
Abstract
Background
Incidence, risk factors, case fatality and survival rates of ischemic stroke subtypes are unknown in the Middle East due to the lack of community-based incidence stroke studies in this region.
Aim
To characterize ischemic stroke subtypes in a Middle Eastern population.
Methods
The Mashad Stroke Incidence Study is a community-based study that prospectively ascertained all cases of stroke among the 450,229 inhabitants of Mashhad, Iran between 2006 and 2007. We identified 512 cases of first-ever ischemic stroke [264 men (mean age 65.5 ± 14.4) and 248 women (mean age 64.14 ± 14.5)]. Subtypes of ischemic stroke were classified according to the TOAST criteria. Incidence rates were age standardized to the WHO and European populations.
Results
The proportion of stroke subtypes was distributed as follows: 14.1% large artery disease, 15% cardioembolic, 22.5% small artery disease, 43.9% undetermined and 4.5% other. The greatest overall incidence rates were attributed to undetermined infarction (49.97/100,000) followed by small artery disease (25.54/100,000). Prevalence of hypertension, diabetes and atrial fibrillation differed among ischemic stroke subtypes. Overall, there were 268 (52.34%) deaths and 73 (14.25%) recurrent strokes at five years after incident ischemic stroke, with the greatest risk of recurrence seen in the large artery disease (35.6%) and cardioembolic (35.5%) subgroups. Survival was similar in men and women for each stroke subtype.
Conclusions
We observed markedly greater incidence rates of ischemic stroke subtypes than in other countries within the Mashad Stroke Incidence Study after age standardization. Our findings should be considered when planning prevention and stroke care services in this region.
Introduction
Ischemic stroke has various pathophysiological mechanisms. 1 Outcome, prognosis, and stroke recurrence differ markedly according to the underlying ischemic stroke etiologic subtype, and there exists significant implications for clinical management.2,3
There are large geographic variations in the distribution of subtypes of ischemic stroke (IS). 4 For example, small artery disease (SAD) is more prevalent in East Asians while large artery disease and cardioembolic stroke are overrepresented in Western communities.5,6 Accordingly, it is essential to have a clear understanding of the distribution of stroke subtypes in geographically or ethnically defined populations. In part, improved characterization of stroke subtypes within a population can be used to direct the allocation of resources towards higher-yield stroke preventative measures, particularly in developing countries.
Population-based studies from the Middle East are scarce. Most previous epidemiological investigations in this region are based on hospital-acquired data that exclude general community-dwelling individuals who do not seek acute medical care, and have few details on the etiology and subtypes of stroke. 7 Recently, using a large population-based study design, we provided evidence of a greater incidence of first-ever stroke, particularly IS, in Iran than in most other regions of the world, with IS occurring approximately one decade earlier. 8 Etiological analyses of these stroke subtypes may help explain regional differences in incidence of IS and assist in reducing future burden of stroke by refining diagnostic, therapeutic and preventive strategies. In this analysis, we aimed to determine the incidence of subtypes of IS and their associated risk factors and survival rates using a mechanism-based classification scheme.
Materials and methods
The Mashhad Stroke Incidence Study (MSIS) is a population-based incidence stroke study in Mashhad, Iran. Mashhad is the second most populated city in Iran, with a population of over three million. The study population, clinical definitions, methods of investigation and other details of this cohort have been described elsewhere. 8
In brief, from 21 November 2006, all patients with stroke were identified prospectively in all age groups in a community that comprised 450,229 inhabitants. Multiple overlapping sources were used to identify patients with stroke, and additional efforts were made to identify those who were not admitted to the hospital; non-hospitalized patients were examined by a study neurologist (MRA) and three neurology residents (MTF, RK, MP).
Stroke was defined as an acute-onset focal neurological deficit of vascular etiology that persisted for >24 h. 9 Neuroimaging was used to differentiate patients with definite stroke into IS, intra cerebral hemorrhage and subarachnoid hemorrhage types.
Ischemic stroke was defined as a stroke for which either computed tomography (CT) performed within 28 days of symptom onset showed a normal appearance, or CT or magnetic resonance imaging (MRI) showed an area of recent infarction corresponding to the incident symptoms. Possible and covert strokes were not included in the incidence figures. The term covert stroke refers to incidental findings of stroke on brain CT, but without the required signs and symptoms outlined in the WHO clinical definition of stroke. 9
Etiology of ischemic stroke
TOAST (Trial of Org 10172 in Acute Stroke Treatment) criteria were used to define pathophysiological subtypes of IS which were classified into five major mechanistic categories as follows: large-artery disease (LAD), cardioembolism (CE), SAD, stroke of other determined cause, and stroke of undetermined etiology. 10 If there was more than one possible cause for IS, cases were classified as undetermined stroke. Ischemic venous thrombosis was classified as ischemic stroke of other determined causes. An expert panel of neurologists adjudicated controversial cases at group meetings, and a consensus was required for assignment to a particular category.
Risk factors
TIA was defined as an acute transient focal neurological deficit caused by vascular disease, which completely reversed within 24 h. 11 Hypertension was defined by medical history, use of anti-hypertensive medications, or having a mean blood pressure greater than 140/90 mmHg on two separate occasions. 12 Diabetes mellitus (DM) was defined when patients had fasting blood glucose levels above 126 mg/dL, previous diagnosis of DM by a physician, or were taking medications for DM. 13 Atrial fibrillation (AF) was defined when patients had a history of AF or when chronic or paroxysmal AF was present on electrocardiography or prolonged cardiac monitoring. Hypercholesterolemia was defined as total serum cholesterol levels >200 mg/dL or the use of lipid-lowering agents. The presence of a past history of cardiac disease, and family history of stroke and TIA was obtained from medical records or through patient interview. In addition, information regarding the individual’s alcohol consumption was ascertained, as was smoking status, defined as never, ex-smoker, and current smoker.
Follow-up
Patients were followed up using one of three ways. Some had regular outpatient visits, while those who had severe disability were followed up with a telephone call, home visit and/or by reviewing their medical charts. When patients could not be reached by telephone, they were followed up by community health volunteers for possible change of address, or death.
Statistical analysis
Average annual incidence rates for subtypes of ischemic stroke were calculated using the denominator from a census that was conducted from October to November 2006. Results were adjusted for sex and age according to the World Health Organization (WHO) and European population to allow comparisons with other incidence studies. Distributions of risk factors among subjects in the five subtypes were compared using the chi-square test. For each risk factor, a logistic regression model with age group and sex was used to examine whether the proportions of risk factors were different between stroke subtypes. ANOVA was used to test differences in age between the five subgroups of ischemic stroke. The Kaplan–Meier product-limit method was used to estimate survival rates for each subtype of first-ever ischemic stroke. Patients were censored at the time of last follow-up or after one year. The log-rank test was used to compare rate estimates and Cox proportional hazards models were used to determine differences in survival between ischemic stroke subtypes with adjustment for age, sex and other factors that were statistically significant in univariable analyses. Statistical analyses were performed using the SAS®9.3 software package and a two-tailed P < 0.05 was considered statistically significant in all analyses.
Ethics
The study was approved by the ethics committee of Mashhad University of Medical Sciences (MUMS). Informed consent was obtained from each subject before any interview or neurologic examination was conducted. Consent by next of kin or guardian was obtained for severely ill or unconscious subjects.
Results
Between 21 November 2006 and 20 November 2007, 624 strokes occurred in this population including 512 patients with first-ever IS (264 men and 248 women). Among these patients, the mean age was 65.67 (SD 14.37) for men and 64.14 (SD 14.51) for women. The main ethnic groups were Persian (84%), Turk (8%), Afghan (4.3%), Kurd (2.7%), Arab (0.6%), and other (0.4%). Brain imaging (99.6 % CT scan and 12% MRI) and ECGs were performed in all patients, 70% had a duplex, 62% has transcranial Doppler, and fewer than 15% had any other test (such as echocardiography, angiograms, or venograms; Supplementary Table 1).
Among incident cases of IS, there were 72 (14.1%) with extra or intracranial LAD, 77 (15%) cardioembolic strokes, 114 (22.2%) SAD strokes, 226 (44.1%) undetermined strokes, and 23 (4.5%) due to other causes (Table 1). Patients with undetermined infarction were on average the oldest group (68.76years, SD 13.09), followed by LAD (67.67 years, SD 11.71), SAD (64.55 years, SD 11.65), cardioembolic (62.1 years, 16.56), and other causes (41.91 years, SD 16.19). In patients with undetermined ischemic stroke subtype, no identifiable mechanism was found in 137 patients (60.6%) despite diagnostic work-up; 89 patients (39.4%) had incomplete work-up; and three patients (1.3%) had more than one possible etiology (both extra/intracranial vascular stenosis and AF). Other determined sources of IS included eight venous sinus thrombosis, three drug abuse, two complicated migraines, two aortic dissections, two iatrogenic, and one each of head trauma, giant aneurysm, common carotid artery hyperplasia, pregnancy complication, and temporal arteritis.
Risk factors
Age-specific and adjusted incidence of subtypes of ischemic stroke per 100,000 individuals in Mashhad, Iran.*

Numbers in specified age groups indicate crude number of first-ever ischemic stroke. SAD: Small artery disease; LAD: Large artery disease; WHO: World health organization.
Risk Factors among 512 patients with first ischemic stroke in Mashhad, Iran
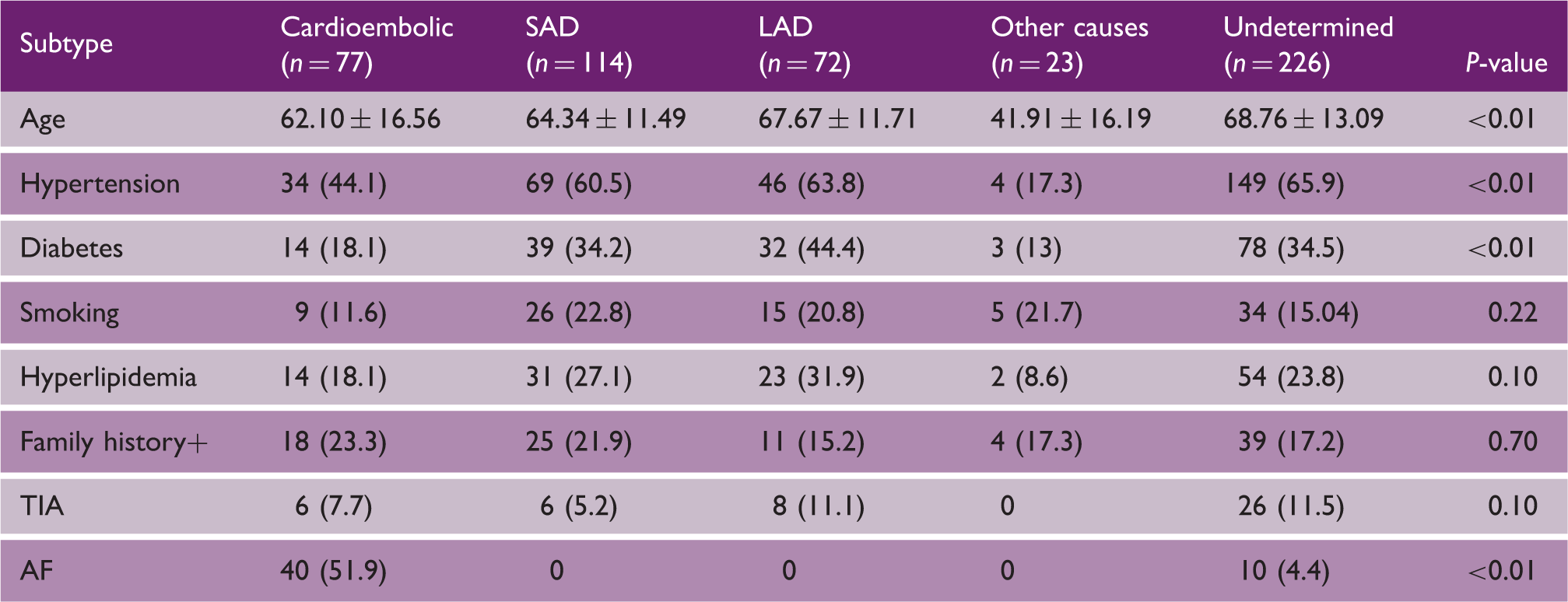
SAD: small artery disease; LAD: large artery disease; WHO: World Health Organization; TIA: transient ischemic attack; AF: atrial fibrillation.
Incidence rates
The greatest overall incidence rates were attributed to undetermined infarction (50.20/100,000) followed by SAD (25.32/100,000), cardioembolic (17.10/100,000) and LAD (15.99/100,000) (Table 1). Incidence rates for LAD, cardioembolic, and SAD were slightly higher in men than in women, while incidence of undetermined stroke type was higher in women. Incidence rates of each subtype were not significantly different between men and women. After age standardization to WHO and European populations, incidence was highest for undetermined stroke type (89.92/100,000 WHO and 205.79/100,000 European population) followed by SAD (43.37/100,000 WHO and 86.22/100,000 European population), LAD (28.39/100,000 WHO and 62.44/100,000 European population) and cardioembolic (27.93/100,000 WHO and 56.35/100,000 European population) (Table 1). Figure 1 presents a comparison of percentage of subtypes of ischemic stroke across different regions.
Percentage of subtypes of ischemic stroke across countries. MSIS: Mashhad Stroke Incidence Study; SLSR: South London Stroke Register; OCSP: The Oxfordshire Community Stroke (OCSP) Project; OXVASC: The Oxford Vascular Study (OXVASC).3,14–20.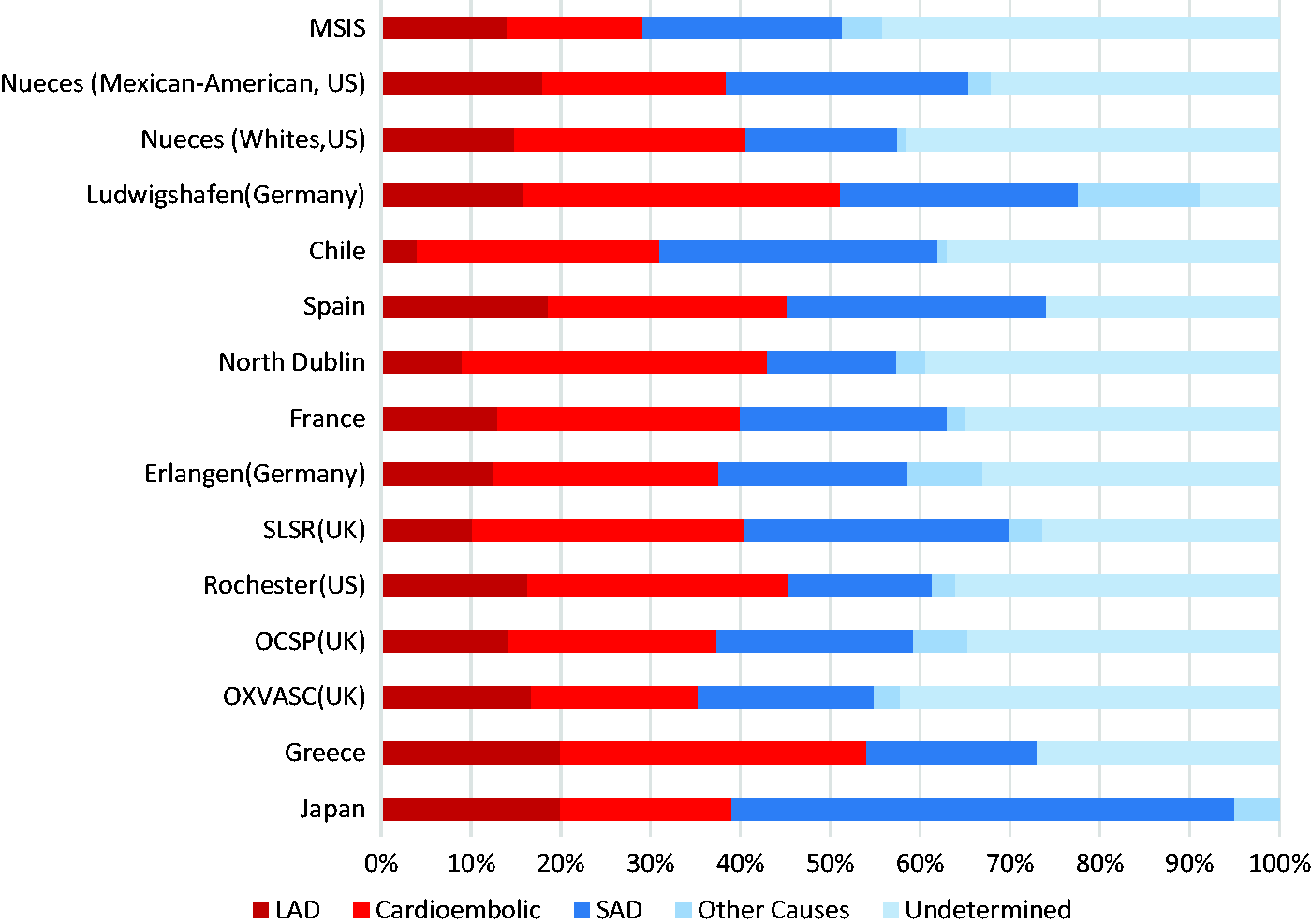
Survival and recurrence
Despite all attempts, we were unable to follow four patients immediately after discharge, a further 16 were lost to follow-up at one year, and 67 more patients were lost to follow-up five years after ischemic stroke. Thus, 445 patients (87%) were followed up. Overall, there were 268 (52.34%) deaths, with variations in mortality across subgroups (49 (63%) cases in cardioembolic, 34 in SAD (29%), 35 in LAD (48%), six (26%) in other causes and 144 (63%) in undetermined infarction) at five years after initial ischemic stroke (Figure 2(a)). At five years, 73 patients (14.25%) had a recurrent stroke with the highest cumulative risk of recurrence seen in the LAD (35.6%) and cardioembolic (35.5%) subgroups (Figure 2(b)). Outcomes did not appear to vary by sex or ethnicity, although sample sizes were small for all ethnicities other than Persian.
Kaplan–Meier curves showing the five-year survival rate free of death and recurrence for all subtypes of ischemic stroke. (a) Kaplan–Meier curves showing the five-year survival rate for all subtypes of ischemic stroke. (b) Kaplan–Meier curves showing the five-year survival rate free of recurrence for all subtypes of ischemic stroke.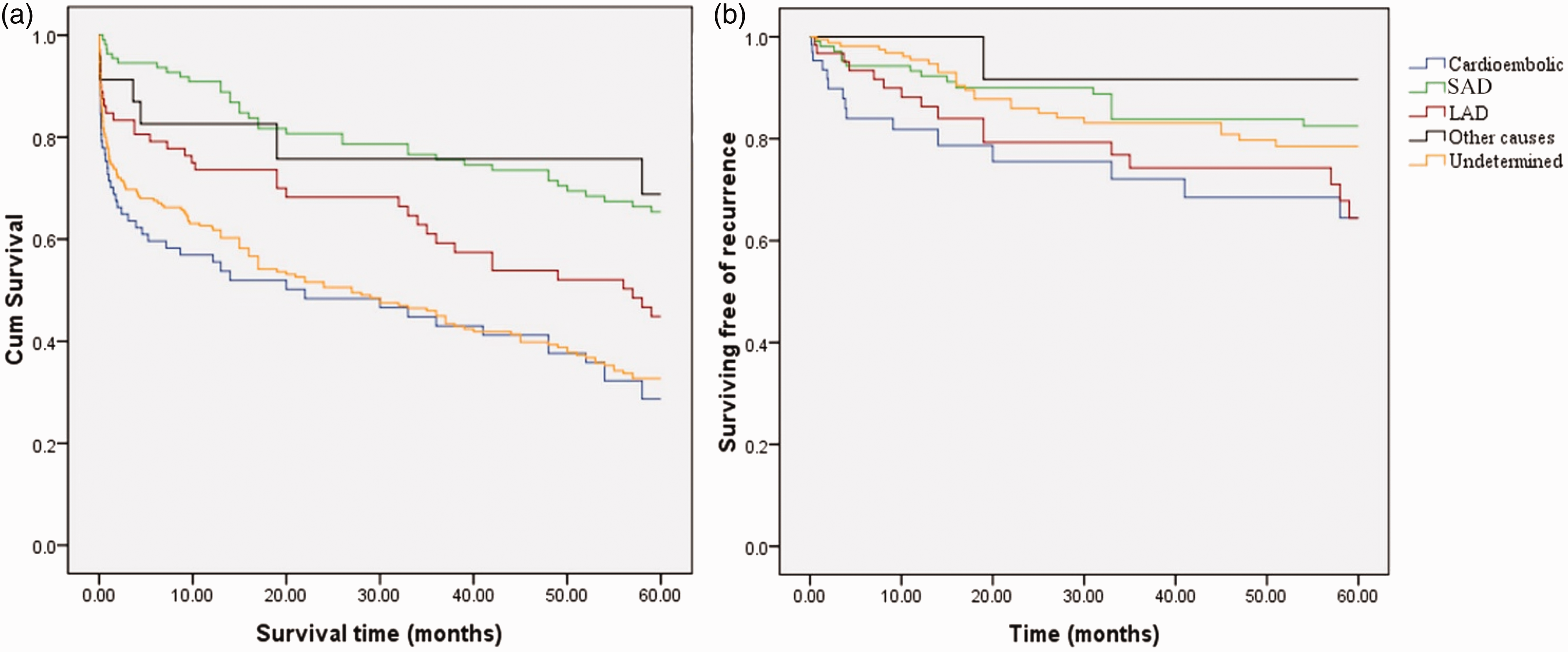
Discussion
To the best of our knowledge, this is the first population-based report from the Middle East on stroke incidence and survival by subtype of ischemic stroke. Patients with undetermined subtype comprised the highest proportion of IS, followed by SAD, CE, and LAD. After adjusting for age, the incidence of SAD and LAD subtypes was significantly higher in our population compared to most cohorts from other countries, including Germany, England, France, New Zealand, Chile and Japan.3,14–20 The high proportion of undetermined stroke in our study may be due to lower access to diagnostic studies (Vascular studies and long-term cardiac monitoring to diagnosis paroxysmal/occult AF) needed to classify subtype in cases managed outside tertiary hospitals. Indeed, 37% of undetermined strokes had incomplete evaluation, and so we may have underestimated cardioembolic and LAD and overestimated undetermined strokes.
Most previous population-based studies of stroke have been performed in Western countries, and incidence rates may significantly be different than that of the Middle Eastern population. While CE is the dominant type of IS in Western countries and SAD the most common subtype in Eastern Asia, the high rates of SAD and LAD in our community may be attributed to variability in risk factor distribution, and genetic and environmental factors including race/ethnic differences, age, and socioeconomic status. This would represent a very high potential burden of atherothrombotic stroke in this population. In addition, Middle Eastern countries are comprised of populations with somewhat similar genetic, lifestyle, and diet that may influence stroke risk, type, and survival after stroke, as well as other characteristics in comparison to Western and East Asian populations. Therefore, our results may be applicable to other parts of the Middle East, and provide a useful basis for future comparisons of stroke epidemiology in this region.
Age was significantly different across stroke subtypes. Interestingly, the average age for CE stroke was younger than that of LAD and SAD and also much lower than the average age of CE stroke in western countries. The predominantly young structure of our population may also explain a relatively lower rate of CE as compared to Western countries. However, CE due to AF could rise in the future, as the current population ages. Hence, our results will provide a basis for evaluation of trends for IS in order to optimize future diagnostic and preventive strategies.
We found a high frequency of hypertension in all subtypes of IS, most considerably in the LAD and undetermined subtype, which is consistent with the results of other studies conducted in Western populations.3,14 The large proportion of LAD and SAD could be explained by an increased prevalence of risk factors for atherosclerosis, such as hypertension, DM, smoking, and/or poor compliance with treatment. Results from a recent hospital-based cross-sectional study in Iran demonstrated high rates of IS and vascular risk factors (hypertension, diabetes and hyperlipidemia) in this population. 21 Hence, primary prevention measures such as control of blood pressure, reducing fat in the diet, and smoking cessation are needed to be reinforced in Iran as they are largely lacking. Since these measures have been put in place in the west, the proportion of LAD and lacunar stroke has significantly declined in the past two decades, and so similar declines might be likely in Iran.
Survival rates differed across stroke subtypes. Case fatality was greatest for CE and undetermined, and least for SAD subtype. Our finding of no sex-specific differences in survival of subtypes of IS is consistent with several recent studies.22,23 Survival at one year after stroke was also greater than in other cohorts. 4 Because older age is associated with greater mortality after IS, higher survival rates might be explained by the younger average age of our population.
One strength of our study includes the precise diagnosis of first ever stroke and use of neuroimaging in more than 99% of cases. 8 In addition, we utilized multiple overlapping sources in an attempt to ascertain all cases, thereby improving generalizability.24,25 A limitation of our study is the large number of strokes of undetermined subtype. Overall, TOAST criteria lead to an overestimation of undetermined strokes as compared to other mechanism-based classifications of stroke, mainly because patients with incomplete investigation, as well as those with no cause despite extensive evaluation, or two or more potential etiologies fall in this group. The TOAST classification was one of the first classification systems based on stroke mechanisms, and has been used widely in prior epidemiologic studies.15–20 Apart from concerns about over-interpretation of causality, 26 there are significant limitations in its use in epidemiological studies, particularly in developing countries where there may be lack of access to some diagnostic tests. Recent efforts have been made to better characterize patients with undetermined stroke and some of these may be better applied to epidemiological studies, where investigators are unable to influence the type of diagnostic tests undertaken. For instance, in the ASCO system (A-S-C-O: atherosclerosis, small-vessel disease, cardiac source, and other causes), each of the four ASCO phenotypes is graded 0, 1, 2, or 3, based on the likelihood of underlying mechanism, and has been shown to lead to fewer strokes of undetermined subtype (by including all possible mechanistic categories) and more of LAD subtype (by including <50% stenosis with luminal thrombus), as compared to TOAST criteria. However, there are no population-based epidemiologic studies in different populations based on this system, and reporting all possible subtypes of stroke may lead to difficulty in interpretation. Therefore, TOAST criteria would provide the most reliable methods for comparing outcome of IS subtypes in our population with existing reports from prior studies.
In our study, a considerable number of stroke cases were captured in the community (outside referral hospitals), and so diagnostic tests were not available (Incomplete investigation). Also, as in most developing countries, diagnostic modalities in Iran are less accessible than in developed countries. These factors contributed to the large proportion of undetermined strokes in our study. Early mortality after stroke may also have led to an overestimate in the proportion of undetermined strokes. Despite this limitation, we have been able to provide a detailed characterization of recurrence in those patients in whom there were adequate diagnostic tests.
Summary
In summary, we report population-based epidemiologic data on etiologic, risk factors, and survival of subtypes of IS in Mashhad, Iran. Undetermined type was the dominant subtype of ischemic stroke, and was associated with older age, greater prevalence of vascular risk factors, and reduced survival. We also observed a high incidence of LAD and SAD, associated with a high prevalence of underlying hypertension and DM. This basic information can be used to customize and implement regional primary and secondary preventive programs aimed at reducing the future burden of IS in Iran.
Footnotes
Acknowledgment
We are grateful to Mojgan Khaniani, Mohamad Taghi Frazdfard, Reza Kiani, and Majid Panahandeh who assessed the majority of the patients, and to Drs Mohsen Mohebaty and Ali Eshraghy for cardiac examination. Special thanks are extended to all of the community health volunteers without whose help this research would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from MUMS. Dr. Shoamanaesh is supported by the Marta and Owen Boris Chair in Stroke Research and Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.