
Abstract
Background
Elevated D-dimer levels are a marker of both thrombin formation and fibrinolysis. Currently D-dimer measurement is routinely used for ruling out venous thromboembolism and diagnosis/monitoring of disseminated intravascular coagulation. Recent emerging data suggest that D-dimer may become an important biomarker in ischemic stroke as well as in cardiovascular diseases.
Aims
To outline the clinical utility of D-dimer in work-up and management of ischemic stroke.
Summary
D-dimer measurement is most useful in stroke with active cancer as it can confirm etiologic diagnosis, predict recurrent stroke risk, and aid treatment decision in cancer-associated stroke. In cryptogenic stroke, high D-dimer levels can also provide clues for the cause of stroke as occult cancer and undetected cardiac embolic source as occult atrial fibrillation and may be helpful in treatment decision making of secondary stroke prevention. Serial D-dimer measurements should be further studied to monitor antithrombotic therapy effectiveness in both cardiogenic and cryptogenic etiologies.
Conclusion
Accumulating data suggests the utility of D-dimer test in the management of ischemic stroke, although the evidence is still limited. Future studies would clarify the role of D-dimer measurement in ischemic stroke.
Keywords
Introduction
D-dimer is a degradation product of fibrin, produced when plasmin is activated. It is a marker of both thrombin formation and fibrinolysis. D-dimer is relatively stable and resistant to ex vivo activation. In addition, D-dimer measurement is relatively simple, readily accessible, and inexpensive. Thus, D-dimer is most commonly used clinical assay among the various biomarkers that reflect activation of coagulation and fibrinolysis. 1
The utility of D-dimer measurement in clinical practice has been established for the exclusion of venous thromboembolism (VTE) and diagnosis/monitoring of disseminated intravascular coagulation (DIC). A negative test result is widely used to exclude the diagnosis of deep venous thrombosis (DVT) or pulmonary embolism (PE) in suspected patients without a high clinical probability.2,3
Recent studies indicate potential uses of D-dimer for coronary and aortic disease. 4 A review published in 2009 concluded that D-dimer measurement could not replace either clinical or radiological evaluation in etiological diagnosis and outcome prediction in ischemic stroke. 5 However, emerging data in the last decade suggest that D-dimer measurement can provide useful diagnostic and prognostic information in some stroke settings. Therefore, we aimed to summarize current clinical utility and potential future applications of D-dimer measurement in ischemic stroke patients in this review.
Search strategy
We searched PubMed for related articles published from 1990 to March 2019 using search terms (D-dimer) AND (Stroke) AND (“ischemic stroke” OR “cryptogenic stroke” OR “cancer”). Additionally, we searched references from relevant articles.
The final reference list was generated based on relevance for the current review.
Cardiogenic embolism and other stroke etiologies
Several studies have investigated the diagnostic value of D-dimer as a biomarker for etiological classification. Most previous studies have shown D-dimer values within 48 h from stroke onset are significantly higher in cardioembolic stroke than in noncardioembolic stroke.6–13 D-dimer values in cardiogenic stroke are presumed to reflect fibrin-rich thrombus formation due to blood stasis in the cardiac chambers. Thrombus originating in the large arteries is mostly platelet-rich during high flow and therefore is expected to produce mild D-dimer elevations. Small vessel disease etiology is often due to lipohyalinosis and expected to have minimal D-dimer elevation7,14 (Figure 1). The cut-off value of plasma D-dimer levels for diagnosis of cardioembolic stroke was reported to vary from 0.3 µg/ml to 2.0 µg/ml.6–8,12,13 Conflicting results exist on the association of elevated D-dimer levels and cardioembolic stroke,15,16 which could be caused by heterogeneity in coagulation status among various cardioembolic sources. On the other hand, the combination of lacunar syndrome and low D-dimer value was reported to improve the diagnostic accuracy of small vessel disease.
17
Thus, D-dimer measurement can provide a clue for diagnosis of any stroke etiology. However, current advanced modalities including diffusion-weighted imaging (DWI) and vascular imaging are generally more valuable for large artery or small vessel etiological diagnosis.
Median, 1st quartile and 3rd quartile D-dimer values in acute ischemic stroke and non-stroke patients.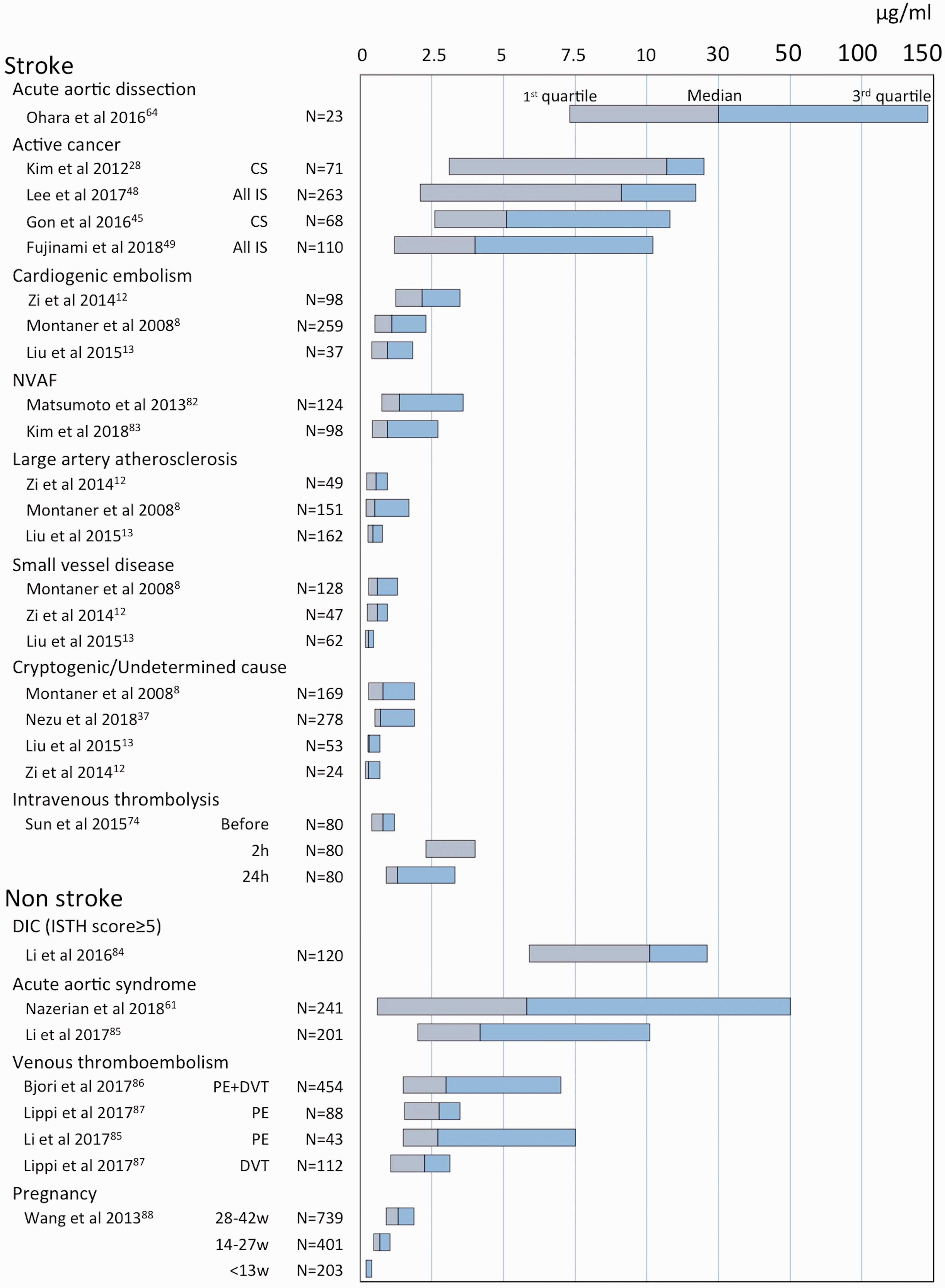
The substudies of large clinical trials for direct oral anticoagulants (DOACs) have shown higher D-dimer values at baseline to be predictive of subsequent stroke in atrial fibrillation (AF) patients (including patients with and without prior stroke) independent of established risk factors such as the CHADS2 score valuables.18,19 Several studies have shown that increased D-dimer levels are significantly associated with left atrial enlargement and the presence of an atrial thrombus in AF patients.20–22 These results suggest that D-dimer measurement may be useful for the subsequent risk assessment in cardioembolic patients with AF.
Cryptogenic stroke/embolic stroke of undetermined source
Etiological diagnosis
Cryptogenic stroke is thought to comprise about 25% of all ischemic stroke. Cryptogenic etiology is slowly be replaced by a more stringent clinical construct called embolic stroke of undetermined source (ESUS) which is one subgroup within crypogenic stroke whereby workup is complete and no cause found for an embolic appearing infarct. 23 Presumed causes for cryptogenic stroke/ESUS include occult AF, minor cardiac sources, paradoxical embolism, cancer-related stroke, and non-stenotic arterial sources. 23 D-dimer measurement may provide clues for the cause of stroke and guide an efficient extensive evaluation within cryptogenic stroke/ESUS.
Occult cancer
Occasionally, ischemic stroke can be a first manifestation of cancer. In previous studies, occult cancer was newly diagnosed in 0.3 to 2.8% in all the stroke patients and the incidence increased up to 6.5% in cryptogenic stroke patients.24–28 This fact suggests occult cancer can be causative for cryptogenic stroke presumably by cancer-associated hypercoagulation. Gon et al. 27 reported that 10% of cryptogenic stroke patients without known active cancer had occult cancer. High D-dimer value and multiple vascular territory infarcts (MVTIs) on DWI independently predicted occult cancer. Cryptogenic stroke patients with occult cancer had a median D-dimer value of 6.2 µg/ml. Kim et al. 28 reported high D-dimer value and MVTI were predictors for active cancer in cryptogenic stroke patients. Optimal diagnostic cut off D-dimer value for cancer was ≥2.15 µg/ml. Occult cancer was identified in 45% of cryptogenic stroke patients with D-dimer values ≥2.15 µg/ml and in 100% of patients both with the above D-dimer cutoff values and MVTI.
Paradoxical embolism
Detection of VTE and right to left shunt are essential for the diagnosis of paradoxical embolism as etiology of stroke. Venous ultrasound is the preferred test for the diagnosis of paradoxical embolism. However, venous ultrasound may not be enough for detection of DVT in pelvis or other veins, which can be causative.29,30 Therefore, D-dimer measurement can be a screening test for VTE in cryptogenic stroke. Further extensive imaging as pelvic magnetic resonance venography and chest contrast CT for detecting VTE should be considered in patients with high D-dimer in acute stroke even when having negative results by ultrasound.
Occult AF
High D-dimer in cryptogenic stroke may be also suggestive of undiagnosed cardiac embolic disease as occult AF. A recent report suggested elevated coagulation marker including D-dimer predicted occult AF in cryptogenic stroke. 31 Some studies reported elevated D-dimer values were more predictive of cardiogenic stroke when combining with B-type natriuretic peptide and a clinical predictive score for occult AF in stroke patients.8,32
Prediction of recurrent stroke
D-dimer measurement may be useful for evaluating the risk of recurrent stroke in cryptogenic stroke. Previous studies showed that D-dimer levels in full cohorts including all etiologies with acute ischemic stroke were not predictive of long-term recurrent stroke.33,34 D-Dimer measurement in transient ischemic attack (TIA) predicts DWI-positive TIA but did not predict stroke recurrence. 35 However, some recent studies reported that high D-dimer levels at admission were predictive of the recurrent stroke in cryptogenic stroke patients. Kim et al. 36 showed elevated D-dimer levels (>1.0 µg/ml) at admission significantly increased the risk of recurrent stroke with 9.7% of annual stroke rate (1.8% in D-dimer levels ≤1.0 µg/ml) in cryptogenic stroke and were an independent predictor for recurrent ischemic stroke especially in cryptogenic stroke with patent foramen ovale (PFO). Similarly, Nezu et al. 37 showed high D-dimer levels (≥0.7 µg/ml) at admission were independently associated with recurrent stroke and all-cause mortality with hazard ratio of 3.76 in cryptogenic stroke patients with right to left shunt. A recent study reported that persistent elevation in markers of coagulation tests including D-dimers beyond two weeks after stroke predicted newly diagnosed AF, newly diagnosed malignancy or recurrent stroke in cryptogenic stroke patients receiving antiplatelet therapy. 31
Cancer-associated stroke
Currently, 10% of hospitalized ischemic stroke patients have comorbid cancer. 38 Cancer-associated hypercoagulation is a main pathophysiological mechanism of cryptogenic stroke in patients with cancer.38,39
D-dimer values in acute stroke patients with active and occult cancer
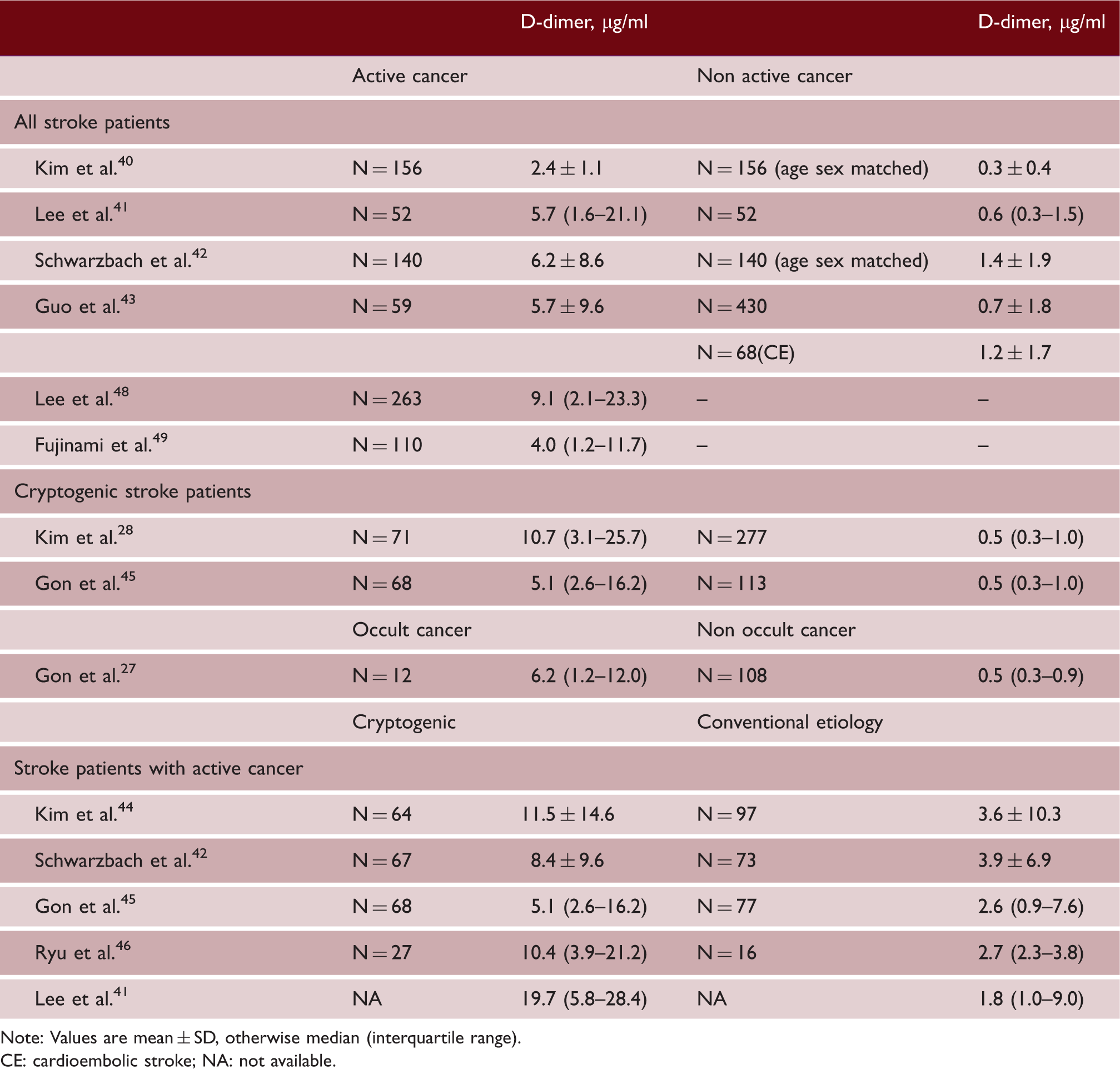
Note: Values are mean ± SD, otherwise median (interquartile range).
CE: cardioembolic stroke; NA: not available.
Identification of cancer-associated hypercoagulation is important in predicting recurrent stroke and may guide better stroke management in stroke with active cancer patients. Fujinami et al. 49 showed the concurrence of very high D-dimer levels (≥10.4 µg/ml) and MVTI was an independent predictor of early recurrent stroke in active cancer patients. Recurrent stroke within 30 days occurred in 35% (8 of 23) of patients with both these factors. Another recent study reported elevated D-dimer level was an independent predictor of neurological deterioration within 72 h in cryptogenic stroke in active cancer patients. 50 In stroke due to cancer-associated hypercoagulation, low-molecular weight heparin (LWMH) may be the most suitable therapy for effective secondary stroke prevention.38,39 Based on multiple clinical trials, LWMH is recommended for treatment and secondary prevention of VTE in patients with cancer.51,52 Heparin can have multiple beneficial actions on several of the proposed pathologic mechanisms in cancer-associated hypercoagulation. 53 Moreover, the likely biologic explanation favoring heparin, not warfarin may be that heparin releases tissue factor pathway inhibitor ultimately blocking the production of factor Xa that could be triggered by tumor-derived tissue factor-positive microparticles.54,55 Small nonrandomized studies have suggested that subcutaneous LWMH or unfractionated heparin might be effective for secondary prevention in stroke patients with cancer-associated hypercoagulation.56,57 Jang et al. 56 showed that D-dimer levels were dramatically decreased in cancer-associated stroke patients treated with enoxaparin, while they did not change with use of warfarin. Recurrent stroke was observed in 3.4% of enoxaparin-treated patients and 16% of warfarin-treated patients stroke during the mean follow-up period of 4.9 months. Successful reduction of D-dimer level by anticoagulants has been linked to less stroke recurrence and mortality in other cancer-associated stroke studies.48,58 Serial D-dimer measurements may be useful for judging of the effect of anticoagulation in this setting.
Acute aortic dissection
D-dimer value elevates in patients with acute type A aortic dissection (ATAAD) with a high sensitivity of ≥95%. 59 Generally, the suspicion of ATAAD is based on clinical information as chest/back pain and pulse deficit. 60 However, negative D-dimer result is useful as a rule-out tool especially in patients with low probability by the ATAAD clinical risk assessment.59,61
Ischemic stroke occurs in ATAAD patients due to its extension to the cervicocerebral arteries or emboli from the site of dissection. ATAAD was seen in 0.31% of ambulance transported stroke-suspected patients and 1.70% of acute ischemic stroke patients presenting within 4 h of onset. 62 The diagnosis in ATAAD patients with stroke is more challenging compared to those without stroke because they sometimes present predominantly with neurological symptoms and about half of them have no chest/back pain, probably due to consciousness disturbance, aphasia, or amnesia.63,64 This fact causes a delayed diagnosis of ATAAD, resulting in inappropriate intravenous thrombolysis and delay of surgical treatment. 65 One study reported that all of the 23 ATAAD patients with acute stroke showed extremely high D-dimer values (median 29.7 µg/ml, range: 4.2–406.2 µg/ml) on admission. 64 Another study showed a high D-dimer level (≥4.1 µg/ml) is highly sensitive (100%; specificity, 86%) for detecting ATAAD and useful for screening in acute stroke patients with 4.5 h of onset. 66 CT angiography (CTA) remains the best method for the definite diagnosis of ATAAD and should incorporate the aortic arch in neck/head vessel assessment of acute stroke patients.67,68 In hospitals where CTA is not available readily, D-dimer measurement would be useful for rule-in and rule-out of ATAAD in acute stroke patients.
Limitation of D-dimer measurement in acute stroke
Currently, many different assays using different monoclonal antibodies for D-dimer measurement are used in clinical practice. Thus, the results as cut-off values from studies using one assay cannot simply be extrapolated to another. 69 In addition, D-dimer measurement has lack of a standardized unit of measure. There are two different units used to describe D-dimer mass as purified D-dimer units (DDUs) and fibrinogen equivalent units (FEUs); 1 µg/ml of D-dimer as measured in DDU is about equal to 2 µg/ml in FEU. However, many reports did not clearly describe which mass unit they used. 70 Therefore, clinicians need to be aware of the limitation of D-dimer values and characteristics of the particular D-dimer assay at their institution.
Another limitation is low specificity of D-dimer values. D-dimer levels elevate more or less in acute phase of ischemic stroke on underlying pathophysiology. Furthermore, many thrombotic diseases and specific conditions in which the coagulation system is activated can impact on D-dimer levels. Therefore, slight D-dimer elevation in acute stroke may be non-specific. However, extreme high D-dimer levels suggest a specific stroke etiology or concomitant disease. 71 We demonstrate median D-dimer values in acute stroke and non-stroke condition just for a reference in routine practice, although D-dimer values among different studies are not comparable due to aforementioned limitation (Figure 1). The presence of cancer, VTE, and acute aortic dissection should be considered in acute stroke patients with higher D-dimer as more than 3 µg/ml (FEUs), when DIC and other conditions as trauma and post-surgery are excluded. Further studies are needed for biomarkers that reflect coagulation status more specifically.
The timing of D-dimer measurement in acute stroke remains undefined. As D-dimer values from most studies in this review were measured at admission or within a couple of days, earlier measurement after admission is more evidence based. In terms of ESUS/cryptogenic stroke patients, it may be preferable to measure when it is suspected after initial extracranial/intracranial artery, brain and heart workup at admission completed (days 3–4). It should be noted that D-dimer values are influenced by acute thrombolytic treatment as alteplase and tenecteplase inducing D-dimer elevation that peaks after 1 to 3 h and persists for up to 72 h.72–74 Routine blood sampling for D-dimer at ED arrival would be another strategy to avoid the influence of acute treatment.
Future directions
Standardization and harmonization of D-dimer measurement and reporting are needed to increase confidence that individual study results can translate to clinical practice.
D-dimer has the potential to influence treatment decision making in secondary prevention of cryptogenic stroke/ESUS. NAVIGATE ESUS and RE-SPECT ESUS have failed to show that DOACs provide more benefit than aspirin in the secondary prevention of ESUS.75,76 However, a recent review of ESUS suggested there may be a subgroup with occult embolic mechanisms likely to respond to anticoagulant therapy such as occult AF, PFO, atrial cardiopathy, or cancer. 77 As aforementioned, high D-dimer levels are suggestive of occult AF and cancer in ESUS patients. Therefore, future ESUS trials should include baseline D-dimer levels to determine if the high values identify the subgroup that may benefit from anticoagulation.
Another potential use of D-dimer would be treatment monitoring of anticoagulant by serial measurements. It is known that elevated D-dimer levels in patients with AF drop over time by anticoagulants such as warfarin or DOACs.19,78 Nakatani et al. 79 reported the low time in therapeutic range <67% under warfarin therapy in AF patients was associated with the increase in D-dimer level. Mahe et al. 80 showed that D-dimer increase during the follow-up in AF patients predicted higher risk of cardiovascular events in the following months, whereas D-dimer level in patients without events kept stable. Furthermore, Zhang et al. suggested D-dimer-guided adjustment of anticoagulation intensity could reduce stroke events in patients after mechanical heart valve replacement. 81 Some studies reported successful D-dimer reduction by anticoagulant predicted less recurrent stroke in patients with active cancer.48,56,58 Thus, serial measurement of D-dimer under anticoagulation could be helpful in predicting recurrent stroke and guiding clinicians to modify the intensity of anticoagulation and select appropriate anticoagulant agents. Future studies are required to confirm whether D-dimer-tailored anticoagulation strategy can be effective for secondary prevention in cardiogenic and cancer-related stroke. Several ongoing studies (Clinical trials.gov. ID NCT03570281 [Edoxaban vs. Enoxaparin in cancer-related stroke] and NCT02743052 [an observational study for anticoagulant in cancer-related stroke]) are using D-dimer levels to evaluate the effects of anticoagulant in patients with active cancer patients.
D-dimer is already routinely measured in acute ischemic stroke in some stroke centers, especially in East Asian counties. Yet current literature is insufficient to recommend routine D-dimer measurement on admission in stroke patients. Large prospective cohort studies are needed to demonstrate the long term cost-effectiveness of routine testing through reduced recurrent stroke risk; and/or early VTE/occult cancer detection.
Conclusion
In conclusion, accumulating data suggest the utility of D-dimer test in the management of ischemic stroke in some certain settings. The most useful setting of D-dimer measurement would be in stroke with active cancer. D-dimer can be used for diagnosis and recurrent stroke risk evaluation in cancer-related stroke. D-dimer measurement would be also helpful in cryptogenic stroke. High D-dimer levels are suggestive of occult cancer, undetected cardiac embolic source as occult AF and VTE causing paradoxical embolism. In addition, D-dimer may be a potential marker for treatment decision and monitoring in the future. A proposed flowchart of D-dimer measurement for acute stroke management is shown in Figure 2. Although evidence addressing this is still limited, future studies would clarify the role of D-dimer measurement in ischemic stroke.
Proposal of D-dimer measurements in the management of acute ischemic stroke.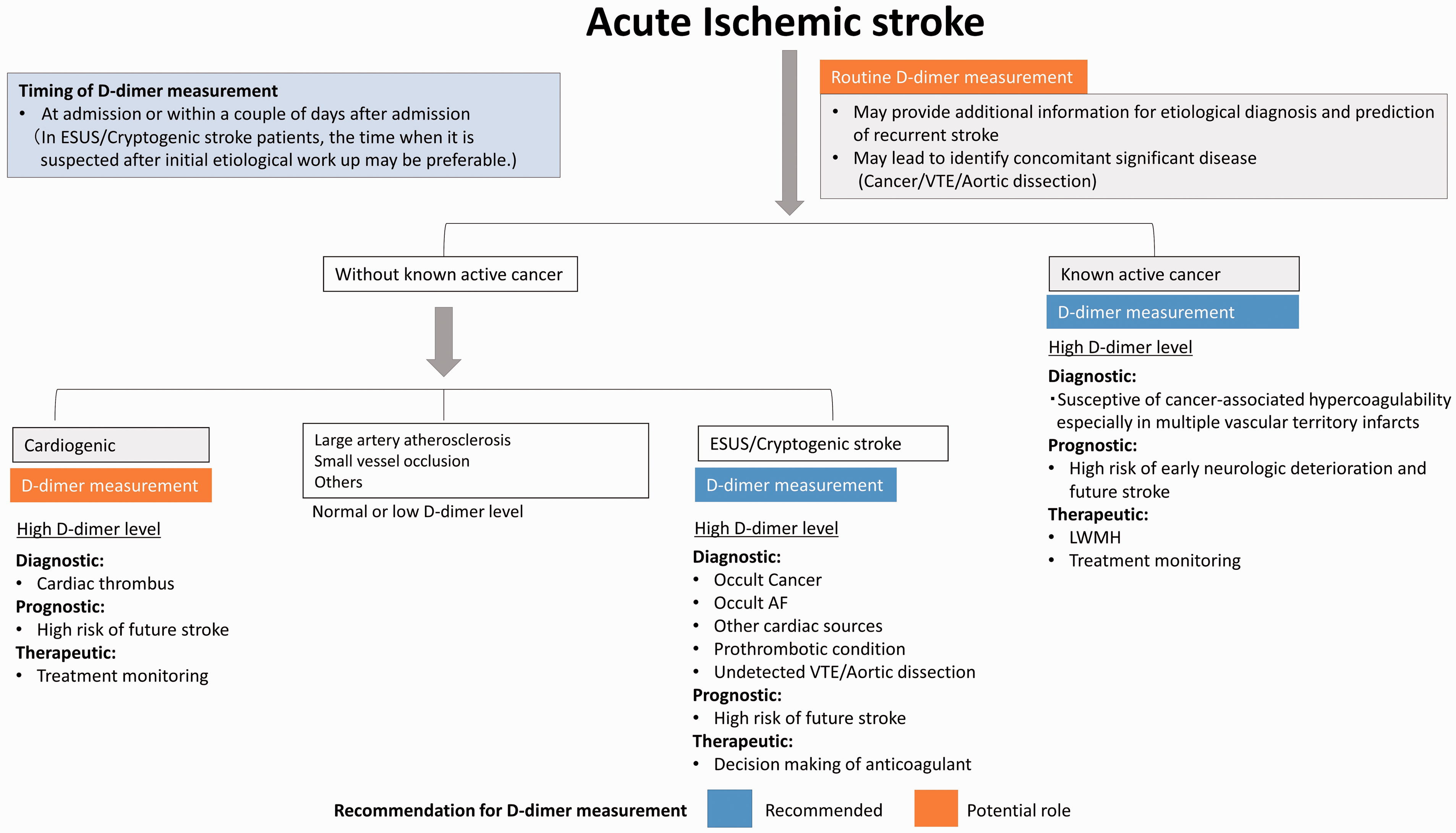
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest. Dr. Demchuk received honoraria from Bristol-Myers Squibb, Pfizer, Bayer, and Servier.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.