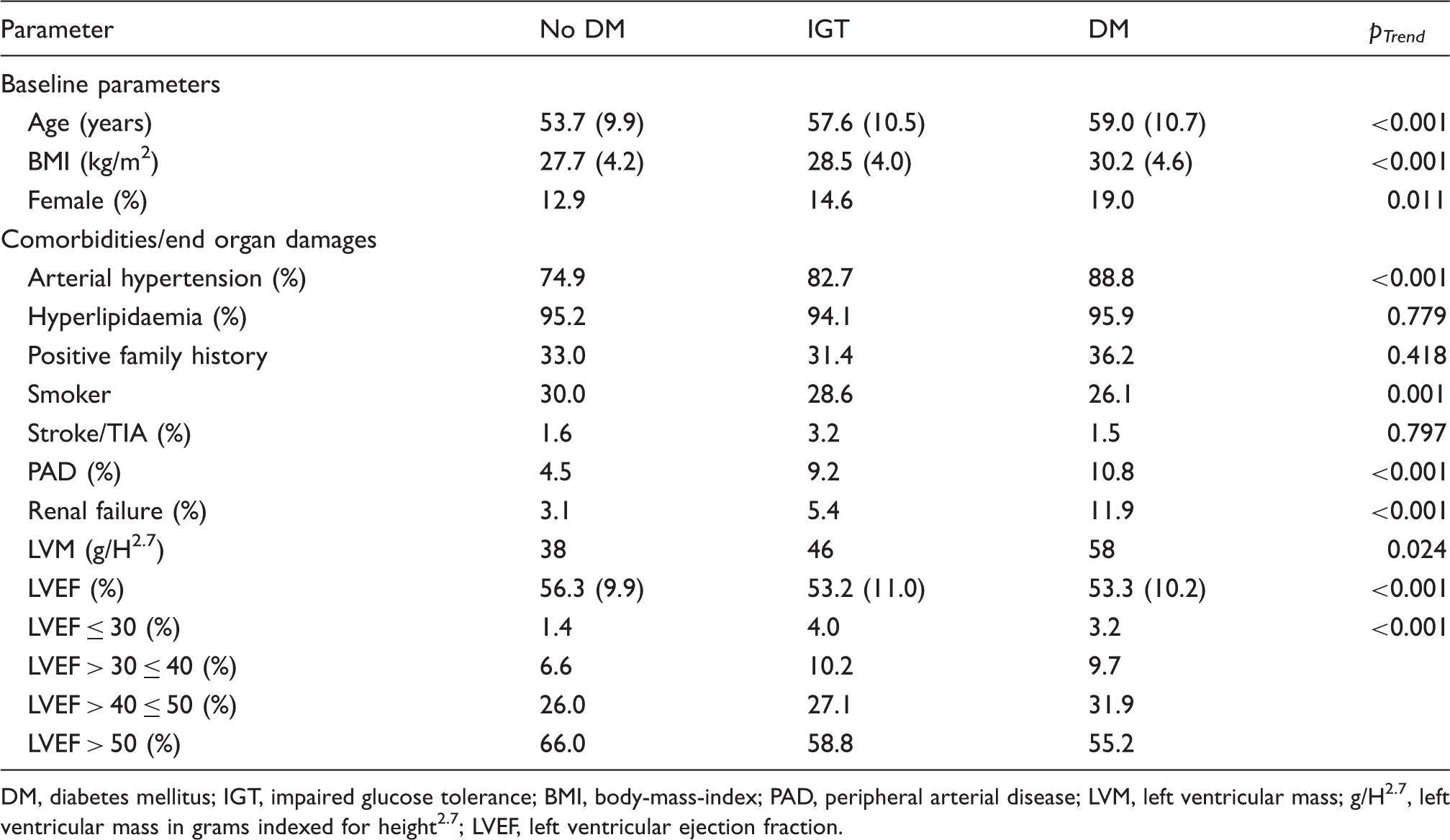
DM, diabetes mellitus; IGT, impaired glucose tolerance; BMI, body-mass-index; PAD, peripheral arterial disease; LVM, left ventricular mass; g/H2.7, left ventricular mass in grams indexed for height2.7; LVEF, left ventricular ejection fraction.
Pharmacotherapy
At the time of discharge, there was no significant trend between ND patients, patients with IGT and patients with T2DM regarding the prescription of beta-blockers (96.3%, 97.0% and 97.5%, respectively; pTrend = 0.314), ACE inhibitors (82.5%, 80.7% and 81.2%, respectively; pTrend = 0.872) and statins (94.4%, 93.4% and 95.8%, respectively; pTrend = 0.493). However, a trend was observed with a more frequent use for aspirin (ASA) in ND patients (97.3%, 95.2% and 93.3%, respectively; pTrend = 0.002). The trend for the prescription of vitamin K antagonists (3.6%, 5.4% and 8.3%, respectively; pTrend = 0.001), diuretics (24.8%, 41.0% and 47.1%, respectively; pTrend < 0.001), and ARB (9.9%, 13.3% and 17.9%, respectively; pTrend < 0.001) increased with the occurrence of IGT and diabetes.
Change in pharmacotherapy during follow-up
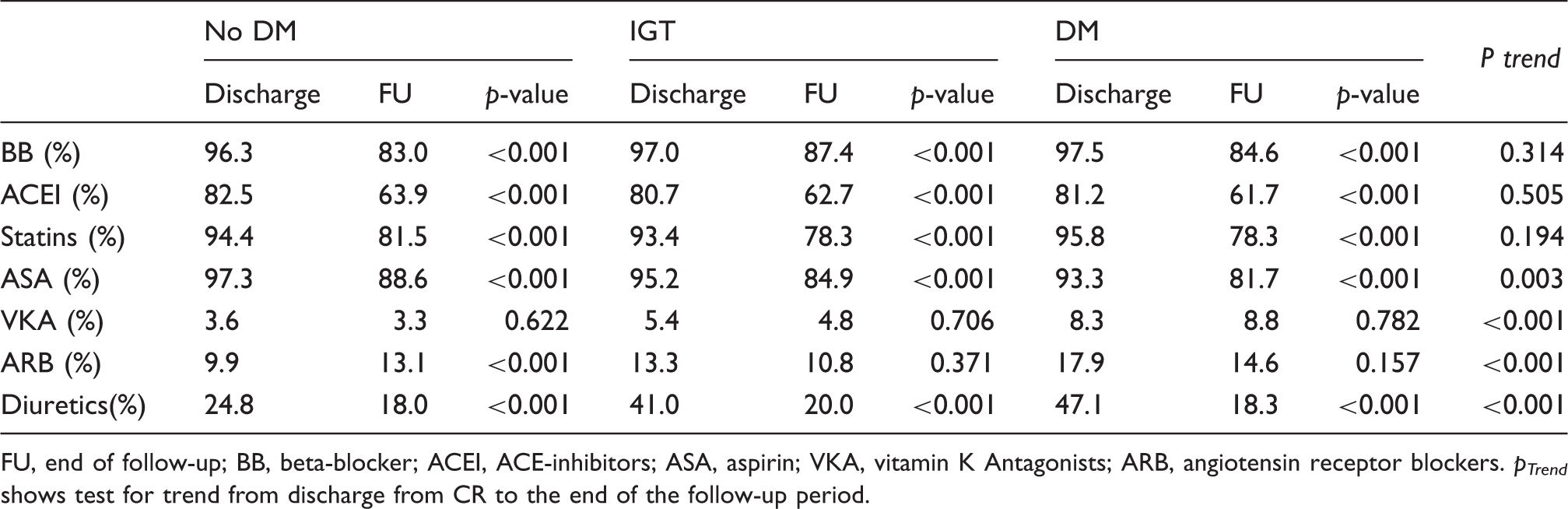
FU, end of follow-up; BB, beta-blocker; ACEI, ACE-inhibitors; ASA, aspirin; VKA, vitamin K Antagonists; ARB, angiotensin receptor blockers.
p Trend shows test for trend from discharge from CR to the end of the follow-up period.
Risk factors and target value attainment
Cardiovascular risk factor at discharge from CR
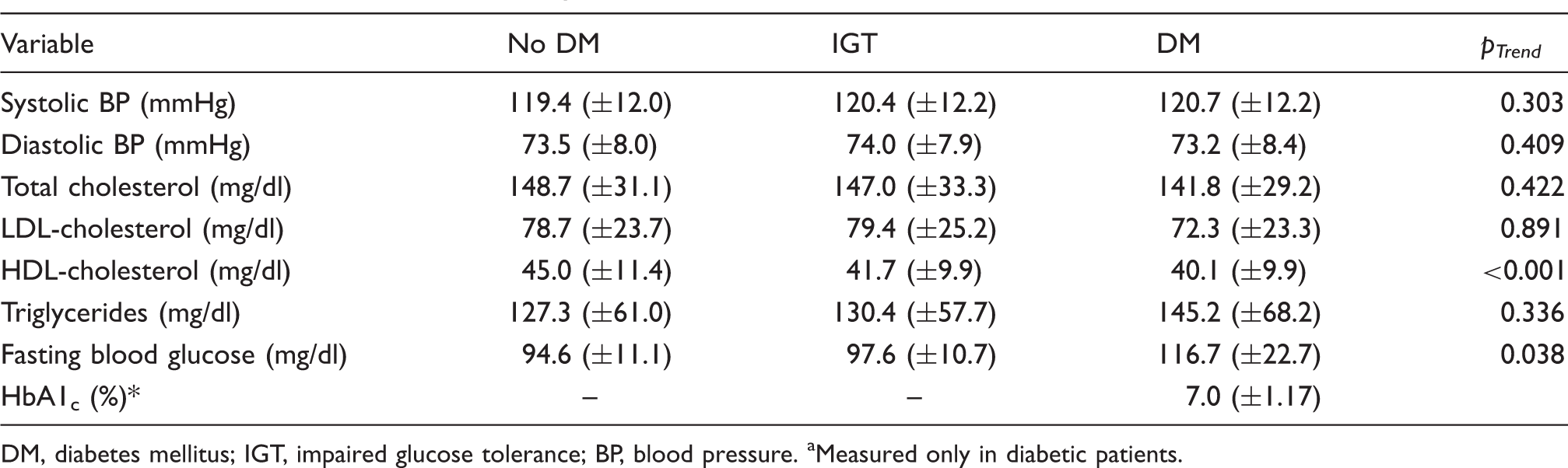
DM, diabetes mellitus; IGT, impaired glucose tolerance; BP, blood pressure.
Measured only in diabetic patients.
The individual target values for BP (<140/90 mmHg) were achieved in 90.8%, 89.1% and 88.7% of patients in groups 1, 2 and 3, respectively (pTrend = 0.267), whereas the target values for LDL-C (<100 mg/dl) were achieved in 81.5%, 80.8% and 87.0% of patients in these groups, respectively (pTrend = 0.066). There was also a trend of a lower proportion of patients reaching target values for HDL-C (60.8%, 51.4% and 46.1% of patients in group 1, 2 and 3, respectively; pTrend < 0.001) and triglycerides (74.6%, 73.9% and 65.1% of patients in groups 1, 2 and 3, respectively; pTrend = 0.004) (Figure 1a).
Distribution of target value attainment in postinfarctional patients at CR discharge. (a) Moderate target values (see text). (b) Strong target values for T2DM patients (see text). ND, non-diabetic; IGT, patients with impaired glucose tolerance; T2DM, diabetes mellitus. **p < 0.01, ***p < 0.001.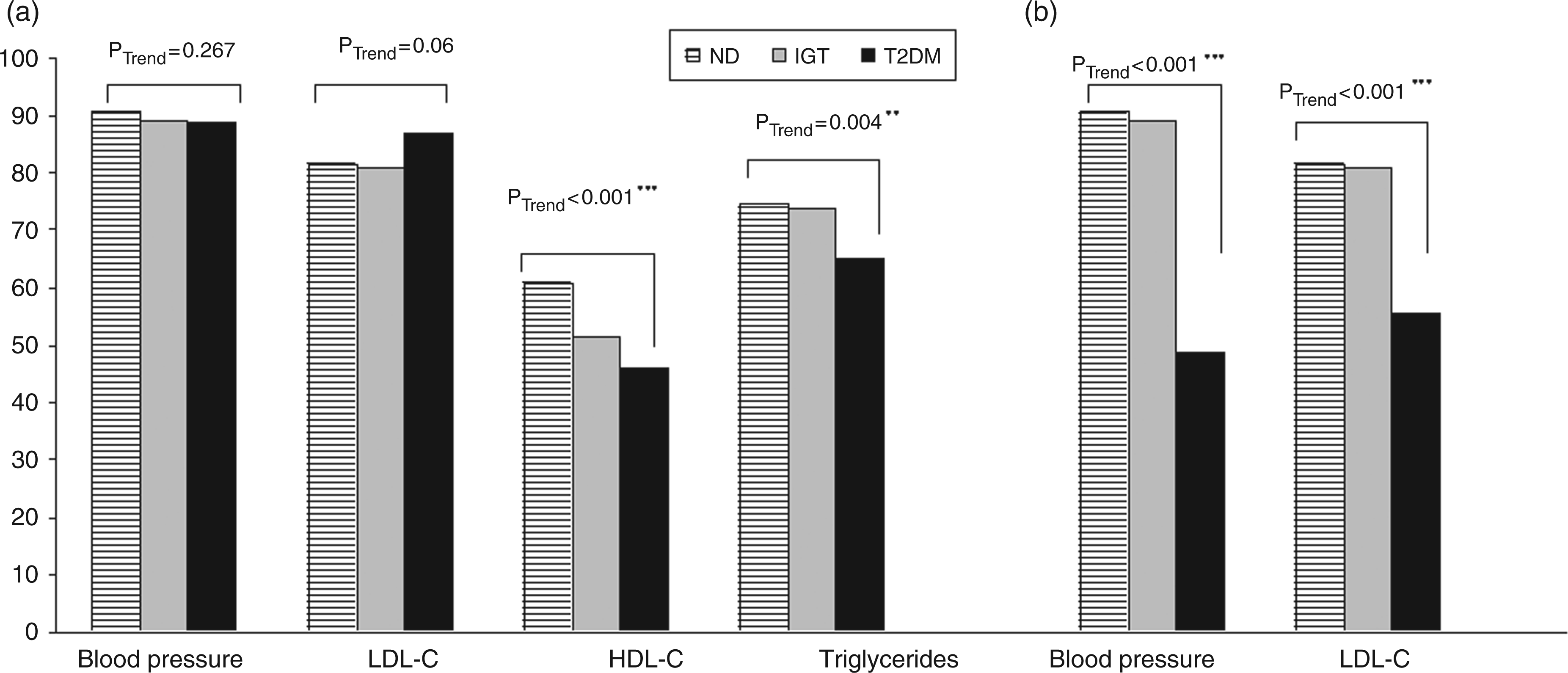
In post-ACS patients with T2DM, a higher blood pressure was achieved in only 48.9% of the patients with diabetes, whereas better lipid target values were achieved in only 55.6% of these patients (Figure 1b).
Prognosis
Death and rehospitalization due to cardiovascular events in 1-year follow-up
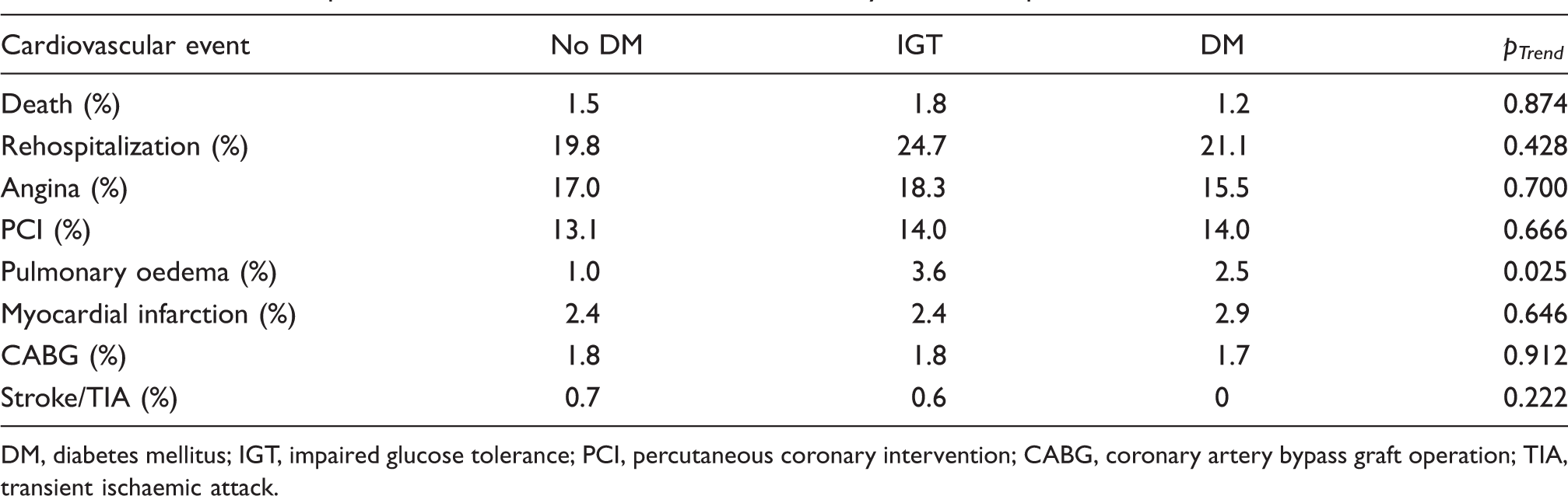
DM, diabetes mellitus; IGT, impaired glucose tolerance; PCI, percutaneous coronary intervention; CABG, coronary artery bypass graft operation; TIA, transient ischaemic attack.
In the multivariate analysis, the diagnosis of diabetes or IGT did not have any predictive value for overall mortality. The strongest multivariate predictors were history of stroke (OR, 6.29 [95% CI: 1.06–37.19]; p = 0.042) and with a trend PAD (OR, 3.60 [95% CI: 0.95–13.68]; p = 0.061). An improved left ventricular ejection fraction (1% increase was associated with a 5.5% mortality risk reduction) and increased BMI (1 kg/m2 caused a 3.8% mortality risk reduction) were associated with a good prognosis (Figure 2).
Predictive parameters for overall mortality. Glucometabolic status shows no significant prognostic influence, whereas previous stroke and, by trend, peripheral artery disease were associated with a worse outcome. OR, odds ratio; CI, 95% confidence interval; IGT, impaired glucose tolerance; BMI, body mass index; LVH, left ventricular mass; EF, left ventricular ejection fraction.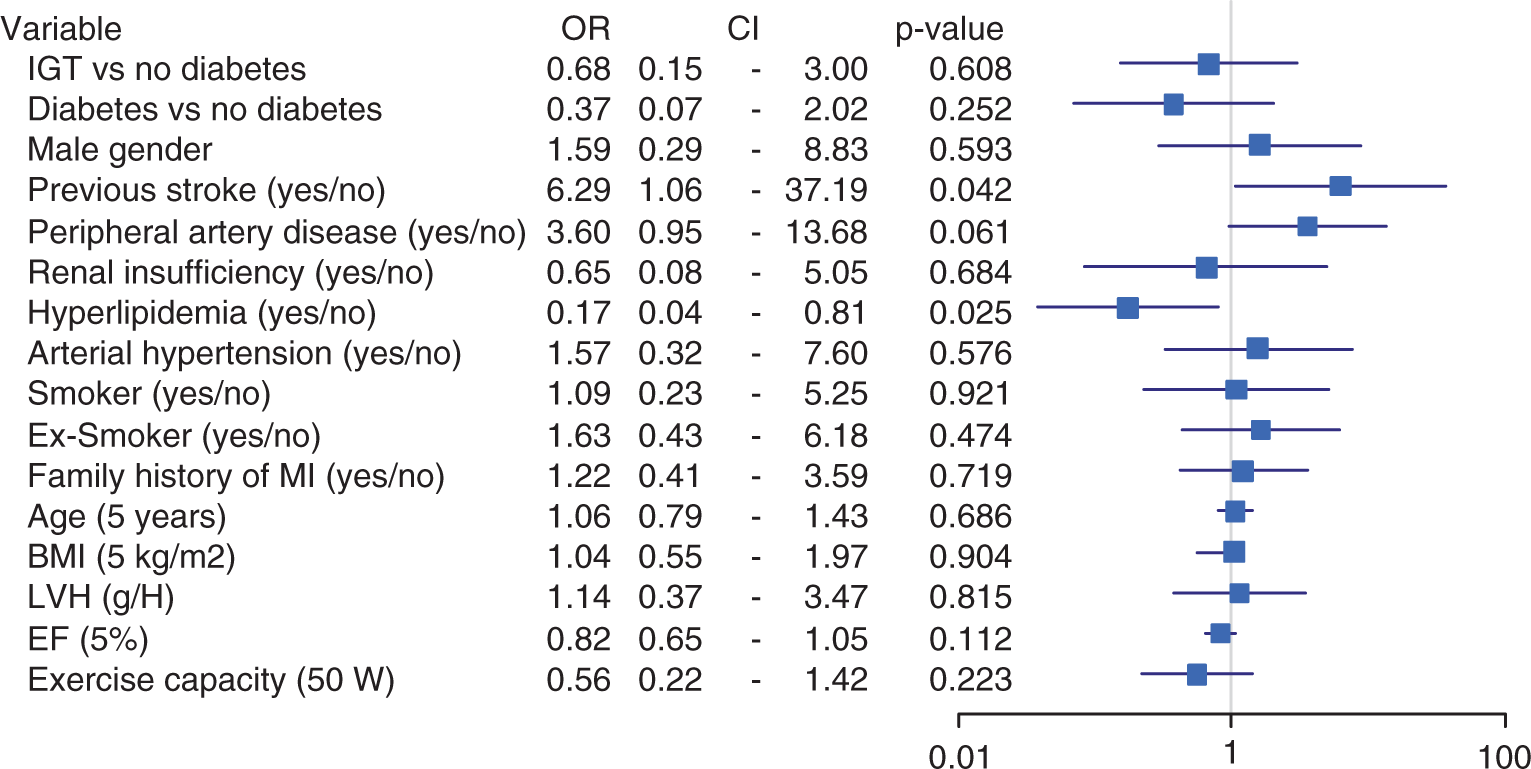
Discussion
This study had three important findings. First, due to the combination of optimized revascularization, secondary preventive pharmacotherapy and comprehensive rehabilitation programmes, the prognosis of both diabetic and non-diabetic patients after ACS was favourable.
Second, despite the subsequent implemented pharmacotherapy, the achievement of the recommended lower target LDL-C and blood pressure levels for patients with T2DM occurred less often compared to ND patients. Nevertheless, in our study population, mortality was not associated with the presence of diabetes or IGT, but with selected comorbidities, including stroke and PAD.
Glucose metabolism
In the registry, the percentage of post-ACS patients with diabetes was comparatively low (16.6%). In earlier studies, the proportion of these patients with diabetes was reported to be up to 30%. 9 The smaller proportion in our analysis may be explained by the younger age of the patients (mean 55 years). However, it is important to emphasize that if impaired glucose tolerance is also taken into account, which is presumably a negative prognostic parameter, every sixth patient after an ACS event had impaired glucose metabolism.4,10 Therefore, the fundamental goal in every CHD patient should be the evaluation of pathological glucose metabolism using a routinely performed oral glucose tolerance test during cardiac rehabilitation. This criterion has been implemented as a Class I recommendation in the most recent EASD guidelines. 11
Blood pressure
In patients with T2DM, a high incidence of additional risk factors have been observed, with arterial hypertension and lipid disorders being the predominant factors. On the basis of the UKPDS 12 and the Hypertension Optimal Treatment Study 13 in diabetic patients, the current guidelines recommend a blood pressure target of <130/80 mmHg. 11 In our study, a conservative target BP value of <140/90 mmHg was attained in a high proportion of patients; however, there was a significant difference in favour of ND patients. As in other studies,14,15 we found that fewer than half of the diabetic patients met the requirements of a BP target value below 130/80 mmHg in our study. A comparable use of antihypertensive medication across the groups may be a crucial factor for the reduced efficacy in blood pressure therapy seen in patients with T2DM, indicating the need for intensified management of diabetic patients who are particularly hypertensive. Although ESH/EASD guidelines still suggest stringent blood pressure control, the recently published ACCORD-BP trial 16 demonstrated that targeting a more stringent systolic blood pressure (<120 mmHg vs <140 mmHg) in diabetics was not associated with a better outcome, but was associated with an increase of serious adverse events related to blood pressure medication. Therefore, further data are needed to determine the most appropriate blood pressure targets for T2DM patients.
Lipid management
Regarding LDL-C targets, we focused on the 100 mg/dl threshold for non-diabetic and IGT patients as well as the 70 mg/dl threshold for diabetic patients according to NCEP ATP III criteria, 17 which have been adopted by many societies.11,18
In comparison to other large registries (e.g. GRACE or RIKS-HIA), in which statins were prescribed in less than 50% of the patients, the high prescription rates of over 90% in all groups in this study could hardly be increased.19,20 A high proportion of diabetic and non-diabetic patients achieved the conservative target values during CR, yet a preponderance of these patients had T2DM. Nevertheless, despite an above-average statin prescription rate of 95.8%, only half of the diabetic patients achieved the required level below 70 mg/dl. This may be explained by the comparatively short monitoring period during the 3-week cardiac rehabilitation.
Prognosis
In the last two years, several large-scale trials, including ACCORD, 9 ADVANCE, 21 and VADT, 22 have demonstrated a predominant reduction of microvascular complications in T2DM patients under stringent blood glucose control, but failed to show a positive impact on macrovascular events. In contrast, the UKPDS 10-year Post-trial monitoring 23 together with the Steno-2 study 15 revealed a reduction of macrovascular damage and thus, of morbidity and mortality over a long-term observation period of more than 10 years.
Although it has been widely demonstrated that all stages of glucometabolic perturbations are associated with a worse cardiovascular outcome, 24 our population had a favourable prognosis. While Donahoe et al. 25 reported a one-year mortality rate of 13% for patients with T2DM and 8% for ND patients in a 62,000 post-infarction patient cohort, we found a markedly lower mortality rate of 1.3% without statistical differences between groups. Our findings are in agreement with previous data by de la Hera et al., 26 which also showed that diabetes and IGT had no impact on cardiovascular outcome at 12 months. We hypothesize that this may be due to the comparatively young age of our patients (mean 55 years), the high rate of revascularization and the stringent guideline-based secondary preventive pharmacotherapy.
The multivariate analysis showed that the overall mortality was determined by a history of previous stroke and the presence of PAD. These findings are in accordance with data of the getABI study, 27 which supports the deleterious prognosis of patients with PAD even in the absence of symptoms. It has been previously shown that an ankle branch index of <0.9 is prevalent in 42% of hypertensive patients after ACS and is strongly associated with a worse outcome. 28 Even in healthy subjects, a low ABI (≤0.9) is associated with a doubling of the 10-year total mortality rate. 29 In contrast, patients with hypercholesterolaemia have a better prognosis, most likely due to the simultaneous administration of statins. Therefore, our data raise the question of whether the diagnosis of glucometabolic perturbation is independently associated with a worse outcome. A study with a larger cohort of post-ACS patients and a longer follow-up are necessary to confirm this hypothesis.
Limitations of this study
This study had several limitations. First, this observational prospective study was performed without randomization. Participation was voluntary and a selection bias cannot be ruled out. We focused on a highly selected population of nearly complete revascularized patients in a follow-up examination after CR. Second, the data reported here had nominal p-values without adjustment for multiplicity. The study was not powered for the multitude of statistical tests we performed and therefore some significance could have occurred by chance alone. Furthermore, we do not have HbA1c values in the follow-up as an indicator of the quality of diabetes treatment. The differentiation between patients with newly diagnosed versus long-standing T2DM was also not performed. Finally, the follow-up in this study was 13 months and comparatively shorter than other studies, and therefore the overall event rate was comparatively low. This may explain the large confidence intervals of prognostic parameters.
Conclusion
After the first acute coronary syndrome, a large percentage of both diabetic and non-diabetic patients achieved moderate target blood pressure and lipid values. Moreover, these patients demonstrated a favourable and comparable one-year prognosis independent of the glucometabolic status. Our results are in agreement with recent data that showed that a more aggressive reduction of blood pressure in diabetic patients may not improve outcome. Therefore, the target BP and lipid values of T2DM patients continue to be the subject of debate.
Funding
This study was funded by MSD SHARP & DOHME GMBH, Haar, Germany and Essex Pharma, Munich, Germany. KB and CJ are employees of MSD SHARP & DOHME GMBH.
Conflicts of interest
The other authors declare no conflict of interest.
Footnotes
Acknowledgments
The TROL registry was run in cooperation with the German Society for Prevention and Rehabilitation of Cardiovascular Diseases (DGPR). Parts of this work were presented at the Annual Congress of the EACPR, 8 May 2009, Stockholm, Sweden.