
Abstract
Introduction
Type 2 diabetes is a chronic health condition that requires ongoing self-management. This often includes changes in diet, which may be open to influences from relatives. Family support in terms of diet may be linked with gender and the assumption that meal preparation is a traditionally female activity. This article looks at the role of gender in diet management in people with type 2 diabetes and their relatives.
Methods
Seventeen semi-structured interviews were conducted with 23 participants (10 people with type 2 diabetes, 13 relatives of people with type 2 diabetes) in Scotland, UK. The aim was to uncover changes people have made to their diet following diagnosis of type 2 diabetes in oneself or a family member. Data were analysed using Framework Approach.
Discussion
The study findings have implications for family-based interventions as gender may play a crucial role in the management of type 2 diabetes.
Introduction
Type 2 diabetes is a chronic health condition that requires ongoing self-management in order to minimise negative health consequences such as developing comorbidities. 1 People with type 2 diabetes are advised to monitor their diet in order to maintain certain blood glucose levels. 2 A ‘healthy and balanced’ diet that is rich in fibre and low in salt and sugar is recommended. 2 Diabetes self-management can be facilitated by relatives and partners who can provide advice and support, and assist with daily activities.3,4 This is particularly relevant to diet management, which as a shared activity, may be more open to influences from family members than other behaviours.4,5 However, family support in terms of diet may be linked with gender and the assumption that meal preparation is a traditionally female activity.6,7 This may be particularly relevant to middle-aged and older women who are less likely to rely on spouses with everyday activities. 8 Previous research in diabetes suggests specific gender differences in relation to diet management. For example, Maclean 9 found that married men with type 1 diabetes were at ‘an advantage’ because in almost all cases of their sample the wives prepared meals, which conformed to the prescribed diet. Women with type 1 diabetes in Maclean’s 9 study, however, often had to balance their personal needs with the food needs of their family. More recent research shows a similar pattern. A systematic review by Li et al. 10 found that women with type 2 diabetes often prioritise the needs of their family and adopt multicare giving responsibilities. They often subjugate their own needs for the needs of their family members and cook separate meals for themselves. 11 As a result, women show low dependence on their spouses and do not identify their spouse as a source of support.10–12 On the other hand, men with type 2 diabetes are more likely to be dependent on their spouses in relation to diet management and identify their wife as a main source of support.11,12 This is particularly problematic in respect to morbidity and mortality: women with type 2 diabetes are at increased risk of death from cardiovascular disease and stroke, compared to men.13,14 In addition, women with caregiving responsibilities may experience higher levels of perceived burden which can lead to poor physical and mental health. 15 Traditional gender role orientation in relation to diet management may be particularly prominent in certain cultures. For example, in a Mexican sample, women were viewed as ‘food preparers’ so they took the responsibility for managing a patient’s diet. 16 Similarly, a qualitative study conducted in Pakistan showed that men view diet change as a matter for wives whose job it is to prepare the right food. 17 In an African American sample, traditional gender roles extended to daughters, who were the main providers of diabetes-related care, including diet management. 18
In the UK, there has been a decline in traditional gender role perceptions with 72% of respondents in 2019 disagreeing that women should be viewed as homemakers. 19 However, there is still a gap in understanding how gender plays a role in diet management following diagnosis of type 2 diabetes in oneself or a family member. In addition, the majority of previous research has explored this from the perspective of the person with type 2 diabetes. The experiences of family members and the role gender plays in providing support for someone with type 2 diabetes are seldom the focus of research. A better understanding of traditional gender roles in diet management can provide insight into ways to improve self-care in patients and provide support for relatives.
The objective of this article is to describe the role of gender in diet management in response to a recent diagnosis of type 2 diabetes. The study builds on previous research by presenting the views of both patients with type 2 diabetes and relatives of such patients.
Methods
Ethical approval for this study was granted by the University of Stirling, School of Health Sciences ethics committee (SREC 15/16, Paper No. 37, version 1).
This was a qualitative study, conducted in Scotland (UK), which explored the way people respond to and cope with diagnosis of type 2 diabetes in oneself or in a family member. The aim was to interview people who had recently been diagnosed with type 2 diabetes and at least one of their non-diabetic family members in order to uncover people’s shared experiences of diabetes. A recent diagnosis in oneself or a family member decreased the risk of recall bias and optimised the chance of participants recollecting specific changes that occurred as a result of the diagnosis. This article presents the findings related to diet management.
Recruitment
Recruitment was carried out through community outreach in Forth Valley, Scotland. Posters and flyers, explaining the study, were distributed at 109 community locations, such as community centres, libraries, charity shops, bowling clubs, golf clubs, local post office branches and the University of Stirling. In addition, Diabetes UK advertised the study on their website, newsletter and social media pages. The study was also advertised by word of mouth.
People who expressed interest were screened for eligibility on the basis of the following criteria: (1) over the age of 18 years; (2) able to speak and write in English; (3) a recent diagnosis of type 2 diabetes in oneself or a family member. As type 2 diabetes is a chronic condition, people’s perception of what constitutes a recent diagnosis may differ so a specific timeframe was not used. If a participant was eligible to take part, they were asked to nominate one non-diabetic family member who might be willing to take part in the study (or nominate the relative with diabetes if it was the family member who got in touch). The participant was then asked to provide their family member with the study flyer and the researcher’s contact details.
Data collection
Semi-structured face to face or phone interviews were conducted with people with type 2 diabetes and relatives of people with type 2 diabetes. First, participants completed a brief questionnaire that collected information about duration of type 2 diabetes, route to diagnosis, relationship with the person with type 2 diabetes (for relatives), gender, age, highest education, employment status, relationship status and postcode to enable calculation of the Scottish Index of Multiple Deprivation (SIMD) or full address if the participant wanted to receive information about study findings. The SIMD is used to identify areas of multiple deprivation in Scotland by ranking small areas from most deprived (ranked 1) to least deprived (ranked 10) 20 The interview aimed to uncover changes in participants’ lives since the diagnosis of type 2 diabetes in themselves or in a family member. The topic areas included psychological changes in perceptions of diabetes severity and risk of complications (or developing type 2 diabetes in relatives), behaviour changes in relation to physical activity, diet and responsibilities, communication about type 2 diabetes and suggestions for diabetes service improvements and intervention design. Example questions in relation to diet included: ‘What changes in relation to diet have you made since the diagnosis?’, ‘What barriers have you experienced?’, ‘Tell me more about your family and what they do in relation to your diet?’. The interviews were semi-structured so questions varied depending on the participant’s response. Probes included: ‘How easy was it to change your diet?’, ‘Do you and your partner do anything differently together?’,‘Have your responsibilities in the house changed?’.
An important consideration for the study was whether to interview members of the same family together or separately. Joint interviews are useful when the interviews seek to explore the way people collectively cope with illness. Individual interviews are useful when each individual’s perspective is sought. Although the initial aim was to interview people together, not all participants could agree on a suitable time, so some members of the same family were interviewed separately. In some cases, the interviews also included only one member of a family as other family members did not agree to take part. The decision not to exclude people whose family members were unable to take part was influenced by three reasons: (1) the study did not aim to explore discrepancies in the views of men and women from the same family; (2) to reduce the risk of coercion from family members who want to take part and (3) practical considerations, such as time and money, as this study was part of a PhD project. Although a family interview would shed light into the way people interact when talking about diet management, individual perspectives are important as in some cases people may be more open if family members are not present.
The interviews were conducted by a female researcher with training and experience in collecting qualitative data (EDD). Data collection continued until data saturation was reached. We conceptualised data saturation in terms of the study target group and quality and quantity of information. The study participants represented a group with specific characteristics (i.e. recent diagnosis of type 2 diabetes in oneself or a family member, living in the UK). Participants openly talked about their experience, which enabled the researcher to gain sufficient information and notice similarities (or differences) in experiences throughout the data collection process. In order to avoid data redundancy, saturation was deemed to have been achieved when no new data emerged.
Data analysis
The interviews were audio-recorded, transcribed verbatim and checked against the recordings for accuracy. All information was anonymised and participants were given study numbers. The file linking the study numbers with participants’ details was kept separately from the recordings and transcripts. Data were analysed using Framework Approach, which is based on the assumption that the researcher stays close to the original data in order to ‘capture, portray and explain the social worlds of the people under study’ (p. 279). 21 This approach was chosen because it is better adapted to research that has specific questions and a priori issues that need to be explored and as it helps to facilitate case analysis. In addition, it provides systematic and clear stages to the analytic process, thus allowing people to see the stages, by which the results are obtained. 22 This transparency ensures trustworthiness of data, especially in terms of credibility and confirmability. In addition, having a clear process increases study transferability and dependability making it easier for others to explore the consistency of findings and compare them to other contexts and conditions. Analysis followed the data analysis stages, suggested by Spencer et al. ., 21 which include familiarisation, constructing an initial framework, indexing and sorting, reviewing data extracts, data summaries, developing categories, mapping linkages and providing explanations and interpretations. The interview questions were initially used to guide data analysis. During the developing categories stage, while detecting elements initial themes had in common, it became apparent that participants’ responses in relation to diet management appeared to differ between men and women. This enabled the identification of the themes presented in this article. Analysis was conducted by the primary author. Another author with extensive experience in qualitative research (VS) reviewed the data analysis stages to ensure that the final themes emerged from the data.
Findings
Forty-two people showed interest in the study (22 people with type 2 diabetes, 20 relatives). Twenty-three participants took part in 17 semi-structured interviews. Sample characteristics are presented in Table 1.
Participants’ characteristics.
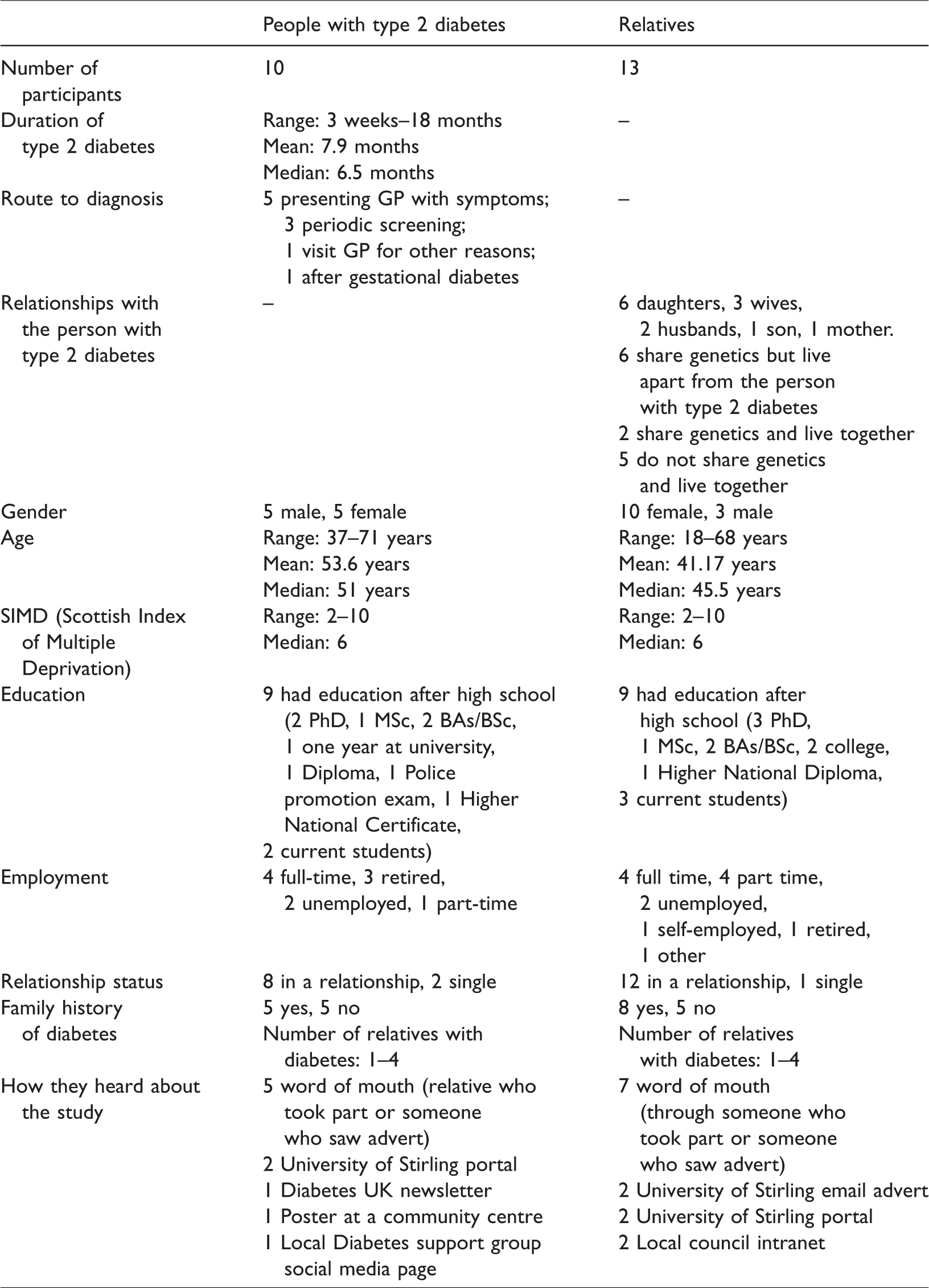
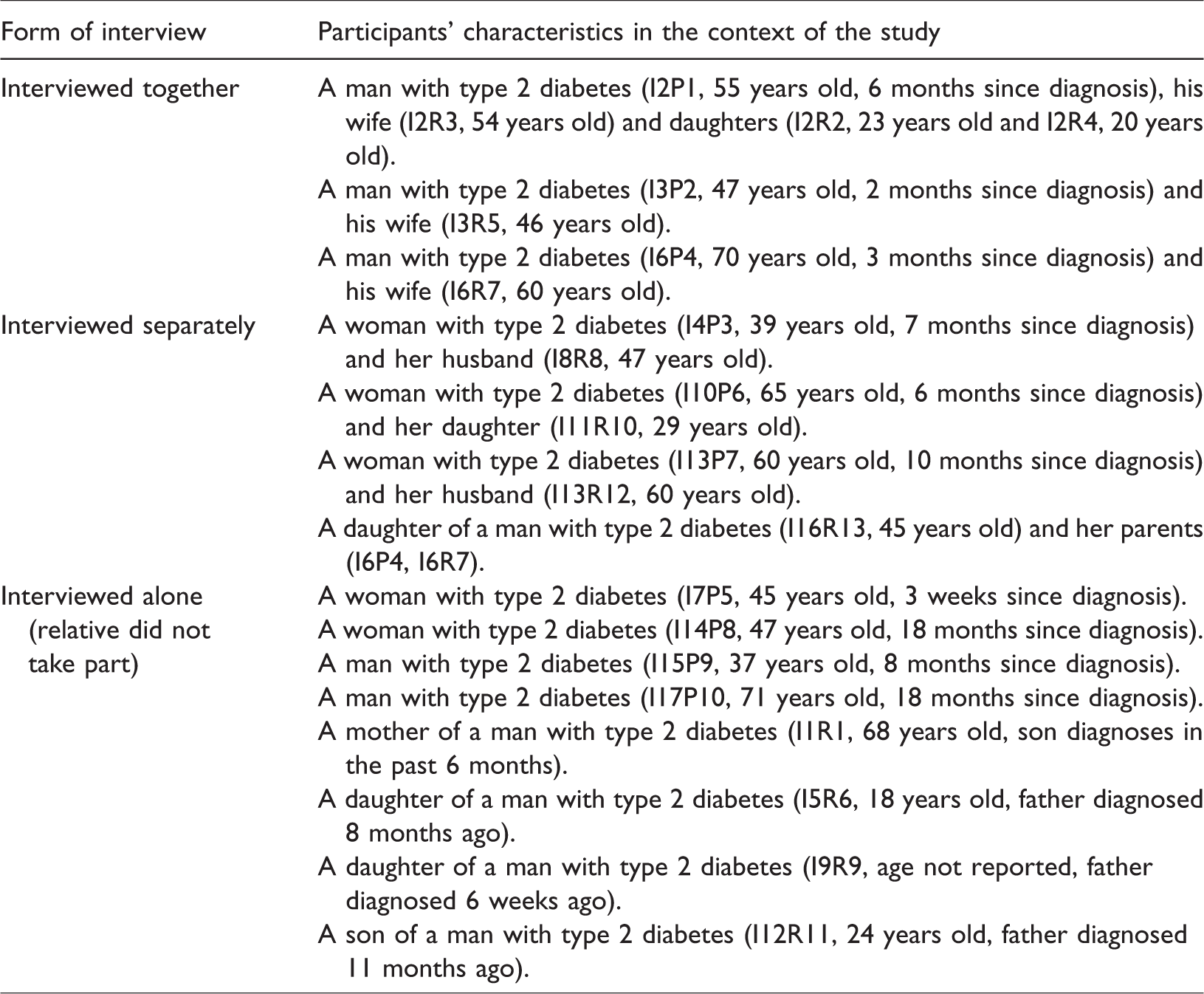
Thirteen of the interviews were individual and four included the person with type 2 diabetes and their relative(s). Ten were people with type 2 diabetes and 13 were relatives of people with type 2 diabetes. Relationships included two families (father, mother, two daughters; father, mother, daughter); a mother-daughter dyad; and three couples. The remainder were either a person with type 2 diabetes or a relative whose family members were unable to take part. Details about the relationships between participants and how they were interviewed are presented in Table 2.
Participants and form of interview.
Interviews were conducted between November 2015 and March 2016 and took place in participants’ homes (N = 6), private rooms at University of Stirling (N = 6), a local hotel (N = 1), a local library (N = 1) and a private office at a participant’s workplace (N = 1), and over the phone with the researcher in a private room (N = 2). Interviews lasted between 25 and 85 min. Participants were given £10 as reimbursement for participation.
Data analysis yielded two themes addressed by both people with type 2 diabetes and their relatives: Women – taking responsibility for diet management, and Men –‘going along’ with the new diet.
Women – Taking responsibility for diet management
Virtually all relatives of people with type 2 diabetes talked about supporting diabetes self-management. However, compared to men, women more often talked about a desire to manage the person’s condition, take an active role in trying to prescribe a specific diet regimen and ensure the person with type 2 diabetes adheres to it: ‘The female always has a bit of a problem because they usually stereotypically are the ones responsible for shopping and cooking food, so you’ve got to manage this condition for them, at least for one meal a day.’ R5, wife of a man with type 2 diabetes ‘Just trying to research food for dad, trying to make him better meals. Make him different sandwiches all the time at work.’ R4, daughter, lives with father with type 2 diabetes ‘I make sure what he [father] has every day: “you are not allowed to eat that anymore” so it’s quite hard to have to balance my university with all this watching his diet as well as mine, and they’re just jumbled up with each other.’ R6, daughter, lives apart from father with type 2 diabetes ‘Yeah, I try and buy less sweet things but for me, the dilemma is very difficult, because our daughter is underweight and doesn’t eat very much at all and she is much more likely to eat biscuits and cakes and sweets than anything else, so it’s trying to balance her need to have a high calorie [diet].’ R5, wife of a man with type 2 diabetes ‘… so for me one of the changes is knowing what’s supportive and what’s not, so the challenge existing is trying to police and say “you can’t do this and you can’t do that, you know, do you really need to eat that or should you be eating that, you know” because it’s not gonna help, you know, ‘cause you can just eat it when I’m not there, if you wanted to, but I find it hard to resist the urge to interfere.’ R5, wife of a man with type 2 diabetes ‘… I think he eats sweet packets so that gives me a reason to shout at him for it.’ R6, daughter, lives apart from father with type 2 diabetes ‘I would say usually, growing up your dad looks after you, but I’m suddenly thinking I need to look more after my dad as well.’ R2, daughter, lives apart from father with type 2 diabetes ‘… I suppose because I had the diagnosis and because of the potential for strokes and things like that, you can tell for the very first time they are thinking of me as someone who can die.’ P6, a woman with type 2 diabetes, lives alone ‘I think probably the balance in our relationship has changed. I would probably see me having more of a caring role than I had before. And I think like [husband] said, [husband] used to do all the cooking and the balance in that has changed.’ R7, wife of a man with type 2 diabetes ‘She [wife] likes caring for people, you know, she likes caring for me so in fact one thing, here you go, that's one thing that's changed, she does a lot more cooking than she used to (…) she is not a great cook but she is trying, she is doing a lot more of it to try and make things easier for me’. P9, a man with type 2 diabetes, lives with family ‘I'll sometimes cook whatever they [family members] want and I'll have something separate or I'll do myself something separate.’ P8, a woman with type 2 diabetes, lives with family ‘I am much less willing to offer him cakes or biscuits or anything like that … erm … I am much more focused on giving him salads.’ R1, mother, lives separate from son with type 2 diabetes
Men – ‘Going along’ with the new diet
Compared to the women in this sample, men provided support for their relatives with type 2 diabetes but were less likely to take responsibility for managing their relatives’ diet. Men were understanding of the fact that their relative with type 2 diabetes needs to adopt diet changes and they expressed willingness to support them by complying with the new diet regimen. Men also provided advice and encouragement to their relative with type 2 diabetes. However, they made a clear distinction between themselves and their relatives by highlighting that the responsibility for diet management falls on the person with type 2 diabetes: ‘I mean I understand that, you know, what [wife]’s got, you know, I am quite happy to go along with it and if I need to pig out or something, I'm probably gonna do it.’ R12, husband of a woman with type 2 diabetes ‘So I do try and get him to go out, like I always invite him for runs and stuff like that (…) He is very aware that it’s his diagnosis and it’s up to him to manage it himself’. R11, son, lives together with father with type 2 diabetes ‘Yeah, as I say, she prepares the meals, so she prepares meals that are good so I eat more healthy because of what she is cooking.’ R8, husband of a woman with type 2 diabetes ‘I make him be healthy but it’s rubbish … he would just eat anything’. P3, female with type 2 diabetes talking about her husband
Men with type 2 diabetes also appeared to rely on their female relatives for diet management: ‘She is telling me what to eat, I eat it.’ P4, male with type 2 diabetes, lives with wife ‘If I do something that’s gonna make it [type 2 diabetes] worse, I’d hope somebody either the doctor or a nurse or [wife] would point out that I was doing it’. P4, male with type 2 diabetes, lives with wife ‘I would’ve sort of wanted to be more supportive but I wouldn’t have got five textbooks and all that kind of stuff’. P2, male with type 2 diabetes, lives with family ‘I think initially I probably drove her quite mad with my weighing portions and so on, I think because she wasn’t doing it. I think she found that a bit irritating but beyond that she was quite accommodating’. P10, male with type 2 diabetes, lives with wife
Discussion
The findings in this article illuminate the role of gender in diet management for people with type 2 diabetes and their families. The study found that female relatives are more likely to take responsibility for ensuring the person with type 2 diabetes conforms to the new diet. Similarly, women with type 2 diabetes believed it is their responsibility to change their own diet, which sometimes resulted in adopting additional responsibilities. Men, whether patients or relatives, were more likely to comply with diet changes, initiated by women, rather than actively manage diet.
Women – Taking responsibility for diet management
In this study, women talked about their desire to take an active role in diet management in response to type 2 diabetes in their relative. This is consistent with previous findings that women are more likely, compared to men, to assume responsibility for the management of their partner’s diabetes. 23
The behaviour exhibited by female relatives in the current sample can be described by using the dyadic perspective of coping,24,25 according to which patient and partner interact with each other to mutually influence the adjustment process. Although the model of dyadic coping was developed in partners/spouses, it could apply to other family dyads, such as parent–offspring dyads. Women appear to engage in delegated dyadic coping, where they take over certain responsibilities to alleviate the burden from the person with type 2 diabetes. 25 Women were more likely to monitor other people’s diet and engage in “policing”, which in some cases resulted in a shift in relationship balance (women adopting new roles) and role reversal (children telling parents what to do). Similar patterns of behaviour in terms of family roles following diagnosis of diabetes have been observed before.16,18 Samuel-Hodge et al. 18 explored diabetes management in African Americans and found that family members often engage in food policing. A potential explanation for women’s increased likelihood to adopt a caregiving role is the suggestion that women internalise and take the caregiving role more seriously. 26 This could be rooted in historical and social practices. Bourdieu 27 argues that traditional gender roles have been maintained through social construction and gender socialisation, so women are considered to be inherently more likely to be caregivers. This is further confirmed by recent findings that women may be viewed by their husbands as ‘food preparers’.16,17 Bourdieu’s 27 suggestion also supports the finding that women with type 2 diabetes in the current study prioritised the needs of their family thus adopting additional responsibilities (for example by cooking two separate meals). Often, in families where men did the cooking, after their type 2 diabetes diagnosis women’s role in the kitchen appeared to increase. However, when women were the ones diagnosed with type 2 diabetes, they continued to cook without men taking additional responsibilities in relation to food preparation.
Although not directly explored in this study, the likelihood of relatives to adopt a caring role may be influenced by geographical distance. According to Carmichael and Charles 28 geographical distance is a type of a ‘non-economic’ factor that influences people’s decision to adopt a caring role. Some of the participants in the current study admitted that they thought more often about their relative with type 2 diabetes but having work and family obligations and living far away from their relative, interfered with their ability to provide support. However, female relatives talked about changing the meals they prepare when their relative with type 2 diabetes visits them.
Men – ‘Going along’ with the new diet
Men, in the current sample, often talked about relying on their relatives to make diet changes and ‘going along’ with these changes was perceived as supportive behaviour. This can be explained in terms of supportive dyadic coping where men provided support, advice and encouragement. 25 This is consistent with previous research that men with type 2 diabetes are more likely to depend on their spouses.11,12 Del Rio-Lozano et al. 26 suggest that men have a more flexible approach to care and do not identify with the caregiving role. This may put men at a position of advantage because their wives prepare meals that conform to the prescribed diet. 9 Although the sample of male relatives in the current study was small, the results showed that men provided support and advice to their relatives with type 2 diabetes but were less likely to feel responsible for monitoring the patient’s diet. We were not able to explore differences in support provision between husbands and sons but previous research suggests that there is a difference between sons’ and husbands’ perception of caregiving. 29 Sons perceive a filial obligation to provide care for their mothers while husbands see caregiving as an extension of their marital role. 29
Implications
The current study supports previous research suggesting that women are more likely than men to provide hands-on care with instrumental activities of daily living, such as shopping and preparing meals. 30 This has implications for family-focused care as women who adopt a caregiving role experience more chronic health disorders, such as stress, anxiety and depression.10,12,15 Also, when women try to manage the other person’s condition, they may undermine their confidence to control their own condition. 31 Family interventions have the potential to reduce caregiving burden and depression. 31 A systematic review and meta-analysis by Armour et al. 32 show that interventions which involve family members can lead to improved diabetes knowledge and better controlled diabetes, and reduction in family conflicts. Future interventions can utilise established behaviour change techniques 33 to provide information about diabetes, encourage communication within the family and set clear goals in terms of diet management for the whole family. In addition, interventions could capitalise on dyadic coping theory 25 to account for different coping styles and optimise family cooperation. This may be particularly important as the current study shows women and men may engage in different types of dyadic coping. Supportive dyadic coping (often adopted by men) is a stronger predictor of relationship satisfaction than delegated coping (often adopted by women). 34 Family interventions can help families discuss roles in relation to diet management and re-negotiate these roles by taking into account potential gender differences. However, interventions need to be sensitive to cultural values when addressing gender roles and chronic illness. For example, Latinos are more traditionally gender role oriented than other cultures and women are encouraged to provide emotional support for their partners. 34 African American families may not talk about diabetes as they do not think it should be discussed with family members. 35 This could lead to the adoption of traditional gender roles where people with type 2 diabetes and their relatives do not establish what their new role in the family is. For example, women with diabetes adopt a multi-caregiving role, assuming family members do not understand their needs and their husbands would not be supportive of diet change.36,37 However, this may not be the case as husbands are often willing to modify their behaviour to support the wife’s dietary needs. 37 Having culture-sensitive interventions is particularly important in places where ethnic minority groups live. For example, in Scotland the percentage of ethnic minority groups varies from 6% to 12% in different council areas 38 so a population-wide approach to diabetes management may not be suitable for these groups.
The study also has implications for direct provision of diabetes-related care. It shows that the experiences of diet management in response to type 2 diabetes are not limited to the patient, so patients can be encouraged to bring relatives to their diabetes appointments. Currently, in the UK explanations about what to expect at diabetes appointments do not specify whether the patient could bring a relative.39,40 Attending a diabetes appointment together may provide a platform for family discussion about the best way to manage dietary needs.
Study limitations
The current study has several limitations that should be considered. Sampling bias cannot be excluded as participants who took part in the interviews contacted the researcher so it is not clear whether people who volunteer to take part, have different characteristics from people who are randomly chosen. In addition, all participants were white and living in the UK so the findings are not transferable to other countries. A recent study in 5 European countries shows that gender differences in relation to diet management may be particularly evident in Spain and Greece. 41 The authors suggest that in countries with particularly strong family structures, women take responsibility for diet management. The role of culture in relation to gender roles should be further investigated in future studies. Another limitation is the fact that not all interviews included a person with type 2 diabetes and a relative from the same family and that the form of the interviews was not consistent (individual vs family interview). More work is needed to uncover different perceptions of roles in relation to diet and type 2 diabetes among family members. Finally, the number of male relatives was low and this should be taken into consideration when interpreting the study findings.
Conclusion
The current study suggests that women (whether with type 2 diabetes or relatives) may be more likely to prioritise the needs of their family and take an active role in relation to diet management. This is consistent with previous findings on gender and diet management in diabetes. The study builds on previous work by showing that traditional gender roles, where women are responsible for food preparation, may be still prevalent in the UK. Family-based interventions should focus on the role of gender when adapting to chronic illness. While the results in this paper are drawn from secondary analysis, they provide meaningful contribution to existing literature on gender and diet management in relation to type 2 diabetes.
Footnotes
Acknowledgements
We would like to thank all the organisations who assisted with recruitment of participants and all the participants who took part in the study.
Contributorship
All authors were involved in the conception of the study. EDD was the main researcher who conducted data collection and analysis. JMME and VS were the PhD supervisors. EDD wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the University of Stirling, School of Health Sciences ethics committee (SREC 15/16, Paper No. 37, version 1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council (ESRC) as part of a PhD project.
Guarantor
EDD
Informed consent
Written informed consent was obtained from all subjects immediately before the start of the interview.
Trial registration
Not applicable because the study is not a trial.