
Abstract
Introduction:
Caesarean scar ectopic pregnancy (CSEP) is a potentially serious complication of caesarean section (C-section) which consists of the implantation of the gestational sac (GS) in the hysterotomy scar. All women with a history of C-section are at risk for CSEP. Early diagnosis and treatment are critical to avoid maternal morbidity and mortality. There is overlap in the sonographic appearance of CSEP, low-lying normal pregnancy, cervical ectopic pregnancy and miscarriage in progress. In 2022, a standardised sonographic evaluation and reporting system for CSEP in the first trimester was published to raise awareness of this entity. We aim to provide a practical guide to the sonographer by outlining the pertinent obstetric history, imaging findings and differential diagnoses in these patients.
Case Report:
We report three cases of CSEP, diagnosed by ultrasonography in the first trimester. We also report three different conditions that may mimic CSEP. We include the clinical details, sonographic findings and patient outcomes.
Discussion:
The incidence of CSEP is suspected to be under-recognised and thus underreported. CSEP presents a substantial risk for severe maternal complications including uterine rupture, severe hemorrhage and placenta accreta spectrum disorders. This is complicated by challenges in securing an early diagnosis. When a first-trimester ultrasound reveals a GS in the lower third of the uterus, the sonographer must consider the differential diagnoses herein.
Conclusion:
We will present the recommended criteria using cases demonstrating the sonographic findings. Raising awareness of the four key sonographic markers of CSEP may improve sonographer detection rates, thus facilitating better patient management.
Keywords
Introduction
Caesarean scar ectopic pregnancy (CSEP) refers to implantation of a pregnancy in the niche from a previous C-section. CSEP can only occur when a niche is present. 1 Early diagnosis is critical due to the potentially life-threatening complications to the mother if left untreated. The true incidence of CSEP is unknown because the condition is under-recognised and under-reported. 2 The rising rates of C-section have increased the incidence of CSEP, reported at this point in time to be 1 per 1800–2000 of all pregnancies, and 1 per 531 among women who had at least one C-section. 2 Approximately 6.1% of ectopic pregnancies in women with a history of C-section are expected to be CSEP. 3
When first-trimester ultrasound reveals a gestational sac (GS) in the lower third of the uterus, the differential diagnoses include a CSEP, miscarriage in progress, low implantation of a normal pregnancy or cervical ectopic pregnancy.
The diagnosis of CSEP can be difficult, due to the lack of awareness and knowledge of sonographic findings and the low prevalence. In 2022, a standardised sonographic evaluation and reporting system for CSEP in the first trimester was published by Jordans et al. 4
We present three proven cases of CSEP, which demonstrate four diagnostic criteria, that are often used in the sonographic diagnosis of CSEP.
Making the diagnosis
The most important part: patient history
The patient history is an important part of making the diagnosis of CSEP. The clinical presentation is highly variable. Some patients are asymptomatic and are diagnosed incidentally during an early obstetric exam, while others may present with vaginal bleeding, abdominal pain or, if diagnosis is delayed, uterine rupture. The key to avoiding missed CSEP is to ask about a history of prior C-section for all first-trimester ultrasounds. 6 At the outset of every early obstetric exam, patient history recording should include gravida, para status and prior C-section or peripartum complications such as haemorrhage or a retained placenta which may suggest prior placenta accreta syndrome. If a low-lying GS is subsequently identified on ultrasound, the sonographer will have an elevated level of suspicion for this diagnosis and can assess its position in relation to the site of the previous hysterotomy.
Variability in appearance of C-section scars
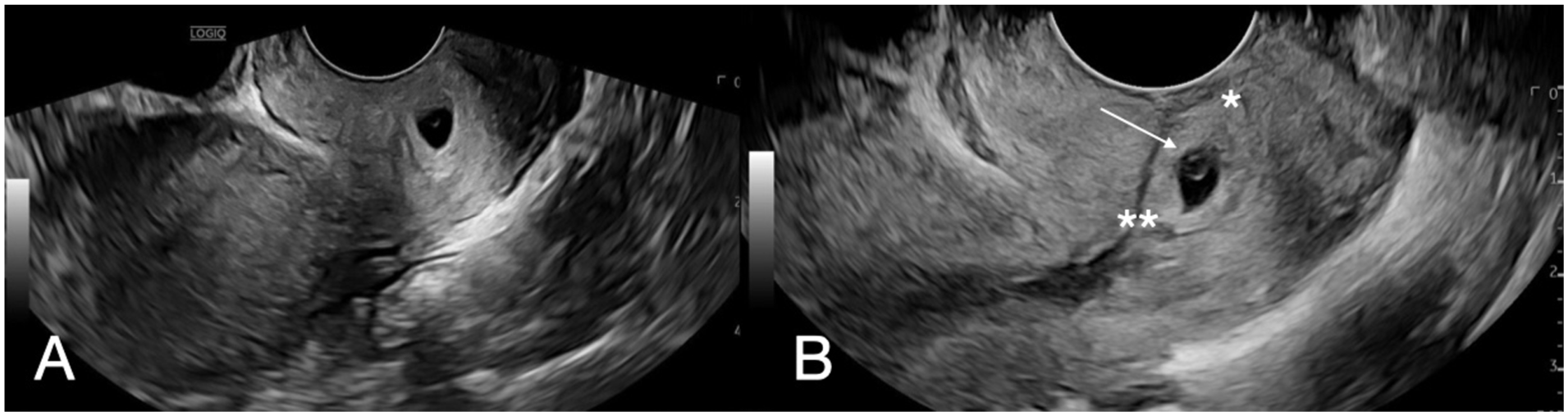
The prevalence of uterine niche after C-section is common, reported to be 49.6% by transvaginal ultrasound (TVUS) 6–12 weeks post C-section, although many become less conspicuous over time. C-section scars are often visible if the sonographer is aware of the history of C-section. The scar can have a variable appearance, sometimes subtle (as in Figure 1(a)), but occasionally there is a prominent “niche” (as in Figure 1(b)). A niche may place the patient at higher risk of a future CSEP, although most subsequent pregnancies will be entirely normal. In a normal pregnancy, the GS implants in the upper uterine cavity, well away from the caesarean scar (Figure 2(a) and (b)).
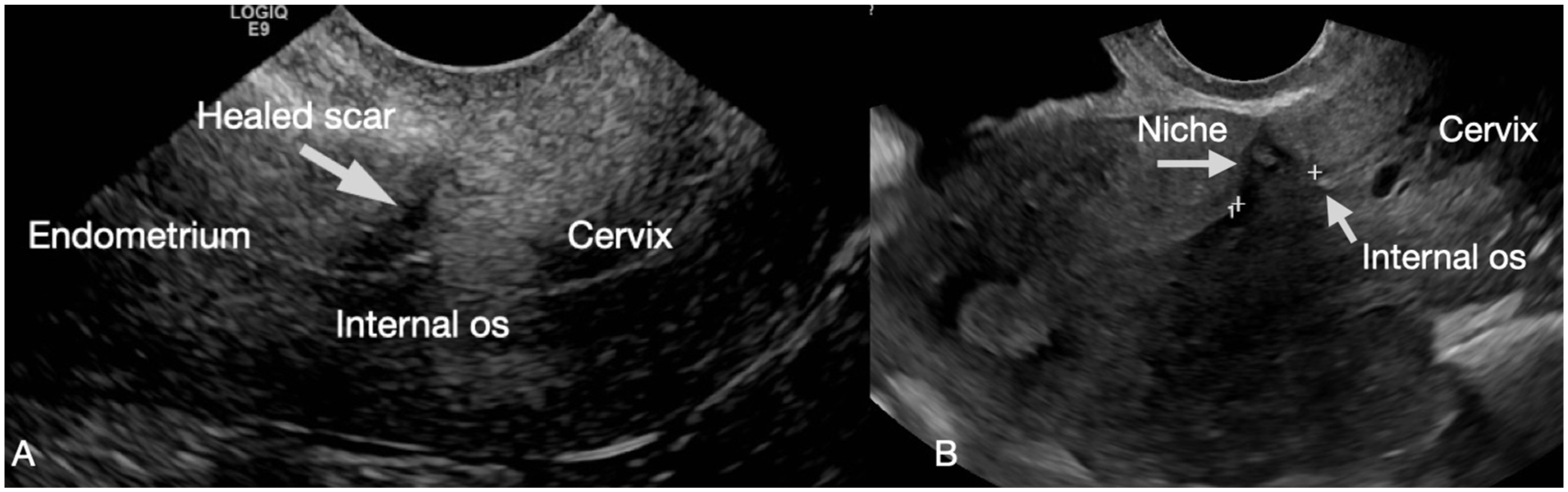
Comparison of a well-healed scar and a niche of incomplete healing in the non-gravid uterus. (a) Sagittal TVUS image of the lower uterine segment shows a well-healed C-section scar (arrow). (b) Calipers measure a 1.1-cm niche representing incomplete healing of a previous C-section.
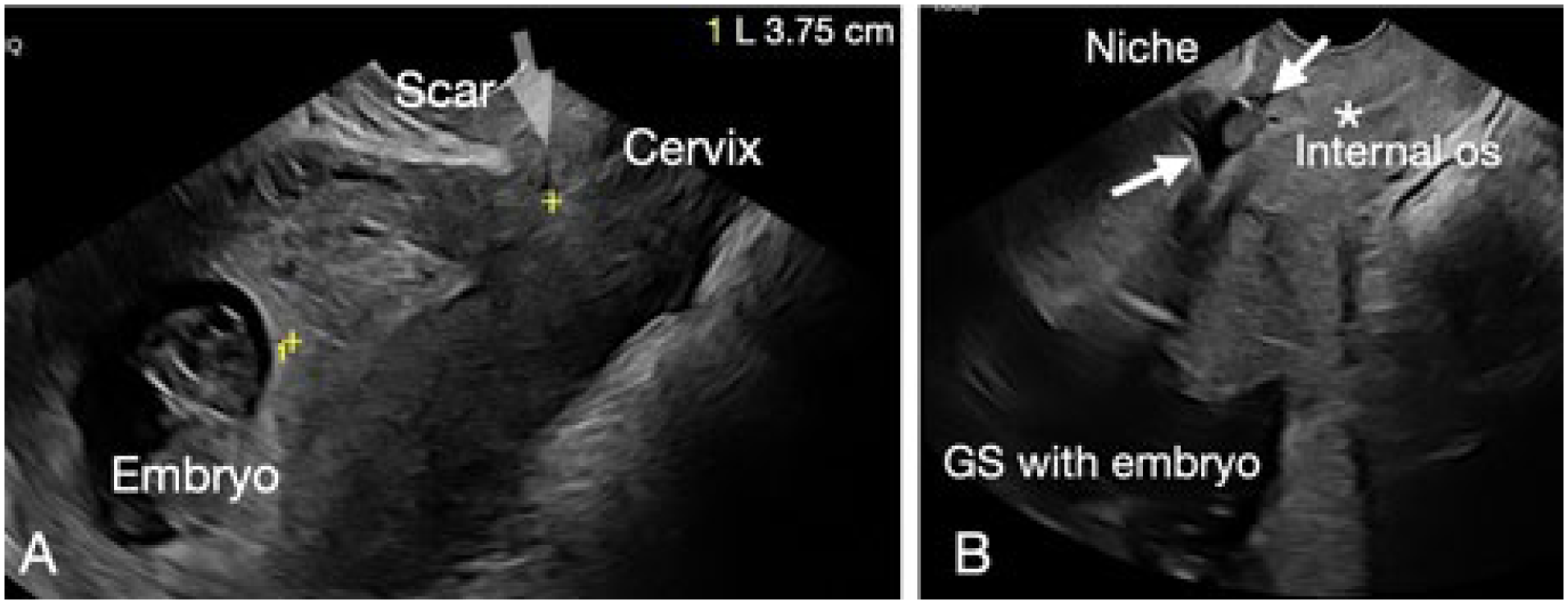
Comparison of the appearance of caesarean scar in the gravid uterus. Sagittal TVUS image at 10 weeks of gestation (a) shows a normal sac implantation high in the uterine cavity, 3.75 cm from a well-healed caesarean scar. Sagittal TVUS image at 10 weeks of gestation (b) shows a normal sac implantation high in the uterine cavity, distant from the prominent niche that persists from a prior C-section (arrows) in the anterior myometrium.
Sonographic criteria of CSEP and scanning technique
1. Abnormally low and anterior location of a GS in a patient with a history of prior C-section (Figure 3). The uterine cavity and cervical canal are both empty
A sagittal transabdominal scan (TAS) long axis image of the uterus to include the fundus and the cervix allows accurate localisation of the GS, low implantation and abnormal growth pattern. TVUS should then be offered for detailed evaluation. The sac may be triangular or round with displacement in the anterior myometrium. Images should be obtained to show its relationship to the C-section scar. The GS may distort the serosal surface of the uterus. Document the location of the GS above the internal cervical os. The upper uterus, endometrium, cervix and endocervical canal should be assessed (Figure 3).
2. Thin (or absent) myometrial layer
Assess the anterior myometrial wall, measure the residual myometrial thickness (RMT) and the normal, adjacent myometrial thickness (AMT) for comparison. Thin or absent myometrium between the GS and bladder wall is an important prognostic marker. Record mean sac diameter (MSD), yolk sac (YS), embryonic crown-rump length (CRL) and embryonic cardiac activity when present.
3. Prominent vascular pattern at or around the GS.
Assess for peritrophoblastic flow with colour Doppler, on TVUS. The presence of flow suggests viable placental tissue and helps identify the implantation site. CSEP will often appear well perfused with high velocity (peak velocity of >20 cm/s) and pulsatility index (PI) lower than 1 (Figure 3). 7
4. Negative sliding sign
This is assessed dynamically during the transvaginal portion of the scan. Gentle pressure using the TV transducer is applied on the GS. Non-displacement of the GS from its position at the scar indicates a sac adherent to or implanted within the scar. Link to video demonstrates a negative sliding sign (https://youtu.be/fC4ropWcLfU).
Sagittal TVUS image of the lower uterine segment illustrates three of the four sonographic criteria for a caesarean scar ectopic pregnancy: GS location is low and adherent to the C-section scar, above the internal cervical os (white arrow).
Technical note: After 12 weeks of gestational age (GA), these criteria may no longer apply (Table 1).
CSEP criterion, scan tips for assessment and corresponding images.
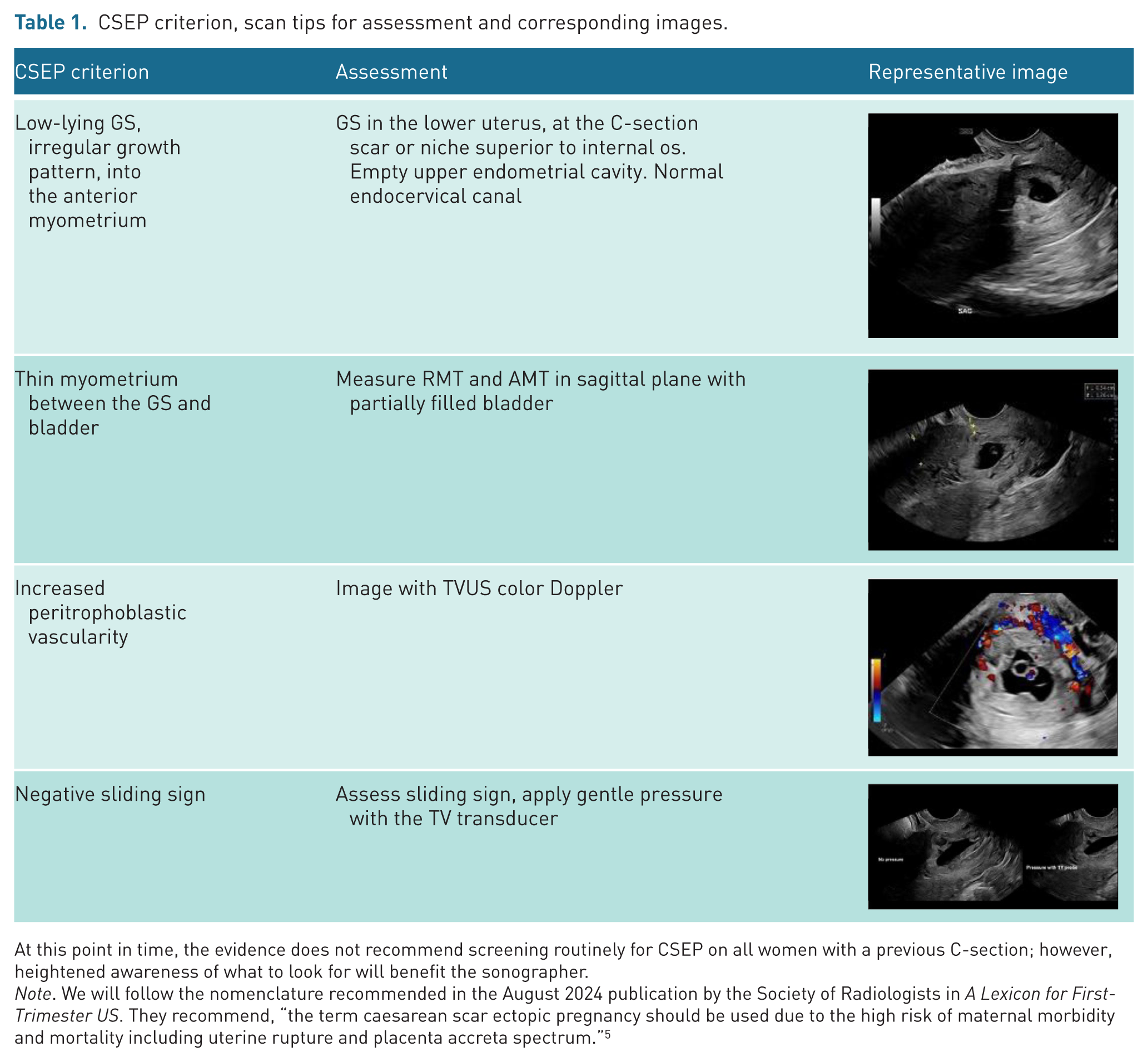
At this point in time, the evidence does not recommend screening routinely for CSEP on all women with a previous C-section; however, heightened awareness of what to look for will benefit the sonographer.
Note. We will follow the nomenclature recommended in the August 2024 publication by the Society of Radiologists in A Lexicon for First-Trimester US. They recommend, “the term caesarean scar ectopic pregnancy should be used due to the high risk of maternal morbidity and mortality including uterine rupture and placenta accreta spectrum.” 5
Case reports of three patients with CSEP
Case 1: CSEP, treated with systemic methotrexate
This patient presented at 7 weeks 0 days (7w0d) with vaginal bleeding and pelvic pain. Her beta human chorionic gonadotropin (β-hCG) was 1092; she has a history of G3P2 with two previous caesarean deliveries. The upper uterine cavity was empty. On the TAS and TVUS exams, the GS appeared very low in the uterus, near the caesarean scar (Figure 4). It was triangular and eccentric from the endometrial cavity, projecting into the anterior myometrium with very thin RMT. The GS was filled with low-level echoes; it contained an embryo, measuring 6 weeks 5 days (6w5d) (Figure 5). No embryonic cardiac activity was evident. The appearance was consistent with CSEP despite the absence of peritrophoblastic vascularity, which may indicate that this pregnancy was failing. The patient was administered intramuscular methotrexate (IM), resulting in the resolution of ectopic pregnancy and passage of tissue 1 week later, as seen on follow-up exam.
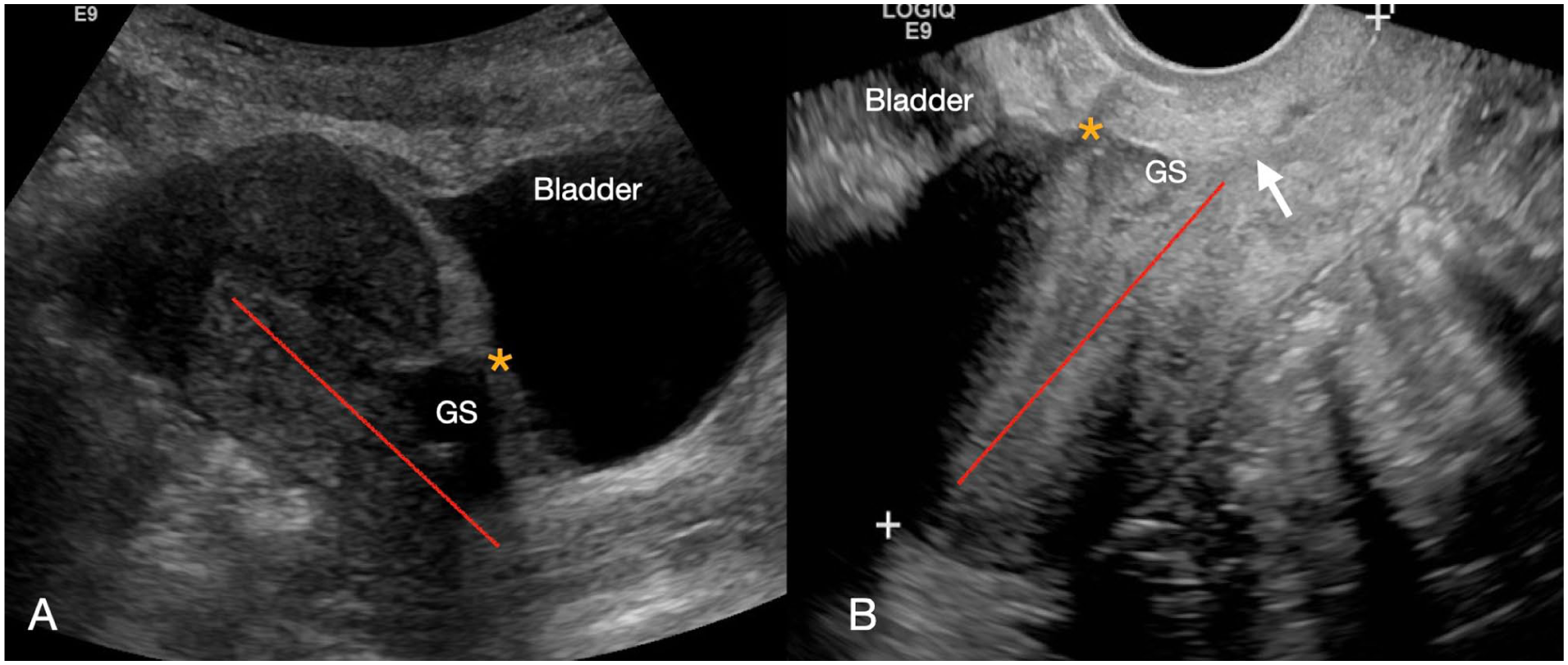
Sagittal TAS image (a) demonstrates the GS in the anterior myometrium of the lower uterine segment. The endometrial stripe (red line) demonstrates the location of the GS implanting beyond the endometrial cavity. The endometrial cavity in the upper uterus is empty. The GS distorts the serosal surface of the uterus toward the bladder (*). In this case, there was effectively no residual overlying myometrial mantle. Sagittal TVUS image (b) confirms the TAS findings; the GS is not contained within the endometrium (red line). The RMT is redemonstrated (*), although the interface with the bladder is harder to recognise with the bladder empty. The location of the GS above the internal cervical os is better visualised (arrow).
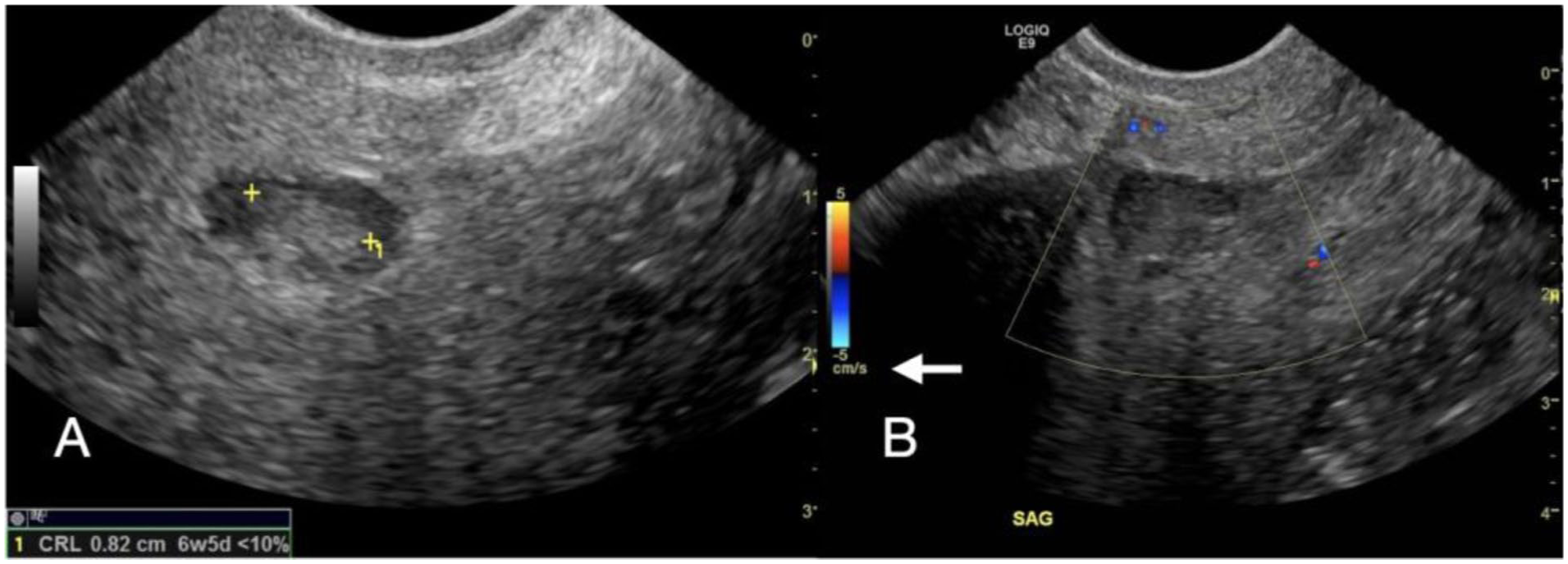
(Same patient as Figure 4). The sagittal TVUS image shows debris in the GS (a) and absence of vascularity at or around the GS (b). The lack of flow suggests the pregnancy has likely stopped developing and may imply a lower risk of haemorrhage, although other parameters will also be considered by the clinical team.
Case 2: CSEP treated with systemic methotrexate
This patient was G2P1 with a history of one previous C-section (Figure 6), presented with painless bleeding, at 8 weeks of gestation by dates and β-hCG levels. On TAS, the upper endometrial cavity was empty. On TVUS, a GS containing a YS and GS was seen protruding into the anterior uterine wall at the location of the previous C-section scar. There was a very small embryo. No embryonic cardiac activity was present. The patient was successfully treated with systemic methotrexate. She had a normal pregnancy 1 year later, delivered by C-section. The delivering obstetrician noted the “paper thin” myometrium at the previous C-section site.
Sagittal TAS image shows an empty endometrial cavity (a). The GS in the lower uterine segment is difficult to appreciate. On TVUS (b), the GS is seen protruding outward, perpendicular to the endometrial cavity. The RMT is much thinner than AMT. This conveys a higher risk of uterine rupture. These measurements are best obtained with at least some urine in the bladder.
Case 3: CSEP requiring surgery
A 41-year-old G3P1 patient presented with vaginal bleeding and mild pain in early pregnancy. She had a previous therapeutic abortion (D&C) in her first pregnancy, cervical cerclage with C-section in her second, and a cervical loop electrosurgical excision procedure (LEEP) prior to the current pregnancy. On TAS and TVUS, the GS appeared low-lying, close to the scar from her previous C-section. Embryonic cardiac activity was present; GA was estimated at 6 weeks. This case well demonstrates the four sonographic criteria mentioned earlier in the diagnosis of CSEP.
Sac location and growth pattern
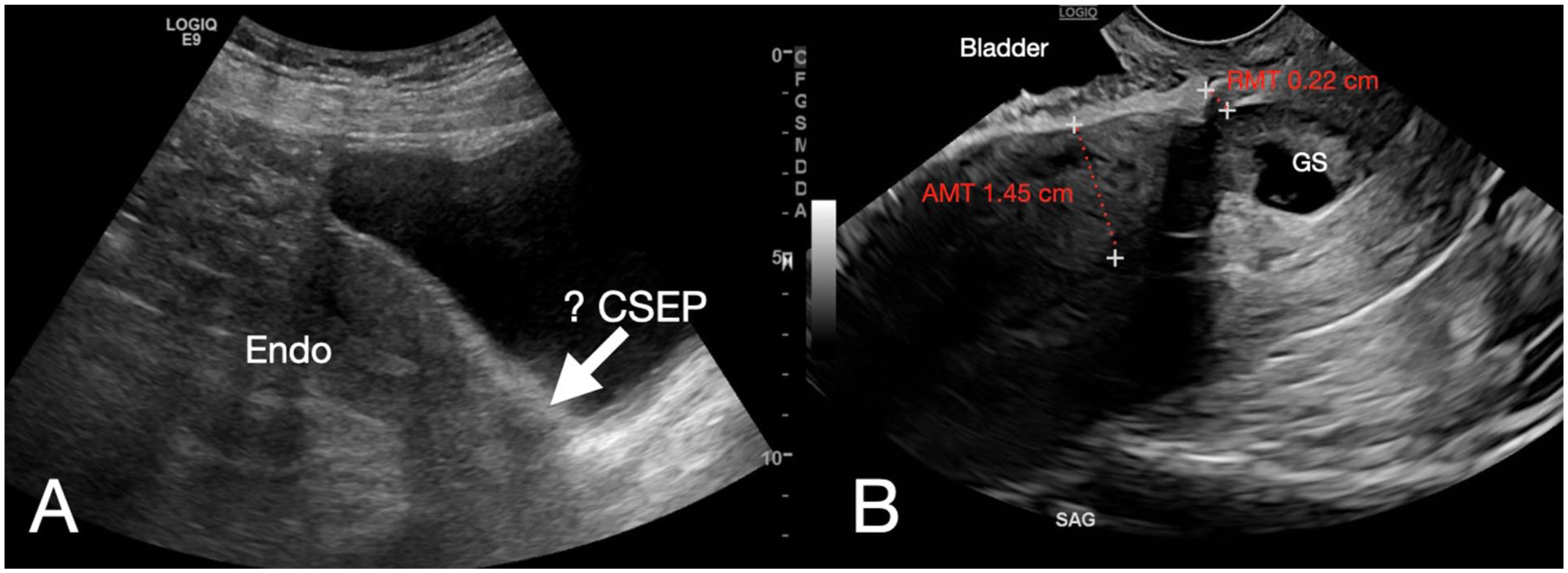
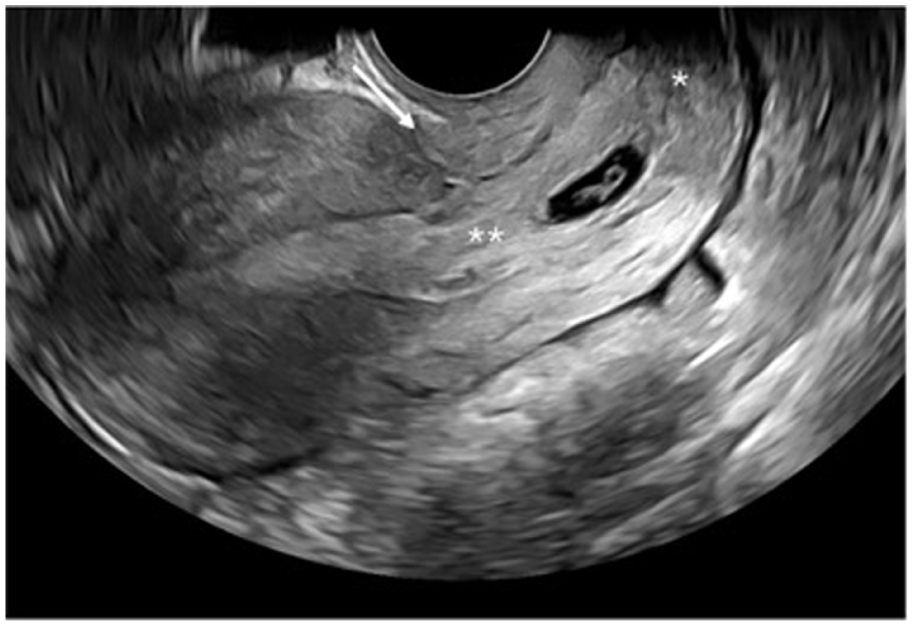
On TAS (Figure 7(a)), the upper endometrial cavity was empty and the GS was low, although it was difficult to visualise in its entirety. This could have been mistaken for a miscarriage in progress. TVUS provided better delineation of the relationship to the C-section scar. The TVUS (Figure 7(b)) demonstrated a distinct triangular-shaped GS, with echogenic trophoblastic tissue implanted in the scar site of the anterior myometrium and confirmed the location above the internal os.
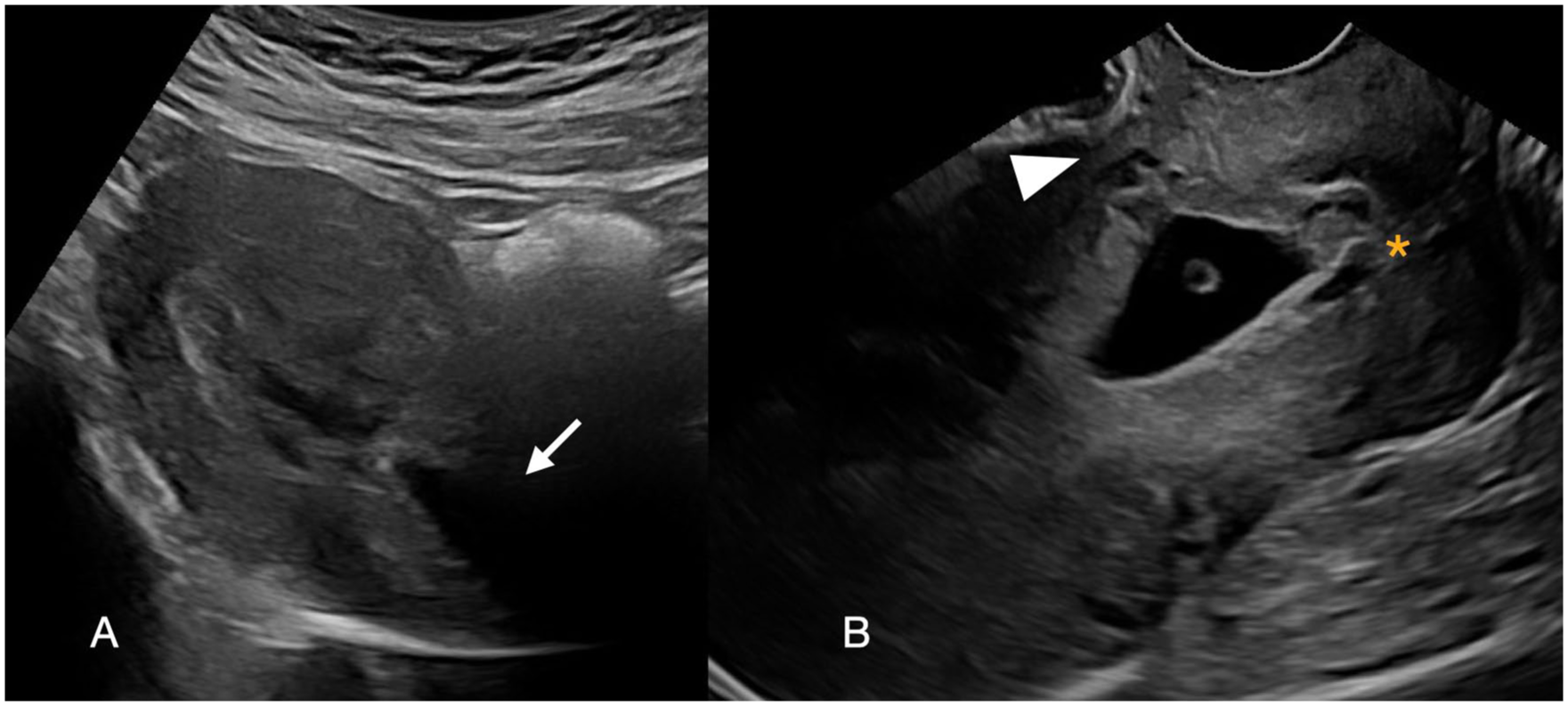
TAS image (a) demonstrated a low-lying GS which was difficult to see in its entirety. TVUS image (b) more clearly shows the low location of the GS but above the internal cervical os (*). The tethering of the sac into the C-section scar results in a triangular appearance to the GS. The residual myometrium is thin (arrowhead).
Measurements
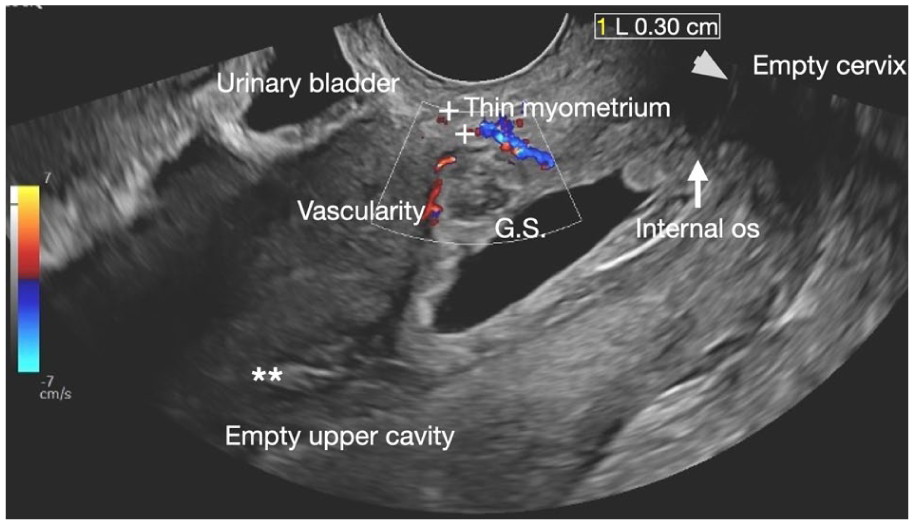
The RMT measured 0.34 cm, and the AMT measured 1.26 cm (Figure 8). This TVUS image shows the correct caliper placement when measuring the myometrium.
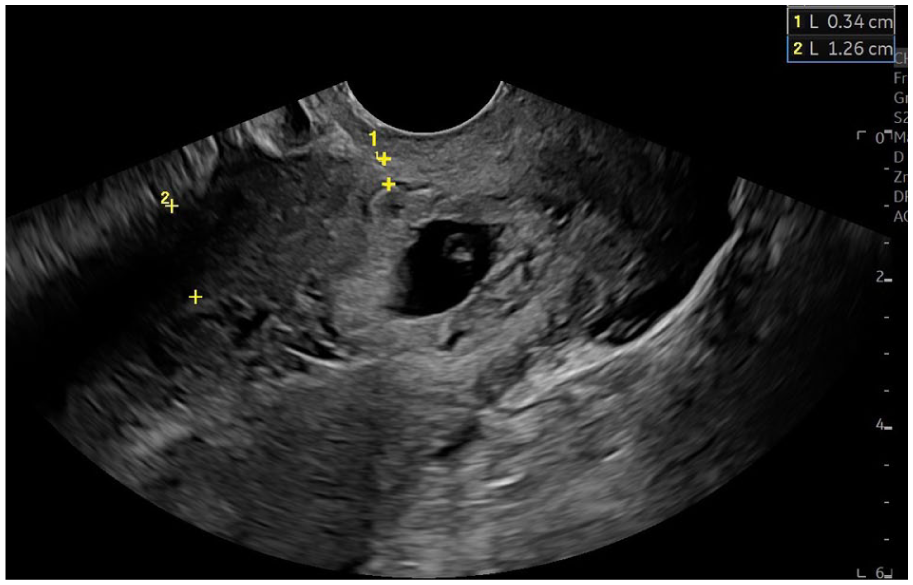
Same patient. This shows the thin myometrial layer over the pregnancy. Note the caliper placement to compare the residual myometrial thickness (RMT 0.34 cm) to the normal adjacent anterior myometrial thickness (AMT 1.26 cm).
Vascularity
There was vascularity seen surrounding the GS (Figure 9) imaged here at the initial scan at 6 weeks 0 days (6w0d) and a subsequent scan at 7 weeks 1 day (7w1d). This suggests the tissue was still viable with a higher risk of treatment failure and haemorrhage (contrasted with Case 1 in Figure 5). Link to video demonstrates the increase peritrophoblastic vascularity on the scan at 6 weeks (https://youtu.be/0j0TWSa7BSY).
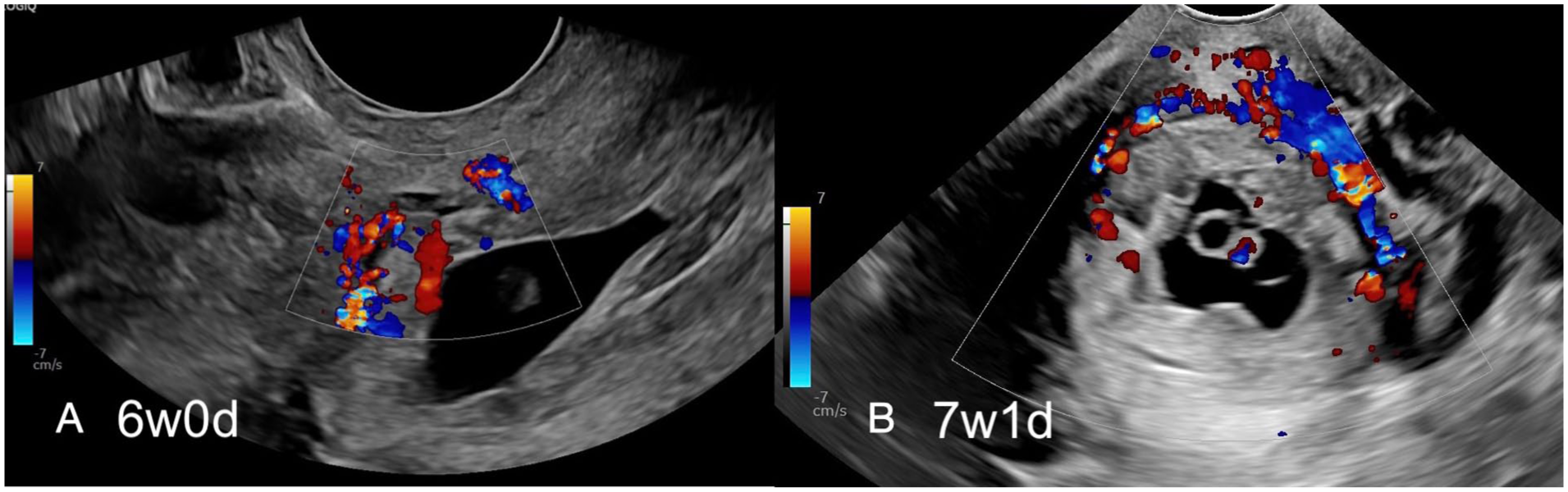
Same patient. Sagittal TVUS image at 6 weeks of gestation (a) with increased peritrophoblastic vascularity seen around the GS, suggesting active trophoblastic tissue. Eight days later (b), the GS is now larger and demonstrates persistent vascularity. The relationship of the GS to the C-section scar became more challenging to identify as the pregnancy continued, showing the benefit of early diagnosis.
Sliding sign
To confirm the diagnosis of CSEP and exclude low-lying pregnancy or miscarriage in transit, gentle pressure was applied with the TV transducer. The gestational sac did not move; it was adherent to the C-section scar, a so-called “negative” sliding sign, most in keeping with CSEP. Link to video demonstrates non-displacement of the GS from the caesarean scar niche (https://youtu.be/2snQbemoI1M).
The patient was initially treated with systemic IM. Local methotrexate injection (+/− KCL) directly into the GS is typically reserved for viable CSEP with embryonic cardiac activity and may be available in centres with interventional expertise.
Initial follow-up ultrasound indicated growth of the GS in keeping with treatment failure. She underwent a second treatment with systemic methotrexate and inpatient observation but discharged herself against medical advice. The patient presented acutely 6 days later to another institution with heavy vaginal bleeding, haemodynamic instability and a drop in haemoglobin. She required three units of blood and definitive surgical management, consisting of dilation and gentle suction. Her β-hCG was then followed to zero.
Differential diagnoses
There are three differential diagnoses that need to be considered and excluded before definitively diagnosing a CSEP:
Miscarriage in progress.
Low implantation of a normal pregnancy.
Cervical ectopic pregnancy.
The site of trophoblastic implantation and vascularity can assist in discriminating between these.
Miscarriage in progress
This is the most likely diagnosis when a GS is in the lower uterine segment or endocervical canal. The pregnancy has failed and is in the process of expulsion. Presenting symptoms include vaginal bleeding and pain. The GS is centrally located within the endometrial cavity, equidistant from the anterior and posterior uterine wall (Figure 10). The myometrium immediately anterior to the sac appears of normal thickness, and the pregnancy does not distort the outer contour of the uterus. Sliding sign may be helpful, as the GS is not adherent to the wall, so it may move independently with transducer pressure, a positive sliding sign. There typically is no increased peritrophoblastic vascularity on colour Doppler because the trophoblastic tissue is no longer viable. The sac may appear deformed and disorganised. The cervix may be open or closed depending on whether some contents have passed through. If there is uncertainty, repeating the study after several hours can show a change in location or complete expulsion of the pregnancy.
Sagittal TVUS image of a miscarriage in progress.
Low implantation of a normal pregnancy
A low-lying GS can also occur in a pregnancy implanted in the lower uterine segment close to but not involving the C-section scar. Ultrasound findings that support a low implantation of a normal pregnancy include a GS within the endometrial cavity, above the internal cervical os, with decidual reaction, +/− YS and embryo. Peripheral hypervascularity indicates trophoblastic tissue is implanted and viable (although colour flow is not routinely performed in the first trimester of a normal pregnancy).
Figure 11 is an example of a normal pregnancy measuring 6 weeks 3 days (6w3d) with embryonic cardiac activity, implanted in the lower third of the uterus. This patient had a history of a previous C-section, although the scar is not readily apparent. Note the oval-shaped GS lying parallel to the endometrium. The GS does not protrude into the myometrium, and the overlying myometrial thickness is normal. In contrast, the GS of a CSEP or cervical ectopic pregnancy is often oriented perpendicular to the endometrium due to tethering. Close follow-up is recommended, as the GS may move superiorly toward the fundus with expected embryo development.
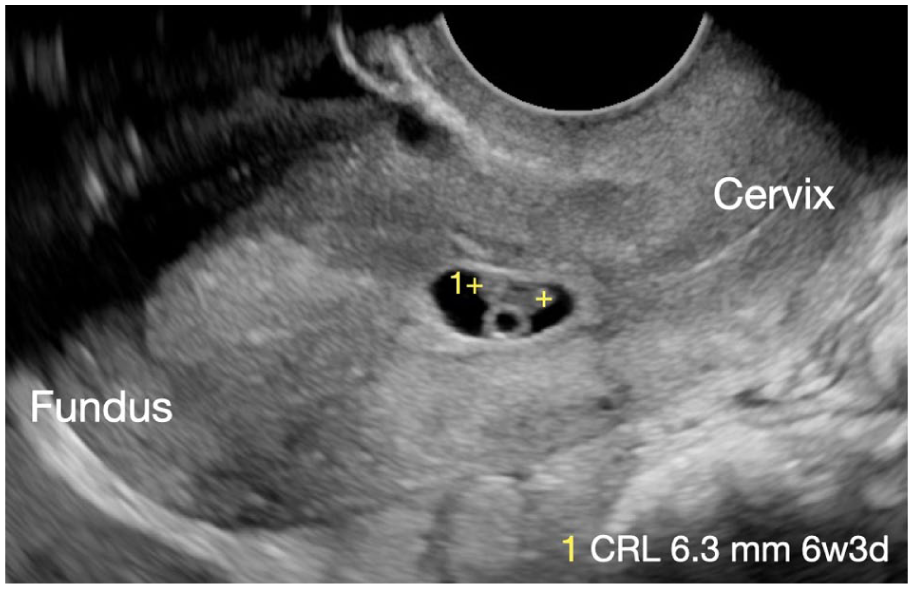
Sagittal TVUS of a normal, albeit low-lying pregnancy at 6w3d in a patient with a history of a previous C-section.
Cervical ectopic pregnancy
This is a rare diagnosis; a history of previous surgery to the uterus or cervix is known to increase the risk. Differentiation from CSEP is important, as the management is different. The GS in cervical ectopic pregnancy is implanted lower than a CSEP, below the internal os, within the endocervical canal rather than the endometrial cavity Figure 12. The internal cervical os is closed which can result in an hourglass shape of the GS. There is likely peripheral hypervascularity on Doppler if the trophoblastic tissue remains implanted and viable. Because it has implanted, the GS will not slide (negative sliding sign), although this should be performed with caution so as not to precipitate bleeding.
Sagittal TVUS image (a) with a close-up view (b) of a cervical ectopic pregnancy.
Discussion
CSEP is defined as implantation within the scar of a previous C-section. In a normal implantation, the superficial layer of endometrium becomes circumferentially decidualised throughout the uterus. The decidua protects the myometrial layer of the uterus from the actively invading trophoblastic cells and the placenta. A C-section scar reflects a focal area of discontinuity or thinning of the myometrium, making it more vulnerable to invading trophoblastic cells. A prominent niche increases this risk further.
As C-section rates are increasing worldwide, the collective index of suspicion for CSEP needs to be commensurate for this potential complication. Early diagnosis of CSEP is desirable as the sonographic findings at 6–7 weeks of gestation are easier to recognise than later in the first trimester. Early diagnosis allows for multiple therapeutic interventions and can lead to successful management, with 70% of women preserving fertility after treatment. 8 A reported seven out of eight pregnancies where the implantation is very close to or in the niche will undergo spontaneous abortion in the first trimester due to the reduced blood supply. 8
Definitive treatment recommendations in a CSEP, which does not spontaneously abort, are not firmly established. A large study published in 2024 stated that in more than 90% of cases, management with either suction evacuation, balloon treatment or surgical excision was successful. 9 Intra-sac treatment with methotrexate (+/− KCL) or systemic methotrexate in combination with surgical intervention may be needed. 10 The effectiveness of all treatments decreased with GA. 9
Although we have focused on first-trimester ultrasound, if the pregnancy continues into the second trimester, the diagnosis becomes harder to establish with ultrasound. As the GS becomes rounder and enlarges, it may extend into the upper endometrial cavity, making diagnosis more difficult.
The consequences of a missed diagnosis and delayed treatment are serious and can be life-threatening including uncontrolled haemorrhage (from placenta previa and placenta accreta spectrum disorders) and uterine rupture. Histologically, CSEP and placenta accreta spectrum share common findings. Pathologists report the myometrial or scar tissue is invaded by placental villi with scant or no intervening decidua. 11 The difference in their clinical presentation is thought to be due to the different gestational ages at which symptoms appear and are treated. 11
Any effort to learn the four key sonographic findings of CSEP and apply them could help prevent complications in the second and third trimesters. Recently, Timor-Tristch et al. 12 published a new classification system that proposes a change in the terminology of pregnancies after caesarean deliveries.
Three differential diagnoses must be considered before definitively diagnosing a C-section ectopic pregnancy, one of which is a normal pregnancy, and therefore, care must be taken not to cause harm. Treatments for a miscarriage in transit and a cervical ectopic pregnancy are different from CSEP, and these conditions need to be differentiated.
Conclusion
CSEP is a “do-not-miss diagnosis” due to the serious consequences of delayed treatment. With the global increase in caesarean deliveries, the incidence is increasing. The most important question a sonographer can ask prior to a first-trimester scan is the patient’s obstetric and surgical history, specifically the history of a previous C-section. When TAS or TVUS reveals a low-lying GS, in the anterior myometrium, the patient history should alert the sonographer to consider CSEP. A careful assessment of the relationship of the pregnancy with the C-section scar, the internal cervical os, the residual myometrial thickness, surrounding vascularity and sliding sign will have an important role in making a confident diagnosis and prognostication of risk.
We hope that the criteria described here will aid sonographers in obtaining ultrasound images that are indicative of CSEP, allowing early diagnosis.
There are no underlying research materials related to this paper.
Supplemental Material
sj-docx-1-ult-10.1177_1742271X261444869 – Supplemental material for Sonographic evaluation of low-lying gestational sac in the first trimester: A sonographer’s guide to identify caesarean scar ectopic pregnancy
Supplemental material, sj-docx-1-ult-10.1177_1742271X261444869 for Sonographic evaluation of low-lying gestational sac in the first trimester: A sonographer’s guide to identify caesarean scar ectopic pregnancy by Karen Letourneau, Amandeep Dusanj and Sarah Barrett in Ultrasound
Footnotes
Acknowledgements
The authors acknowledge Dr Susanne Johnson FRCOG, Southampton UK and Dr Michael Gregory Kozoriz FRCPC, Duncan Canada for their assistance and guidance on this topic.
Ethics
We were approved in a Statement of Waiver on March 5, 2025, by Island Health Research Ethics Board, Queen Alexandra Centre, Room 205, 2400 Arbutus Road, Victoria, BC, V8N 1V7. The letter has been uploaded with our submission.
Contributors
KL contributed to the conceptualization, investigation, writing the original draft, review and editing, data curation, ethics coordination, facility approval, project administration, image acquisition and submission process. AD contributed to the review and editing and original draft of the quiz. SB contributed to the review and editing, data curation, ethics coordination, investigation, supervision of the content and image interpretation, critical revision and guidance for accuracy of intellectual content.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research authorship and/or publication of this article.
Guarantor
Karen Letourneau.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Yes, signed consent from all patients has been obtained for publishing their sonographic images and brief medical histories. All images have been anonymized.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
Yes, although not applicable in this article, no photos have been used, only sonographic images.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.