
Abstract
There continues to be debate over the nature and progression of ovarian endometriomas in adolescence due to the possibility that they may have a different origin and to the impossibility to be able to predict progress.
The hypothesis of a different origin traces its roots in the phenomenon called “neonatal menstruation” (NUB), occurring in approximately 5% of newborn. The retrograde shedding of neonatal endometrium may contain progenitor cells and stroma that may lie dormant under the peritoneal surface until being activated when estrogens begin to rise.
In teenagers, ovarian endometriomas are often preceded by highly angiogenic implants in the fossa ovarica, with adhesion formation resulting in the invagination of the ovarian cortex and the creation of a pseudocyst.
Use of imaging techniques makes it possible to diagnose even small endometriomas. This is vital to their management, since there is evidence that the disease in an adolescent represents a severe condition, with tendency to progression. In addition, if intervention is decided, the first surgical procedure can determine the ultimate outcome of her reproductive life, because there is a significantly higher risk of inadvertently removing ovarian tissue in the presence of an endometrioma than of other ovarian pathologies. For this reason, techniques avoiding additional trauma to the ovary should be preferred and those who wish to become pregnant should attempt conception as soon as possible; if pregnancy is not sought, hormonal therapy is strongly advised.
Finally, young age at diagnosis may constitute a pivotal factor in considering fertility preservation.
Introduction
The nature and severity of endometriosis appearing during adolescence has been the object of a controversy, both in general and for the ovarian variant, that has yet to be resolved. The reason is that, as of today, there is no way to predict in which cases the disease will progress, leading to disagreement on the best approach to management.
Back in 2013, we reviewed existing knowledge of the early-onset variant of endometriosis and identified 12 publications utilizing classification systems allowing proper comparison, for a total of 437 adolescents with laparoscopy-proven disease. We concluded that “endometriosis in adolescents is a hidden, progressive and severe disease that deserves attention, not just compassion” (1). Our conclusion about the “progressive nature” of early-onset disease was not shared by Evers who argued in an Editorial that in the seven published trials where laparoscopy was performed before and after a period without treatment, in 71% of the cases the disease did not progress (2). Two considerations are in order when analyzing Evers’ conclusion. On the one hand, it is clearly impossible to predict in which cases endometriosis will progress; on the other, the investigations upon which Evers based his conclusions were conducted in adult women and, over the last few years, we have argued that there is strong indirect evidence that the adult and the pre-pubertal and adolescent variants of endometriosis may have a different origin and phenotype (3).
According to this hypothesis, early-onset disease traces its roots in the retrograde fetal endometrial shedding occurring in approximately 5% of neonates at the time of birth that is manifested by a well-documented, but neglected phenomenon called “neonatal menstruation” (4, 5). The visible bleeding with retrograde endometrial shedding has the ability to affect pelvic organs and become the source of disorders that may develop later in life and pose a risk for the future reproductive health of the adolescent (3, 6-7-8). We believe that the theory of a different origin of pre-pubertal or adolescent and adult forms of endometriosis is well founded, thanks to a series of investigations carried out half a century ago. At the same time, there can be no proof that neonatal menstruation can represent a valid marker of an increased risk of early-onset endometriosis as long as neonatal uterine bleeding (NUB) remains unregistered. This is all the more necessary when considering that clinico-pathological studies have shown that NUB occurs with increased frequency in neonates after intrauterine stress such as preeclampsia, fetal growth retardation and postmaturity (9-10-11-12).
Until recently, ovarian endometriomas have been considered by most as a disease of adult women: in 1948, Meigs (13) stated that endometrial cysts are not found until 13 to 19 years of menstrual life have elapsed and Parsons (14) noted in 1968 that they very rarely occur in women younger than 20 years. However, in the same period Moore et al (15) presented the case of seven young girls aged 10 to 17 years with large endometriomas, varying in size between 5 and 15 cm. He specified that in three cases they were located on the right, in two on the left and in the last two on both ovaries. Then, in 1976, Roth and Goodner (16) published the case of a 19-year-old girl with an 18 × 11 × 5 cm large endometrioma with minimal symptomatology. They commented on the paradox that a large endometrioma may be an incidental finding at the time of a routine pelvic examination, while the presence of exquisite pain associated with menstruation may be caused by only minimal uterosacral ligament endometriosis.
More recently, evidence has been gathered that when the diagnosis of endometriosis is posed during adulthood, the first symptoms have often started during adolescence or young adulthood (17-18-19), indicating the presence of a substantial diagnostic delay, estimated to vary between 6 and 11 years. This in turn has fathered extensive research on biomarkers for the presence of the disease, so far without any real success. As a result, the suffering continues, while knowledge that an adolescent had a menstruation at birth could raise suspicion, facilitate diagnosis and eliminate delays.
In this paper, we specifically address the ovarian variant of endometriosis, describing first the neglected phase of neonatal menstruation; second, the silent formation of the ovarian endometrioma during early adolescence; and, third the risk of progressive loss of the ovarian function as the ovarian disease progresses.
Origin of adolescent endometrioma
As already mentioned, we have produced indirect evidence that early-onset peritoneal, as well as ovarian endometriosis may have a different origin than the adult variant. Based on this theory, it is plausible that the evolution of the specific phenotype of ovarian endometriomas in adolescence may be different than in adulthood. At the same time, since among teenagers both the NUB and menstrual variants may be present, adolescent endometriomas may vary widely in severity and progression.
The fetal endometrium and its response to progesterone
The new hypothesis draws its origin in the peculiar situation of the fetal endometrium, discovered more than half a century ago by Ober and Bernstein (20) who reported on 169 autopsies of female infants for which sections of the uterus were available. Briefly, 40% of the cases evaluated were full term infants (38 to 42 weeks) of whom the great majority (84%) died within the first 3 days of life and the remaining between day 4 and 14. The remaining 60% comprised almost evenly stillbirths and premature infants (32 to 38 weeks). In 68% of the cases with a uterine specimen, also sections of one or both ovaries were available. Of importance is the fact that causes of death were known and no correlation between the cause of death and the condition of the endometrium or the ovaries could be established. In view of the fact that throughout pregnancy fetal endometrium is exposed to ever increasing circulating levels of progesterone, the pathologists were looking for secretory activity and decidualization. The first was defined as the presence of subnuclear and supranuclear vacuolation of the cytoplasm in the cells of one or more glands. On the other hand, they defined decidualization as an increase in the cytoplasmic substance of stromal cells with a tendency of these cells to form a pavement or mosaic. The authors found that in the eight cases with progestational endometrium, three showed stromal decidualization. Therefore, there was no implication that the bleeding was a response of the endometrium to cyclic changes in hormonal balance.
The sections of the ovaries were evaluated in terms of follicular development with formation of an antrum in the proliferated granulosa cells, or for cyst formation the presence of a cavity over 2.5 cm in diameter and the flattening of the cells lining the cyst. The presence of antrum formation as a stigma of gonadotropic (hCG) action was the one observation which was most consistently found. The study showed a lack of any positive correlation between the changes seen in the ovaries and those seen in the endometrium and led to the conclusion that the endometrium response was unrelated to ovarian changes.
In the same year, Rosa (21) published his investigation of fetal endometrium, concluding that physiologic changes during fetal life mimic a long menstrual cycle, resulting in either no or interstitial bleeding; rarely, changes progress to endometrial luteinization followed by shedding as seen in a true menstruation.
These histological observations are important as in clinical practice the occult bleeding may represent interstitial bleeding and should be distinguished from the visible bleeding which represents true menstruation.
Retrograde neonatal bleeding and risk of endometriosis
There is evidence that in the approximately 5% of cases with visible NUB, retrograde pelvic shedding can occur. Indeed, an autopsy study of a newborn with McKusick-Kaufman syndrome documented the presence of serosal implantation of endometrial epithelium with rapid formation of pelvic adhesions (22). In addition, there is evidence that endometrial cells and stroma (most likely stem/progenitor cells) lying dormant under the peritoneal surface (6), can be activated as soon as estrogens begin to rise producing, in exceptional cases, endometriotic lesions even before menarche. Indeed, Gogacz et al (23) have described the presence of adhesions and of an 8-cm large endometrioma lined by endometrial epithelium and stroma with hemosiderin-laden macrophages in the left ovary of an 11-year-old premenarcheal girl.
Recently, Schuster et al (24) described a fetus of 38 weeks with a thin-walled cyst adherent to the ovary with no evidence of endometriosis in the pelvis. The histological findings were consistent with a hemorrhagic cyst with focal endometriosis, although they were not typical of an ovarian endometrioma.
The existence of a variant finding its roots in neonatal bleeding is supported also by cases of perimenarcheal peritoneal endometriosis. In 2005, Marsh and Laufer (25) described the case of five premenarcheal girls with chronic pelvic pain in whom at laparoscopy clear, red, and/or white lesions consistent with endometriosis were found. Microscopic evaluation of biopsies of the lesions confirmed the diagnosis. They concluded that “the presence of lesions visibly consistent with endometriosis in premenarcheal girls without an obstructive anomaly supports the concept that some cases of endometriosis may result from an etiology other than retrograde menses”. We believe we have identified the origin of these forms.
Endometrioma in the adolescent and young woman
Pathophysiology
In a review, Hufnagel et al (26) described the results of recent studies documenting the role of stem cells in the etiology and pathophysiology of endometriosis. These investigations indicate that stem cells are critical to the cyclic regeneration of a healthy endometrium and have documented the presence of a stem cell population within the endometrium. Both endometrium-derived and bone marrow-derived stem cells can migrate to ectopic sites and contribute to the development of endometriosis and even modify the eutopic endometrium of these subjects. In addition, it seems that both progenitor cells within the endometrium and multipotent cells from bone marrow contribute to endometrial growth. In this respect, it is well-known that, while the functional layer of the endometrium is shed in each menstrual cycle, the basal layer remains intact and Schwab et al (27) observed no significant difference in clonogenicity of epithelial and stromal cells between proliferative, secretory, and inactive endometrium. This means that even the inactive endometrium contains clonogenic cells and that the basal layer of the endometrium may be an important source of endometrial progenitor cells.
Under the circumstances, several obvious overall questions remain. First, why is endometriosis restricted to less than 10% of menstruating women? Second, does the phenotype of endometriosis change with age with subtle, red angiogenic peritoneal lesions and occasionally the formation of ovarian endometriomas in the adolescent, and endometriomas with a thickened fibrotic wall and deep, fibrotic peritoneal lesions in the adult? Third, is NUB the result of spontaneous decidualization caused by chronic fetal distress during the third trimester of pregnancy (28)? In this regard, the study of Lévy et al (9) showed that NUB occurred more frequently in fetuses of women with preeclampsia and fetal growth restriction. One point worth mentioning is that, although neonatal bleeding represents endometrial shedding and has been described as a true menstruation, the type of endometrium shed in NUB is likely to be different than that in the cyclic menstruation. This phenomenon could explain not only the incidence of endometriosis, but also the different phenotype of adolescent disease.
In teenagers, ovarian endometriomas are often composed of highly angiogenic endometrial implants in the fossa ovarica, with adhesion formation following recurrent bleeding and resulting in the invagination of the ovarian cortex with the formation of a pseudocyst in a plastic ovary. The fact that the endometriomas in infants and adolescents tend to be large probably reflects the absence of fibrosis in the ovarian cortex allowing expansion and increase in size depending on the bleeding episodes.
At the molecular level, Filippi et al (29) investigated gene expression of hypoxia-inducible factors (HIF) 1/2α, protease-activated receptors (PARs) 1/4, and vascular endothelial growth factor (VEGF)-A by quantitative reverse-transcription polymerase chain reaction. Ovarian endometrioma expressed high levels of HIF-1/2α, PAR-1/4, and VEGF-A, while deep endometriosis did not show significantly different gene expression compared to endometrium from unaffected women. The examination of the aberrant microRNA (mRNA) expression profile responsible for changes in angiogenesis in endometriotic lesions has shown that the higher angiogenic and proteolytic activities in the eutopic endometrium of subjects with endometriosis might facilitate implantation of endometrial cells in subjects with an ovarian endometrioma (30). This phenomenon seems evident in the ovarian endometrioma in young women. Yerlikaya et al (31) attempted to identify genes and biological pathways that contribute to angiogenesis in the eutopic endometrium, the peritoneal environment and ectopic cells and stroma during the formation of ectopic nests. The observation that angiogenic factors are differently expressed in the unaffected peritoneum of women with endometriosis compared to women without the condition explains how an ovarian endometrioma can develop from a superficial peritoneal lesion adherent to the ovary, through an invagination of the cortex and the formation of the endometrioma cavity.
Clinical presentation
We have mentioned the possibility that the two variants of endometriosis may coexist among adolescents and show different severity. In this respect, since dysmenorrhea has been the main indication for laparoscopic investigations, this may have influenced the early findings of predominantly subtle superficial lesions in adolescents. It is a fact that until recently, endometriomas in adolescents were not identified unless they were present as large ovarian cysts (1). Today the minimum diameter suggested by the European Society of Human Reproduction and Embryology (ESHRE) guidelines to warrant intervention is 3 cm; this however has been arbitrarily chosen on the assumption that below that size an image may represent a dysfunctional hemorrhagic cyst (32). In addition, severity of endometriosis has been described according to the revised American Fertility Society (rAFS) classification system. Unfortunately, this staging classification system may not reflect the specific pathology of pelvic organs involved such as the ovaries. The unsatisfactory state of diagnostics in the case of early-onset ovarian endometriosis is exemplified by a remarkable observation made by Yang et al (33) showing a difference in the proportion of cases of severe endometriosis between adolescent cohorts published in Western and Asian countries. In this respect, it is precisely the use of the rAFS classification that makes it impossible to establish whether the difference involves the ovarian localization.
Fortunately, today, the use of imaging techniques makes it possible to diagnose an increasing number of even small ovarian endometriomas. This reality deserves full attention since, although progression of the disease is unpredictable and therefore expectant or conservative management are legitimate, the situation must be carefully monitored to prevent future damage. In addition, it must be stressed that current guidelines are based on observations in the adult and do not reflect the possibly different situation in adolescents and young women.
In a recent, retrospective cohort study reporting on 86 adolescents or young women (aged ≤22 years), Smorgick et al (34) found early stage I or II disease in 66 (76%) and advanced stage III or IV in 20 (23%). The pathology with advanced stage endometriosis included ovarian endometriomas in 14 cases, rectovaginal nodules in 1 case and diaphragmatic and pulmonary endometriosis in 1 case. The group of women with advanced stage was found to be slightly older at the time of diagnosis than those with milder disease, suggesting that adolescent endometriosis may be a progressive disease when affecting the ovaries. The situation was even worse in the cases (aged ≤20 years) reported by Yang et al (33) who documented stage I or II disease in only 11% of their patients, with 89% being at stage III or IV. It is interesting to note that by comparing the clinical features of the endometrioma in adolescents to those of women of older age groups, Lee et al (35) found that adolescents with the disease experienced menarche at a significantly earlier age, and that in them the main symptom was pain.
In a group of 63 young adults, Özyer et al (36) observed that a majority (65%) of patients had endometrioma on the right ovary, 14 (22%) patients had bilateral endometriomas and in one patient the posterior cul-de-sac was completely obliterated. The mean diameter of the endometriomas was 5 ± 2 cm. It should be noted that 55 (87%) patients had endometriomas with ovarian adhesions. Deep peritoneal endometriosis occurred in 14 (22%). The study supports the view that from early age the ovarian endometrioma has a complex structure adherent to the fossa ovarica. In a series of 114 laparoscopic cystectomies, Oh et al (37) found that the thickness of the removed ovarian tissue correlated with inadvertent follicular loss (p<0.001); however, there was no correlation between any clinical parameter tested and the thickness of the removed ovarian tissue. There was a correlation between ovarian follicular loss and the thickness of the removed ovarian tissue among patients aged <40 years (p<0.001), but not among patients aged ≥40 years (p = 0.123).
In adolescents, an ovarian endometrioma may present the paradox of a large cyst with minimal symptomatology: in an early case reported by Roth and Goodner (16) bilateral large ovarian endometriomas of 18 cm and 7 cm occurred in a 19-year-old teenager with minimal symptomatology. More recently, Wright and Laufer (38) reported the incidental finding of a 35-cm pelvic mass in an 18-year-old girl consisting of bilateral ovarian endometriomas that were treated by lysis of the adhesions and resection of the cysts. Obviously, the large size may involve a great risk of follicle loss in these young women after cystectomy.
Progression
As already mentioned, information on endometriosis progression in adolescents is scanty and data on early-onset endometriomas are minimal. An indirect suggestion of lack of progression was reported by Vicino et al (39), who found no difference in stages of endometriosis between adolescents aged 18-19 years (n = 12) and 19-21 years (n = 26). Both groups had, respectively, 41.7% and 30.8% severe endometriosis. However, the already-mentioned limitations due to use of the rAFS classification apply also to this series.
On the other hand, direct proof of the progressive nature of early-onset endometriosis has been provided by Unger and Laufer (40), albeit on a very small scale. They have published an evaluation using second-look laparoscopy of three cases (aged 13 to 16 years) not compliant with menstrual suppressive therapy. Although visible endometriotic lesions had been cauterized, all three cases showed progression of the disease, as documented by a larger number of peritoneal implants and the formation of a small endometrioma.
Slightly more information is available for early-onset endometriosis in general. A review of publications up to the end of 2013 indicates that some 35% of the 403 cases of adolescents with endometriosis diagnosed by age 20 or less, were stage III or IV; indirect, but strong evidence of a tendency of the disease to progress and produce early damage (1).
Changes in the ovarian endometrioma bed with age
Mimicking the uterus
Knowldege of the mechanism of endometrioma's formation in adult women comes from a study by Hughesdon (41) who, some 60 yeras ago investigated a series of 29 ovaries with chocolate cysts in situ from patients aged 26 to 58 years. He showed through multiple sections that underneath its mucosa the endometrioma possesses an inner cortex, derived from the folding of the cortical layer to form a pseudocyst. He investigated the structure of the endometriotic cyst and confirmed that in 26 out of 29 specimens, inner cortex can be identified in the cyst's wall because of the presence of primordial or early ripening follicles that are at times stretched. In 25 of 29 chocolate cysts, as the process progressed, the identity of the inner cortex was obscured by its metaplasia into smooth muscle in one layer or another.
Hughesdon concluded that “ectopic endometrium does not simply erode its way into the ovary: it is actively invaginated, thus producing a pseudo-uterus, to which follows a more or less abortive attempt at creating a muscular wall”.
Vascular changes
Using transvaginal color Doppler sonography, Qiu et al (42) demonstrated that in women aged <40 years, the ovarian endometrioma can be associated with a variable degree of interstitial fibrosis and microvascular injury. Compared with controls, ovarian interstitial flow in the study group was decreased and four stages of devascularization could be distinguished. In a recent review of age-related differences in sonographic characteristics of endometriomas, Guerriero et al (43) reported that with age there is an increased frequency of multilocular cysts, cysts with papillations or endometrial tufts, while ground glass echogenicity of cyst fluid becomes less common. Unfortunately, in addition to the absence of critical information such as previous surgery, the study did not describe separately cases of adolescent endometriomas. Also, no mention exists of features of the invaginated structure, such as stigma of invagination, presence of adhesion to superficial endometriosis in the fossa ovarica and particularly the progressive devascularization of the ovarian endometrioma bed with age.
Effect of endometrioma surgery during adolescence on ovarian function
It is well known that the first surgical procedure in a young woman with an endometrioma can determine the ultimate outcome of her reproductive life.
Most experts agree that surgical excision of an ovarian endometrioma in an adolescent should be avoided whenever possible. At the same time, the possible progressive nature of at least some of the early-onset endometriomas and the progressive changes in their pathology raise a key question: does surgical excision of an ovarian pseudocyst in a young patient lead to greater ovarian damage than expectant or medical management? No direct answer to this question exists today. At the same time, data exist to reach at least a tentative conclusion.
In 2009, Alborzi et al (44) compared the amount of ovarian tissue inadvertently excised with endometrioma to that with other benign ovarian cysts in patients undergoing laparoscopy versus laparotomy. They made two important observations: first, more tissue was excised with laparotomic than with laparoscopic surgery. Second, with both types of surgery, more tissue was excised with endometriomas than with other types of cysts. In laparotomic surgery, ovarian tissue was seen in 80% of endometriomas and 41% in other cysts. In laparoscopic surgery, percentages decreased to 65% in cases with endometriomas and 32% with non-endometriotic cysts.
Perlman and Kjer (45) recently evaluated the risk of inadvertently removing ovarian tissue after endometrioma excision in a retrospective cohort study of 393 laparoscopically ablated benign cysts with a diagnosis of either endometrioma (n = 294) or dermoid (n = 99). They found a significantly higher risk of inadvertently removing ovarian tissue in the endometrioma cohort than in the dermoid, despite the fact that procedures were performed by skilled laparoscopic surgeons.
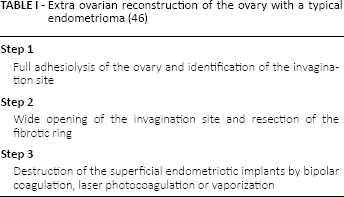
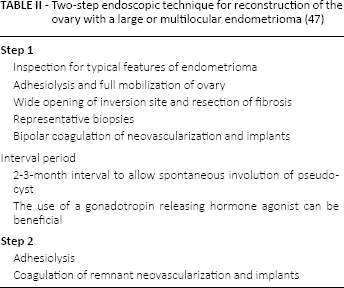
It is therefore likely that excision of endometriomas exposes adolescents and young women to a greater risk of loss of normal ovarian tissue as not only is the tissue normal, but the cyst may also be larger than in the adult. Moreover, in adolescent and young women ovulation may occur in the healthy wall of the endometrioma and enlarge the cyst by communicating cavities where the luteal cyst has been shown to be colonized by endometrial-like tissue. A two-step endoscopic technique for reconstruction of the ovary with a large or multilocular endometrioma has been proposed by Brosens et al (46) (Tabs. I, II). In contrast with the surgical excisional technique the extraovarian technique makes use of the stigma of inversion and opens the cavity while avoiding additional trauma to the ovary. Closing by apposition of the walls and suturing of the cortex is not indicated because the ovarian stroma is not exposed and the ovarian cortex is preserved. The basic principle of the surgical treatment of small and large ovarian endometriomas therefore includes adhesiolysis, first, to achieve full mobilization of the ovary and relief of the invagination and, second, to selectively destruct superficial endometriotic implants. In the young woman, the wall is usually not fibrotic and the superficial implants can be destroyed by bipolar coagulation or laser photocoagulation or vaporization causing minimal damage to the ovarian cortex.
Extra ovarian reconstruction of the ovary with a typical endometrioma (46)
Two-step endoscopic technique for reconstruction of the ovary with a large or multilocular endometrioma (47)
Hazards to future reproductive health
Risk of recurrence and potential prevention
As is the case for disease progression, few data exist for the rate of recurrence for adolescent endometriomas, whereas more information is available for endometriosis at large. Moreover, in a prospective laparoscopic study of 51 patients aged between 21 and 46 years with endometriosis, including chocolate cysts of 3 cm or more on one or both ovaries, Brosens et al (47) used ovarian cystoscopy with selective biopsy to investigate the histological type in a total of 59 ovarian chocolate cysts. While the presence of endometrioma was confirmed in 40 (75%) of the “no previous surgery” group, the presence of a hemorrhagic dysfunctional cyst was diagnosed in 14 (73%) out of 19 “previously operated” ovaries. Unfortunately, the diagnostic accuracy of imaging technique to differentiate the recurrent ovarian endometrioma from the dysfunctional hemorrhagic cyst has not been established and therefore these findings need to be taken in consideration for the management of recurrent ovarian hemorrhagic cysts.
The study by Tandoi et al (48) showed in a retrospective cohort that the rate and determinants of long-term recurrence of endometriosis was higher in a population of young than in older women. However, they found no clinical determinants.
In 2012, Yang et al (33) followed up for a mean period of 46.3 months (range 12-98 months) 35 adolescents with different types of endometriosis, following surgery. They observed recurrence in 45.7% of these cases, with an average recurrence time of 33.4 months.
Among risk factors for recurrence, an important role was played by the presence of multiple site lesions at operation. Interestingly, recurrence occurred in 60% of 15 adolescents who were not treated post-operatively; in 46% of 13 who received an oral contraceptive medication; in 1 of the 2 subjects given a progestin and in none of the 5 treated with a gonadotropin-releasing hormone (GnRH) analog. The difference between untreated and GnRH analog-treated subjects was statistically significant (p = 0.038).
More recently, Koga et al (49) explored ways to prevent recurrence of symptoms and lesions after conservative surgery and made several observations. On the one hand, they found that medical treatment prior to laparoscopic surgery is a risk factor for recurrence. On the other, pregnancy soon after surgery has a protective effect on recurrence. In addition, evidence is accumulating that the administration of oral contraceptives, of a combination of a GnRH analog plus an oral contraceptive, or the insertion of a levonorgestrel-releasing intrauterine system may be beneficial.
The recent study by De Cicco Nardone et al (50) confirmed previous in situ observations that there is a strong association between adhesion of the endometrioma to the ovarian fossa and the presence of endometriosis on the peritoneal surface of the fossa. Histopathologic examination of the peritoneum of the ovarian fossa revealed the presence of endometriosis in 87% of patients presenting adhesions of the endometriomas with the ovarian fossa and in only 15% of those without adherent endometrioma (p<0.0001). Pain symptoms were more frequent in patients with endometriomas adherent to the ovarian fossa, a condition significantly correlated with pain symptoms that may be predictive of endometrioma recurrence.
In a cohort built over 15 years of 55 adolescWents aged 12 to 19 years (mean age: 18 years), Audebert et al (51) encountered superficial implants in 31 cases (56.4%), endometriomas in 18 cases (33%) and deep infiltrating endometriosis in 6 cases (11%). All subjects were submitted to laparoscopic surgical excision or ablation of the lesions and during the follow-up, the recurrence rate for endometriomas was 37%; in five cases formation of new endometriomas was reported.
In conclusion, women should be well-informed about the risks of endometrioma recurrence and those who wish to become pregnant should attempt to conceive as soon as possible. Furthermore, hormonal therapy is strongly advised for patients who do not want to conceive immediately, and it should be continued until pregnancy is desired (49). A factor worth mentioning is that, in contrast with transvaginal hydro-laparoscopy, trans-abdominal access prevents the direct observation without manipulation of the site of ovarian adhesion and the invagination of the ovarian endometrioma. The full removal of the endometriotic implants in the fossa ovarica may potentially reduce the risk of recurrence.
Infertility
The management of endometriomas in the context of infertility has recently been the subject of much debate, especially in view of the growing success of in vitro fertilization (52). According to Rombauts (53), the two questions at the center of the debate are whether surgery still has a place, and if so, which procedure gives the best results. Shervin et al (54) claimed that in advanced cases associated with deep endometriosis and infertility, fine excision and stripping of the endometrioma along with radical resection of the deep lesions improves fecundity without any significant adverse effect when compared to patients with intact ovaries.
Roman et al (55, 56) have evaluated comparatively the effect of endometrioma ablation using plasma energy on subsequent pregnancy in a total of 124 women with ovarian endometriomas, associated or not to colorectal disease. The mean follow-up was 32 ± 18 months. Of the 83 women wishing to conceive, 61.4% became pregnant and in 64.7% of them conception occurred spontaneously. Among women with associated colorectal endometriosis, pregnancy rate was 65.8%. The only independent factor for which association with pregnancy rates approached significance (p = 0.06) was age over 35 years. They concluded that recurrence and pregnancy rates with this technique seem comparable to the best results reported after endometrioma cystectomy.
In exploring the relationship between endometriomas and infertility, Berlanda et al (57) concluded that management in adolescent and young women should not be based upon surgery alone, but upon a combination of surgery (with a refinement of the operating technique), long-term oral contraceptive, in vitro fertilization and oocyte cryopreservation.
In short, available data suggest that better results can be obtained if, in addition to technical refinement, surgery is based on detailed knowledge of ovarian pathology which – as detailed above – differs greatly between the adolescent and the adult woman. The key to success seems the use of ovarian cortex preserving surgery.
Use of fertility preservation techniques
In 2009, Elizur et al (58), confronted with a 25-year-old nulliparous woman with severe and symptomatic endometriosis and low antral follicular count, carried out three cycles of ovarian stimulation, harvesting 21 oocytes that were cryopreserved, inaugurating a new alternative to preserve future fertility.
Today, young age at diagnosis may be an independent but pivotal additional factor to be taken into consideration in the balance of the pros and cons of fertility preservation, in particular for those with bilateral un-operated endometriomas and for those who previously had excision of unilateral endometriomas and require surgery for a contralateral recurrence (59). Women affected by every iatrogenic or pathologic condition known to compromise ovarian function severely have been considered as potential candidates for fertility preservation, since they are at increased risk of premature ovarian exhaustion and about half of them will experience infertility.
Conclusions: a double edge sword
Research has still not identified the optimal technique for treating ovarian endometriosis, particularly in the adolescent. Laparoscopic ovarian cystectomy on the one hand offers the lowest risk of recurrence and the highest chance of spontaneous pregnancy rate, on the other may expose the young woman to the risk of significant ovarian damage.
Although present knowledge suggests that there is no evidence that surgical management improves fertility in women with endometrioma (60), there is also evidence that the presence of the endometrioma progressively affects the cortical lining causing fibrosis and interstitial devascularization, with significant risk of decreasing ovarian function (61).
Clearly, the endometrioma in the adolescent differs from that of adult women and for this reason management of this specific variant requires careful investigation. Therefore, the application of new imaging techniques should focus on ways to evaluate the progression of detrimental effects that its presence causes on the ovarian vascularization. Time has come to individualize the management of an endometrioma, taking into account in the first place, age, and if surgery is needed, adapt the procedure to the surgical pathology.
To this end Benagiano et al (62) explored a new pharmacological approach to its management capable of preserving future fertility. To optimize medical management, however, the molecular pathology of ovarian endometriomas and the mechanisms by which the endometrioma progressively affects the ovary need to be investigated.
Footnotes
Financial support: No grants or funding have been received for this study.
Conflict of interest: None of the authors has financial interest related to this study to disclose.