
Abstract
Background
Menstruation can be complex and challenging to manage, including for those with intellectual disability. People with intellectual disability experience additional barriers that prevent adequate access to information and support. Parents play an important role in supporting young people with intellectual disability with menstruation.
Objectives
The aim of this study was to explore parental experiences and identify areas of complexity associated with menstruation for their young people with intellectual disability to guide the development of priority supports.
Design
A qualitative interview study to deeply explore the rich experiences of parents.
Methods
Parents of young people with intellectual disability were interviewed about their experiences of supporting their child’s menstruation, including their decision-making processes and information and management needs. Data were analysed using inductive reflexive thematic analysis with NVivo software.
Results
The sample comprised 16 parents (all mothers) who discussed 17 young people with intellectual disability (10-25 years). Five themes were constructed: (1) Setting up for success (establishing positive menstruation attitudes), (2) Competing priorities (wellbeing, convenience, and inclusion prioritised over menstruation), (3) Support from multiple avenues (support from different people, professions, and organisations was important) (4) Protecting dignity and safety (concerns about sexual abuse, pregnancy, distress, socially unacceptable behaviours, and pain), and (5) There is more to be done (information and attitudes need to be improved).
Conclusions
It is important to understand the menstruation experiences and needs of parents of young people with intellectual disability because of management uncertainty and complexity. This study contributes to an under-researched field and can inform changes to better support families including much needed information and education.
Plain language summary
Managing menstruation (period) can be difficult. It can be even more challenging for people with intellectual disability and their families because of limited information and support. Parents play an important role in supporting young people with intellectual disability with menstruation. In this study, we aimed to understand what parents do and what they need to manage menstruation with their young person with intellectual disability. We interviewed 16 parents of young people with intellectual disability about what they do, how they make decisions, and what information and support they need. We analysed the interviews using a reflexive thematic analysis. The information was organised into five themes: (1) Setting up for success (creating positive menstruation attitudes), (2) Competing priorities (wellbeing, community inclusion, and convenience often prioritised over menstruation), (3) Support from multiple avenues (e.g., support from different people, professionals and groups was important), (4) Protecting dignity and safety (concern for sexual abuse, pregnancy, distress, socially unacceptable behaviours, and pain), and (5) There is more to be done (information and attitudes need to be improved). This is important information that can be used to create resources, programs, and practices to better support people with intellectual disability and their families manage menstruation.
Introduction
Menstruation is an important developmental milestone for young people. Managing menstruation can be challenging and especially complex for people with intellectual disability who may experience greater associated emotional, behavioural, physical, sensory, and psychological difficulties.1–3 The ratification of the United Nations Convention on the Rights of Persons with Disabilities 4 in many countries globally sanctions the right for people with intellectual disability to be involved in decisions that affect their life, including decisions about menstruation. However, people with intellectual disability have historically had limited control over their menstruation and reproductive rights and restrictive and invasive management strategies have been commonly used.5,6
People with intellectual disability can experience challenges related to menstruation. 7 For example, communication differences can result in menstrual pain going unrecognised and untreated, 2 which is problematic because premenstrual syndrome and painful menstruation are more common for people with intellectual disability compared to those without. 8 Additionally, difficulties using and dislike of menstrual products can result in risk of poor health outcomes such as genitourinary infections and lead to exclusion from social and school activities.9–11 People with intellectual disability can also experience anxiety, shame, and confusion around menstruation when adequate information and support is not provided. 5
Health literacy is the ability to identify, understand, evaluate, and implement strategies that promote and maintain health and wellbeing. 12 People with intellectual disability experience barriers to developing health literacy skills including limited access to relevant health information and education.13,14 Menstruation education tends to be limited and restricted to anatomical information, omitting practical management skills. 15 People with intellectual disability receive less health education than their peers without disability, and have less opportunities to learn informally from peers, resulting in poorer menstruation knowledge.16–18
Parents play a pivotal role in advocating for and managing the health of young people, with and without disability. The health literacy of parents is important in managing and making decisions to support their families wellbeing; however, gaps have been identified in parental menstruation knowledge. 9 Adequate menstruation knowledge of parents has been associated with a reduction of invasive and restrictive practices for people with intellectual disability. Such practises include involuntary hysterectomies and use of long-term contraceptive medical intervention such as Depo-Provera injections for people who are not sexually active.6,19 Parental support to involve people with intellectual disability in personal healthcare can lead to their child developing positive mental and physical health outcomes and greater quality of life.13,20,21 However, managing menstruation can be challenging for parents of people with intellectual disability and can lead to stress, anxiety, and depression. 5
Little is known about parental experiences of managing menstruation with young people with intellectual disability, particularly regarding information needs and decision-making considerations and processes.18,20 This information is important because of the lack of education resources to assist parents in their approach to menstrual management. 19 Contributing to this literature could improve knowledge and support around menstruation resulting in better health outcomes and quality of life for young people with intellectual disability.13,18 In this study, we aimed to explore parental experiences of supporting young people with intellectual disability with menstruation focussing on decision-making practices and information and support needs. This information will improve awareness of challenges and needs as well as identify priority areas for future resource development.
Method
Ethical approval was obtained through UWA Human Research Ethics Committee (2021/ET000902) and reciprocal ethics was granted through the Curtin Human Research Ethics Committee (HRE2025-0287). The exploratory nature of this study called for a qualitative research design that facilitated the collection of rich data 22 in an under-researched topic. We adopted a strengths-based approach, with researchers valuing the capabilities, experiences, and perspectives of families. The team included experienced researchers in the field of disability. One of the researchers is a parent of a young person with intellectual disability and was involved in shaping the study aims, design, and analysis interpretation.
Participants
Participants were eligible to take part if they resided in Australia and were the parent or caregiver of a person with intellectual disability who had previously or was likely to soon menstruate and was aged between 10 and 25 years (no other criteria applied). A range of purposive sampling processes aimed to capture a diverse sample including those from metropolitan and regional areas with a range of child diagnoses, communication modes, mobility levels, and support needs.
This study’s sample size was determined through consideration of information power and not data saturation. Braun and Clarke are critical of using data saturation as a means of determining sample size especially for a reflexive thematic analysis study (as used in this study) and recommend information power as a more useful and theoretically complementary framework. 3 A sample of approximately 15 participants was considered adequate to achieve information power because of the rich knowledge of parents and depth of analysis. 23
Potential participants were recruited from three databases housed at The Kids Research Institute Australia 24 (11 of 13 contacted were available to participate) and through study advertisements (five of eight who made contact were interviewed). JK (PhD; female researcher with experience conducting research interviews in disability research) explained the study by telephone, and if interested, an interview was scheduled. All participants were interviewed once on their own; one parent discussed two young people with intellectual disability in the interview.
Materials
A 5-minute pre-interview Qualtrics (https://www.qualtrics.com) questionnaire was used to identify demographic information to help understand and describe the sample. Questions queried the child’s communication mode (clear or difficulties with verbal communication, assistive technology, or non-verbal),25,26 mobility level (no difficult or difficulty walking and running, assisted walking or unable to walk), 27 and support needs (independent, little support required, significant support needed, and dependent).25,26 This information informed how the interviewer approached interviews and allowed them to be responsive to the young person’s context.
The semi-structured interview guide was designed collaboratively by drawing on interview guides previously used by the team to explore parent experiences, decision-making processes, and needs when supporting young people with intellectual disability with their menstruation. Open-ended questions were designed to explore parental experiences of managing menstruation with their child. First, participants’ general experiences were explored including discussion of pain, behaviour, and product use. Second, decision-making was discussed including medical interventions, parent considerations, and the level of their child’s involvement. Finally, participants were asked about their experiences and needs relating to information and support. Probing questions were asked to clarify answers and further examine perspectives and experiences. The interview guide is included in the
Procedure
The planning and preparing phases of this study took place between March and July 2025. Before the interview, each parent was emailed the participant information sheet, interview guide, a link to the pre-interview questionnaire, and a Microsoft Teams invitation. The online questionnaire was completed before the interview and informed consent was obtained verbally and audio recorded at the beginning of the interview. JK conducted the first two interviews with EK (female psychology honours student with experience working with young people with disability). EK conducted the remaining interviews, having frequent discussions with JK and LJB (PhD; female psychologist and senior researcher with experience conducting research interviews across a variety of health and disability research areas) and getting periodic feedback from the broader team. Online interviews were conducted from The Kids Research Institute Australia, or EK’s home office and ranged from 41 minutes to 73 minutes (M = 58 minutes) in duration and took place between July and August 2025. Field notes were taken throughout. Microsoft Teams was used to audio record and transcribe interviews, which EK checked for accuracy against the recordings. Participants were compensated for their time with an honorarium.
Analysis
Data were analysed using a reflexive thematic analysis, a method that enables the identification and categorisation of data into themes.
28
Braun and Clarke proposed six phases in reflexive thematic analysis: (1) familiarisation with the data, (2) generating initial codes, (3) developing initial themes, (4) reviewing themes, (5) refining and defining themes, and (6) writing the report.
28
NVivo (10th ed., QSE International Pty Ltd., Burlington, MA) software was used to aid analysis. The analysis began while interviews were taking place in August and was completed in October 2025. Codes were inductively (i.e., data-driven) and systematically developed from the data representing aspects of meaning related to the research question by EK. A second coder (AA; speech pathologist with post graduate qualifications and clinical experience working with young people with disability) independently coded two transcripts before meeting with EK and comparing coded transcripts, exploring code definitions, and reconciling minor differences. Codes were collated into potential themes that were frequently reviewed by the team to ensure they were clear, comprehensive, and representative. An initial thematic map generated by EK was discussed by the team, which led to further refinement and consolidation of themes. For example, the codes ‘Pain’ and ‘Potential for Conception’ were merged into ‘Protecting Dignity and Safety’ due to the underlying consideration and concern for the child’s comfort and safety. The final coding tree is included in the
Trustworthiness
We used several strategies to optimise the analytical and interpretative trustworthiness of the study. Credibility was enhanced by including some participants that have previously engaged in other components of the broader project, to build on established relationships and rapport.
29
Additionally, reflexive journalling and team discussions allowed researchers to reflect on their positionality and its impact on analysis. Reflexive journalling also heightened confirmability together with thorough note taking on the methods and decisions made to ensure that the process was transparent.
29
Further, participants were emailed a summary of the findings as a form of member checking and asked to provide general feedback. Five participants responded and all feedback was positive and confirmed data interpretation. Reporting clear recruitment strategies and providing a detailed description of the sample improved the study’s transferability, as information can be used to assess the applicability of findings to other research and populations.
29
An audit trail was kept including extensive notes on meeting summaries and coding processes (e.g., minor changes to code definitions as new data influenced the scope of meaning) which allows for study replication and increases dependability.
29
Braun and Clarke’s
30
15-point checklist for a good thematic analysis (included in the
Results
Demographic information of participants’ children with intellectual disability.
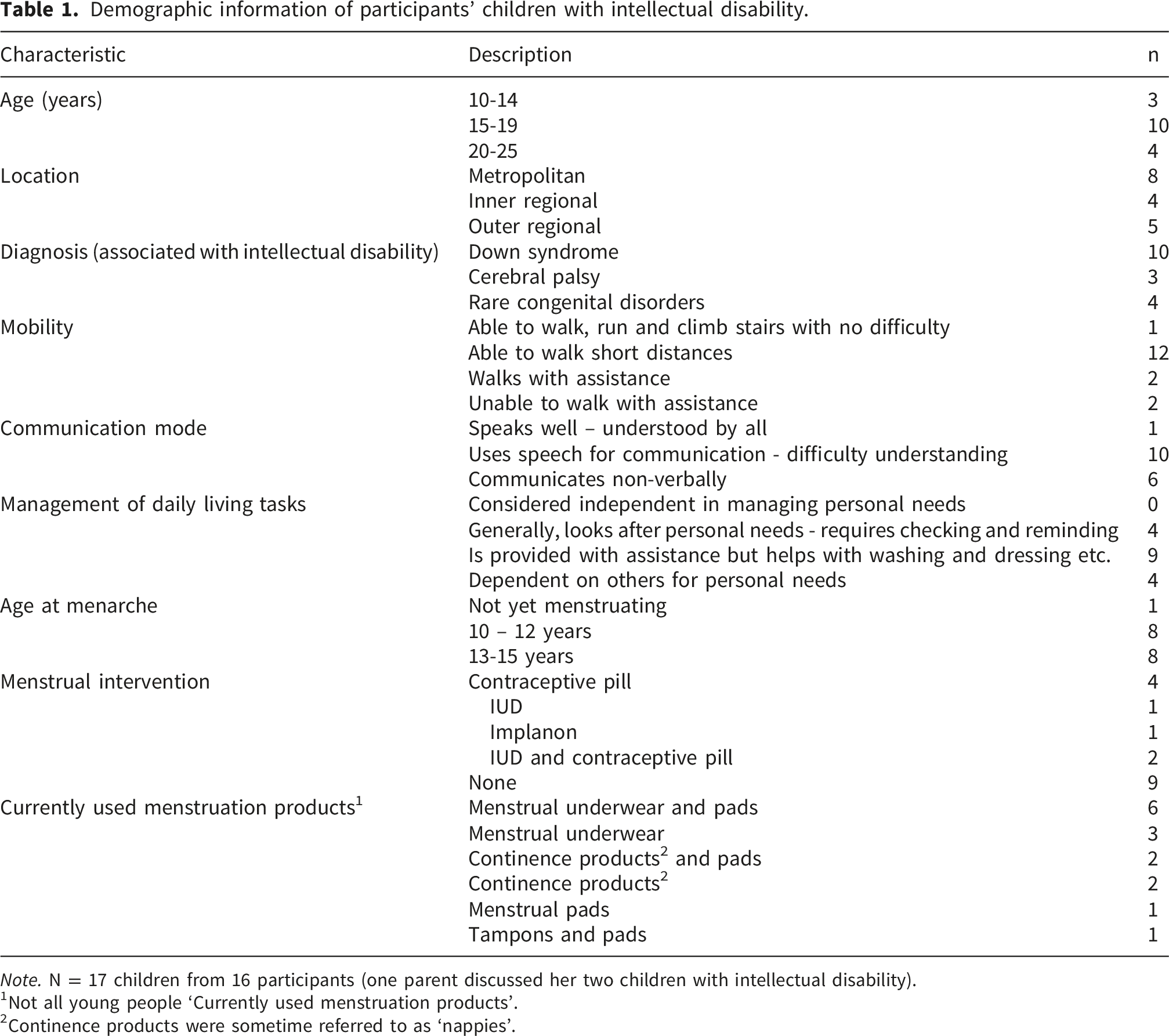
Note. N = 17 children from 16 participants (one parent discussed her two children with intellectual disability).
1Not all young people ‘Currently used menstruation products’.
2Continence products were sometime referred to as ‘nappies’.
The analysis resulted in five themes: (1) Setting up for success, (2) Competing priorities, (3) Support from multiple avenues, (4) Protecting dignity and safety, and (5) There is more to be done. The relationship between these themes is depicted in Figure 1. Setting up for success underpins the experience of menstruation management by laying a foundation of positive menstrual attitudes and knowledge that influences the other themes. Support from multiple avenues was central to parent experiences and connected and related to the themes of Competing priorities and Protecting dignity and safety. There is more to be done is a theme that outlines opportunities to improve support. Participant numbers are assigned to the quotes below to demonstrate the range of perspectives represented. Thematic map depicting parents’ experiences of menstruation management for their child with intellectual disability.
Setting up for success
Parents highlighted the importance of modelling positive attitudes towards menstruation and implemented strategies to promote optimal menstrual management and support their child’s emotional wellbeing and quality of life. Parents reported demonstrating relaxed attitudes to normalise menstruation. One parent reflected that it was important to “not get... panicky, or overanxious about their [child’s] period” adding that, “if you act like that, your child’s going to act like that, too” (P11). Another parent discussed the importance of openly sharing information saying that: Having those conversations around [the young person] just to like, really normalise, you know, the fluctuation in mood and how our body’s feeling and that it’s quite normal, yeah. Just those kind of things and she’s not getting those conversations elsewhere. But she’s not having them with peers, she’s not, you know, being able to Google stuff on her own. So, I’m kind of like you know, that’s one of her main sources of information (P4).
Some parents also celebrated menarche such as with cake, “like it was a birthday” (P3) and as “an exciting moment” (P11).
Parents discussed how taking an individualised approach to menstruation information and education was beneficial and that they often considered their child’s functional and sensory needs when making menstruation product decisions. Some parents described period underwear as “quite good” (P5) when their child did not have the dexterity to use pads or tampons independently or when seeing blood on a white pad would be considered “graphic” (P3) and potentially disturbing for the young person.
Competing priorities
Parents discussed weighing up competing priorities in their lives and often prioritised ease and their child’s well-being over other considerations such as menstruation. Some parents discussed medically suppressing their child’s menstrual bleeding when they perceived menstruation as an unnecessary challenge for themselves and their child. One parent of a young person who had not started menstruating discussed how they were contemplating medically preventing bleeding, saying that “due to her being in nappies, we are considering that once her period starts, we will do something to stop it” (P8). When discussing anticipated challenges, the same parent mentioned concerns relating to “pain and it will be messy” (P8). Referring to menstruation and people with intellectual disability, one parent explained that “for our guys, it’s a lot to take on” adding that “life’s tough enough for them usually” (P1).
Participating in preferred activities was also often prioritised above menstruation. Some parents discussed the impact of menstruation on their child’s ability to participate in water-based activities and therapies. One parent described how her daughter underwent hydrotherapy as a form of pain relief and explained that not being able to participate due to menstruation “definitely affected her...greater wellbeing” (P14). Menstruation swimwear was sometimes discussed as an alternative in the water, as using tampons was often considered an impossible and impractical “nightmare” (P14).
Managing menstruation related behaviours and emotions was often a significant consideration. Parents described wanting to avoid any potential additional menstruation related behaviour difficulties that could arise from alternative management methods saying, “it’s not broken, so don’t try and fix it” (P4). When there were no immediate issues, parents tended to prioritise behaviour regulation over exploring menstruation management alternatives.
Support from multiple avenues
Engaging with different networks of support had a significant impact on how parents managed their child’s menstruation in a range of areas (e.g., product use, education approaches, medical interventions). Parents found support from multiple personal and professional networks, including family members, medical professionals, other parents, and online forums. Parents particularly valued the support and understanding they received from other parents of young people with intellectual disability saying, “we’re all in this together” and adding, “if you’re not part of a community, it’s so much harder” (P9). Some parents reported not having those social supports. For example, one parent said, “I don’t really have that network around me, unfortunately” (P15) and instead had to conduct her own research and rely on medical support and information rather than personal networks.
Parents reported that it was important to find suitable professional support for their child and that effective communication often played an important part in what made that support successful. Healthcare professionals who “actually talked to [the young person]” (P10) were valued as good communicators who facilitated their child’s involvement in the medical processes and decisions around menstruation. Another parent described a time when they had an effective sexual health therapist saying, “we had a really great therapist who was incredible with nonverbal communication. [The young person] was really engaged. She used a lot of resources, lots of pictures. Talked to [the young person] gave her lots of really good processing time” (P16). However, they stopped using the service with a different therapist who “didn’t have the same kind of skills to communicate” (P16). Another parent of a young person living in supported accommodation reported that a lack of communication was an important part of what made the provided care inadequate saying, “No, I definitely don’t get any information, that’s completely dropped off. The whole support had really dropped off” (P4). The parent was concerned in relation to her child’s menstruation saying, “I don’t get anything (information) and that may be why I think that she hasn’t had any breakthrough bleeding for 5 years or so years because I’m not being told.”
Many parents reported seeking information in preparation for menarche which they shared before or after bleeding commenced. One parent explained how they sought support from their occupational therapist who provided social stories that were implemented once menstruation started, saying when “the physical evidence of periods was there, it would become more real for her...I didn’t attempt to present her with social stories prior to it” (P11). This parent sought professional assistance to support her child in the way that complemented her learning style and avoided distress.
Mothers were generally the primary source of menstruation support for the young person; however, some fathers also had a role. Examples of involvement included taking part in or supporting decision making, changing and cleaning menstruation underwear and products, and supporting their child independently. Some parents emphasised the need to educate fathers on how to manage menstruation and “educate them on what’s normal” (P16) to improve the support provided.
Protecting dignity and safety
Parents reported that managing and making decisions around their child’s menstruation was a significant responsibility sometimes involving decision making around avoiding invasive treatments, managing pain, and minimising the risk of sexual abuse and pregnancy. A major consideration for parents, was limiting interventions that were perceived as potentially harmful or invasive. Some parents weighed up the risks and benefits of using the contraceptive pill to manage menstruation. One parent described having “concerns about...chemically altering the body,” explaining “I’d have reservations about the pill” (P6). Many parents aimed to reduce the likelihood of their child experiencing undesirable outcomes, selecting medical interventions that provide the “least amount of invasiveness for the maximum amount of benefit” (P16).
Communication about pain was a concern for many. Some parents reported that their child did not clearly communicate their pain generally and in relation to menstruation and were concerned that they were “actually in more pain than we know” (P13). Many parents reported providing analgesic medications (e.g., paracetamol, ibuprofen) as a preventative measure to relieve potential menstruation-related pain.
Medical menstruation management was also discussed in relation to sexual abuse. The heightened risk of sexual abuse was “a frightening thing to hear as a parent” (P10). One parent described considering the implementation of the IUD because “the thought of [the young person] having to manage an unplanned pregnancy is beyond what I want her to have to endure on top of any abuse” (P5).
Using contraception to manage menstruation was often considered in relation to potential pregnancies. Parents generally reported that contraceptives were used to manage menstrual bleeding but considered “the added benefit of contraception” (P5) as an important factor influencing this decision. However, one parent discussed her child’s right to conceive, saying “childbirth’s not really something we’re kind of looking at, but still, it’s not my decision, is it” (P7).
There is more to be done
Parents discussed priorities for improving menstruation support and management for young people with intellectual disability, including healthcare professional attitudes and information access and delivery. Although parents were generally satisfied with the support they received from medical professionals, they reported some instances where a lack of awareness and understanding of people with intellectual disability was displayed. Parents reported that some healthcare professionals held outdated views about people with intellectual disability, which limited the application of point of care activities with a person-centred care framework. One parent shared that these attitudes could be addressed by healthcare professionals maintaining current knowledge by “seeking out fresh information” (P11). It was also detrimental when healthcare professionals did not accommodate the individuals needs such as those associated with communication differences and provide adequate time for genuine involvement in conversations and decision-making processes. For example, one parent said, “it’s a very rare occasion that a medical professional will give her enough time to process the information” (P16).
Parents reflected on the menstruation information available and how it could be improved. Some parents reported that the young person had taken part in peer-to-peer sexual health education groups and reported the benefits of informal conversations. Parents reported that some “formal resources are incomplete and leave a lot to be desired” (P9), and that knowing where to find information can be difficult. Parents wanted resources to support how they could discuss menstruation with their child, for example, “maybe more like prompts for parents ... on how they could, you know, approach the subject” adding that “that sort of thing would be really useful I think with parents or families” (P13). Others suggested the use of videos and online content that could be visually engaging and accessed by the individual more independently. Parents reinforced the need to individualise this educational approach to suit the support needs and interests of young people with intellectual disability.
Discussion
This qualitative study explored how parents educate, support, and make decisions about menstruation for and with young people with intellectual disability. Data were analysed using inductive reflexive thematic analysis. Five themes were developed: Setting up for success, Competing priorities, Support from multiple avenues, Protecting dignity and safety, and There is more to be done.
In this study, parents discussed modelling positive attitudes to shape their child’s perceptions of menstruation. Some parents reported celebrating their child’s menarche and marking it as an important life event, as has been shown in previous research. 32 Having positive attitudes towards menstruation has been related to better menstruation management. 33 Part of developing these positive attitudes included taking part in open discussions and providing education. Many young people with and without disability are not aware of or educated on menstruation at the point of menarche.8,32,34 This lack of understanding can result in the experience being frightening and lead to misconceptions, shame, and poor management.8,32,35 Demonstrating positive attitudes and providing information and education can support young people with intellectual disability to understand and manage their menstruation more effectively. Future research and educational resources should seek to assist parents to create environments and discuss menstruation with the young person in a way that supports positive attitudes.
Parents reported wanting to navigate menstrual issues and prioritise outcomes that would avoid causing their child pain, distress, or increase exclusion. Swimming was described as a social and therapeutic activity that could be prevented by menstruation management difficulties. Other research has reported negative impacts on well-being as a result of menstruation related exclusion from school, sport, and community participation.10,11 Consequently, parents in the current study often opted to medically suppress menstruation using a contraceptive implant, pill, or intrauterine device to prioritise their child’s comfort and inclusion and avoid difficulties. Other research has reported the use of medical suppression and sterilisation when parents have found managing their child’s menstruation difficult or overwhelming and when experiencing menstruation is not thought to benefit the individual. 35
Despite some parents in the current study valuing medical management of menstruation to manage pain and increase ability to participate in activities and therapies, there remains a tension if the young person is not involved in the decision-making process. People with disability have the right to be involved in decisions that affect their life, including those associated with menstruation 4 ; however, opportunities for involvement are not consistently provided. 13 The legal requirements for young people to be able to make medical decision differs depending on the individual’s age and location 36 ; however, all people, regardless of impairment should be involved. 4 Involvement does not always have to constitute making the decision, and there are other ways young people can be involved such as being informed, having their perspectives considered, and making low-risk decisions around larger medical ones. Long-term contraception without the knowledge or permission of the person is considered a form of involuntary sterilisation by some in the field who argue that the person as well as families, health professionals, and advocates should be involved in the decision-making process. 6 Beyond initial decision-making processes, the implementation of menstruation suppression itself is complex in terms of optimising the individual’s quality of life without restricting their human rights. Problematically, parents’ difficulties in managing menstruation are often valued above those of the person with intellectual disability resulting in the convenience of the family being prioritised above the dignity of the individual. 5 Understanding how to enhance involvement in decision-making processes while continuing to honour essential roles family play in supporting decision making is integral to achieving the fulfilment of the rights people with intellectual disability.
In the current study, parents strove to protect the dignity and safety of the young person by maintaining privacy, managing pain, and preventing pregnancy. Sexual abuse was a significant concern, influencing decision-making around product use and medical intervention. While estimates of rates vary and are likely underestimated, the literature suggests that the risk of sexual abuse for children with intellectual disability is two to ten times higher compared to those without 37 and is often a concern for parents in relation to menstruation.11,19,38 In this study, parents expressed worry that requiring assistance with menstruation products would put the young person in situations where sexual abuse was more likely to occur. Some parents attempted to navigate this risk by using period underwear that can be used more independently or suppressing bleeding through medical interventions. Further, health literacy has been identified as a protective factor for sexual abuse because understanding appropriate touch and accurate anatomical vocabulary can lead to the development of stronger protective behaviours and increased reporting ability.11,18 Future research should explore how to enhance menstruation health literacy for people with intellectual disability to protect against sexual abuse.
Parents reported that receiving support was an important factor in managing their child’s menstruation successfully. Gaining support through multiple personal (e.g., family and other parents of young people with intellectual disability) and professional (e.g., GPs, occupational therapists) avenues is considered beneficial and increases access to resources and interventions that enhance the ability to manage health and wellbeing.24,39 Previous research has identified that social support is important for families of young people with intellectual disability in providing health information and practical advice 24 and protecting against caregivers becoming overwhelmed. 40 However, discussions of menstruation can be considered socially and culturally inappropriate reducing opportunities to access social support.11,41 Stigma is associated with both menstruation and disability, further restricting opportunities to access support.11,35,41 Future research should identify facilitators and barriers of accessing support, including stigma-reduction, to inform ways to help families to make and sustain social connections.
As has been shown in previous research, parents identified a lack of engaging and accessible menstruation educational resources for themselves and their child.19,41 In this study, parents recommended taking a personalised approach to achieve accessibility in peer-supported educational programs, instructional videos, and Easy-Read information (https://www.inclusionaustralia.org.au/wp-content/uploads/2023/04/A-Guide-to-Commissioning-Easy-Read-Resources.pdf). The development of these resources should be informed by accessibility guidelines to create accessible materials with families and young people with intellectual disability to optimise their meaningfulness. 42 Research suggests that menstrual health education should be evidence-based, engage multiple senses (e.g., visually engaging, tactile) and take a stepwise approach to learning. 5
Although parents reported generally feeling supported by healthcare professionals, they also discussed instances where deficit-based attitudes were displayed, information was not addressed to their child, or adequate time was not provided for meaningful engagement. The Royal Commission into Violence, Abuse, Neglect, and Exploitation of People with Disability 43 in Australia recommended that healthcare professionals have further disability training during their formal education and throughout their careers to support the implementation of models of care suitable for people with intellectual disability. 44 Having access to comprehensive and quality information and training for people with intellectual disability, their families, and healthcare professionals can optimise communication and engagement and improve menstruation management and should be advocated for.
Strengths and limitations
This study makes an important contribution to an under researched area, expanding on knowledge of the experiences of parents managing menstruation with and for young people with intellectual disability. The sample included participants from a range of locations across metropolitan and regional areas of Australia and was diverse in terms communication modes, mobility levels, and support needs of the young people discussed resulting in the inclusion of a broad scope of perspectives and experiences.
This study had some limitations. Volunteer bias may impact outcomes and transferability 45 in that parents who are well informed and who hold positive perspectives on menstruation and research participation may be more likely to volunteer to participate than others. Only five parents responded to our request for feedback on the analysis summary. Although feedback was positive and confirmatory, we do not know if those who did not respond were also satisfied or, if not, or how their feedback might have shaped our interpretations.
A majority of the sample were parents of young people with Down syndrome suggesting that these viewpoints may be overrepresented. However, the young people with Down syndrome represented a range of impairment severity in communication and independence in managing activities of daily living that may reflect a wider population with intellectual disability. Additionally, other perspectives and considerations were not included (e.g., the sample did not include fathers, people in other caring roles, and socio-economic or employment information were not collected). Consequently, the findings represent a subset of perspectives and future research should seek to explore a broader range of viewpoints including large representative quantitative studies to determine generalisable experiences. Most importantly, although the focus of this study was on parental experiences it is also critical to understand those of people with intellectual disability. Future research should further seek to understand the experiences, perspectives, and needs of young people with intellectual disability to identify ways to best provide education and support. Additionally, it would be valuable to investigate how experiences, perspectives, and needs change over time (e.g., with greater independence) and later in life (e.g., menopause) to enhance support opportunities and resourcing across different groups.
Conclusion
This study provides novel insights into how parents of young people with intellectual disability manage menstruation with their child. Practices within education, community, and advocacy settings should navigate the impacts of menstruation management challenges on participation (e.g., swimming), safety (e.g., sexual abuse) and families (i.e., providing menstruation support). Further, thorough and accessible menstruation education and information is needed for young people with intellectual disability, their parents, healthcare professionals, and carers to improve knowledge, attitudes, healthy management behaviours, decision-making, distress, and stigma. Understanding the unique and complex experiences, decision-making processes, and needs of parents who support people with intellectual disability is an important step towards understanding how to inform and support families to optimise menstrual health outcomes.
Supplemental material
Supplemental material - Understanding parents’ experiences and needs when managing menstruation with young people with intellectual disability
Supplemental material for Understanding parents’ experiences and needs when managing menstruation with young people with intellectual disability by Emily Kearns, Lauren J. Breen, Rachel Skoss, Aasta Abbott, Thom Nevill, Jenny Downs, and Jessica Keeley in Women’s Health.
Footnotes
Acknowledgements
We acknowledge the parents and caregivers who shared their time and experiences with us.
Ethical considerations
This study was approved by The University of Western Australia Human Research Ethics Committee (2021/ET000902).
Consent to participate
Participants provided informed consent before taking part in interviews. Informed consent was obtained from participants verbally and audio recorded before interviews commenced.
Consent for publication
Participants provided informed consent for publication.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Health and Medical Research Council (GTN2015902). J.D. is supported by a Fellowship from the Stan Perron Charitable Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is not available due to confidentiality of participant information.
Artificial intelligence
Artificial intelligence was not used in any way to conduct this research or develop this paper.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.