
Abstract
Background:
For neurodegenerative diseases, the inter-individual variability in the functional response to pathology is explained by the construct of cognitive reserve (CR). We aimed to evaluate the association of CR with stroke outcome to improve the understanding of its inter-individual variability and prediction.
Methods:
The peer-reviewed protocol was preregistered on PROSPERO (CRD42021256175). The systematic review and meta-analysis followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), Meta-analysis of Observational Studies in Epidemiology (MOOSE), and CHecklist for critical Appraisal and data extraction for systematic Reviews of prediction Modelling Studies (CHARMS) reporting guidelines. Original studies reporting the association between CR-proxies (e.g. level or years of education, occupational attainment) and measures of non-cognitive stroke outcome (e.g. National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale, Barthel Index, Functional Independence Measure) were selected. Risk of bias was assessed using Quality In Prognosis Studies (QUIPS). Estimates were pooled using a random-effects model.
Results:
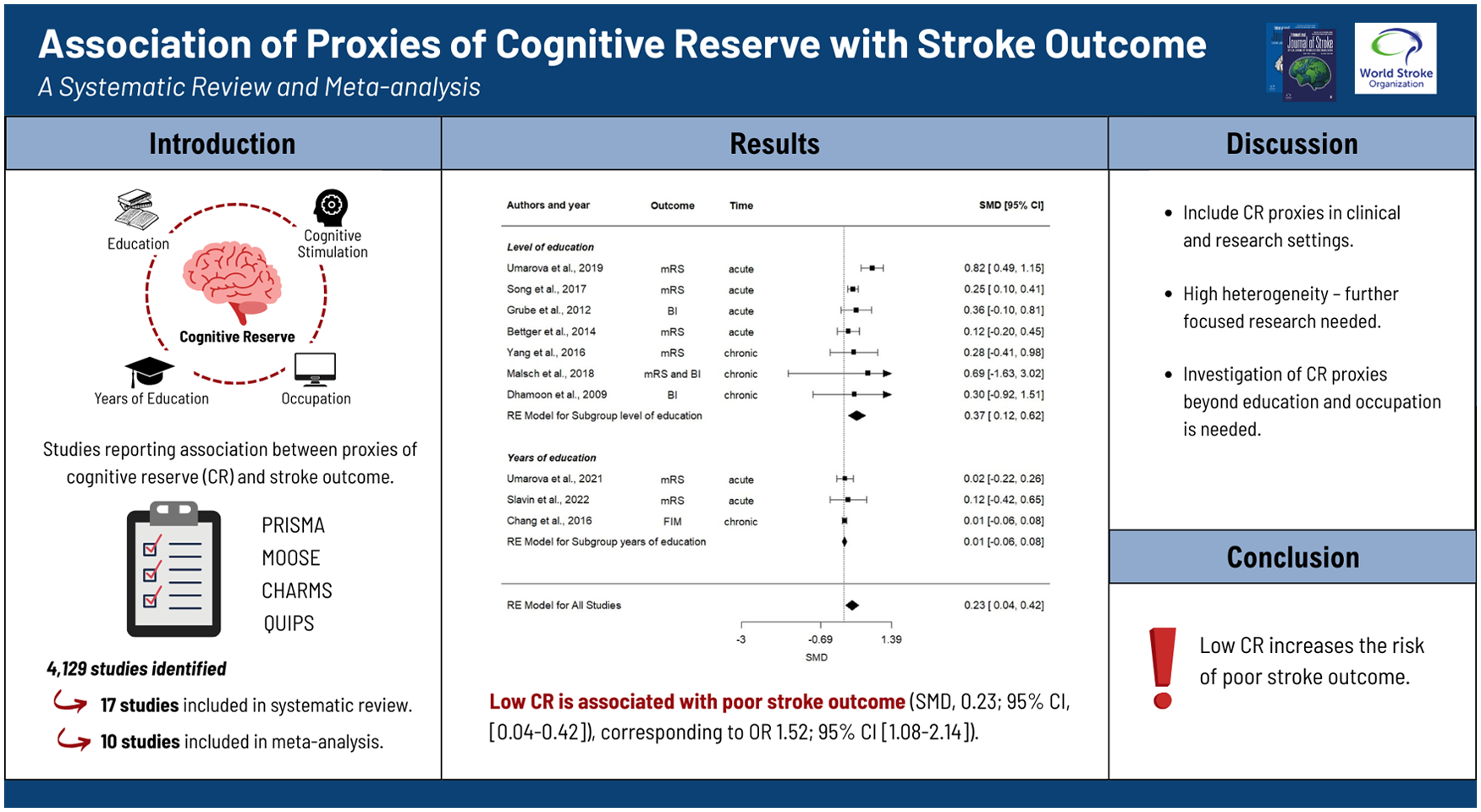
Of 4129 studies identified, 17 were included in the systematic review. Based on the quality check, 10 of them involving 19,308 patients were included in the meta-analysis, whereby only five studies directly addressed the association of CR-proxies with stroke outcome. Pooled standardized mean differences (SMDs) showed evidence for the association of low CR with poor stroke outcome (SMD = 0.23; 95% confidence interval (CI) = 0.04 to 0.42 corresponding to odds ratio (OR) = 1.52; 95% CI = 1.08 to 2.14). Subgroup analysis showed a greater association of level of education (SMD = 0.37; 95% CI = 0.12 to 0.62) and occupational attainment (SMD = 0.34; 95% CI = 0.10 to 0.57) with stroke outcome, as compared to years of education (SMD = 0.01; 95% CI = −0.06 to 0.08). The effect of CR was greater in the acute-subacute stroke phase (⩽3 months post-stroke, SMD = 0.28; 95% CI = 0.04 to 0.52) than in the chronic phase (SMD = 0.01; 95% CI = −0.06 to 0.08).
Conclusion:
We found evidence that CR explains inter-individual variability in stroke outcome and thus may improve its prediction. Low CR increases the risk of poor stroke outcome, and its proxies should be considered in both clinical and research settings. However, we observed high heterogeneity across studies, and further research with specific focus on this topic and CR-proxies extending beyond educational and occupational attainment is needed.
Introduction
To achieve further improvements in stroke outcome, there is an urgent need for individualized prognosis. This will facilitate the implementation of individually tailored therapeutic approaches, ultimately enhancing patient care. 1 In recent years, several global studies have proposed prognostic models to predict clinical and functional outcomes after stroke.2–5 However, due to the heterogeneity of the condition and the studies themselves, understanding of inter-individual variability and accurate prediction of stroke outcome require further research. While several main risk factors for unfavorable stroke outcome have been identified, 5 the role of behavioral and socioeconomic factors remains a topic of debate.
The concept of cognitive reserve (CR) has been proposed to explain the inter-individual variability in the clinical manifestation of normal aging and neurodegeneration.6,7 CR is known to mitigate the impact of brain insults, where higher reserve has been associated with better cognitive outcomes across various neurological conditions.7,8 Namely, CR embodies the active process of coping with aging or brain damage using compensatory strategies that have been boosted throughout one’s lifetime through various cognitive exposures. 6 Thus, CR can only be measured indirectly, through proxies and questionnaires.9,10 The most widely accepted CR-proxies are years or level of education, occupational attainment, cognition-stimulating activities, social activities, bilingualism, and crystallized or verbal intelligence.8,9–11 Similar to its role in neurodegeneration, there is increasing evidence supporting the protective influence of CR on post-stroke cognition.12–18 CR is associated with better outcomes in the context of a brain health insult, so its association with better outcomes in stroke seems intuitive. However, studies investigating its impact on non-cognitive stroke outcome are scarce. 19 Stroke recovery is defined as behavioral compensation provided by remaining and newly developed brain circuits that results in altered and/or new response strategies. 20 Providing higher reserve, network efficiency and compensation, 8 higher CR may be associated with better cognitive as well as non-cognitive stroke outcomes. Even notwithstanding the assumption that the impact of CR on functional outcome measures might be purely cognition-driven, it remains to be ascertained whether the effect is significant enough to be considered in clinical practice and prognostic models and whether it varies across different post-stroke time points. It is important to emphasize that clinical trials and prognosis studies do not routinely consider factors such as educational attainment.
Altogether, models operating with cardiovascular, metabolic, neurological, and neuroradiological factors cannot fully account for the inter-individual variability in stroke outcomes.21–23 CR-proxies, which reflect life-course cognitive enrichment and adaptability, may offer additional explanatory value for this variability and improve stroke outcome prediction. The absence of a data synthesis specifically targeting the relationship between CR-proxies and global (non-cognitive) stroke outcome therefore represents a relevant knowledge gap that the present work aims to fill. We aimed to (1) investigate evidence for the association of CR with non-cognitive stroke outcome, (2) explore whether different CR-proxies demonstrate a distinct association with stroke outcome, and (3) explore whether the effect of CR on stroke outcome varies depending on the stroke phase (i.e. acute vs. chronic stroke phase).
Methods
The study was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), 24 the Meta-analysis of Observational Studies in Epidemiology (MOOSE), 25 and Enhancing the Quality and Transparency of Health Research (EQUATOR) 26 guidelines.
Search strategy and data source
We systematically searched the Cochrane, EMBASE, PubMed, and Web of Science electronic databases for English articles published between January 1, 1980, and March 10, 2022. We screened the reference lists of relevant studies and meta-analyses for additional publications. Relevant keywords and adapted medical subject heading (MeSH) terms for CR-proxies and measures of non-cognitive stroke outcome were used. The detailed search strategy is provided in Supplemental eAppendix 1.
Eligibility criteria
We included human studies reporting the association between CR-proxies and non-cognitive stroke outcome. Original prospective and retrospective cohort and cross-sectional studies, and controlled trials including >20 adults with a first-ever ischemic stroke were eligible for inclusion. From studies with combined populations (e.g. including patients with previous or hemorrhagic stroke or transient ischemic attack), we included only those with a proportion of first-ever ischemic stroke patients >80% or that made adjustments for previous stroke or stroke type in the statistical model. This was done to reduce the heterogeneity of the studies and the risk of bias due to the different pathophysiological mechanisms, recovery trajectories and prognoses, and therefore outcomes, after transient ischemic attack (TIA) and hemorrhagic or recurrent stroke. 27 Studies analyzing the impact of CR on chronic stroke outcome >5 years after stroke onset were excluded to avoid the uncontrolled bias introduced by new critical events, neurodegenerative diseases or individuals’ differences in aging, and new critical comorbidities such as tumors and their management on such a long-term follow-up period. In studies with different assessment times, data from the first and most complete visit were extracted. Studies operationalizing CR as socioeconomic status (e.g. household or individual-level measures of income, wealth or assets, caste, deprivation, poverty, and material ownership) were excluded for the following reasons. First, the socioeconomic status does not represent cognition-stimulating lifetime activities and, correspondingly, is not a CR-proxy,11,28 although it might be indirectly associated with CR. Second, socioeconomic status is often associated with restricted health care access. Third, recent systematic reviews already addressed the impact of socioeconomic status on stroke.29–31
Meta-analyses, case reports, meeting abstracts or posters, studies published in languages other than English, and studies published in non-peer-reviewed journals were excluded. In case of duplicate reports of the same data set, only the most comprehensive study report was included to avoid double counting of cohorts.
Measures
The exposure of interest was the CR operationalized through following proxies: years of education, level of education (e.g. illiterate, primary school, high school), occupational attainment (e.g. manual, non-manual, professional, not working), intelligence, cognition-stimulation leisure activities, and similar measures. 27 The outcome of interest was the non-cognitive stroke outcome (i.e. stroke severity, functional disability, dependency, and activities of daily living) measured with validated and standardized clinical scores including the National Institute of Health Stroke Scale (NIHSS), modified Rankin Scale (mRS), Barthel Index (BI), and other activities of daily living scales.
Study selection and data extraction
The identified publications were imported into Zotero (https://www.zotero.org), and duplicates were removed. One author (L.G.) screened titles and abstracts of potentially relevant studies. Two authors (L.G. and R.M.U.) independently evaluated full texts for inclusion and exclusion criteria. Disagreements were resolved by consensus or by consulting a third reviewer (M.R.H.) for arbitration. Insufficient information for the evaluation of inclusion criteria (e.g. rate of non-ischemic stroke or history of stroke) led to study exclusion after its corresponding author was contacted for the required information.
Two authors (L.G. and R.U.) independently extracted data according to a pre-specified standardized data extraction form 27 in line with the CHecklist for critical Appraisal and data extraction for systematic Reviews of prediction Modelling Studies (CHARMS checklist), 32 or if necessary, extracted data from reported percentages, tables, or figures. Information on demographic and clinical characteristics, CR-proxies, and assessment of stroke outcome measures was extracted with the reported cut-offs and time of assessment since stroke. Confounding factors including presence of cardiovascular risk factors and comorbidities were recorded.
Publication bias assessment and quality of evidence
We examined publication bias using a funnel plot by visual assessment of asymmetry and statistically through the Egger test. 33 We evaluated certainty and strength of evidence according to the Grading of Recommendations, Assessment, Development and Evaluations (GRADE). 34
Risk-of-bias assessment
Two authors (L.G. and R.M.U.) independently assessed the risk of bias of all eligible studies using an adapted version of the Quality In Prognosis Studies (QUIPS) 35 tool that covers study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis and reporting. Judgments on the risk of bias were rated as “low,” “moderate,” or “high.” Disagreements were resolved by discussion and consensus. A third author (M.R.H.) was consulted for an external quality assessment of studies with R.M.U. as the first author.
Statistical analysis
Studies rated with a low or moderate risk of bias were included in the meta-analysis for further synthesis. We excluded high risk-of-bias studies from the meta-analysis in line with Cochrane recommendations 36 as they may produce a misleading or inaccurate summary of the true effect. In studies reporting more than one CR-proxy, the most completely reported one was integrated in the meta-analysis to ensure inclusion of independent samples and reduce the risk of bias. Conversely, all proxies were analyzed in the independent subgroup analyses. In studies reporting two outcome measures, we included only one in the meta-analysis to ensure the inclusion of independent samples only; we included the most frequently used outcome measure to increase study homogeneity.
According to the study protocol,
27
we extracted data for exposures and outcome measures reported as continuous and/or categorical variables. Ordinal exposures with >2 levels were dichotomized to low versus high CR according to the reported data distribution; consequently, odds ratios (ORs) were calculated with the resulting 2×2 contingency table (exposure × outcome). The category “retired” was excluded from the dichotomization, since it reflects an age-dependent class and not the occupational attainment per se. In case of insufficient data for the transformation, the corresponding author was contacted to complete the necessary data. As a reference category for exposures, we used “high CR”; as a reference for outcome, we used “poor outcome.” In studies using “low CR” as a reference, we transformed the originally reported measure of association (OR and 95% confidence interval (CI)) into 1/OR.
37
The resulting ORs and effect size were transformed into standardized mean difference (SMD) and standard error (SE) for synthesis that enabled analysis of both continuous and dichotomous outcome measures according to guidelines.37,38 Detailed information on the transformation is provided specifically for all included studies. The pooled SMD and SE were used as a measure of the association of low CR with poor stroke outcome. Pooled SMD and SE were calculated through random-effects meta-analysis, due to the expected substantial heterogeneity in reported CR-proxies and functional assessments.
27
Heterogeneity was assessed using the I2 and its 95% CI and Cochran Q statistics. To achieve the interpretability of SMD, we additionally represent it as OR for poor versus favorable outcome according to
Statistical analyses were performed using RStudio (Version 4.1.2, package metafor). Statistical significance was considered with two-sided tests with a P-value < 0.05.
Standard protocol approvals, registrations, and patient consents
The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO database CRD42021256175) and published as a peer-reviewed article in July 2022. 27 We used summary data from published manuscripts, and we did not use individual-level data, so informed consent or approval of the ethics committee was not required.
Data availability
Data not provided in the article because of space limitations may be shared at the request of any qualified investigator for purposes of replicating procedures and results.
Results
Of the 4129 articles identified, 17 fulfilled the inclusion criteria (Figure 1). Eligible studies were published between December 2002 and January 2022, and included a total of 22,604 patients with a mean age of 64.9 (SD = 7.8) years, and 8337 (36.9%) patients were female. The sample size ranged between 26 12 and 11,226 patients, 39 with a median of 443 included patients. The time point of outcome assessment ranged from hospital admission to 5 years post-stroke, with a median of 6 months post-stroke. Six studies12,15,40–43 were conducted in Europe, four studies44–47 in the United States, and seven studies39,48–53 in Asia. Sixteen studies12,39–53 reported rates of poor outcome with 6387 (28.4%) patients achieving it. Supplemental eTable 1 reports the data synthesis of the eligible studies; additional data and information were available for two articles.12,40
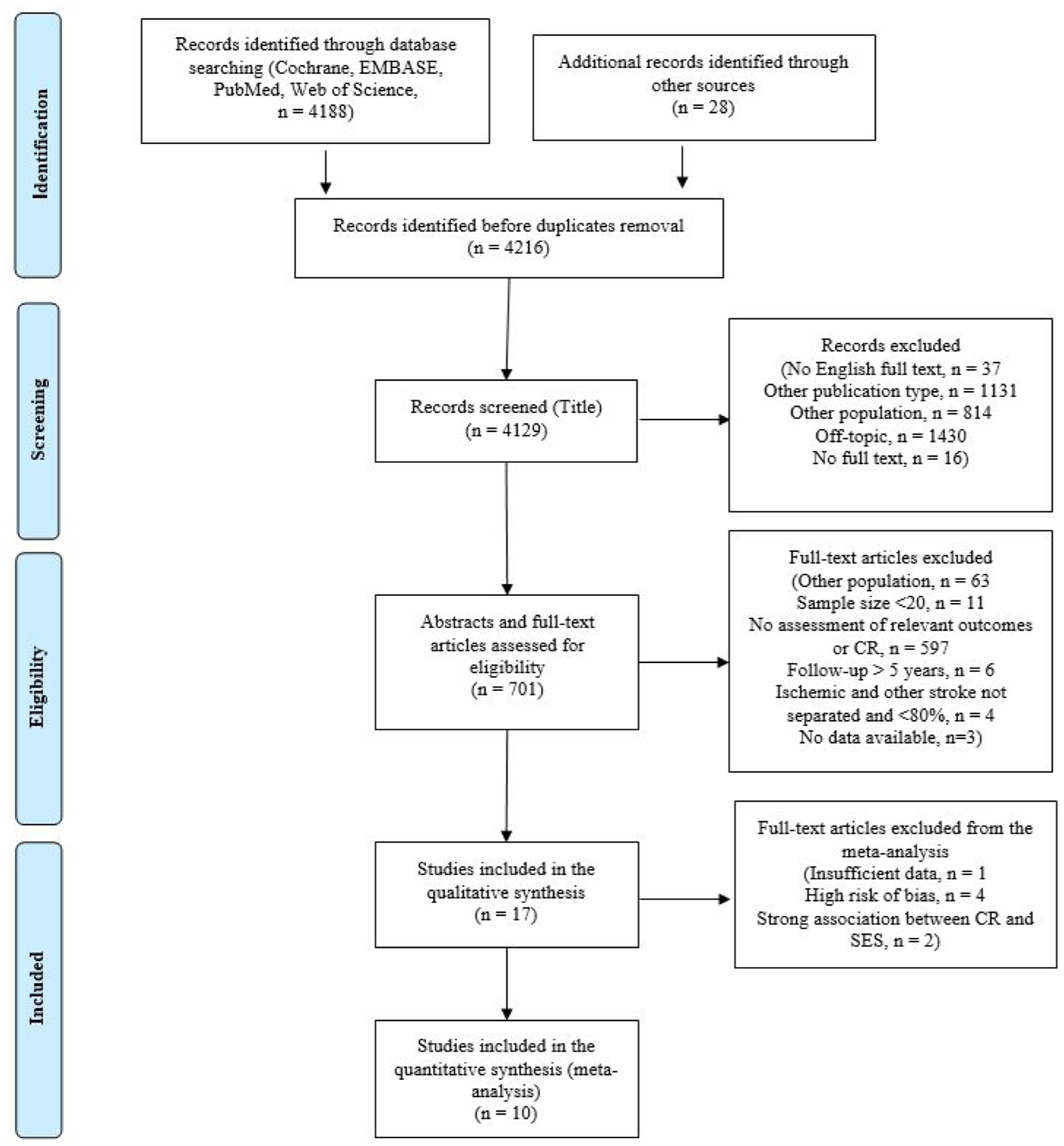
Flowchart of included studies. Abbreviations: CR, cognitive reserve; SES, socioeconomic status.
CR-proxies
Only five studies aimed to assess the association of CR with stroke outcome, others investigated CR-proxies among other socio-demographic variables. Four CR-proxies were reported in the eligible studies: 12 studies12,39–46,49,52,53 operationalized CR through level of education (categorical variable), six studies15,42,47,48,50,51 through years of education (continuous variable), seven studies39,40,44,47,50,51,53 through occupational attainment (categorical variable), and one study 12 through crystallized intelligence. However, IQ was not integrated in the meta-analysis as CR-proxy, since data were available for n < 20 patients. 27 Eight studies15,41,43,45,46,48,49,52 operationalized the CR through only one proxy.
Stroke outcome measures
Non-cognitive stroke outcome was assessed using four measures: NIHSS (two studies),12,15 mRS (13 studies),12,15,39,40,42–44,46,47,49,51–53 BI (five studies),41–43,45,50 and one study used the Functional Independence Measure (FIM). 48 Thirteen studies39–41,44–53 assessed stroke outcome through only one measure, whereas four studies12,15,42,43 through two measures. Three studies12,15,46 assessed stroke outcome in the acute/subacute phase (<3 months post-stroke), six studies39–41,44,47,51,54 at 3 months, six studies43,45,46,48,50–52 at 6 months, and five studies15,42,43,49,53 at 1 year post-stroke or later. Four studies15,43,46,51 had longitudinal design with two15,46 or three43,51 assessment time points.
Covariates
Adjusted measures of association were collected, but a core set of covariates was not established due to heterogeneity in covariate control across included studies (Supplemental eTable 1). Nevertheless, 14 studies controlled for certain risk factors and reported adjusted measures of association.
Risk-of-bias assessment
According to the QUIPS, the risk of bias was low in five studies (29.4%), moderate in eight studies (47.1%), and high in four studies (23.5%) (Supplemental eFigure 1). Overall, we assessed the risk of bias across all studies as moderate. Studies with a high risk of bias were excluded from the meta-analysis. We further excluded two studies with only moderate bias, due to a reported strong association between CR-proxy (lower level of education) and restricted health care access in these studies, providing the unresolved bias on functional outcome (detailed information on risk of bias and reason for exclusion are listed in Supplemental eTable 2).52,53
Meta-analysis
After the exclusion of studies with a high risk of bias, 11 studies remained eligible for the meta-analysis. Due to insufficient data to calculate the association of the prognostic factor (CR-proxy) either in a dichotomous or continuous way, we further excluded one study 46 from the meta-analysis. Finally, 10 studies with independent samples of 19,308 patients (mean age = 65.7 (SD = 12.1) years, 7122 [36.9%] female) were included in the meta-analysis (Supplemental eTable 3). All included studies reported measures of functional stroke outcome (mRS, BI, or FIM). Random-effects meta-analysis indicated evidence for the association of lower CR with poor stroke outcome (SMD = 0.23; 95% CI = 0.04 to 0.42; Figure 2). This corresponds to the OR of 1.52 (95% CI = 1.08 to 2.14) of lower CR for poor versus favorable outcome.
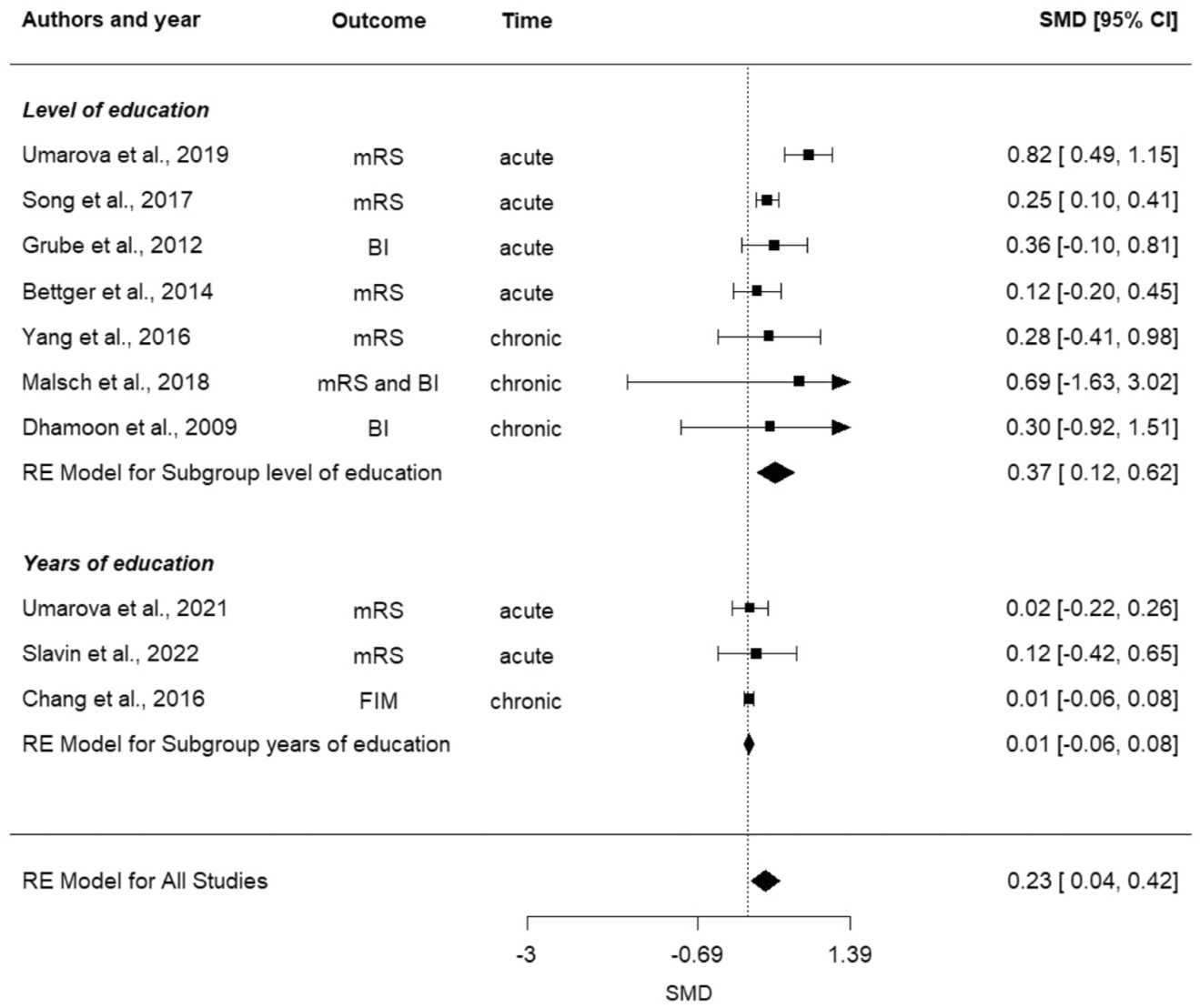
Forest plots of pooled SMD [95% CI] of studies reporting the evidence for the impact of CR on stroke outcome stratified for different CR-proxies. Abbreviations: BI, Barthel Index; CI, confidence interval; FIM, Functional Independence Measure; mRS, modified Rankin Scale; NIHSS, the National Institute of Health Stroke Scale; RE, random effect; SMD, standardized mean differences.
Publication bias and certainty of evidence
Funnel plots for all CR-proxies displayed asymmetry, but the Egger test indicated no evidence of publication bias (t = 1.8577, P = 0.1003, Supplemental eFigure 2). Considerable heterogeneity was observed across the ten studies (I2 = 75.5%, Q = 31.18, P < 0.001) but not when stratified for CR-proxies (level of education: I2 = 55.48%, Q = 11.32, P = 0.079; years of education I2 = 0.00%, Q = 0.18, P = 0.915; and occupational attainment I2 = 0.00%, Q = 0.54, P = 0.462).
We applied the GRADE framework 34 to assess the certainty of evidence. The certainty of evidence was rated as moderate for the following reasons: (1) moderate risk of bias due to the inherent limitations of the included studies, as only part of them directly addressed the association of CR-proxies with stroke outcome; (2) adequate imprecision as assessed by confidence intervals and the number of studies included; (3) no inconsistency was observed, as indicated by low heterogeneity (I2); (4) presence of indirectness, but no randomized studies are feasible in this context; and (5) moderate publication bias based on the funnel plot and the Egger test.
Subgroup-analyses
Association of different CR-proxies with stroke outcome
We performed a subgroup analysis of different CR-proxies. Studies operationalizing CR through the level of education (stratified as high vs. low) indicated evidence for the association of lower level of education with poor stroke outcome (SMD = 0.37; 95% CI = 0.12 to 0.62) (Figure 2). Similarly, studies operationalizing CR through occupational attainment (high vs. low) indicated that lower occupational attainment was associated with poor stroke outcome (SMD = 0.34; 95% CI = 0.10 to 0.57). Conversely, no significant evidence for the association with outcome was observed in studies operationalizing the CR through years of education as a continuous variable (SMD = 0.01; 95% CI = −0.06 to 0.08).
Association of CR with acute-subacute versus chronic stroke outcome
The subgroup analysis of studies within the first 3 months post-stroke indicated evidence for the association of lower CR with poor outcome in the acute and subacute stroke phase (SMD = 0.28; 95% CI = 0.04 to 0.52; Figure 3). Conversely, the subgroup analysis of studies assessing outcome >3 months post-stroke indicated no significant evidence for this association in the chronic stroke phase (SMD = 0.01; 95% CI = −0.06 to 0.08; Figure 3).
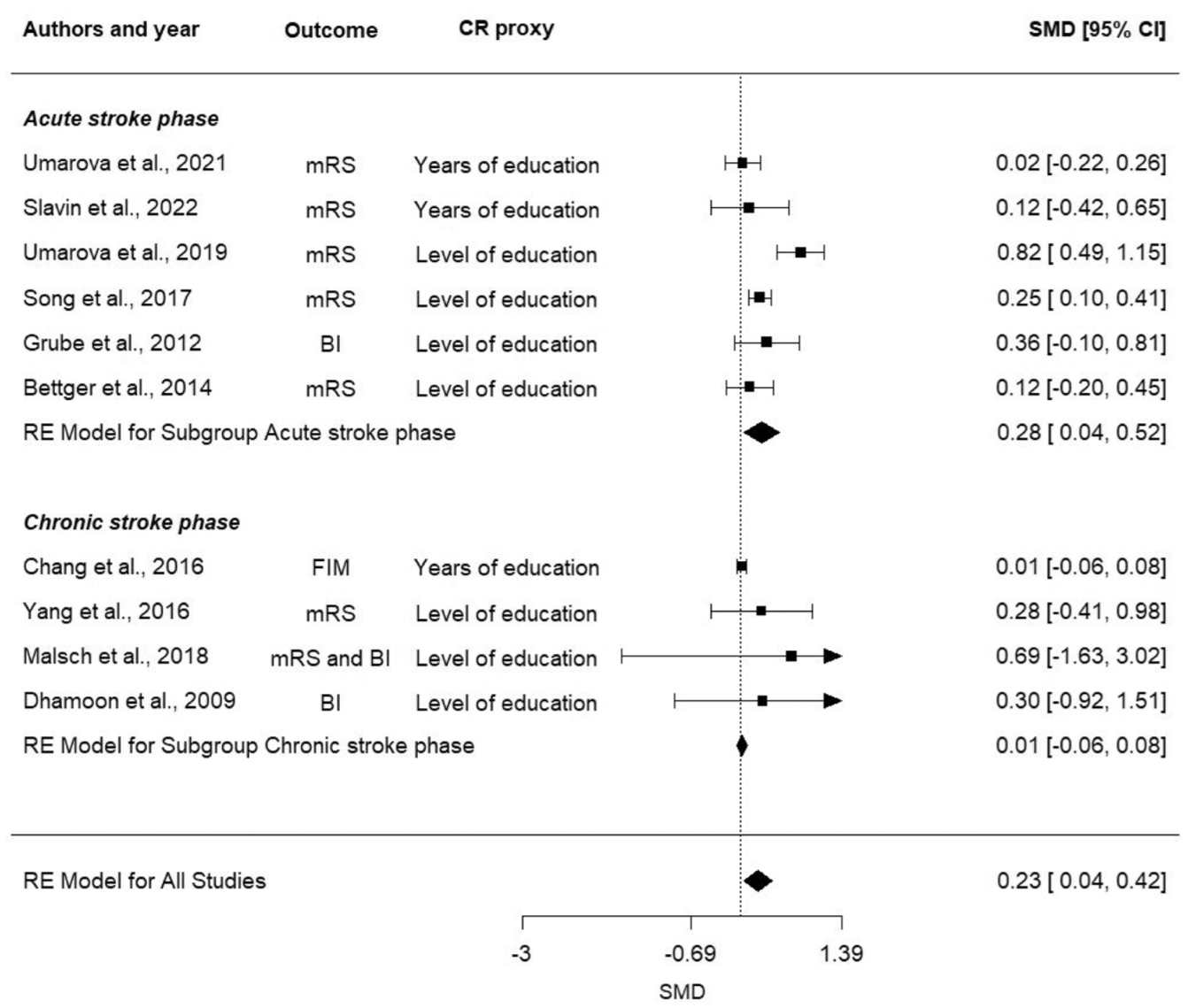
Forest plots of pooled SMD [95% CI] of studies reporting the impact of CR-proxies on stroke outcome stratified for time of assessment. Abbreviations: BI, Barthel Index; CI, confidence interval; CR, cognitive reserve; FIM, Functional Independence Measure; mRS, modified Rankin Scale; NIHSS, the National Institute of Health Stroke Scale; RE, random effect; SMD, standardized mean differences.
Discussion
This systematic review and meta-analysis demonstrate evidence for the association of CR with stroke outcome. Specifically, the strongest evidence was observed for the association of CR operationalized through level of education and occupational attainment and in the first 3 months post-stroke. Precise stroke outcome prediction has always been among the principal aims in stroke research and in patient care to enable individually tailored therapeutic approaches.1,55 However, previous studies have highlighted the limitations of existing prediction models in capturing high inter-individual variability in stroke patients.1,23 This suggests the presence of unconsidered factors influencing stroke outcome. In this context, the present meta-analysis sought to investigate the impact of CR-proxies on stroke outcome, aiming to address the gap in our understanding of the factors contributing to inter-individual variability in response to stroke. Comparisons of evidence across different stroke phases showed the stronger associations of CR-proxies and stroke outcome in the acute and subacute phases, namely in the first 3 months post-stroke. This might be attributable to other factors influencing long-term stroke outcome, such as different lifestyles, country-dependent health systems, comorbidities, potential new critical events, and aging processes. 56 Thus, we believe that more complex multidimensional models in which CR-proxies do not play a major role are required to explain the chronic outcome.
Several factors may underlie the positive influence of CR on stroke outcome. A key mechanism underlying the protective effect of CR is its ability to positively influence brain plasticity, that is, the capacity to maintain or adapt function by increasing neural efficiency and improving neural compensation mechanisms in the presence of pathology or injury.8,57 In more detail, CR may sustain plasticity by enhancing synaptic connectivity and making more efficient use of preserved neural networks. Individuals with higher CR-proxies, such as higher education, intellectually demanding occupations, or lifelong cognitive engagement, appear to be better able to optimize the use of existing networks (neural efficiency) or recruit alternative compensatory circuits (neural compensation) when damage occurs.8,58,59 This model also enables the impact of CR to be extended to non-cognitive domains, for example, motor function and global outcome measures. Furthermore, there are many reasons beyond the direct influence of CR as to why educational or occupational attainment may influence stroke outcome. For instance, patients with higher educational and occupational attainment may have a healthier lifestyle prior to stroke,60,61 being less frail at the time of stroke and/or demonstrating better treatment compliance after.62,63 CR may also reflect differences in the ability to actively engage with the environment 8 that includes the capacity to utilize rehabilitation services more effectively, adhere to therapy, and take advantage of available social and healthcare resources. Thus, the identified difference in stroke outcome between patients with high and low CR is not solely a factor of reserve but might also reflect other associations. 9 Finally, cognitive performance may also contribute to the scoring of global measures of stroke outcome. While the present study is unable to mechanistically separate these associations, evidence of the protective effect of CR-proxies on stroke outcomes cannot be ignored and should be considered in stroke research and healthcare.
Determining the proxy that best operationalizes CR and exhibits the strong relation with stroke outcome measures presents a challenge because of the intercorrelation of CR-proxies and their inconsistent assessment in stroke research. Only half of the studies included in the meta-analysis directly focused on the impact of CR-proxies on stroke outcomes.12,15,39,41,44 Other studies analyzed CR-proxies as a covariate or after univariate selection of predictors. This reduced the quality of the included data. In the subgroup analysis stratified for CR-proxies, we found no significant evidence for the effect of years of education but for the level of education. Although both CR-proxies measure the same construct, the way in which CR is operationalized appears to matter, with more robust effects being found for level of education than for years of education. The lack of evidence in the meta-analysis regarding years of education may be explained by the heterogeneity of education systems across different ethno-regional and demographic groups, which hinders direct comparability of this continuous measure across them. Similarly, the same number of years of education for older and younger adults in the same country corresponds to different levels of education due to the reforms in educational systems. Therefore, level of education may be a more accurate proxy for the education aspect of CR than years of education, also providing a more accurate prediction of stroke outcome.
The study has identified significant knowledge gaps in the field of CR in stroke. The low number of identified eligible studies may suggest that many stroke studies either do not collect CR-proxies, do not report them, or do not analyze them in relation to outcomes. Despite being searched for, no studies were found that investigated the associations of global non-cognitive stroke outcome with other well-established CR-proxies, such as leisure activities or global aggregate measures summarizing educational and occupational attainments and leisure activities. Previous studies on post-stroke cognition and dementia demonstrated the impact of intelligence,12,17,64 bilingualism, 65 and leisure activities66,67 on cognitive outcomes. These proxies might be promising factors that should be investigated in future studies on non-cognitive or global stroke outcome measures. Furthermore, because of the dynamic and heterogeneous nature of the CR concept, the aggregation of multiple CR-proxies could provide new insight into the topic.
Limitations
This meta-analysis has some limitations. First, despite the exclusion of studies with high risk of bias from the meta-analysis, we observed substantial variability in study methods and assessment measures. The different cut-offs for low versus high levels of education used across studies are explained by disparities across countries in socioeconomic and demographic factors, as well as education systems. This made comparison across studies difficult and lowered the grade of certainty in the evidence. The included studies were not randomized; however, the present research question might be barely addressed via randomized trials. Second, as expected, we observed high heterogeneity among included studies due to the variability in time of outcome assessment, definition and assessment of CR-proxies and outcome measures, as well as limited availability of consistently adjusted effect estimates across the included studies. We addressed the heterogeneity by including well-known and defined CR-proxies7,11 and validated and standardized measures of stroke outcome. We further addressed the heterogeneity by conducting a random and not fixed effect meta-analysis and by performing subgroup analyses stratified by CR-proxies and time of outcome measurement. However, the heterogeneity across studies and the unavailability of adjusted effect estimates prevented the adjustments for risk factors and the conduction of prognostic synthesis that would allow greater exploration of the adjusted association of CR-proxies with outcome. The uniform approach in the design of studies on stroke outcome—standardized acquisition of CR-proxies and outcome measures—would overcome the heterogeneity problem in future studies. Future research should also explore CR-proxies in the context of other predictors to assess the unique variability explained. Third, the asymmetrical funnel plot indicated evidence of publication bias, though the Egger test did not provide evidence for it. Previous research has demonstrated that heterogeneity in the comparators or interventions (namely CR-proxies) might result in funnel plot asymmetry, 68 as in the present study. Since CR-proxies, despite their intercorrelation, represent different aspects of CR, and have different definitions and assessments, we assume that our comparators are highly heterogeneous, and this might lead to an asymmetrical funnel plot. However, we cannot exclude a publication bias, also due to the novelty of the topic in stroke with only half of the studies directly investigating the role of CR. We tried to handle the possible publication bias by excluding studies with high risk of bias and conducting subgroup analyses stratified for CR-proxies. Fourth, in some countries, the socioeconomic status, which is associated with CR-proxies, might influence stroke risks, management, and patient care. 29 We tried to minimize this bias by excluding socioeconomic status (e.g. household or individual-level data measures of income, wealth, poverty, and material ownership) as a CR-proxy and excluding studies with this reported bias. However, we cannot exclude that the association between CR and socioeconomic status moderated the present results. Fifth, we excluded from the analysis of occupational attainment the “retired” level since it is strongly age-dependent and does not reflect the lifelong 6 occupational attainment—as posited by the CR theory—but rather represents the demographic variable. However, in this way, we consequently excluded the most representative group in some studies, since usually the elderly account for the majority of stroke patients. Sixth, the identified non-cognitive outcome measures were very basic being mainly represented by disability levels (modified Rankin Score) and BI (dominated scoring on continence/mobility). More granular measures of non-cognitive stroke outcome including those of activities of daily living are available and need to be integrated into research on the impact of CR on stroke outcome. And finally, only educational and occupational attainment as CR-proxies have been included in the meta-analysis due to the unavailability of data on other proxies or on global aggregate CR-measures. Altogether, future research is warranted to explore different CR-proxies and their interactions with other modifiable and non-modifiable cardiovascular risk factors and to refine our understanding of inter-individual variability in stroke outcome.
Building on the present findings, our synthesis also underscores several broader implications. Clinically, selected CR-proxies may provide complementary prognostic information alongside established clinical and imaging markers, thereby supporting more individualized predictions of post-stroke outcome. From a research standpoint, there is a clear need for harmonized, multidimensional assessments of CR; preferably through validated multi-indicator questionnaires or through the simultaneous inclusion of multiple proxies to better capture the construct. Moreover, CR should be systematically considered and assessed in studies investigating post-stroke outcomes, not limited to cognitive endpoints, but also for non-cognitive outcome. Further systematic investigation into the impact of CR-proxies on stroke outcome is required. The integration of CR-proxies into predictive models is a critical next step to improving prognostic accuracy and advancing the development of personalized therapeutic strategies.
To conclude, this systematic review and meta-analysis demonstrated the evidence for the association of low CR with poor stroke outcome. A greater association was observed for CR operationalized as level of education and occupational attainment, and for the acute stroke phase than for the chronic one. However, studies’ quality and completeness in the assessment of CR-proxies limit the degree of certainty to “moderate” in the level of evidence. This critical issue should be addressed in future studies. Further systematic investigation is required into the impact of CR-proxies on stroke outcome. The utilization of CR-proxies within predictive models, and a comprehensive evaluation of CR-proxies, extending beyond educational and occupational attainment, are imperative to enhance the prognostic accuracy of stroke outcome and facilitate the development of personalized therapeutic strategies.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261417825 – Supplemental material for Association of cognitive reserve with stroke outcome: A systematic review and meta-analysis
Supplemental material, sj-docx-1-wso-10.1177_17474930261417825 for Association of cognitive reserve with stroke outcome: A systematic review and meta-analysis by Laura Gallucci, Mirjam R Heldner, Christoph Sperber and Roza M Umarova in International Journal of Stroke
Supplemental Material
sj-docx-2-wso-10.1177_17474930261417825 – Supplemental material for Association of cognitive reserve with stroke outcome: A systematic review and meta-analysis
Supplemental material, sj-docx-2-wso-10.1177_17474930261417825 for Association of cognitive reserve with stroke outcome: A systematic review and meta-analysis by Laura Gallucci, Mirjam R Heldner, Christoph Sperber and Roza M Umarova in International Journal of Stroke
Supplemental Material
sj-docx-3-wso-10.1177_17474930261417825 – Supplemental material for Association of cognitive reserve with stroke outcome: A systematic review and meta-analysis
Supplemental material, sj-docx-3-wso-10.1177_17474930261417825 for Association of cognitive reserve with stroke outcome: A systematic review and meta-analysis by Laura Gallucci, Mirjam R Heldner, Christoph Sperber and Roza M Umarova in International Journal of Stroke
Footnotes
Acknowledgements
We thank Professor Erik von Elm—director of Cochrane Switzerland—and PhD Lukas Bütikofer for their methodological support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is funded by the Synapsis Foundation, the Heidi Seiler Foundation, and the Swiss National Science Foundation (SNSF, project number 10003589). Funders have no role in the study design, execution, data analysis, interpretation, and in writing the manuscript.
Supplemental material
Supplemental material for this article is available online.