
Abstract
Background
Stroke and transient ischemic attack confer greater risk of cognitive decline and dementia.
Aims
We used data from the Perindopril Protection Against Recurrent Stroke Study (PROGRESS), a blood pressure-lowering randomized controlled trial in stroke/transient ischemic attack. We evaluated overall and sex-specific differences in treatment effects for cognitive decline/dementia, as well as associations with vascular and stroke-specific predictors,considering death as a competing risk.
Methods
Multinomial logistic regression was used to estimate overall and sex-specific odds ratios (OR) (95% confidence intervals (CI)) for treatment effects and predictors associated with the risk of cognitive decline/dementia, and the women-to-men ratio of odds ratio (RORs).
Results
Over a median four years, 763 cognitive decline/dementia (30.9% women) were recorded in 5888 participants. Women had lower odds of cognitive decline/dementia than men (OR 0.78, 95%CI 0.63–0.95). Active treatment was associated with lower odds of cognitive decline/dementia (0.84, 0.72–0.98), with no evidence of sex difference. Higher education (0.96,0.94–0.98 (per year)) and baseline Mini-Mental State Examination (MMSE)) were associated with lower odds of cognitive decline/dementia (0.84,0.82–0.86 (per point higher)). Higher diastolic blood pressure (1.11,1.02–1.20 (per 10 mmHg)), low estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2 (1.27,1.03–1.58), and peripheral arterial disease (1.78,1.26–2.52) were associated with higher odds of cognitive decline/dementia. APOE ɛ4 was not associated with cognitive decline/dementia (1.05 (0.85–1.30)). Low eGFR was more strongly associated with cognitive decline/dementia in women than men (RORs, 1.60 (1.03–2.48)). Diabetes was more strongly associated with men than women.
Conclusions
Several risk factors were associated with cognitive decline/dementia in people with prior stroke/transient ischemic attack, with notable sex differences. Long-term cognitive sequelae of stroke should be considered to strengthen joint prevention strategies for stroke, cognitive decline, and dementia.
Introduction
In 2019, the World Stroke Organization called for joint prevention of dementia and stroke. 1 Current trends in global burdens of dementia and stroke projected 200 million stroke survivors and 106 million people with dementia by 2050, 2 with 30 million incident stroke and five million deaths from dementia every year thereafter. 2
Stroke and transient ischemic attack (TIA) are linked to worse cognition, accelerated cognitive decline (CD), and dementia.1,3–5 Epidemiological and genetic studies suggest overlapping susceptibility factors between CD, dementia, and stroke. 6 There are also reciprocal interactions between cerebrovascular disease and neurodegeneration at a pathological level.1,7,8
The Oxford Vascular Study (OxVasc) provided some clarity on how individual characteristics may predict these adverse outcomes. 6 Yet, several questions remain, including predictors for cognitive impairment not satisfying criteria for dementia and the generalizability to other ethnicities. 9 Death may preclude the development of dementia or CD, 7 but this important consideration of death as a competing risk has not been widely incorporated in prior studies of poststroke CD/dementia.
Further, while sex is an important effect modifier for many diseases including stroke and dementia, 10 sex differences in risk factors for CD/dementia have not been explored in stroke/TIA. A study in a general population, free of stroke at baseline, found that several risk factors are more strongly associated with incident stroke in women than men. 11 Considering the commonality of risk factors for stroke and dementia, sex can have a fundamental influence on their reciprocal relationship.
Aims
Given these evidence gaps, our study examined the overall, and sex differences in, effects of blood pressure (BP)-lowering treatments, major vascular and stroke-specific predictors associated with CD/dementia in people with prior stroke/TIA, including death as a competing risk, using the Perindopril Protection Against Recurrent Stroke Study (PROGRESS) randomized controlled trial (RCT).
Methods
Study design and participants
The main results from PROGRESS have been described elsewhere.12,13 In brief, PROGRESS was an RCT of 6105 individuals recruited from 172 collaborative centers in 10 countries (Australia, New Zealand, China, Japan, England, Ireland, France, Belgium, Italy, and Sweden) from 1995 to 1997. Participants were eligible to enter the study, with a history of cerebrovascular disease, including stroke/TIA (but not subarachnoid hemorrhage) in the previous five years. Participants were required to have no contraindication or clear indication for angiotensin-converting enzyme inhibitors use. After a four-week run-in period, participants were randomized to active treatment; a flexible regimen of perindopril (4 mg daily) for all participants, with/without the addition of indapamide (2.5 mg daily/2 mg in Japan); or matching placebo(s). Ethical approvals were obtained from institutional ethics committees of each collaborating center, and all participants provided written informed consent.
Measurement of putative risk factors
At study baseline, information about participant’s sex, birth date, age at highest level of education attained, ethnicity, and region of residence were collected; a history of concurrent diseases, including diabetes (insulin and non-insulin dependent), myocardial infarction, atrial fibrillation, and peripheral arterial disease (PAD); lifestyle habits including alcohol use and smoking were self-reported. Weight and height measurements were taken, and body mass index (BMI) was calculated. Repeated BP measurements were averaged to define baseline BP. Estimated glomerular filtration rate (eGFR) was calculated from serum creatinine measured at baseline, using the updated Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) 2021 equation14,15 and defined as low if <60 ml/min/1.73 m2. The Mini-Mental State Examination (MMSE) 16 was administered to assess cognitive function.
Stroke at baseline was categorized as (1) TIA/amaurosis fugax; (2) unknown stroke; (3) ischemic stroke only; (4) hemorrhagic stroke only; (5) ischemic and hemorrhagic stroke. Barthel Index of Activities of Daily Living (BI) 17 was used to assess disability, with higher BI indicating less disability. Poststroke dependency and recovery were assessed through the Lindley Questions 18 : “In the last two weeks has the patient required regular help with everyday activities?” (dependency question) and “Does the patient feel that he or she has fully recovered from previous cerebrovascular events?” (recovery question).
Lymphocytes were isolated from peripheral blood for subsequent DNA extraction and genotyping for APOE polymorphism (http://www.genevcanvas.org). 19 APOE was characterized as one of the six genotypes: ɛ2/ɛ2, ɛ2/ɛ3, ɛ2/ɛ4, ɛ3/ɛ3, ɛ3/ɛ4, or ɛ4/ɛ4. APOE ɛ4 status was recorded positive for ɛ3/ɛ4 or ɛ4/ɛ4 genotype.
Assessment of cognitive function, CD, and dementia
Both CD and dementia were pre-specified secondary outcomes in PROGRESS.
Cognitive function was assessed using MMSE at baseline, six-, and 12-month visits, then annually until end of the follow-up (Supplementary Figure 1). CD was defined as a three-point or more decrement on MMSE between baseline and last recorded score.
A two-phase screening and assessment process were implemented for dementia diagnosis over follow-up. If the participant screened positive for possible dementia, they were referred for formal diagnostic clinical assessment by a specialist experienced in diagnosing dementia. The clinical assessment for ascertaining dementia was conducted through interviews. Information was gathered via a checklist based on the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria. 19
For all cases that screened positive for dementia, the diagnosis made by the local specialist were further reviewed by a central Dementia Adjudication Committee comprising two neurologists. Dementia was defined as “certain dementia” or “fairly certain dementia” based on the adjudication. All screen-negative cases were classified as “no dementia.” Further details of the CD/Dementia assessment are presented in the supplementary methods.
Statistical analysis
Baseline characteristics by sex were summarized using mean (standard deviation) or median (interquartile interval) for continuous variables, and number (percentage) for categorical variables. Odds ratios (ORs) were estimated using multinomial regression models, with outcomes defined as (0) neither CD nor dementia nor death (reference); (1) CD or dementia, regardless of whether the participants died before the end of follow-up; (2) the competing risk of death preceding CD or dementia. Since the onset of CD and dementia are highly insidious, time to event models may not be reliable.
The effect of BP-lowering treatment in PROGRESS on the risk of CD and dementia has been reported elsewhere 5 ; the present study expands on this by reporting the effects of randomized treatment effects, and a comprehensive list of genetic, cardiometabolic, and stroke-specific predictors by sex and considers competing risk of death. Randomized treatment effects (overall and by combination or single-drug therapy) on the risk of CD/dementia remain unadjusted, consistent with the original statistical analysis plan. 12
The association between each predictor with CD/dementia was explored in two sets of model adjustment: (1) “basic-adjusted” models, adjusted for sex, age, education, region, and randomized treatment; (2) “fully-adjusted” models, in addition to basic adjustments, different sets of a priori covariates (MMSE, systolic blood pressure (SBP), BMI, smoking, alcohol use, diabetes) were included to avoid over-adjustment, for each predictor. The specific adjustment strategy for each model is presented in the supplementary methods.
To address effect modification by sex, associations between predictors and multinomial outcomes were investigated by sex-disaggregated analyses, and the interaction term between each predictor and sex was used to obtain the respective women-to-men ratio of ORs (RORs). 20
Given the robust dementia adjudication in PROGRESS, differential effects of treatments and predictors on CD and dementia as stand-alone multinomial outcomes were examined, defined as (0) had neither CD nor dementia (reference category); (1) had CD only without dementia; (2) had dementia (including CD); (3) death preceding any CD or dementia during the study, using the aforementioned adjustment strategies.
Since the present study focuses on CD and dementia as outcomes of interest, results on death were not presented. Complete case analyses were undertaken and performed in RStudio Version 4.0.3 (R Core Team, 2020).
Results
Baseline characteristics
Characteristics of participants by sex in PROGRESS.
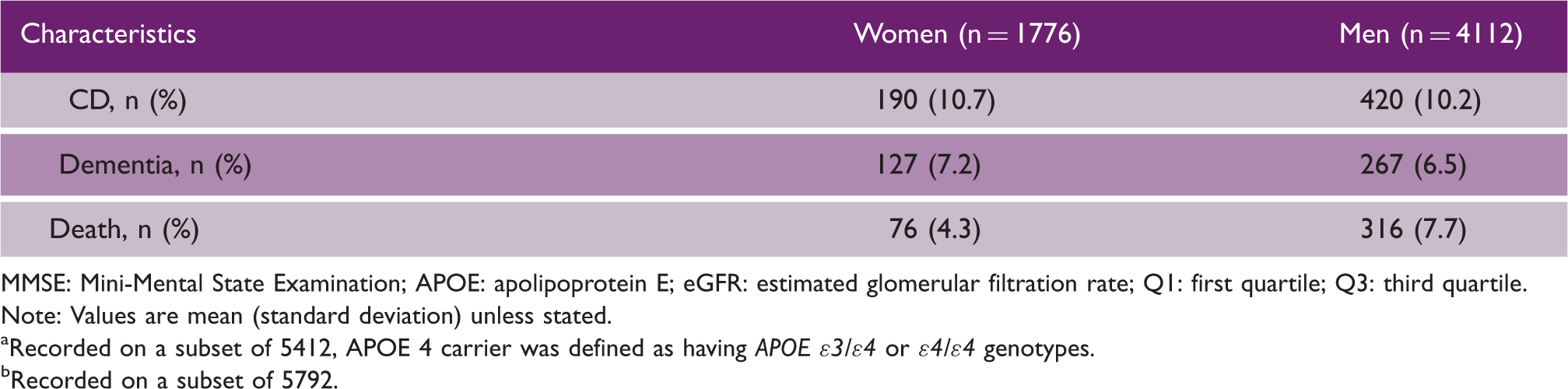
MMSE: Mini-Mental State Examination; APOE: apolipoprotein E; eGFR: estimated glomerular filtration rate; Q1: first quartile; Q3: third quartile.
Note: Values are mean (standard deviation) unless stated.
Recorded on a subset of 5412, APOE 4 carrier was defined as having APOE ɛ3/ɛ4 or ɛ4/ɛ4 genotypes.
Recorded on a subset of 5792.
Follow-up
During four years’ (median) follow-up, 763 CD/dementia (30.9% women) (CD: n = 610, 31.1% women; dementia: n = 394, 32.2% women; CD and dementia: n = 241, 33.6% women) and 392 deaths were recorded (19.4% women) (Table 1). A time chart of PROGRESS was provided (Supplementary Figure 1).
Randomized treatment effects
Active treatment was associated with lower odds of CD/dementia (OR, 0.84, 95%CI (0.72–0.98)), with no evidence of a sex difference (p = 0.17) (Figure 1). Active combination therapy was associated with lower odds of CD/dementia (0.81 (0.66–0.99)) compared with double placebo, though not for single-drug therapy (0.88 (0.70–1.11)). No sex difference was observed for combination or single-drug therapy (p = 0.34, p = 0.15, respectively). Treatment effects by CD and dementia as stand-alone outcomes are presented in Supplementary Figure 2.
Randomized treatments and the association with CD/dementia in PROGRESS, overall and by sex and pre-specified treatment regimen.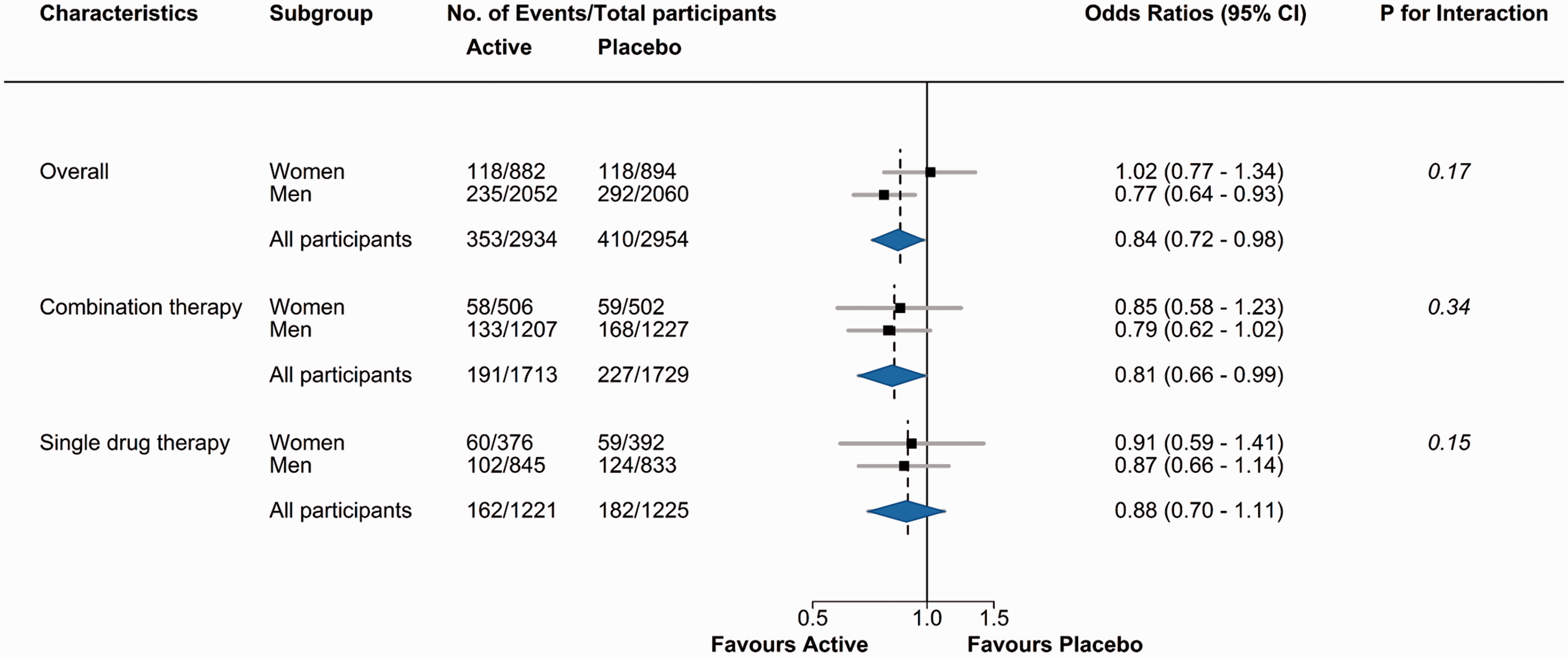
Comparative effects of predictors on CD/dementia
In the fully adjusted models, women had lower odds of CD/dementia than men (OR 0.78 (0.63–0.95)) (Figure 2). Longer years of education (0.96 (0.94–0.98) per year) and higher baseline MMSE (0.84 (0.82–0.86) per point higher) were associated with lower odds of CD/dementia. Higher diastolic blood pressure (DBP) (1.11 (1.02–1.20) per 10 mmHg), low eGFR (1.27,1.03–1.58), and PAD (1.78 (1.26–2.52)) were associated with higher odds of CD/dementia. Compared with those who had ischemic stroke only, TIA/amaurosis fugax was associated with lower odds of CD/dementia (0.72 (0.56–0.92)), participants who had hemorrhagic stroke only had higher odds of CD/dementia (1.74 (1.34–2.26)), and the odds of CD/dementia was over three times as high in those who had both ischemic and hemorrhagic stroke (3.23 (1.79–5.84)). A history of more than one cerebrovascular event was associated with higher odds of CD/dementia in comparison to one event (1.48 (1.23–1.78)). A negative response to the “recovery question” yielded an OR of 1.84 (1.54–2.20), and a positive response to the “dependency question” yielded an OR of 2.94 (2.40–3.60). Each five-point higher in BI was associated with 14% lower odds of CD/dementia (0.86 (0.84–0.89)). APOE ɛ4 was not associated with the risk of CD/dementia compared with non-carriers (1.05 (0.85–1.30)). Estimates from “basic-adjusted” models were broadly similar to the “fully-adjusted” models (Supplementary Figure 3). Results for CD and dementia as stand-alone outcomes are presented in the supplementary results.
Odds ratios (ORs), with 95% confidence intervals (CIs), for the associations between putative risk factors and cognitive decline/dementia in PROGRESS, after full adjustments. All models adjusted for sex, age, education (age at completion of highest education), region (Asia versus non-Asia), and randomized treatments. Sex, age, education, and region were further adjusted for MMSE, systolic blood pressure, BMI, smoking status, alcohol use, and diabetes. MMSE and APOE ɛ4 status were further adjusted for systolic blood pressure, BMI, smoking status, alcohol use, and diabetes; systolic and diastolic blood pressure were further adjusted for MMSE, smoking status, alcohol use, and diabetes; eGFR was further adjusted for MMSE, systolic blood pressure, smoking status, alcohol use, and diabetes; BMI was further adjusted for MMSE, systolic blood pressure, smoking status, alcohol use, and diabetes; smoking status, alcohol use, diabetes, myocardial infarction, atrial fibrillation peripheral arterial disease were further adjusted for MMSE; all stroke-related variables were only adjusted for sex, age, education, region, and randomized treatments. All analyses accounted for the competing risk of death.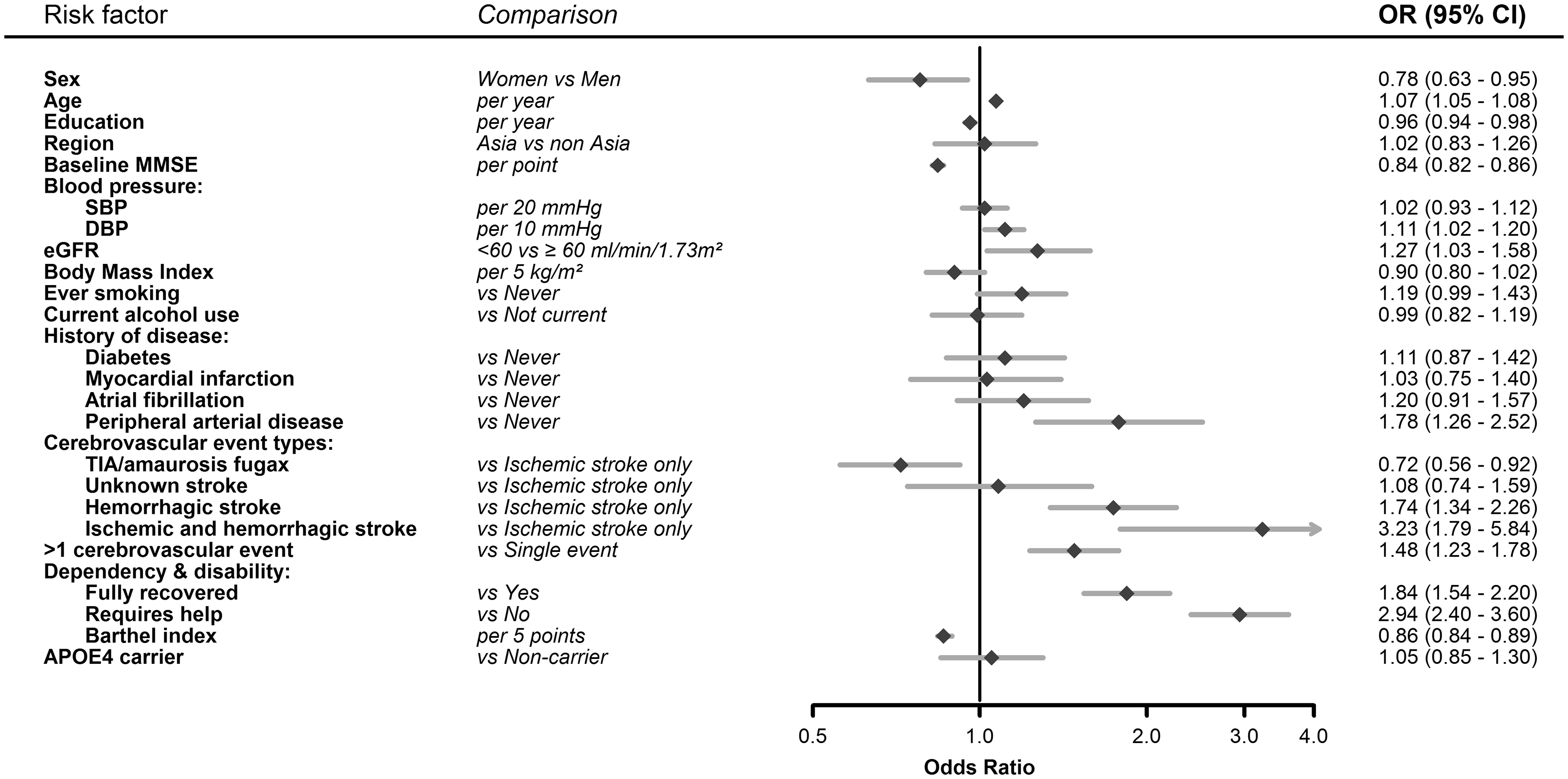
Effect modification by sex
Diabetes was more strongly associated with CD/dementia in men compared with women (women-to-men ROR, 0.54 (0.30–0.98)) (Figure 3). Low eGFR was more strongly associated with CD/dementia in women compared with men (ROR,1.60 (1.03–2.48)). Higher BI was observed as less protective for CD/dementia in women than men (ROR, 1.07 (1.00–1.14)).
Association between risk factors and cognitive decline/dementia—disaggregated by sex (women and men) in PROGRESS. Odds ratios and women-to-men ratio of odds ratios from multivariable model with interactions, after full adjustments. All models adjusted for age, education (age at completion of highest education), region (Asia versus non- Asia), and randomized treatments. Age, education, and region were further adjusted for MMSE, systolic blood pressure, BMI, smoking status, alcohol use, and diabetes. MMSE and APOE ɛ4 status were further adjusted for systolic blood pressure, BMI, smoking status, alcohol use, and diabetes; systolic and diastolic blood pressure were further adjusted for MMSE, smoking status, alcohol use, and diabetes; eGFR was further adjusted for MMSE, systolic blood pressure, smoking status, alcohol use, and diabetes; BMI was further adjusted for MMSE, systolic blood pressure, smoking status, alcohol use, and diabetes; smoking status, alcohol use, diabetes, myocardial infarction, atrial fibrillation peripheral arterial disease were further adjusted for MMSE; all stroke-related variables were adjusted for age, education, region, and randomized treatments only. All analyses accounted for the competing risk of death.
CD and dementia as standalone outcomes
Results for treatment effects and risk factors associated with CD and dementia considered as stand-alone outcomes are presented in Supplementary Figures 2, 4 and 5.
Multinomial regression versus logistic regression
Results for comparing multinomial regression with logistic regression models, which consider death as a competing risk, with traditional logistic regression models, that include death as “no-event” are presented in Supplementary Table 2.
Power calculation
Supplemental Table 3 illustrates the power for detecting various maximum detectable women-to-men risk ratios for CD/dementia.
Discussion
In this new study of the PROGRESS trial, active treatment was associated with lower odds of CD/dementia, with no evidence of sex difference. Longer education years and baseline MMSE were each associated with lower odds of CD/dementia; higher DBP, low eGFR, and PAD were associated with higher odds of CD/dementia. For sex differences, women had lower odds of CD/dementia than men, with low eGFR was more strongly associated with CD/dementia in women, but diabetes was more strongly associated in men than women.
Men overall had higher odds of CD/dementia than women in our study, which can be explained by the generally worse baseline vascular risk profile in men than women. Low eGFR was more strongly associated with CD/dementia in women than men, whereas diabetes was more strongly associated in men than women. While sex disparities in risk management exist, underlying biological differences can also have contributed to sex-specific excess risk of CD/dementia in stroke/TIA observed.
While sex difference was not evident, intensive BP-lowering treatment was associated with lower odds of CD/dementia, specifically in the combination therapy regimen compared with matching placebos. 21 While there are clear benefits for BP lowering in reducing the risk of recurrent stroke, 22 it remains unclear whether hypertension treatments preserve cognition in people with stroke/TIA through other mechanisms. No other stroke trials have demonstrated that BP-lowering treatments provided beneficial effect on cognition.23–26
In comparison to previous studies that examined multiple predictors for dementia and cognitive function in people with stroke/TIA, the OxVasc study 6 found that age, baseline cognition, low education, previous stroke, event severity, dysphasia, premorbid dependency, leukoaraiosis, and diabetes were associated with greater risk of dementia. A pooled analysis from the Stroke and Cognition (STROKOG) consortium found diabetes was the strongest predictor for poorer cognitive function. 3
Our observational findings showed that higher DBP, but not SBP, was associated with higher odds of CD/dementia (and dementia alone) in patients with prior stroke/TIA. In contrast, in the OxVasc study, premorbid higher values of DBP and SBP were predictive of an increased risk of dementia. 27
A history of PAD has been associated with a greater risk of dementia in stroke patients. 28 Low ankle-brachial index has been consistently linked to a greater risk of cognitive impairment and dementia. 29 PAD has important implications for the management and prevention of stroke, 30 whereby ankle-brachial index, and other markers related to PAD, may help to screen and identify those at high risk of CD and dementia after stroke.
Low eGFR was identified as a risk factor for CD/dementia in our study. Previous studies on eGFR as a risk factor for dementia in general populations showed mixed results. A meta-analysis concluded only modest evidence for eGFR < 60 mL/min/1.73 m2 associated with dementia due to substantial heterogeneity across studies. 31 The Systolic Blood Pressure Intervention Trial (SPRINT) in patients with high cardiovascular risk (excluding those with stroke or diabetes) 32 showed that eGFR < 60 mL/min/1.73 m2 was associated with a higher risk of mild cognitive impairment or dementia. 33 There is a paucity of evidence for such associations in patients with prior stroke/TIA. Renal dysfunction increases the risk of stroke and carotid atherosclerosis, 31 and in stroke patients, chronic kidney disease has been reported to contribute to stroke severity, subclinical cerebrovascular abnormalities, and poorer functional outcomes 34 ; it also complicates poststroke management and secondary prevention. 35 While the causal relationships are unclear, strategies to manage renal outcomes in stroke patients, and prevent stroke in people with renal dysfunction may be important in preventing downstream cognitive consequences. 35
Strengths and limitations
A major strength of the study is the adjudicated outcomes of dementia and the large sample size of people with prior stroke. Consideration of the competing risk of death is important in the context of late-life conditions, such as CD and dementia. Notwithstanding the validity of the composite outcome of CD/dementia remain debatable, our sensitivity analysis showed that the findings for dementia were robust, and the composite outcome including CD allowed for consideration of prodromal dementia.
Several limitations were: first, due to relatively short follow-up, together with the onset of CD and dementia being highly insidious, the direction of causality may be difficult to infer. Second, given that the PROGRESS is a clinical trial, generalizability may be limited. While the recent advances in stroke treatment and secondary prevention, mostly in the acute phase, have successfully increased the survival rate of stroke, there have been less therapeutics options for cognitive decline and dementia, and the effects of the stroke treatments on poststroke cognitive sequalae need to be better understood. As such, the generalizability of the results from the current study may also be influenced by the secular changes in stroke therapeutics. Third, the initiation of PROGRESS preceded the NIH Stroke scale/score; thus, there was a lack of information on stroke severity. Lastly, the definition of CD may be less reliable due to limited psychometric properties of MMSE, than other more comprehensive tools used in more recent trials.
Conclusions
Our study showed that several vascular risk factors are associated with CD and dementia in people with prior stroke/TIA, with evidence for sex differences in some risk factors. This may help with patient selection in future trials and inform clinicians managing cognitive outcomes in stroke patients. With the improvement in survival rate of stroke, long-term cognitive sequelae of stroke, together with sex differences in predictors for CD/dementia, the study findings should be considered in order to strengthen the joint prevention strategies for stroke and dementia and move towards bespoke medicine.
Supplemental Material
sj-pdf-1-wso-10.1177_17474930211059298 - Supplemental material for Sex differences in predictors for cognitive decline and dementia in people with stroke or transient ischemic attack in the PROGRESS trial
Supplemental material, sj-pdf-1-wso-10.1177_17474930211059298 for Sex differences in predictors for cognitive decline and dementia in people with stroke or transient ischemic attack in the PROGRESS trial by Jessica Gong, Katie Harris, Christophe Tzourio, Stephen Harrap, Sharon Naismith, Craig S Anderson, John Chalmers and Mark Woodward: On behalf of the NAVIGATE ESUS MRI Substudy Investigators in International Journal of Stroke
Footnotes
Data availability
Individual, de-identified participant data used in these analyses will be shared by request from any qualified investigator following approval of a protocol and signed data access agreement via the Research Office of The George Institute for Global Health, Australia.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CSA reports grants, honoraria, and travel reimbursement from Takeda. JC reports research grants from the NHMRC and Servier for the ADVANCE trial and ADVANCE-ON post-trial follow-up, and honoraria for these studies at scientific meetings, a research grant from Idorsia for the SPIRIT study of Resistant Hypertension. MW does consultancy for Amgen, Freeline, and Kirin outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PROGRESS was funded by Servier, the Health Research Council of New Zealand, and the Australian National Health and Medical Research Council (NHMRC). JG is supported by Scientia PhD Scholarship from the University of New South Wales. CSA holds an NHMRC Senior Investigator Research Fellowship. MW holds a NHMRC Investigator Grant (grant number APP1174120) and MW and JC are supported by the Program Grant (grant number APP1149987). The funders had no role in the study design, collection, analysis, interpretation of data, writing of the manuscript or in the decision to submit the article for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.