
Abstract
Background
Cardiovascular events while driving have occasionally been reported. In contrast, there have been few studies on stroke while driving.
Aim
The objectives of this study were to (1) report the frequency of stroke while driving and (2) evaluate its association with automobile accidents.
Methods
Clinical data prospectively acquired between January 2011 and December 2016 on 2145 stroke patients (1301 with ischemic stroke, 585 with intracerebral hemorrhage, and 259 with subarachnoid hemorrhage) were reviewed to identify patients who sustained a stroke while driving. The ratio of driving to performing other activities was evaluated for each stroke type. Furthermore, the drivers’ response to stroke was reviewed to understand how automobile accidents occurred.
Results
Among the 2145 patients, 85 (63 ischemic stroke, 20 intracerebral hemorrhage, and 2 subarachnoid hemorrhage) sustained a stroke while driving. The ratio of driving to performing other activities was significantly higher in ischemic stroke (4.8%) than in intracerebral hemorrhage (3.4%) or subarachnoid hemorrhage (0.8%). A majority of drivers either continued driving or pulled over to the roadside after suffering a stroke. However, 14 (16%) patients were involved in automobile accidents. In most patients, an altered mental status due to severe stroke was the presumed cause of the accident.
Conclusion
Stroke occurred while driving in 4.0% of all strokes and accidents occurred in 16% of these instances.
Introduction
Stroke may occur during any human activity. Globally, hundreds of millions of person-hours are spent driving a vehicle every year. It is probable that a certain proportion of drivers sustain a stroke while driving and that some stroke-afflicted drivers end up causing automobile accidents. 1 Yet, there are few studies of stroke while driving. Our objectives were to (1) report the frequency of stroke while driving and (2) evaluate its association with automobile accidents.
Subjects and methods
This was a single-center retrospective observational study using prospectively acquired data. The study protocol was approved by our institution’s Ethics Committee. All stroke patients were treated by board-certified stroke specialists according to the Japanese Guidelines for the Management of Stroke. 2 Our institution, a regional Stroke Center serving a suburban population of 800,000, used an integrated clinical database CAP-2000 (Nihon Koden, Tokyo, Japan) since 2010. We used the dataset of 2145 stroke patients, aged 18 or older, who presented to our emergency department (ED) within four days of symptom onset between January 2011 and December 2016. For all the stroke patients admitted via our ED, stroke types and presenting symptoms as well as detailed data on when, where, and how their symptoms developed were registered on the database by ED residents. The information was obtained from the patients, their surrogates, or paramedics. They were also asked about the activities performed immediately before symptom onset. We modified the classification of daily activities by Hayashi et al., in which the activities were classified into eight categories (sleeping, resting, eating, bathing/toilet, walking, hard-working, driving, and other in-house activities). 3 Patients who drove to our institution with symptoms that had occurred while performing other activities were excluded from analysis. Stroke types were classified as ischemic, intracerebral hemorrhage (ICH), and atraumatic subarachnoid hemorrhage (SAH). Stroke severity was evaluated according to the National Institutes of Health Stroke Scale (NIHSS) scores, and the level of consciousness was evaluated according to the Glasgow Coma Scale (GCS) scores. Ischemic strokes were further classified by mechanism using the ASCO classification: atherosclerosis (A), small-vessel diseases (S), cardiac causes (C), and other causes (O). 4 Minor stroke or transient ischemic attack (TIA) was classified as ischemic stroke category. Electrocardiogram, magnetic resonance imaging/angiography, and transthoracic echocardiography were routinely obtained from patients with suspected ischemic stroke shortly after their arrival to ED, and board-certified neurologists and/or neurosurgeons determined the ischemic stroke subtype on the basis of those examinations. Patients with suspected cryptogenic stroke underwent transesophageal echocardiography to identify the source of embolism unless contraindicated. 5
Statistical analysis
Fisher’s exact test was used for categorical variables, and unpaired t test was used for continuous variables. JMP software (SAS Institute, Cary, NC, USA) was used for statistical analysis. Data are shown as mean ± standard deviation, and a P value of <0.05 was considered statistically significant.
Results
Demographics
Demographics of 85 patients with driving-related stroke
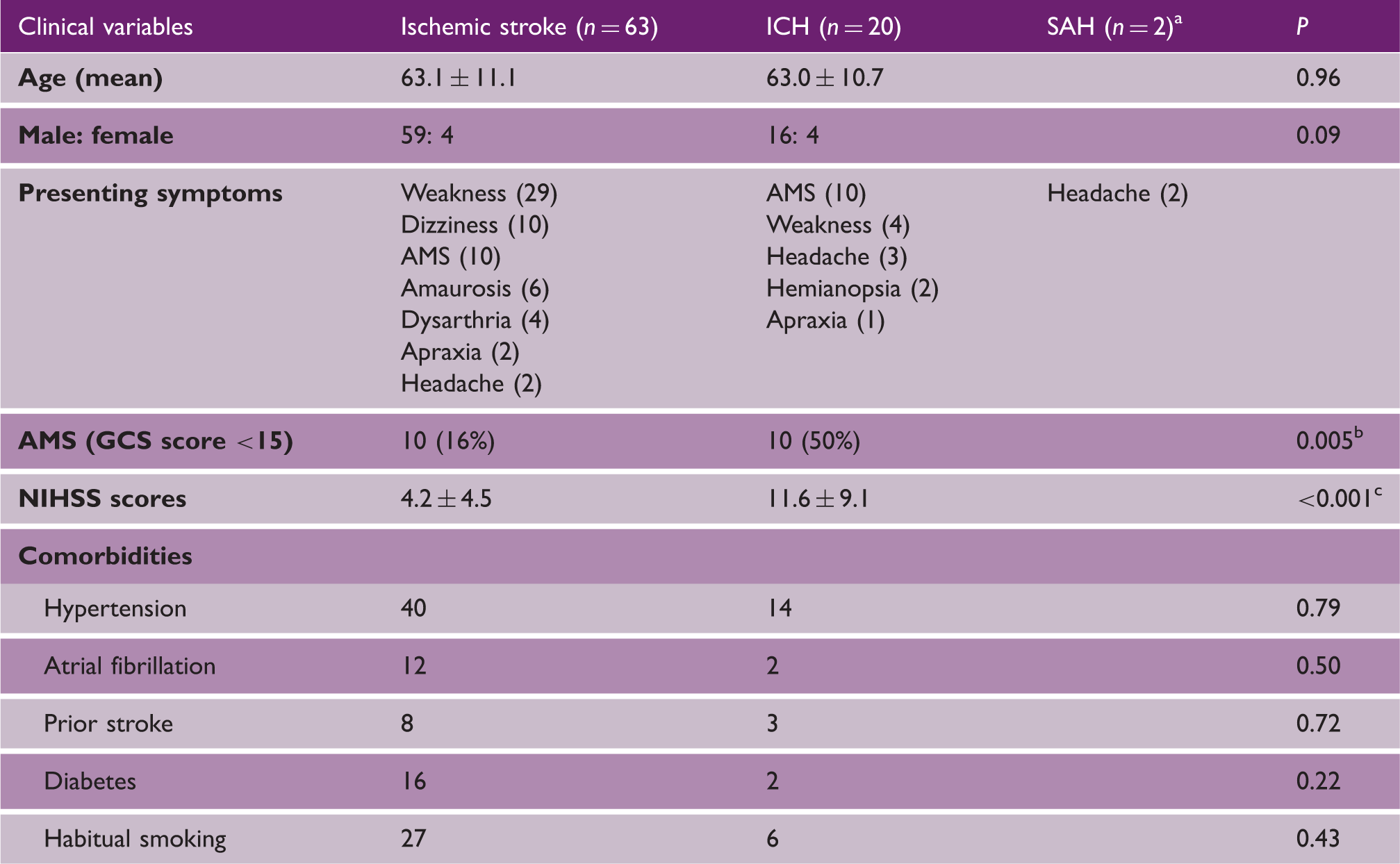
AMS: altered mental status; ED: emergency department; GCS: Glasgow Coma Scale; ICH: intracerebral hemorrhage; NIHSS: National Institutes of Health Stroke Scale; SAH: subarachnoid hemorrhage.
Statistical analysis not performed because of small sample size (n = 2).
Statistically significant.
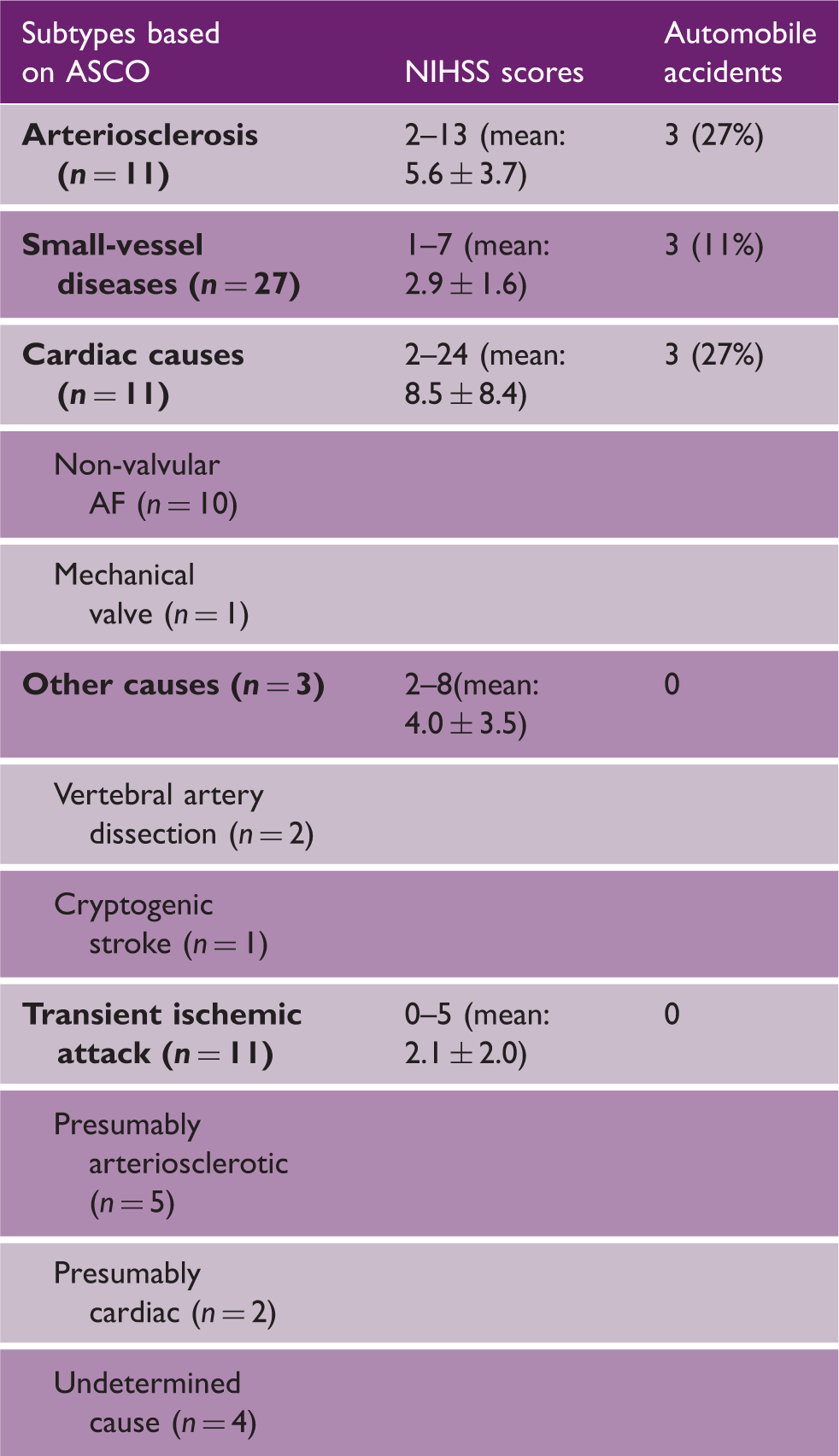
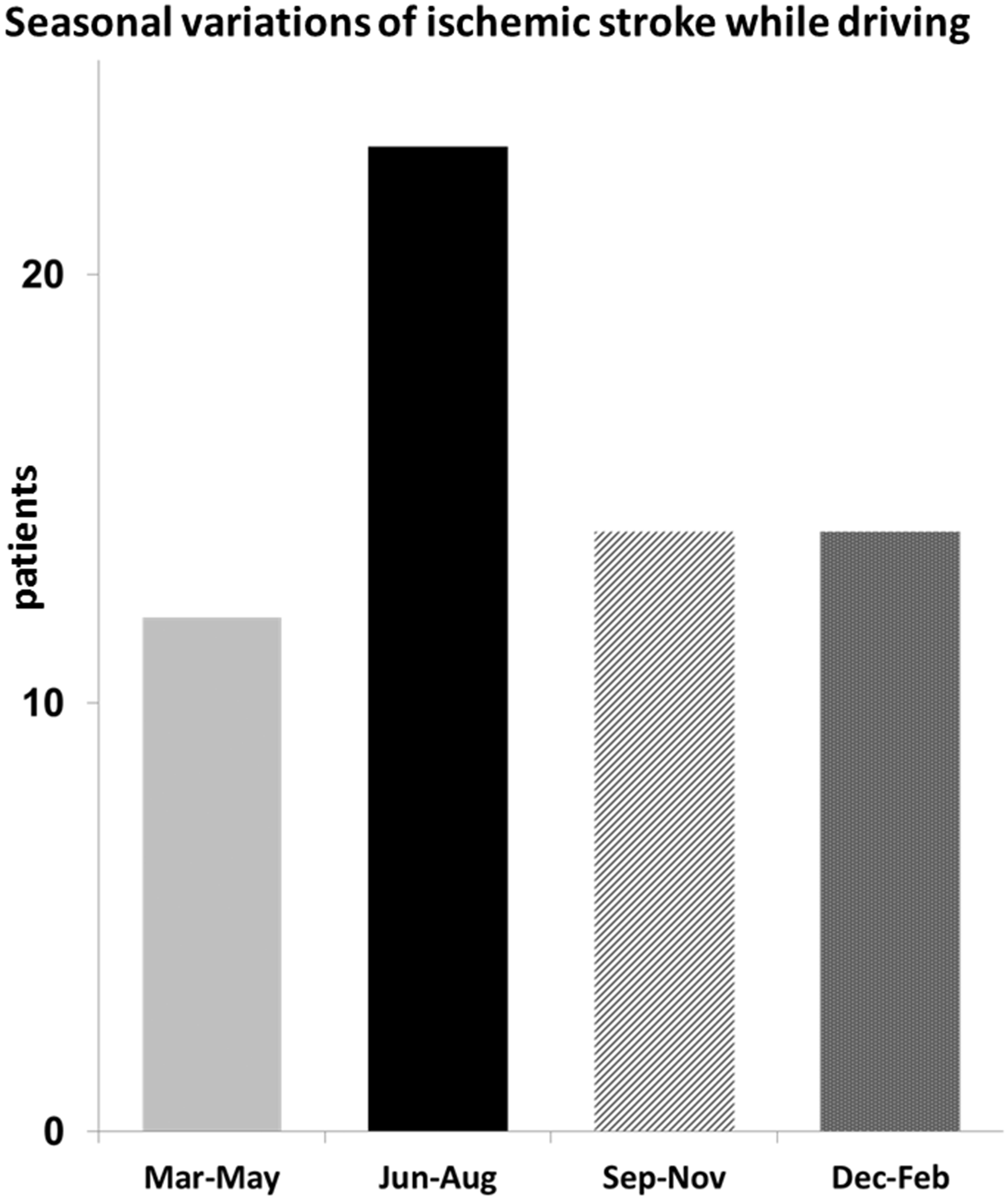
Patients with an altered mental status, defined by a GCS score of ≤14 at ED, were significantly more common in the ICH group than in the ischemic stroke group (50 vs. 16%, P = 0.005). The ICH group exhibited significantly higher NIHSS scores than the ischemic stroke group (11.6 ± 9.1 vs. 4.2 ± 4.5, P < 0.001). Otherwise, there were no significant intergroup differences. The relationship between daily activities and stroke type is shown in Figure 1. The ratio of driving to performing other activities was significantly higher in the ischemic stroke group (4.8%) than in the ICH (3.4%) or SAH (0.8%) group. The causes of ischemic stroke are shown in Table 2, and the timing of driving-related stroke was more common in summer months (Figure 2).
The relationship between daily activities and stoke in 2145 patients (1301 ischemic stroke, 585 ICH, and 259 SAH) was shown. A total of 85 patients (63 ischemic stroke, 20 ICH, and 2 SAH) sustained stroke while driving. The ratio of driving to performing other activities was significantly higher in ischemic stroke. ICH: intracerebral hemorrhage; SAH: subarachnoid hemorrhage. Clinical characteristics of 63 patients with ischemic stroke AF: atrial fibrillation; NIHSS: National Institutes of Health Stroke Scale. The 63 ischemic stroke patients were classified to four seasonal quartiles. Driving-related ischemic stroke occurred most frequently during summer (June–August).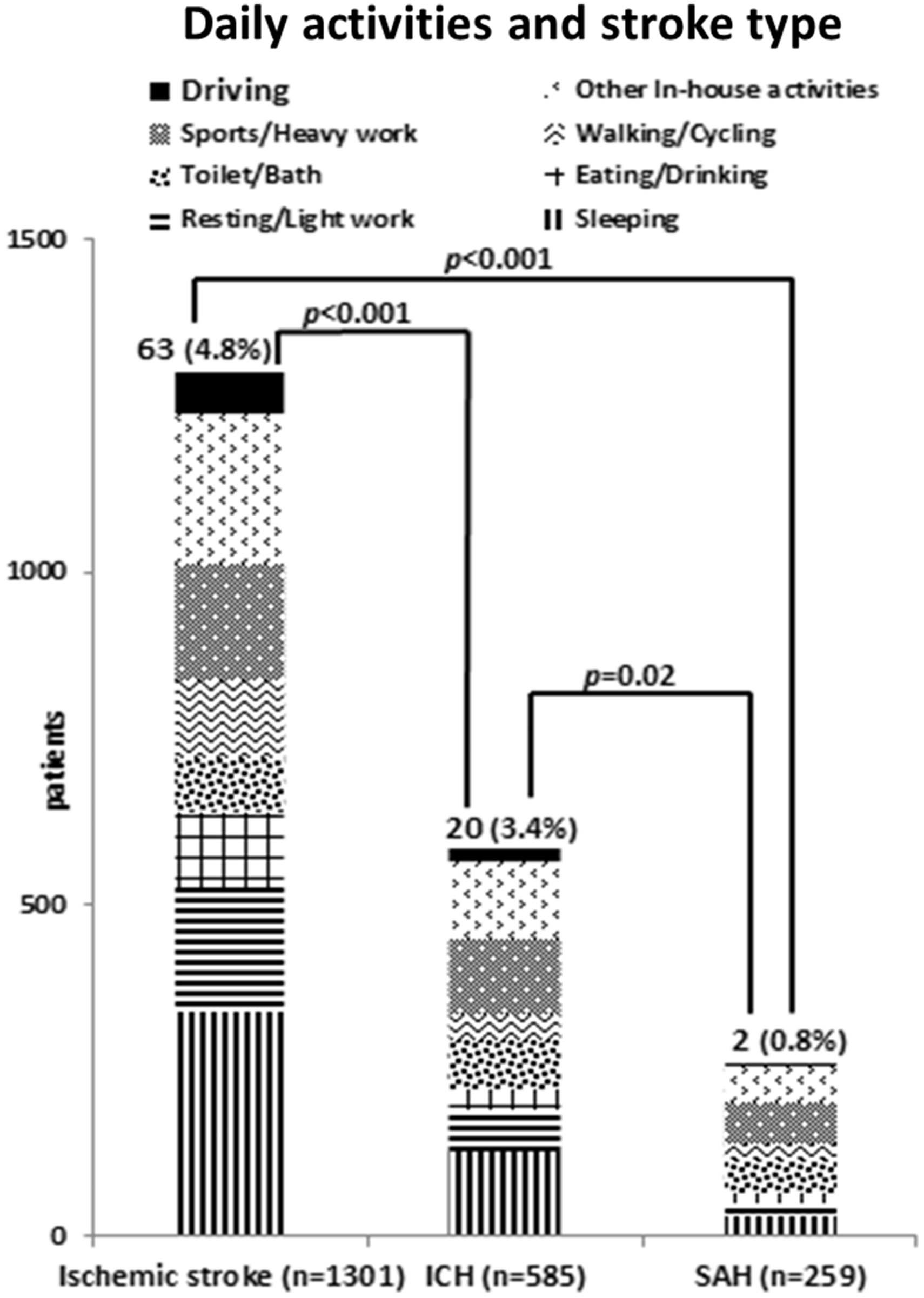
Disease severity and automobile accidents
Clinical characteristics of 14 stroke patients who caused automobile accidents
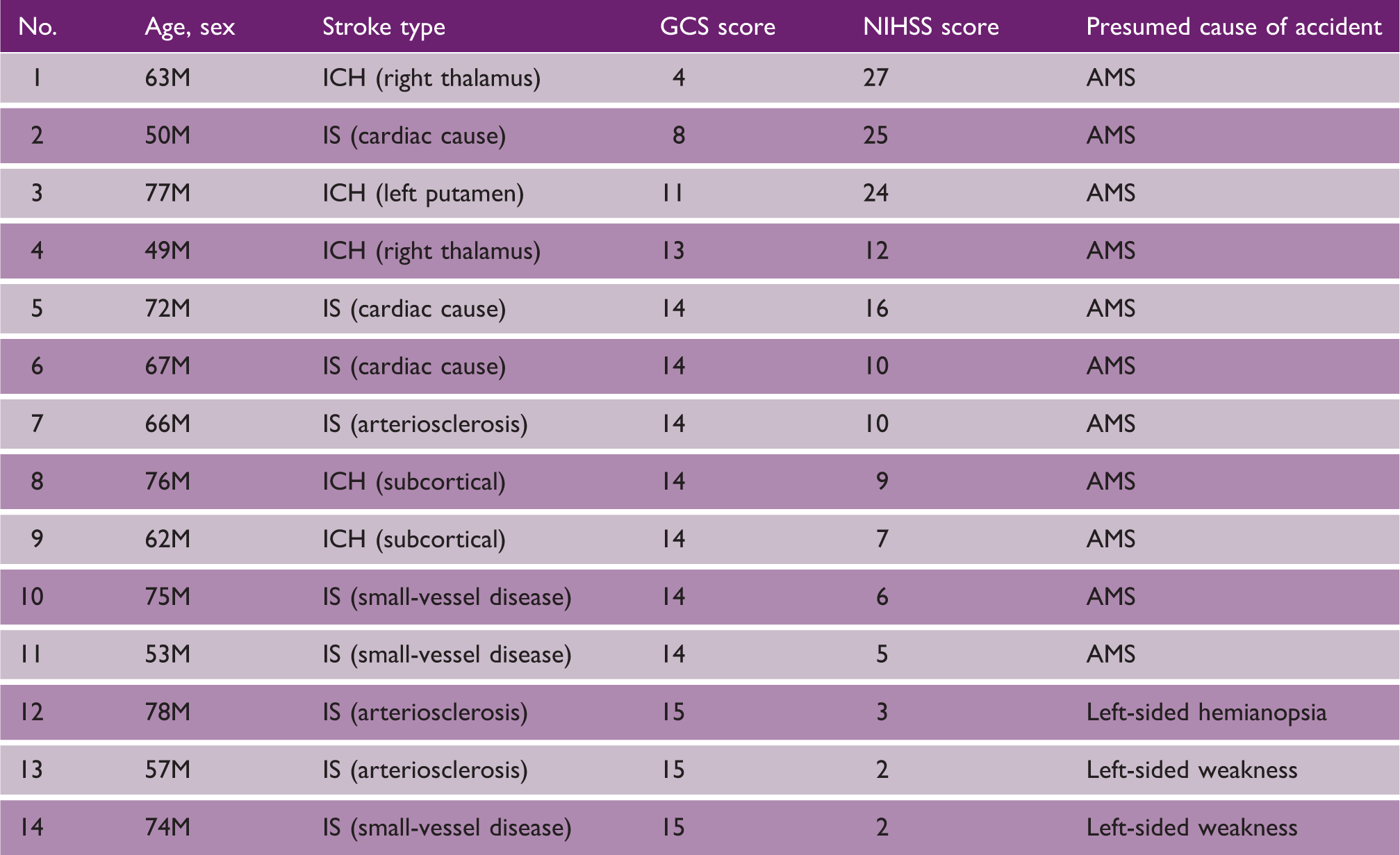
AMS: altered mental status; GCS: Glasgow Coma Scale; ICH: intracerebral hemorrhage; IS: ischemic stroke; M: male; NIHSS: National Institutes of Health Stroke Scale.
Side of weakness and automobile accidents in conscious patients
Thirty-three fully conscious patients exhibited unilateral weakness (hemi- or monoparesis), 21 with left and 12 with right hemiparesis. Two (10%) patients with left and none with right hemiparesis were involved in accidents (P = 0.52).
Response of drivers to stroke
The response of the 85 drivers to stroke is shown in Figure 3. Forty-three (51%) continued driving despite symptoms and sought medical attention only after reaching their destinations. Although 40 managed to arrive uneventfully, three were involved in minor accidents. Thirty-one (36%) pulled over to the roadside. Eleven resumed driving after improvement and another 11 called for help, mostly using cell phones. However, the remaining nine drivers could not call for help and they were later found by bystanders. The other 11 (13%) drivers involved in accidents, severe enough to require help from paramedics. While all the 14 drivers involved in accidents were driving alone, all the 10 drivers who were with front-seat passengers were able to avoid accidents. Head or other bodily injuries inflicted by accidents were either absent or minor in all the cases.
Response of the 85 drivers to stroke. Forty-three continued driving. Thirty-one pulled over to the roadside. The other 11 caused automobile accidents. AMS: altered mental status; ED: emergency department; EMS: emergency medical services.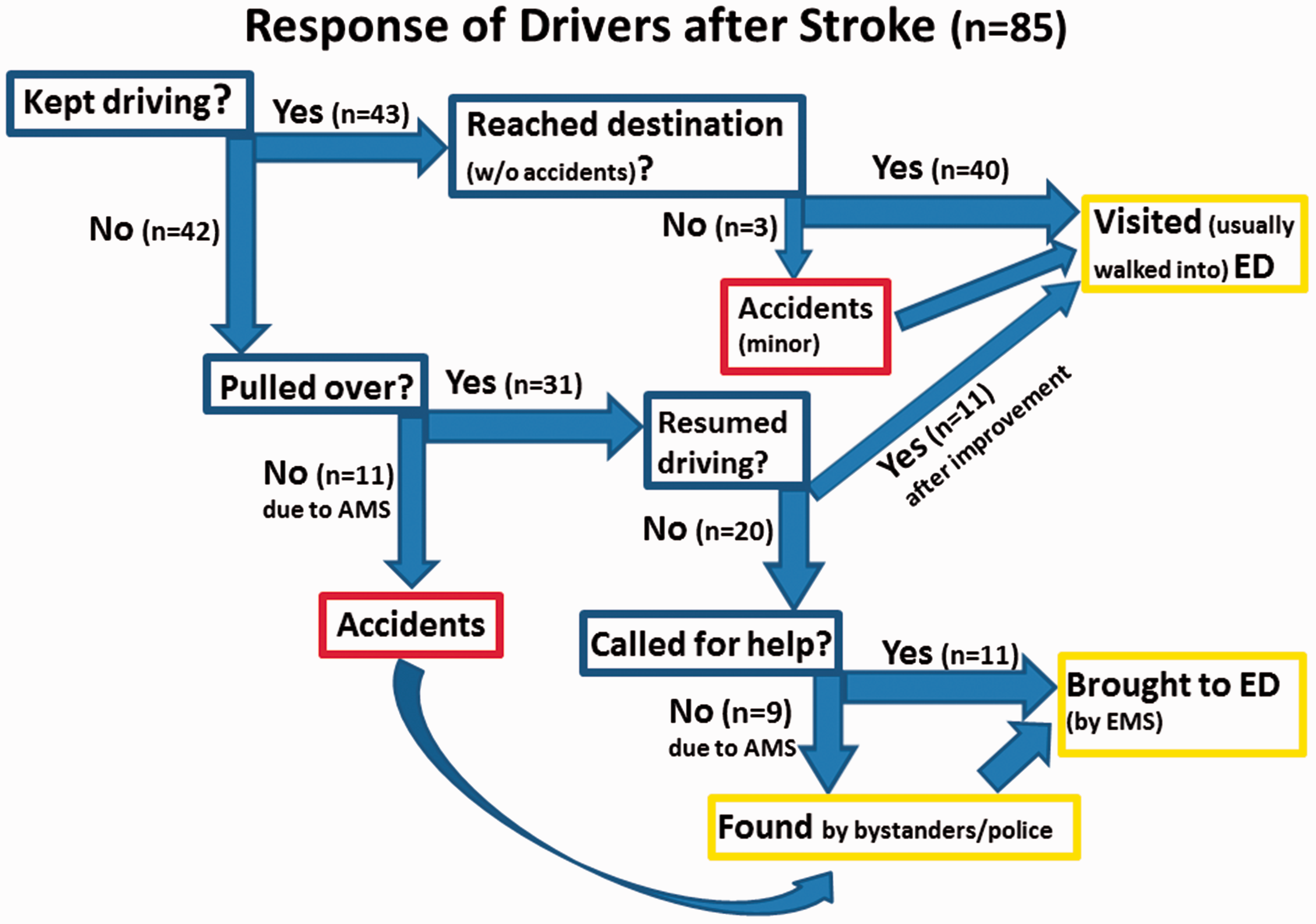
Discussion
Acute cardiovascular events occurring while driving have occasionally been reported in the literature.6–10 However, most of those studies have been conducted either by forensic scientists or by crash scene investigators,7–10 and only patients whose vascular events were severe enough to cause accidents have been identified. We found that stroke while driving occurred in 4.0% of 2145 stroke patients. The marked male preponderance in stroke-afflicted drivers (Tables 1 and 3) may be explained by the fact that elderly women drive less often and cease driving earlier than elderly men. 11
The ratio of driving to performing other activities was significantly higher in ischemic strokes than in hemorrhagic strokes is consistent with the findings of previous epidemiologic studies,12,13 in which professional drivers exhibited a higher risk of ischemic stroke and the relative risk ratio of ischemic stroke to ICH was 1.23. 12 Several explanations are possible regarding why drivers seemed to sustain ischemic strokes more frequently than hemorrhagic strokes. First, uninterrupted sitting while driving may lead to arterial hypercoagulability: drivers sit in a confined space in the same posture for hours. Previous studies have found that uninterrupted sitting increased plasma fibrinogen and reduced plasma volume, with an associated increase in hemoglobin and hematocrit.14–18 In addition, drivers often keep driving without drinking water for hours, and subsequent dehydration and hemoconcentration may facilitate the development of ischemic stroke while driving. In our cohort, 68% of ischemic stroke patients may have sustained an atherothrombotic stroke (Table 2). This elevated ratio of atherothrombotic stroke as well as the marked increase in the occurrence of ischemic stroke during summer (Figure 2) is compatible with hypercoagulability as a contributing cause of ischemic stroke while driving.
Driving requires head rotation for shoulder checking, which may predispose drivers to develop cervical artery dissection or bowhunter syndrome.19,20 In this study, two vertebral artery dissections causing ischemic stroke while driving were identified (Table 2). Neither patient could recall episodes of head rotation preceding symptom onset.
The mechanism underlying hemorrhagic stroke while driving may not be easily explainable. Approximately 70% of patients with driving-related ICH had hypertension (Table 1). However, there was little evidence that driving or uninterrupted sitting raised the systemic blood pressure.
This study is also unique in that it evaluated the relationship between strokes occurring while driving and automobile accidents (Figure 3). In most patients, the stroke severity was mild, and they were able to continue driving. It also became clear that a substantial proportion of patients could avoid accidents by pulling over but could not call for help due to neurological deterioration. Meanwhile, in 16% of driving-related stroke patients, stroke was associated with automobile accidents; and in most of them, an altered mental state was the presumed cause (Table 3). Subsequently, the question of whether the side of weakness had affected the occurrence of accidents arose, considering the fact that both the accelerator pedal and foot brake need to be manipulated with the right foot. Interestingly, most fully conscious patients could avoid accidents regardless of the side of weakness.
This study is observational and cross-sectional and did not establish a causal relationship between driving and stroke onset, and we could not conclude that driving was a risk factor for ischemic stroke. The information on the temporal relationship between driving and stroke onset was obtained from patients, indicating the possibility of a recollection bias. It may be difficult to determine the precise incidence of driving-related stroke: while mild symptoms may be overlooked, some fatal accident victims who are pronounced dead at the scene may actually have sustained a severe stroke, particularly SAH. The low proportion of SAH while driving (0.8%) may be partly attributable to this hypothesis. The incidence of driving-related stroke may be influenced by geographical differences: it may be lower in metropolitan areas where many residents use public transportation and drive less often than suburban residents. We were not able to account for adverse environmental factors (such as bad weather and nighttime driving), which increase the probability of accidents. Finally, this study did not analyze the factors affecting the drivers, such as long-hour driving and sleep deprivation, which are also likely to increase the probability of strokes and accidents. As the world’s elder population continues to grow at an unprecedented rate, stroke while driving is expected to increase from the currently observed 4% of all stroke.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.