
Abstract
Introduction
Throughout the world, 16.7 million deaths are due to cardiovascular diseases (CVD). In Europe these diseases are the principal cause of death; they have a high incidence rate 1 and are one of the primary causes of disability and decline in health. 2 All of the above are owing to the high prevalence of the primary cardiovascular risk factors in European countries. 3 In Spain, CVD constitutes the primary cause of overall mortality and is the second cause of death after cancer among middle-aged Spaniards.
The primary risk factors for development of CVD (smoking, hypertension, obesity/excess weight, dyslipidaemia, and diabetes mellitus) explain a significant part of the incidence of CVD in the population. This association is more frequent than expected in the hypertensive population cared for and cardiovascular risk factors (CVRF) increase its concomitance in an exponential manner. Cardiovascular prevention is based on detection, treatment, and management of modifiable CVRF. Currently, management of this condition is based on knowledge of the overall CVRF of the patient and not solely on an isolated assessment of risk factors as recommended by the current guidelines of the European Society of Hypertension and the European Society of Cardiology (ESH/ESC). 4
There is little information at our disposal in regard to CVRF associated with the beginning of the hypertensive process and its diagnosis in middle age. Younger patients have physiopathological characteristics that differ from those of older patients. Of the two largest components participating in the development of arterial hypertension, volume and vasoconstriction, it is the latter which appears to be predominant in younger patients, as the first mainly coexists with the elevation of blood pressure in older subjects.5,6 Secondly, there is the fact that, at younger ages, hypertension corresponds to what is known as systo-diastolic hypertension, with a better-preserved pulse pressure due to better condition of the large arteries and the increase in peripheral resistance.
Because of the focus on patients of advanced age in primary care, few data exist about younger patients’ cardiovascular profiles. The primary objective of this study was to describe the clinical profile of hypertensive patients under the age of 55, newly diagnosed in primary care in Spain. The secondary objectives were to describe the prevalence of CVRF and associated target organ damage and to quantify the overall CVR of these patients at the time of the hypertension diagnosis.
Methods
This is a cross-sectional, multicentre observational study performed at primary care centres. A total of 2108 primary care physicians evenly distributed throughout the country participated and 6815 patients were included. The study was approved by the research ethics committee of the Hospital Clínico San Carlos in Madrid. All patients gave their written informed consent. Between February and June 2009, the research physicians gathered data from the first three consecutive patients who sought care from them and who met all of the inclusion criteria: (a) of either gender between 18 and 55 years of age; and (b) newly diagnosed with hypertension without antihypertensive treatment or started treatment less than 1month prior.
Only one visit was needed for inclusion. The physician collected data from the visit and data from the clinical chart, in a specially designed electronic survey. The following topics were covered: personal cardiovascular history (establishing the presence of cardiovascular or renal disease), presence of diabetes, record of the global CVRF based on the ESH/ESC 2007 guidelines, 4 that is sex, age (less than 55 years), presence of tobacco abuse defined as at least one cigarette daily, actual measurement of systolic and diastolic blood pressue (SBP and DBP) (average of three consecutive readings taken in sitting position), dyslipidaemia (total cholesterol >190 mg/dl, high-density lipoprotein (HDL) cholesterol <40 for men and <46 for women, low-density lipoprotein (LDL) cholesterol >115 mg/dl, triglycerides >150 mg/dl, or lipid-lowering treatment); fasting glucose 102–125 mg/dl, abnormal glucose tolerance test, reported measurements of height and weight with body mass index calculation and waist measurement (abdominal obesity was considered if waist circumference >88 cm in women and >102 cm in men), and family history of premature CVD (define as male <55 years and female <65 years). Urinary albumin/creatinine ratio (averaged from three first morning void urine samples) ≥22 in men and ≥31 mg/dl for women was considered subclinical organ damage, and >300 mg/24 h established renal disease; left ventricular hypertrophy (Sokolov-Lyon criteria >38 mm or Cornell >2440 mm/ms) and serum creatinine (slight increase 1.3–1.5 mg/dl for men and 1.2–1.4 for woman established renal disease: creatinine >1.5 mg/dl in men and >1.4 mg/dl for woman), low estimated glomerular filtration rate (<60 ml/min/1.73 m2), record of medication actually taken for CVRF. We collected all applicable information to calculate the 10-year risk for CVD based on the ESH/ESC scale. Out of the 6815 clinical research forms returned, 6765 patients were eligible for evaluation. The main criteria for patient exclusion from the analysis were failure to meet inclusion criteria and missing or contradictory data.
Statistical analysis
The sample size of 4500 patients is sufficient in order to obtain reliable estimates for the principal objective, if the precision error is no greater than 1.5% and with a minimum 95% confidence interval. A total of 6000 patients were established for inclusion, assuming that some data would be lacking of any of the analysis parameters in around 25% of the patients. In the end, with 6788 valuable patients, the confidence interval had a precision error of <1.2% in the different parameters analysed.
Descriptive statistics were made of all variables, including measurement of central tendency and dispersion for the quantitative variables and absolute and relative frequencies for the qualitative variables, with 95% confidence intervals in both cases.
The distribution type of the quantitative variables was studied and their adjustment to a Gaussian distribution was evaluated using the Kolmogorov–Smirnov test. When data did not meet the assumptions of normality, non-parametric statistical methods were used.
In the comparisons of independent data (between two analysis groups), the Student’s t-test was used for quantitative variables, the Mann–Whitney U test was used for quantitative variable that did not follow a Gaussian distribution and the chi-squared test or Fisher test was used for qualitative variables. The statistical tests were performed with a significance level of 5% and were bilateral. The SAS version 8.2 statistical package was used to perform all statistical analyses.
Results
Characteristics of study population
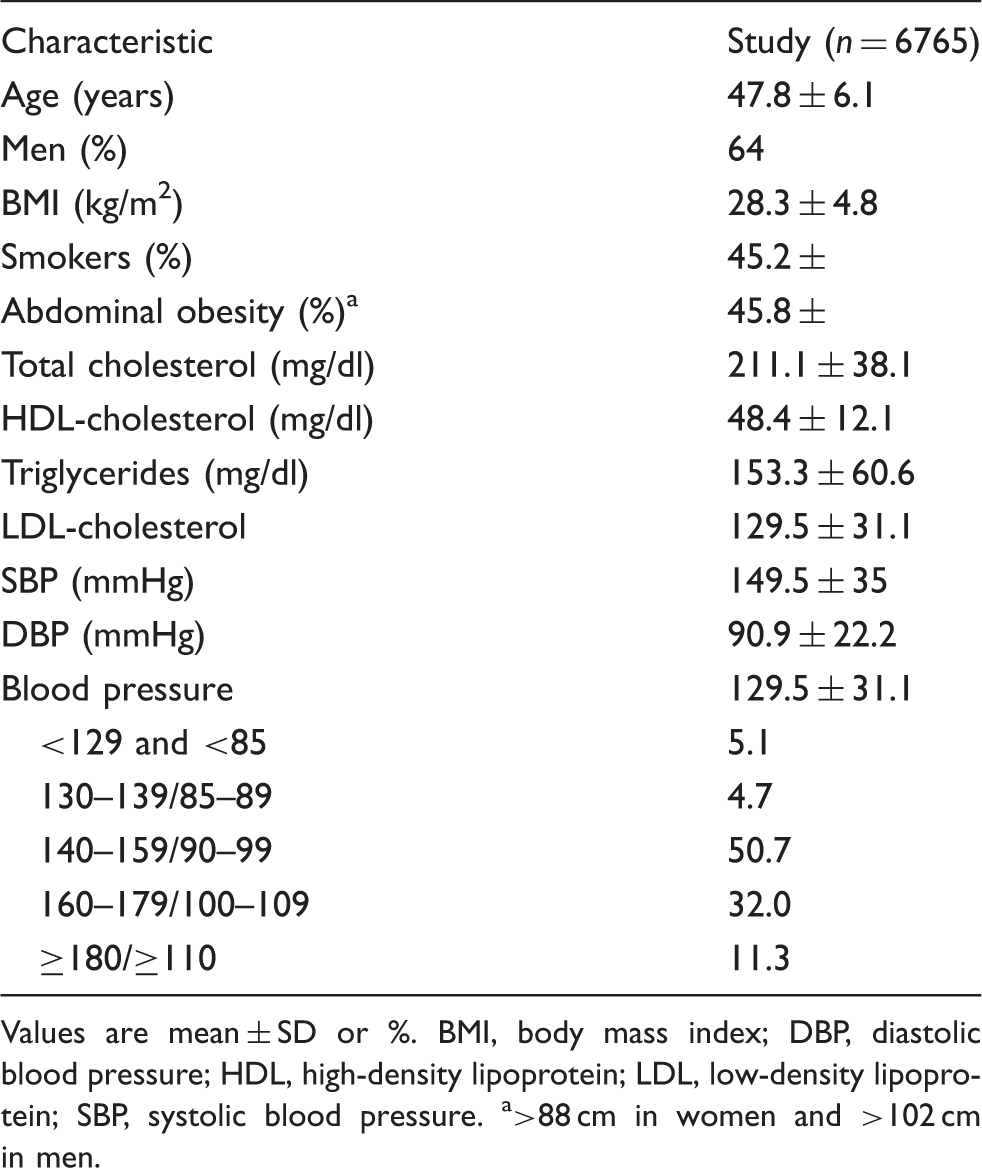
Values are mean ± SD or %. BMI, body mass index; DBP, diastolic blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein; SBP, systolic blood pressure. a>88 cm in women and >102 cm in men.
Regarding the reason for diagnosis, 15.5% of patients asked their physicians for a blood pressure measurement because they suffered symptoms that they thought related with high blood pressure (headache, heaviness of head, dizziness). Of the high blood pressure diagnoses, 15.8% was diagnosed because they had had a cardiovascular event and the remaining 68.7% had had their blood pressure measured during a routine examination. Overall, 81.3% of the diagnoses were made by a primary care physician and 18.7% were made in a different environment (specialist, hospitals, company doctor, etc.).
Associated risk factors
Dyslipaemia was found in 80.4% of the patients, and out of them, 37.9% were taking statins prior to the hypertension diagnosis. Also, 45.2% were smokers, 45.8% had abdominal obesity, 22.2% had a family history of premature CVD.
A total of 13.6% of the patients were diabetics prior to the hypertension diagnosis, with 73.5% of them undergoing antidiabetic treatment. Of the non-diabetic patients, 22.9% had fasting glucose 100–125 mg/dl.
The prevalence of metabolic syndrome (MS) in the total group was 44.4%; when this calculation was made excluding patients diagnosed with diabetes, the prevalence was 39.2%.
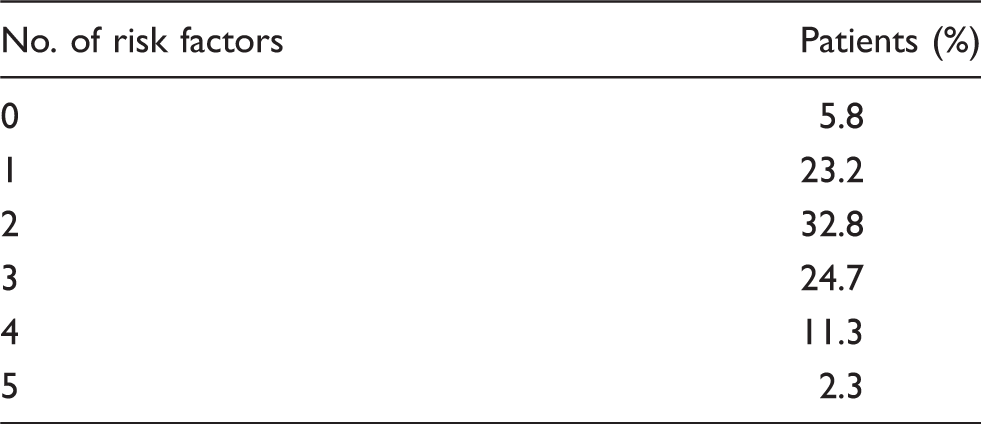
Prevalence of cardiovascular risk factors in young hypertensive patients
Target organ damage
A total of 28.6% of the sample had target organ damage. Left ventricular hypertrophy (diagnosed through ECG using Sokolow or Cornell criteria) was seen in 7.33% of the patients; in 26.1%, cardiac repercussion was not assessed by any method. A slight increase in plasma creatinine or low estimated glomerular filtration rate was seen in 9.75% of the patients, and 19% tested positive for microalbuminuria. The information about microalbuminuria was present in 99.9% of the surveys.
Established cardiovascular and renal disease
Of all subjects, 15.8% had one or more associated clinical disease, with a prevalence of 2.9% for cerebrovascular disease, 6.4% for heart disease, 4% for kidney disease (3.5% of the patients showed proteinuria > 300 mg/g), 6.7% for peripheral vascular disease, and 1.8% for advanced retinopathy. All this patients were diagnosed of hypertension during or after of the cardiovascular event.
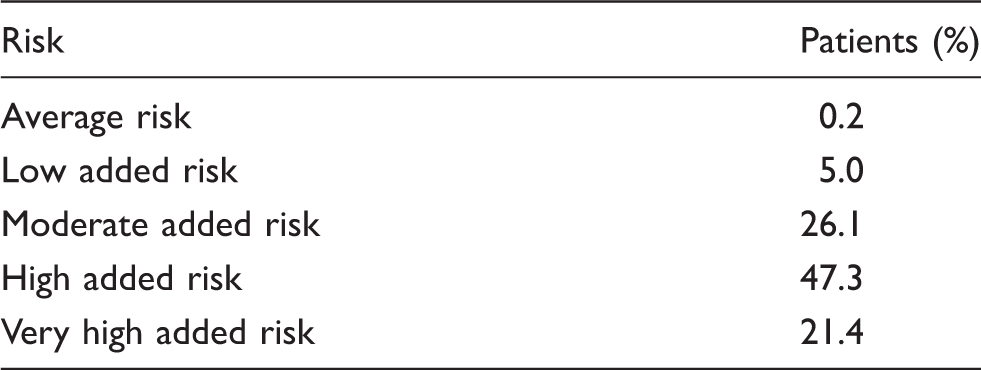
Stratification of cardiovascular risk
Distribution of patients according to 10-year cardiovascular risk (European Society of Hypertension and European Society of Cardiology 2007)
Overall 10-year risk of cardiovascular disease according to European Society of Hypertension and European Society of Cardiology
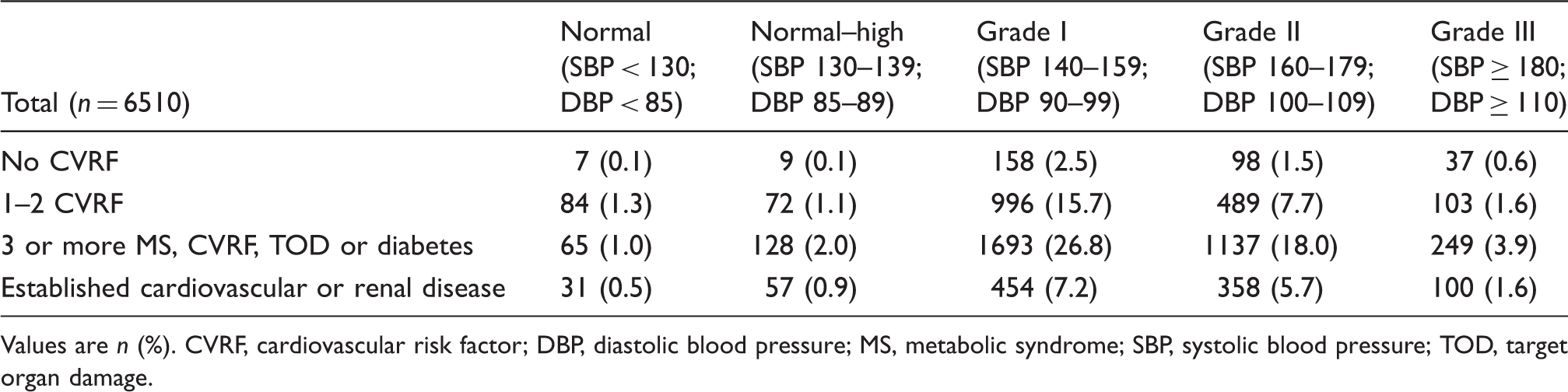
Values are n (%). CVRF, cardiovascular risk factor; DBP, diastolic blood pressure; MS, metabolic syndrome; SBP, systolic blood pressure; TOD, target organ damage.
Discussion
Numerous observational studies recently performed in Spain have shown the strong association of hypertension with other CVRFs. 7 These studies generally encompass patients over the age of 60 and, in these patients, the prevalence of associated CVRF was up to 96% of the sample studied. In the majority of clinical trials, the average age of hypertensive patients is over 658,9 and in others, the age was 56–65 years.10,11 The average age in the CAPP study 12 and in the Steno–2 study 13 was 55. Therefore, we have little information of the hypertensive patients with less than 55 years.
In our study, the first noteworthy piece of information is the strong association of CVRF produced at the time of diagnosis of hypertension in younger patients. The study found that 95.2% of the sample has one or more CVRF associated with hypertension, a percentage similar to data from other studies on older subjects. 14 The second major observation is the high percentage of patients with high or very high cardiovascular risk at the time of hypertension diagnosis in patients under the age of 55. This means that CVRF is being diagnosed late and, therefore, routine blood pressure checks and screening for other CVRF should begin sooner in patients’ lives.
Data from Brent and colleagues 15 showed that the prevalence of hypertension increased over time in individuals aged 40–59 years and 60 years or older. Among patients aged 60 years or older, hypertension awareness and treatment is relatively high, whereas the proportion of patients with hypertension treated and controlled is lower compared with those 18–39 years and 40–59 years. In this study, individuals with hypertension aged 18–39 years were more likely to attain control when treated vs. those 60 years or older. Data suggest efforts to improve blood pressure control in younger adults should focus on raising awareness and linkage to a primary care system.
In our study, we found that 28.6% of the sample showed target organ damage, primarily at the expense of kidney involvement, as 19% showed microalbuminuria. Similar percentage was found in one epidemiological study conducted in patients from primary care in Spain (20%), 16 with age 65 ± 12 years. The prevalence found in the i-Search global study 17 was 54.8%, in which the microalbuminuria was assessed using a dipstick test and the patients were enrolled by cardiologists and internists. The patients of our study have been enrolled by primary care physicians.
It should be noted that almost 100% of the patients have had the microalbuminuria test, which indicates to us that nowadays this is a routine test in the study of hypertensive patients in primary care in Spain.
Dyslipidaemia was the CVRF most associated with hypertension and was present in 80.4% of the population studied. This percentage is greater than in other studies. 14 This may be explained by our use of the criteria proposed by the 2007 European guidelines, with the proposed consideration of hyperlipidaemia at lower levels of the different lipid fractions than those of the 2003 guidelines used in other studies. Less than 40% of these patients had been treated with statins. These data suggest the need for early management of both CVRF, with a need to associate lipid-lowering drug treatments at an early stage to improve cardiovascular prognosis, as demonstrated by the ASCOT study. 18
However, the prevalence of hypertensive patients diagnosed with diabetes was lower than in other studies (13.6%), which may be justified by the age of the patients. Another significant aspect is the glycaemic disorders detected. Thus, despite the percentage of diabetes being lower than that of other studies, if we add the prevalence of abnormal fasting glucose (baseline glycaemia 100–125 mg/dl), the alteration in hydrocarbon metabolism is present in nearly four out of every 10 patients included (36.5%). This may indicate that there must be a significant number of unrecognized diabetic patients, which would coincide with the high prevalence of general and abdominal obesity that we find in the population studied. 19 This could be confirmed if routine oral glucose tolerance tests were given to the population at risk for developing diabetes. 20
The metabolic syndrome is associated with increased risk of CVD independently of age and sex. 21 We found a high prevalence of MS in the absence of known diabetes. This percentage is lower than that found in specialized units, which is around 60%, 22 but is higher than the prevalence of the MS seen in general population.21,23
It is widely recognized that general obesity means an increase in mortality, including cardiovascular, and is also associated with the addition of greater CVRF and metabolic disorders, with a direct relationship between abdominal obesity, CVD, and the development of diabetes mellitus. 24 In our study, 79.7% had a BMI >25 kg/m2, higher than that reported by the IDEA study 24 which found it to be about 50% in the general population. BMI >30 kg/m2 was found in 28.7% of our patients, which is a greater prevalence than that found in the Encuesta Nacional sobre Obesidad (‘National Survey on Obesity’) carried out in Spain in 2000, which was 21% in those over the age of 55 25 and much higher than the 11.4% found in the Spanish population between the ages of 45–54 in the work published by Gutiérrez Fisac et al. in 1994. 26 All of this shows us the constant increase in obesity in middle-aged people that is occurring in Spain, which has become much more evident over the last 10 years, according with data from other countries. 27 This fact indicates the need to propose more effective and earlier interventions in weight alteration.
Our results suggest that patients with high CVR start at an early age and we have the opportunity to diagnose them from the beginning of their contact with the healthcare system. It is important to bear in mind that routine blood pressure checks and evaluation of overall CVR may lead to early diagnosis of these patients. The lack in early diagnosis of hypertension and other CVRFs and adequate preventive management is potentially because of both structural insufficiencies of existing healthcare system and inadequate perception of risk by physician and patients. 28
We cannot fail to think that, even so, the CVR may be somewhat underestimated, given that the measurement of the damage from hypertensive cardiac repercussion, which is to say that the presence of left ventricular hypertrophy, as determined by ECG, underestimates CVR, as shown in the study by Luque et al. 29 This study stratified CVR with an adequate study of target organ damage, which found that a high percentage of recently-diagnosed or not drug-treated hypertensive patients increased their cardiovascular risk and entered into criteria for drug treatment when an echocardiogram was used to assess left ventricular hypertrophy.
As possible limitations and bias to this study, it must be considered that the cardiovascular profile of patients under the age of 55 has been drawn on a consecutive sample of patients who visit a healthcare centre for any reason, and this may differ from the real population profile if patients who do not visit medical services, a frequent occurrence among the young population, were to be included. Another limitation in the survey could be the potential for selection bias, for example, the primary care physician including only patients with readily available data. However, the broad sample attained[6815 patients of which 6788 (>99%) were valuable], the consecutive sampling of patients, and the participation of doctors and patients from all over Spain allow us to generalize the results with a significant population of hypertensive under the age of 55 looked after in primary care.
In conclusion, the data from this study show, for the first time, how patients who were recently diagnosed at an early age in our environment have a strong association with CVRF and target organ damage using the stratification proposed by the 2007 ESH/ESC guidelines. This should make us meditate on the importance of an adequate study of and approach to hypertension at young ages from the moment of diagnosis at initial contact with primary care clinics, allowing CVR to be correctly defined, overcoming its underestimation, and implementing the correct treatment with the objective of reducing CVR, in order to decrease the excess of cardiovascular morbidity and mortality.
Footnotes
Funding
This work was supported by an unrestricted grant provided by Pfizer Spain.
Conflicts of interest
None.