
Abstract
This study utilized a mixed methods approach to examine the feasibility and acceptability of group compassion focused therapy for adults with intellectual disabilities (CFT-ID). Six participants with mild ID participated in six sessions of group CFT, specifically adapted for adults with ID. Session-by-session feasibility and acceptability measures suggested that participants understood the group content and process and experienced group sessions and experiential practices as helpful and enjoyable. Thematic analysis of focus groups identified three themes relating to (1) direct experiences of the group, (2) initial difficulties in being self-compassionate and (3) positive emotional changes. Pre- and post-group outcome measures indicated significant reductions in both self-criticism and unfavourable social comparisons. Results suggest that CFT can be adapted for individuals with ID and provide preliminary evidence that people with ID and psychological difficulties may experience a number of benefits from this group intervention.
Introduction
The role of shame in the development and maintenance of psychological distress in adults with intellectual disabilities (IDs) is relatively neglected and overlooked. Research indicates that some individuals with mild to moderate ID experience their ‘disability’ as a significant stressor, particularly the aspect of being seen as ‘disabled’ by the general public (Bramston et al., 1999). Growing evidence suggests that experiences of social rejection, exclusion, discrimination and stigmatization significantly negatively impact on a number of psychological and emotional processes, and the development and maintenance of psychological distress in adults with ID (Ali et al., 2012, 2015). Many individuals with ID engage in negative social comparisons compared with others. This can lead to a sense of shame and subsequent mental health difficulties such as anxiety and depression (Dagnan and Sandhu, 1999; Dagnan and Waring, 2004), particularly through internalized shame (i.e. self-stigma) that results in negative self-evaluations and self-criticism (Ali et al., 2012; Dagnan and Waring, 2004; Esdale et al., 2015). Perception of stigma in adults with ID has been linked to negative social comparisons, subsequent depression and low self-esteem (MacMahon and Jahoda, 2008; Paterson et al., 2012). Recent research suggests that individuals with ID are more likely to believe and be distressed by social criticism than individuals without ID (Esdale et al., 2015). Group-analytic research has also identified shame, rejection, and grief as common themes among individuals with mild ID (O’Connor, 2001), seemingly driven by the desire to fit in and be ‘normal’, and not be seen as having an ID.
Such research suggests that developing and adapting psychological interventions that explicitly and directly work with shame (external and internal) may be a promising avenue in reducing psychological distress and improving the well-being of individuals with ID, particularly as these processes are often not specifically targeted in interventions. One potential therapeutic avenue as an antidote to shame and self-criticism is to focus on helping people cultivate compassion towards the self and others (Gilbert, 2009, 2010; Hofmann et al., 2011; Neff, 2003a).
Although definitions of compassion often vary (Strauss et al., 2016), most scientific approaches are converging around the conceptualization of compassion as ‘a sensitivity to suffering in self and others, with a commitment to try and alleviate and prevent it’ (Gilbert and Choden, 2013). Compassion is rooted in caring motives (Gilbert, 2005, 2015), which at its core is about building the courage to face, accept and deal with one’s difficulties in life (Gilbert, 2010, 2015), rather than avoiding or denying them, and thus may be a resilience mechanism (Trompetter et al., 2016). Accordingly, compassion-focused interventions focus on changing one’s relationship and orientation to the self, other and experiences in life (Gilbert and Procter, 2006).
Compassion focused therapy (CFT; Gilbert, 2005, 2009, 2010) is a promising approach for adults with ID, as it was specifically developed for people with mental health difficulties characterized by high shame and self-criticism. CFT is a motivational multi-modal therapy that focuses on helping people access and stimulate affiliative motives, emotions and competencies underpinning compassion that play important roles in threat regulation, well-being and prosocial behaviour (Gilbert, 2014, 2015). Thus, CFT targets the development and recruitment of two psychologies or ‘mindsets’ of compassion (Gilbert, 2014; Gilbert and Choden, 2013) (i) to help people empathically engage with their suffering (i.e. engagement) and (ii) to take wise action in dealing with, reducing and preventing that suffering (i.e. alleviation).
This process is likely enhanced in a group setting, as central to CFT is the creation of affiliative contexts to share, de-shame, validate, soothe and encourage (Bates, 2005). Accordingly, a group context has the potential to directly influence the flow of compassion (Gilbert, 2014), namely: receiving compassion from others; feeling compassion for others and directing compassion to ourselves (i.e. self-compassion). CFT sees working with and enhancing this flow of compassion as crucial for buffering against psychopathology (Matos et al., 2015) and for optimal functioning and well-being (Hermanto and Zuroff, 2016; Hermanto et al., 2016).
There is growing evidence for the effectiveness of CFT for a range of psychological difficulties in people without ID (Beaumont and Hollins Martin, 2015; Leaviss and Uttley, 2015). CFT has been shown to be feasible, acceptable and efficacious in a group format for individuals with wide-ranging and complex mental health difficulties (Gilbert and Procter, 2006; Judge et al., 2012; Lucre and Corten, 2013) and when adapted into briefer group therapies (Heriot-Maitland et al., 2014). Group-based CFT has been shown to reduce shame, self-criticism, negative social comparisons, depression and anxiety in clinical populations (Gilbert and Procter, 2006; Judge et al., 2012; Lucre and Corten, 2013).
Group interventions have been developed and successfully adapted for individuals with ID (Rossiter et al., 2016), demonstrating effectiveness in reducing anxiety (Idusohan-Moizer et al., 2015), depression (McCabe et al., 2006) and problematic anger (Rose et al., 2000, 2005). In terms of compassion-based group interventions, one study has attempted to teach self-compassion to adult individuals with ID with recurrent depression and anxiety, but within the context of an adapted mindfulness-based cognitive therapy group intervention (Idusohan-Moizer et al., 2015). While this resulted in significant increases in compassion for self and other, and reduced anxiety and depression, compassion was not the primary focus of the intervention. Hence, it is not possible to tease out the specific effects of the self-compassion component of this intervention.
To date, no known study has formally adapted CFT and related practices of compassionate mind training (CMT; Gilbert and Irons, 2005; Gilbert and Procter, 2006) for individuals with ID and/or investigated whether this is feasible and acceptable in a group format for this population.
Aims
The main aim of this study is to preliminarily investigate and explore whether a CFT group intervention is feasible and acceptable for adults with ID who have concurrent mental health issues. Given that this is the first account of adapting and delivering a CFT group for individuals with ID, outcome data centres largely around session-by-session self-reports of participants’ perceived understanding and acceptability, and qualitative data regarding people’s experiences of and within the group.
Method
Ethics
This study was approved by Bangor University Ethics Committee and the local NHS Research Ethics Committee.
Recruitment procedure
Participants were recruited from NHS Community Learning Disabilities teams in North Wales. The nature and aims of the study were discussed within appropriate multidisciplinary team meetings, and team members were encouraged to identify and refer potentially suitable candidates that met the inclusion criteria. Referral packs were also left for NHS team members as both reminders of inclusion/exclusion criteria, and participant information sheets were shared with potentially interested participants.
The principal inclusion criteria were as follows: (1) a diagnosis of an ID; (2) aged 18+ (no upper age limit); (3) significant psychological distress, indicated by minimum score of 13 1 on the relevant index of the Psychological Therapies Outcome Scale for IDs (Vlissides, 2014); (4) accompanying self-criticism (as indicated by appropriate measures and informal behavioural observations) and (5) participants had to demonstrate the capacity to consent. Exclusion criteria comprised of (1) currently experiencing psychosis or mania and (2) lack of capacity to understand the nature of participating in the research.
Participants
Nine participants were referred as potentially suitable candidates for the group. Two of these individuals were subsequently not assessed, due to one individual being in crisis at the time of referral and the other being referred too late to be able to undergo the pre-assessment process. Accordingly, seven individuals underwent the pre-group assessment process, with all meeting the inclusion criteria for the study. One of these individuals subsequently did not attend any of the group sessions and was thus not included in the study.
The mean age of the six participants included in the study was 38.5 years (standard deviation = 15.6), consisting of four females (67%) and two males. All participants had previously been formally assessed for the presence of an ID, with all diagnosed as having mild ID (i.e. IQ between 51 and 69, and associated impairment in day-to-day adaptive skills), and were receiving some form of specialist support due to their adaptive difficulties. All participants had a documented history of mental health issues that included anxiety (n = 1), depression (n = 1) or mixed anxiety and depression (n = 4).
Two rounds of the groups ran consecutively on one site, in order to recruit a sufficient number of participants after receiving a small number of referrals for the first group. Participants were given a choice as to whether they wished to be accompanied by a supporter/carer. Group 1 consisted of three participants (two females and one male), one of whom was accompanied by a support worker for two sessions. Group 2 consisted of three participants (two females, one male), all of whom were accompanied by support workers for the entirety of the group.
Methods of evaluation
This study utilized a mixed methods design combining quantitative and qualitative measures. Participants completed three outcome measures during the pre-group assessment process, and the same measures between 2 to 4 weeks after the end of the intervention. The principal investigator assisted all participants in completing these measures.
CFT-ID Session Feasibility and Acceptability Measure. This measure was designed by the project team as a descriptive measure of feasibility and acceptability, which was administered at the end of every group session. The measure consists of five questions (each with three response options), which attempt to ascertain (1) how much of the session was understood, (2) whether the group was helpful or not, (3) how helpful the specific exercises were, (4) how easy/hard were the exercises/practices to engage in and (5) whether or not they enjoyed the session. The scale was presented in an easy-read format.
Self-Compassion Scale-Short Form (SCS-SF; Raes et al., 2011). This scale is a shortened 12-item version of the original 26-item SCS (Neff, 2003b) designed to assess an individual’s self-compassion across three components: self-kindness, common humanity and mindfulness. This provides an overall self-compassion score (Neff, 2016), although recent research has suggested that using the total score for the scale is unreliable, and thus not recommended (Muris and Petrocchi, 2017). Alternatively, a two-factor structure, where the original six subscales are separated into ‘self-compassion’ (positive subscales: self-kindness, common humanity and mindfulness) and ‘self-criticism’ (negative subscales: self-judgement, isolation and over-identification) factors, has been proposed (Costa et al., 2015; López et al., 2015), supported by strong psychometric validity in clinical and non-clinical populations (Costa et al., 2015). The original SCS has demonstrated good psychometric properties, with the SCS-SF demonstrating a high correlation with the long form SCS (r ≥ 0.97 all samples) and adequate internal consistency (Cronbach’s α ≥ 0.86 in all samples). This measure has yet to be validated or adequately applied to research within an ID population. Permission was obtained from one of the original authors to adapt the scale for the identified population. Adaptations involved simplifying the wording of the questions so that these were more understandable and accessible for an ID population.
The Psychological Therapy Outcome Scale for Intellectual Disabilities (PTOS-ID; Vlissides, 2014). The PTOS-ID is a 29-item scale designed to measure both psychological distress (encompassing anger and anxiety) and positive well-being (psychological and interpersonal well-being) in people with ID, which lends itself favourably as a scale that is both accessible and meaningful to this population. Preliminary validation of the PTOS-ID suggests that it is a psychometrically robust measure of psychological distress and well-being in this population, demonstrating good levels of construct and concurrent validity, reliability and internal consistency (Vlissides, 2014).
The adapted Social Comparison Scale (Dagnan and Sandhu, 1999). This scale, adapted for adults with ID from the original Social Comparison Scale (Allan and Gilbert, 1995), examines the way people evaluate themselves through comparisons with others, across the domains of rank and achievement, social attractiveness and group belonging. Lower scores indicate feelings of inferiority and general low rank self-perceptions and thus measure aspects of internal shame. The adapted scale has demonstrated a similar psychometric structure to the original scale (Dagnan and Sandhu, 1999) and reasonable Cronbach’s alphas (ranging from α = 0.56 to 0.76) for the full scale with this population (Dagnan and Sandhu, 1999; Paterson et al., 2012).
Statistical analysis. Within-group comparisons for pre- and post-group mean scores across outcome measures were performed. All data were tested for normal distribution.
Focus groups. A semi-structured interview schedule was utilized and adapted (with permission) from a previous study that developed the schedule to similarly investigate adult individuals’ experience of attending CFT groups for acute inpatient settings (Heriot-Maitland et al., 2014). The focus groups were conducted at the end of the final session so as to capture participants’ immediate experiences of having undertaken and completed the group. Both focus groups were conducted by individuals who were not involved in the running of the group (a clinical psychologist and a trainee clinical psychologist), lasting for approximately 45 min. The focus groups were recorded via Dictaphone (with prior consent) in order to aid transcription. All six participants attended the focus groups.
Intervention
CFT is based on an evolutionary and neuroscience model of mind and emotional regulation, known as the ‘Three Circles’ model (Depue and Morrone-Strupinsky, 2005; Gilbert, 2009, 2014). These three systems are (1) the threat and self-protection system; (2) the drive-seeking and reward system and (3) the affiliative/soothing system. CFT suggests that some mental health difficulties arise when these affect regulation systems become unbalanced, particularly when the threat system becomes poorly regulated (Gilbert, 2010). CFT involves a significant amount of psychoeducation around the evolved nature of our minds that have left us with ‘tricky brains’, and how these three systems have become patterned, organized and conditioned by life experiences. A primary focus of CFT is to balance these systems through stimulating the affiliative/soothing system (Gilbert, 2010, 2014, 2015), as this system is proposed to be the natural regulator of the threat and drive systems. This involves a series of compassion cultivation exercises (CMT; Gilbert and Irons, 2005) such as attention training, soothing breathing rhythm, mindfulness, mentalising, compassionate self-identity cultivation, the use of compassionate imagery and enacting compassionate behaviours on a regular basis. Thus, these interventions help to access and cultivate the affiliative motivational system that helps facilitate compassion, becoming the organizing motivational system for the individual.
The group CFT-ID protocol was developed by the first author, drawing on group outlines and protocols from other researched CFT groups (Heriot-Maitland et al., 2014). The group process was guided by the overarching processes and non-linear phases integral to CFT that have been outlined in detail elsewhere (Gilbert, 2010, 2014; Kolts, 2016), in conjunction with the modules and practices of CMT (Gilbert and Irons, 2005; Gilbert and Procter, 2006) to develop the skills and attributes of compassion. Table 1 (see below) summarizes the process, content and practice(s) associated with each session.
Summary content of the Growing Kind Minds CFT-ID group programme.
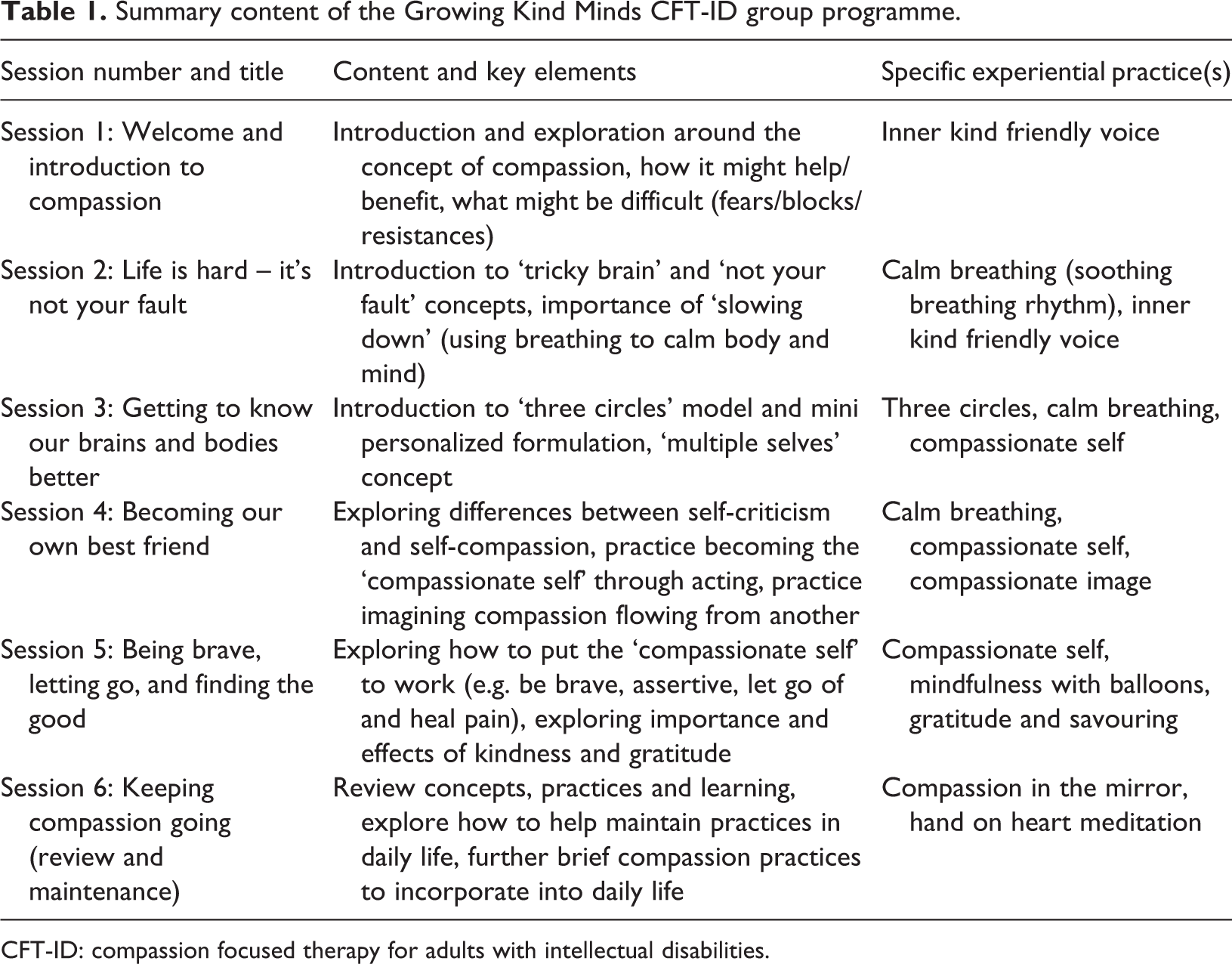
CFT-ID: compassion focused therapy for adults with intellectual disabilities.
Alterations to the application of the model were made on the basis of recommendations for adapting psychological therapies (including mindfulness/acceptance-type interventions) for adults with ID (Gore and Hastings, 2016; Taylor et al., 2013) and clinical experience of working with ID populations. Changes in application included the presentation of psychoeducational material in a concrete, visual manner that minimized the use of abstract language (supported by the use of PowerPoint slides) and other visual methods to support understanding and demonstrate the purpose of particular practices/exercises. A supporting workbook that contained simple written and visual summaries of each session and accompanying practice(s) was also developed to further aid understanding and support home/personal practice.
Each session lasted for approximately 90 min. Participants were instructed to practice the experiential exercises as part of personal practice between sessions, but frequency and duration of practice(s) were not recorded.
The groups were facilitated by the principal investigator (NEC), who has approximately 3 years supervised CFT practice, has attended numerous CFT trainings and workshops, and attends regular group supervision with Professor Paul Gilbert. Group 1 was co-facilitated by a senior clinical psychologist (JW) who has extensive experience adapting and delivering mindfulness and acceptance-based therapies for adults with ID. Group 2 was co-facilitated by a trainee clinical psychologist.
Results
Feasibility and acceptability data – attendance data and session-by-session feedback
Six out of the seven recruited participants (86%) completed the intervention. One individual who completed the pre-group assessment process did not attend any of the sessions and was thus not included in any further analysis. Four participants (66.66%) completed the full six sessions, with the remaining two participants (33.33%) completing five of the six sessions. Participant 1 missed session 4 due to a misunderstanding around dates/times of the group for that session, and participant 2 missed session 1 due to difficulties in finding the location of the group. Due to its foundational and introductory nature, participant 2 was given the session 1 module in a one-to-one session facilitated by the principal investigator.
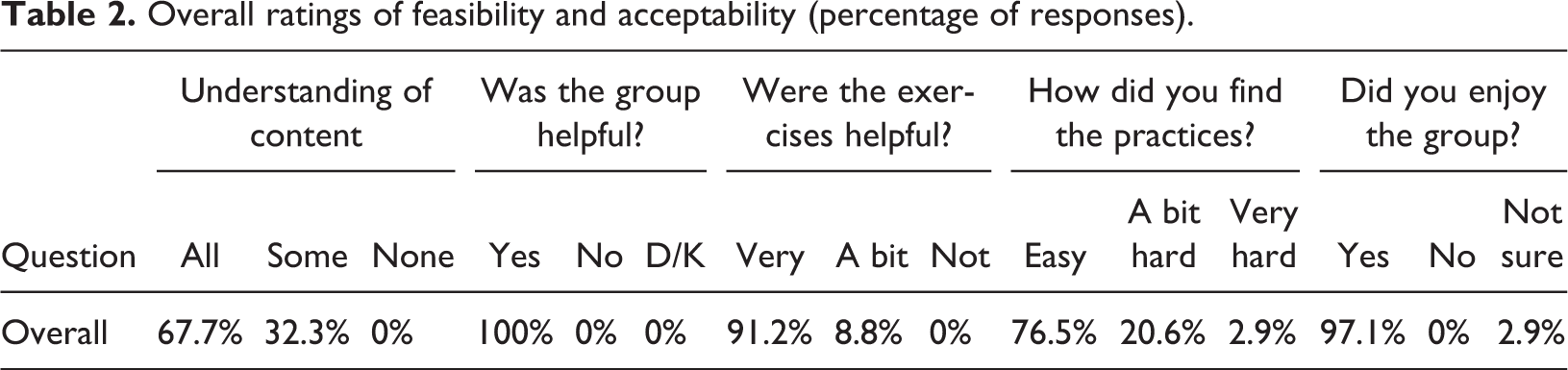
Table 2 provides an overall summary of session-by-session feedback from the feasibility and acceptability measure, regarding perceived understanding and helpfulness of the group and practices. Participants clearly found the groups helpful and enjoyable, while there is more variance in levels of understanding and perceived difficulty of experiential practices across the six sessions.
Overall ratings of feasibility and acceptability (percentage of responses).
Quantitative analysis
Data analysis: Although Kolmogorov–Smirnov tests were non-significant, these tests were considered underpowered due to the small sample size, preventing us from concluding that data met normality assumptions. Accordingly, Wilcoxon signed-rank tests were used to measure differences between pre- and post-group scores across the measures, recommended as the most appropriate non-parametric test for a within-subjects repeated measures design for studies with small numbers of participants (Field, 2005). Table 3 provides a summary of observed changes between pre- and post-group mean scores across outcome measures.
Descriptive and inferential statistics comparing changes in pre- and post-group measures (n = 6).
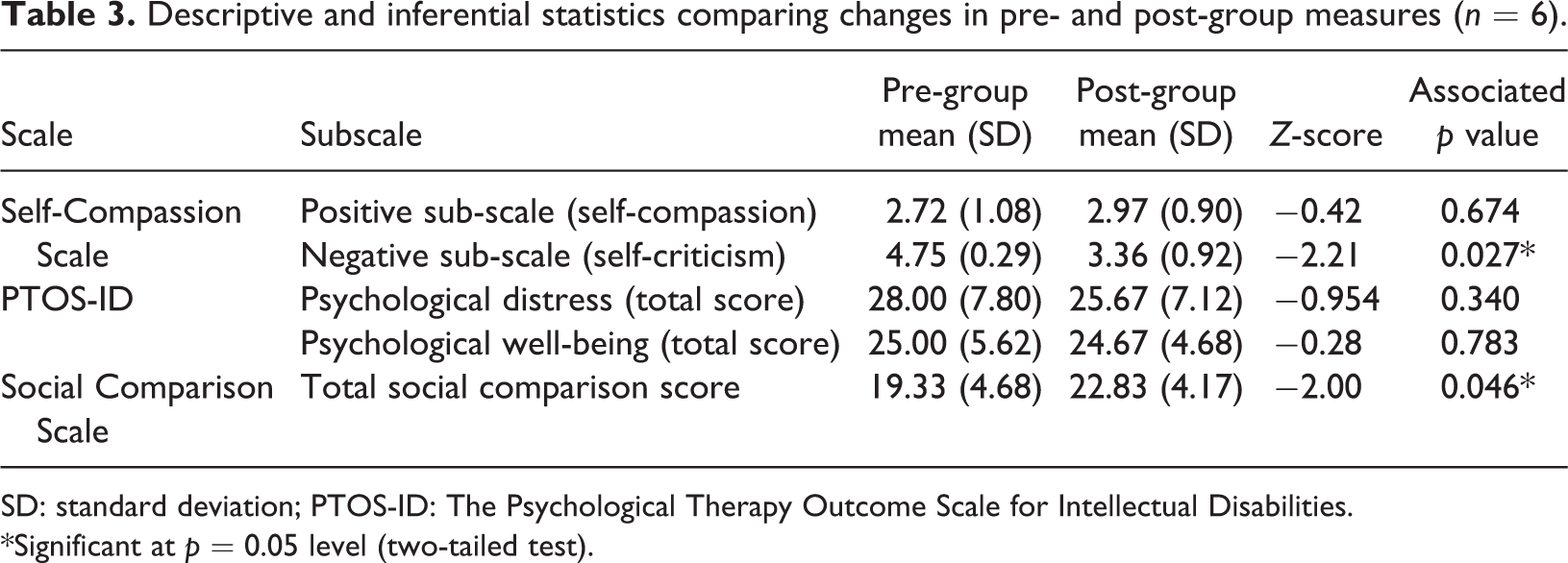
SD: standard deviation; PTOS-ID: The Psychological Therapy Outcome Scale for Intellectual Disabilities.
*Significant at p = 0.05 level (two-tailed test).
Self-Compassion Scale: Using the two-factor structure, scores on the self-criticism factor significantly decreased pre- to post-group (z = −2.21, p = 0.027), but there was no significant change on the self-compassion factor (z = −0.42, p = 0.674).
Psychological distress and well-being: There was no significant change in overall psychological distress (z = −0.954, p = 0.34) or psychological well-being (z = −0.28, p = 0.783) scores.
Social comparison. Post-group scores for social comparison (using the total score) were significantly higher compared to pre-group (z = −2.00, p = 0.046), indicating a reduction in unfavourable social comparisons and thus feelings of inferiority.
Qualitative analysis
Data analysis: All data obtained from the focus groups was analysed utilizing thematic analysis (Braun and Clarke, 2006). This analytical approach was chosen as its primary purpose is to capture emerging themes, which best fit the primary aims of this study in exploring feasibility and acceptability. The form of thematic analysis was primarily inductive in nature, where themes derive largely from the semantic content of the data, and followed the six phases of analysis outlined by Braun and Clarke (2006). This involved the primary researcher familiarizing themselves with the data through full transcription of focus group recordings; identifying and generating codes across the entire data set; collating codes into potential themes, aided by the development of thematic maps; reviewing themes with an expert in qualitative analysis separate from the research team (GG), and the generation of a final thematic map; and defining and naming the themes to form a coherent narrative in relation to the extracts and entire data set.
Thematic analysis yielded three superordinate themes, with some containing sub-themes, which were consistently identified from the focus groups: (1) direct experiences of the group process; (2) fears, blocks and resistances to compassion and (3) changes relating to self, other and life experiences. All participants’ names are pseudonyms.
Theme 1: ‘It’s like…you’re not on your own’ – Experiences of the group intervention and process
Participants often described how the group intervention had been a positive experience and benefitted them in some way. This superordinate theme highlights the process and content of the CFT group (subordinate theme of ‘everything was helpful’), how this helped to de-shame participants’ suffering, and began to facilitate the cultivation of compassion (subordinate themes of ‘we’re not alone’ and ‘our brain works in mysterious ways’).
1.1. ‘Everything was helpful’. A consistent narrative that emerged from all participants’ responses was that they experienced the entirety of the CFT group as helpful: Um, everything about it. (Zooey) Yeah, everything really. (Crispin) Ummm, everything really. Like, help me type of thing, stuff like that…like, how to like cope with things and stuff like that (Crispin) I’m, I’m finding it really positive now thanks to this. (James) I think everything in, in its own way has helped us all in a different way. (Kathy) Umm, it would probably help them through life or something…like, probably if they had a bad life, how to cope with their bad life. (Crispin) It’s like, you’re not, you’re not on your own. You know, there are other people that are going through the same thing…I’d say [chuckles], I’ve managed to realise that, that I’m not on my own. (Kathy)
And being in like the same boat and all that
Yeah
Ahhh, ok, so you learnt that everybody’s in the same boat and
Yeah
Trying to get through life
Yeah?
And we’re not alone.
1.3. ‘Our brain works in mysterious ways’. One participant reported explicitly remembering some of the evolutionary concepts such as the ‘tricky brain’, but their articulation of this concept was vague and did not explicitly communicate a deeper level of understanding:
The way our brain works and that
Ahhh okay, ‘the way our brain works’. How do our brains work?
In many mysterious ways!
This was also true for other core CFT concepts such as the ‘Three Circles’ affect regulation model. Participants demonstrated they had grasped some of the basic concepts, albeit displaying a degree of uncertainty when attempting to articulate their understanding:
The red one is where you’re worried a lot
Uh hum
Hum
The green one is where you’re so peaceful and relaxed
Aahhhh
and the blue one is…(hesitant pause)
In between
Yeah, in between
Furthermore, some participants appeared to demonstrate some level of deeper understanding about these concepts, but some of their responses continued to be vague. Such responses may be indicative of some of the theoretical/conceptual aspects of the intervention being a little too complex for participants to fully grasp:
The green one’s better
Yeah
The green one’s better. Brill. So is that where everybody is trying to get do you think?
Yeah
Yeah? And then if somebody was in the red, how would they know?
They’d be feeling stressed
They’d be down in the dumps
Feeling stressed
Yeah.
Theme 2: ‘It’s hard to be kind to yourself when you’re always used to not being kind to yourself’ – Fears, blocks and resistances to compassion
Many of the participants reported initially finding compassion exercises/practices strange and difficult: When I first did the breathing, I thought ‘what is he [therapist] on?!?’…you know, ‘this is daft!’ (Kathy) I’ve always been the same: beatin’ me self up, doin’ it again, do it again…and the being kind to yourself doesn’t happen. It’s sort of…it’s hard to be kind to yourself when you’re always used to not being kind to yourself…(Kathy) But once I, once I let myself do it [the breathing], it was kind of relaxing, and it does help you out in ways you wouldn’t even think about. (Kathy) …the being kinder part was nice because somebody else saw that in you, that you know is already there but you just can’t access it…I think sometimes you just need to be shown a couple of times, and then it depends on how your head is. Maybe you can carry it through…(Kathy)
At first it was a bit hard, but the easier it got, but at first it’s hard…
Yeah?…do you feel like it’s a bit easier to put it all into practice?
Yeah, like putting a jigsaw together and that! But with practice it gets easier.
In summary, all participants described a journey of initially being sceptical about compassion or finding the practices difficult, to finding their own way to open to compassion and work with the practices, and receiving some benefit. These benefits are further described in Theme 3.
Theme 3: ‘Looking at yourself from the inside’ – Changes in relating to self, other and life experiences
This superordinate theme reflects how engaging in CFT-specific compassion practices both within and outside (e.g. home practice) the group appeared to result in significant emotional changes. The subordinate themes describe positive changes in participants’ sense of self and self-to-self relating, and how compassion practice(s) appeared to be beginning to give them additional skills to cope with difficulties and also flourish in day-to-day life.
3.1. ‘Finding the inner peace of you’ – feeling calmer. Participants unanimously reported significant positive emotional changes, particularly as a result of practicing calm breathing (soothing breathing rhythm; SBR). Many reported increases in affiliative and contented emotion, such as feeling calmer, safer and more relaxed, a core therapeutic target in CFT: I, I’ve learnt the breathing exercises can keep you, keep you more relaxed. (James) …it, it sort of chills you out. (Kathy) Relaxing your body. (Crispin)
What would you say it’s changed? What has it helped you do?
Be the…inner peace of you…like, looking at yourself from the inside.
Some participants described how engaging in CFT exercises helped regulate threat processing and threat-based emotions, such as worries and anxiety, while also increasing affiliative feelings of safeness, contentment and well-being:
Any other ways it has helped?
Urm (brief pause), trying to clear my mind [of my siblings] really, like, not seeing them again sort of thing…just like, be happy really and not worry about it. See like, ‘cos I know they’re safe kinda thing…
3.2. ‘Coping with my inner self’ – increased self-compassion. Participants unanimously reported changes in self-to-self relating, but again their verbal accounts were often vague. A number of participants specifically reported that the intervention in general had contributed to a sense of increased self-understanding: It just…helped me understand myself a little bit better…urm, how to cope with my inner self, basically. (Anne) …I’m not that negative like I used to be…being kind, kinder to yourself ones help, ‘cos ‘cos I don’t think much that I’m a weak link anymore…(James) …and you know you can, you can find it in, in yourself to be nice to yourself, to be nice to other people…instead of being the one that…beating yourself up…(Kathy) Finding the person you really are…on the inside. (Zooey)
…okay, so what sort of time of day do you tend to use it then?
Morning, noon and night! [laughs]
and
Are there any times when you’ve been having a tricky time but you were kinder to yourself?
Probably every day, near enough!
One participant reported that she did not engage in personal compassion practice(s) outside of the group settings and was unable to articulate specific reasons for this, despite reporting having benefitted from the practices within group sessions: No, I don’t do them at home. (Anne)
…before I, sometimes like when I go to places like the Day Centre and that, before I go upstairs sometimes
Ok, so when you go to places where you’re worried?
Yeah…I do before I go there, and it makes me happier and that then.
and I close my eyes, and do the breathing exercises, and I find it helps me with me walk ‘cos I used to have panic attacks when I went out, but it don’t happen so much now. (Beatrice) …it felt, it felt like because I had the courage and the guts to say ‘hang on a minute’, you know…I thought ‘if you don’t say it now, I’m never gonna do it, and it’s gonna continue to get on my nerves, I’ll beat myself up and I’ll be back to square one’, and I don’t want that to happen again this time. (Kathy) …Dad…he used to hate talking to me ‘cos I, I was like a spoilt three year old…he said it’s a joy to speak to me now. He says it’s almost like you’ve grown up overnight. (Kathy)
Discussion
This study of CFT groups for adults with ID aimed to primarily explore and evaluate its feasibility and acceptability for this population. This is the first study to formally adapt and evaluate an explicitly compassion-focused group intervention for adults with ID.
Results from the feasibility and acceptability measures, and high rates of attendance, all preliminarily suggest that group-based CFT was experienced as a safe, accessible and helpful intervention by all participants. This was echoed in the qualitative data of participants’ experience of the group, where a common theme emerged of participants reporting the entirety of the group as helpful.
Thematic analysis appeared to suggest that the CFT group positively impacted on the flow of compassion (i.e. receiving compassion, giving compassion and self-compassion). Specifically, being open to receiving compassion from others appeared to positively impact on their sense of self by reducing their sense of shame and was crucial in their efforts to become more self-compassionate. These processes are supported by emerging research in the non-ID adult literature, in that reducing shame and feeling a sense of safeness in the world is dependent on being able to utilize and experience affiliative relationships as soothing (Hermanto et al., 2016; Matos et al., 2015). This is further supported by CBT process research in adults with mild ID, where affiliative therapeutic relationships have been cited as the most important and beneficial factor in fostering social safeness and acceptance (Pert et al., 2013). However, some of these changes could be attributed to more general group processes and therapeutic factors that are not specific to CFT, such as universality, altruism and group cohesiveness (Yalom, 2005).
One of the themes that emerged consistently from the qualitative analysis and group process was that most participants experienced initial difficulties in being able to receive and generate compassion for themselves. These represent common FBRs to developing compassion, which are increasingly reported in the non-ID adult literature (Gilbert et al., 2011; Lawrence and Lee, 2014; Pauley and McPherson, 2010). This is the first study to document the presence of FBRs to compassion in adults with ID, and that the process of overcoming these FBRs may be similar to those observed in non-ID adult populations (Lawrence and Lee, 2014). This was verified by participants’ accounts of becoming increasingly self-compassionate through repeated practice and desensitization to affiliative affect.
Participants reported that recommended ID-specific adaptations to therapy (Gore and Hastings, 2016), such as the adapted workbook and using coloured sand and water in a bottle to demonstrate the purpose of slowing/stilling the mind-body, were very helpful in supporting understanding. However, some of the data obtained from the acceptability and feasibility measures and thematic analysis suggests that some of the CFT concepts may be too complex for individuals with ID to understand. For example, participants could recall some of the evolutionary concepts such as the ‘tricky brain’, but it was unclear whether they fully understood these concepts and how they might helpfully apply to themselves. It is possible that some of these concepts were presented in a manner that was still too abstract for participants to fully comprehend. Further work may be required to find more creative ways of presenting these concepts in a more concrete, and thus understandable, fashion. This may also be achieved by further reducing the content and spending more time on one particular concept per session, and extending the number of sessions.
Nonetheless, all participants were able to engage with the various compassion practices in session and experience them as beneficial, even if at times encountering challenges when doing so. Although participants often found it difficult to articulate their understanding of concepts and practices, they still reported that they were able to start generalizing the practices to their day-to-day lives. This supports the notion that people with ID can make use of psychological principles and practices, even without being able to describe them and/or changes in private events (Jones and Dowey, 2013). These processes have been observed in other studies examining the experiences of Dialectical Behaviour Therapy (DBT; Roscoe et al., 2015) and mindfulness groups (Yildiran and Holt, 2015) for adults with mild to moderate ID. CFT, like DBT and mindfulness, involves a high degree of experiential and behavioural teaching/learning, and meditative practice(s). This may lend itself more favourably to this population, as it minimizes the cognitive demands and verbal reasoning skills placed on participants that they might otherwise struggle with. The outcomes of this study provide further support for research suggesting that people with ID can benefit from psychological therapies as long as sufficient adaptations are made (Lindsay et al., 2013).
Quantitative data obtained from pre- and post-group measures tentatively suggest that CFT may reduce self-criticism, shame and negative social comparisons in individuals with ID. These findings are consistent with outcomes in studies of group-based CFT in diverse adult clinical populations (Gilbert and Procter, 2006; Heriot-Maitland et al., 2014; Judge et al., 2012; Lucre and Corten, 2013). Due to the small sample size, and the associated lack of power inherent in the study, any findings regarding quantitative data are extremely preliminary and should be viewed with caution. Such data should be viewed in light of the fact that the main aim of this study was to determine the feasibility and acceptability of group CFT for this population, rather than establishing efficacy.
Limitations
Given that this was a feasibility and acceptability study, no control group was utilized, nor were any longer-term outcome measures administered. Thus, it is not possible to begin to speculate about the medium to longer-term impacts of this intervention, whether or not any observed changes were due to specific group content or more general group processes, or its effectiveness compared with other adapted psychological interventions for this population. Future studies should consider expanding the number of sessions and group content while retaining a high degree of fidelity to the CFT model, before proceeding to pilot studies (Eldridge et al., 2016).
Other limitations relate to the fact that some of the measures, such as the SCS-SF (Raes et al., 2011), are not yet validated and/or standardized with ID populations. The modifications to the language used in the SCS-SF appeared to result in a tool that is understandable and accessible to individuals with mild ID. However, there are some theoretical problems with the SCS-SF (Muris and Petrocchi, 2017), coupled with the fact that it does not assess/measure the flow of compassion, that render it problematic as a valid measure of compassion. Future studies should seek to psychometrically validate this measure, and/or develop or adapt other compassion measures, for ID populations. Equally, this study did not utilize any direct measures of shame and self-criticism, mainly due to there currently being no such validated measures developed or adapted for ID populations. Future studies may wish to seek to develop and validate appropriate measures of shame and self-criticism for this population.
Conclusion
The findings from this study suggest that CFT groups specifically adapted for adults with mild ID are safe, feasible and acceptable. The mixed methods design provides promising support for the notion that compassion can be taught and cultivated in adults with mild ID through the CFT model and that this maybe a promising method of intervention to ameliorate complex psychological difficulties in these individuals. Future studies utilizing greater numbers of participants and further adaptations to the group structure and content are required, before conducting pilot studies in preparation for randomized controlled trials against other adapted group-based interventions for adults with ID.
Footnotes
Authors’ note
Neil E Clapton is currently affiliated with Avon and Wiltshire Mental Health Partnership NHS Trust.
Acknowledgements
The authors wish to thank all participants and their supporters/carers for their vast contribution to this research. Thanks to David Oakley and Natalie Boulton (Trainee Clinical Psychologists) for co-facilitating groups and focus groups. Additionally, the authors are grateful to Professor Paul Gilbert for his kindness and generosity in allowing us to adapt the CFT model, and permission to use his work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.