
Abstract
Background:
Despite major advances in the prevention and treatment of stroke, many stroke trials have yielded neutral or modestly positive results due to multiple factors, including patient heterogeneity, small treatment effects, inadequate statistical efficiency, and in some settings limited biological efficacy or insufficient early-phase validation of interventions.
Summary of review:
This review summarizes emerging methodological innovations relevant to contemporary stroke trials, including group sequential methods, adaptive design (response-adaptive randomization, sample size re-estimation, enrichment strategies), Bayesian designs, and master protocol frameworks (basket, umbrella, and platform trials). We also discuss advances in outcome assessment, including hierarchical composite endpoints analyzed using the win ratio, ordinal and utility-weighted analyses of the modified Rankin Scale, and the growing role of patient-reported outcomes in capturing patient-centered benefits across the recovery continuum. Finally, we highlight stroke-specific methodological challenges and outline future opportunities enabled by advances in imaging, digital health, and data-driven approaches.
Conclusion:
Together, these innovations have the potential to improve the efficiency, interpretability, and clinical relevance of stroke trials, provided they are implemented within rigorously pre-specified protocols that preserve trial integrity and valid statistical inference.
Why we need novel designs in stroke trials
Despite advances in the prevention and treatment of stroke during the past decade, the majority of randomized controlled trials (RCTs) across various therapeutic domains in stroke have yielded neutral or modestly positive results.1–8 These neutral findings likely reflect multiple factors, including true absence of treatment effect for some interventions, inadequate early translational evidence, patient heterogeneity, and limited statistical efficiency (Figure 1). A fundamental challenge in stroke trials is their pronounced heterogeneity due to diverse etiologies, lesion locations, patient baseline functional status, and time-to-treatment profiles. 9 Such biological and clinical variability can substantially dilute the average treatment effects of interventions that would be highly effective in specific patient subpopulations.10,11 Traditional trial designs, which typically assume homogeneous treatment effects and rely on dichotomized functional endpoints, are suboptimal to capture the complexity of patient heterogeneity. 12
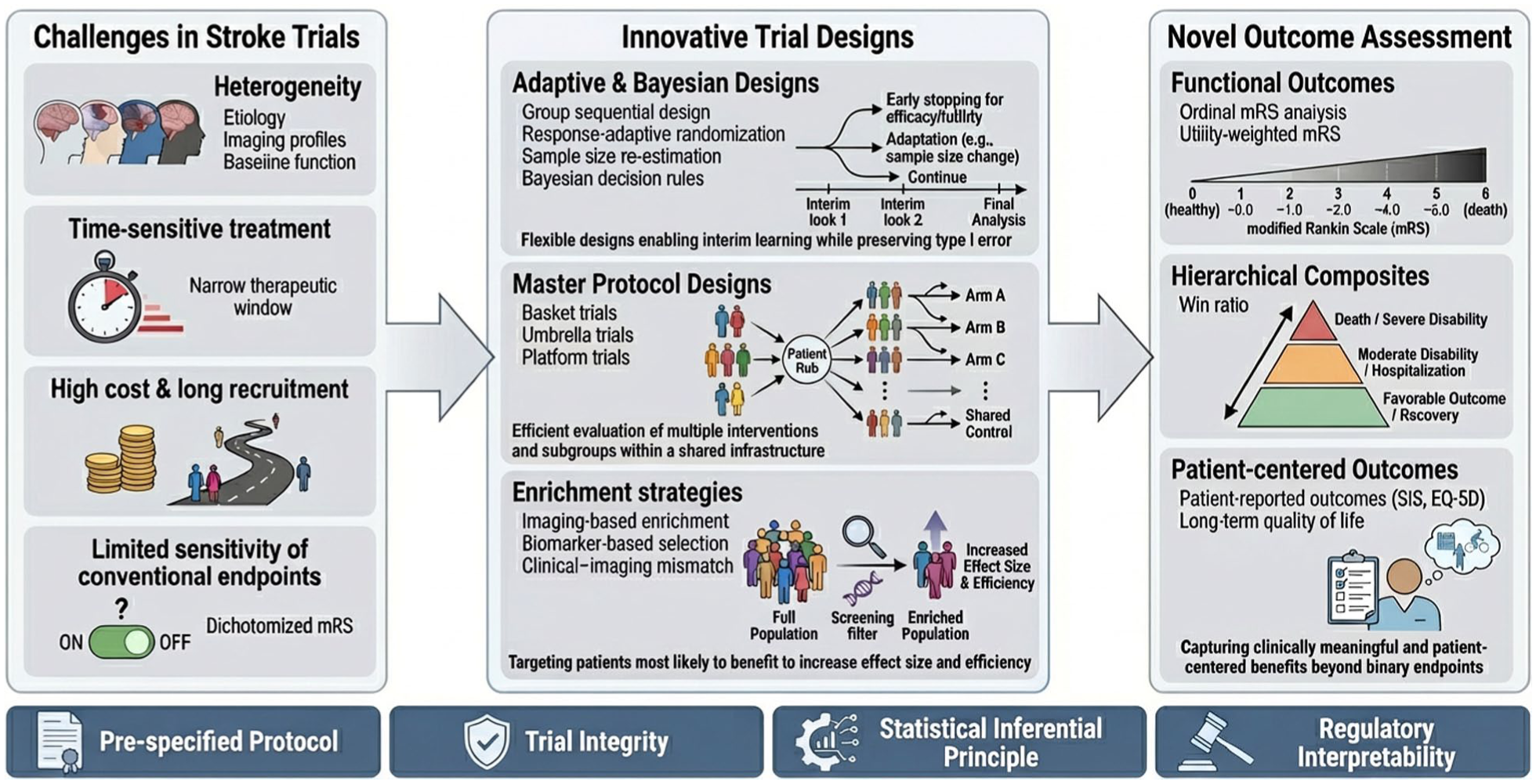
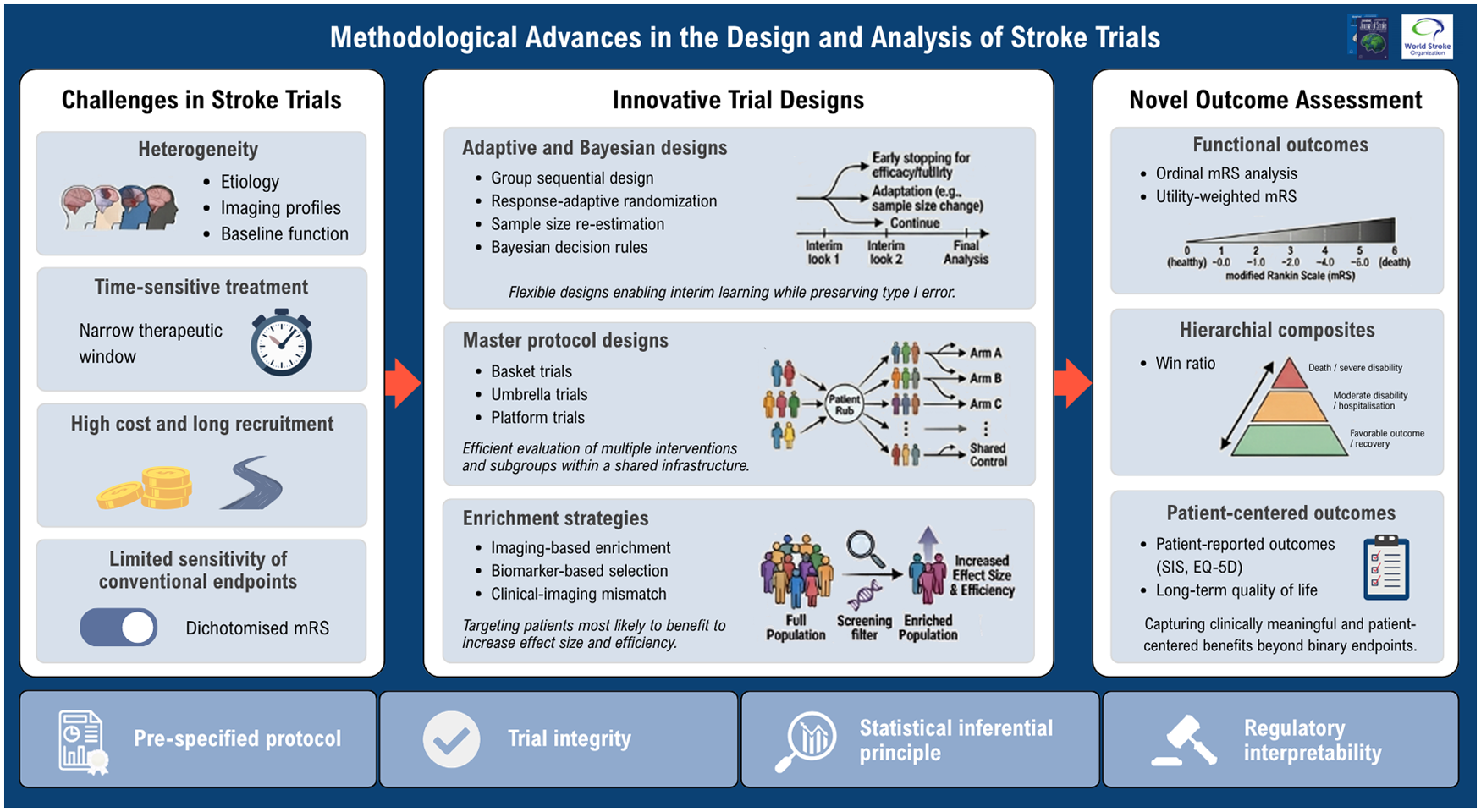
Graphical overview of novel trial designs and outcome assessment in stroke trials. Stroke trials often incur unique challenges related to disease heterogeneity, time-sensitive interventions, high cost, and limited sensitivity of conventional endpoints. Innovative trial designs, including adaptive and Bayesian approaches, master protocols, and enrichment strategies, aim to improve efficiency and precision in evaluating treatment effects. Complementary advances in outcome assessment, such as ordinal and utility-weighted functional analyses, hierarchical composite endpoints, and patient-reported outcomes, enhance the ability to capture clinically meaningful and patient-centered benefits. However, all innovations must be implemented within rigorously prespecified protocols to preserve trial integrity and valid statistical inference.
In addition, stroke trials increasingly incurred high operational costs, prolonged recruitment periods, and ethical considerations related to exposing patients to potentially ineffective treatments.13–15 The requirement for large sample sizes was partly driven by small effect sizes and inefficient endpoint utilization, which further called for financial and logistical challenges. 16 These problems were further exacerbated in the era of precision medicine, where promising interventions may only target specific patient populations defined by imaging, biomarkers, or clinical phenotypes.
Moreover, analytical strategies in stroke trials often adopt the dichotomization of the modified Rankin Scale (mRS), which has been shown to result in substantial loss of statistical information and power.17–19 Although ordinal and shift-based analyses have gained some popularity, their adoption remains inconsistent.20,21 Innovative analytical approaches regarding stroke endpoints are needed to better reflect patient-centered outcomes and treatment-relevant changes of the specific outcomes. Collectively, these challenges underscore the need for novel trial designs and analytic methods in stroke research. Adaptive designs, enrichment strategies, platform trials, and more efficient outcome analyses offer the potential to improve statistical efficiency, reduce trial costs, and enhance the likelihood of identifying clinically meaningful treatment effects, while maintaining methodological rigor and interpretability for clinicians and regulatory agencies. Although these innovative methodologies have been increasingly adopted in oncology and cardiovascular research over the past decade, their implementation in stroke trials remains comparatively limited.
Rather than providing a formal systematic review, this article aims to offer a clinically oriented narrative overview of emerging trial designs and innovative outcome assessment strategies relevant to contemporary stroke research. We focus on representative methodological approaches and landmark stroke trials that illustrate how these innovations may improve trial efficiency, precision, and clinical interpretability.
Novel trial designs applicable to stroke research
Group sequential design
Group sequential designs allow RCTs to have one or more planned interim analyses, when the trial could be stopped early for efficacy, futility, or safety concerns (Table 1).22–24 Unlike conventional designs with fixed sample sizes, group sequential trials offer a greater amount of flexibility by utilizing accumulated trial data while preserving the overall type I error rate. This control is typically achieved through prespecified stopping boundaries or alpha-spending approaches that adjust for repeated interim analyses. Group sequential design also aligns well with ethical imperatives in stroke research, as it is able to reduce unnecessary exposure to ineffective and harmful interventions or shorten trial duration when strong treatment effects emerge early. However, interim monitoring in group sequential design requires close collaboration between principal investigators and trial statisticians regarding the pre-specification of the interim analyses and independent data monitoring. In addition, early stopping, particularly early stopping for efficacy, may overestimate treatment effects and, therefore, require cautious interpretation.
Key methodological features of novel trial designs in stroke research.
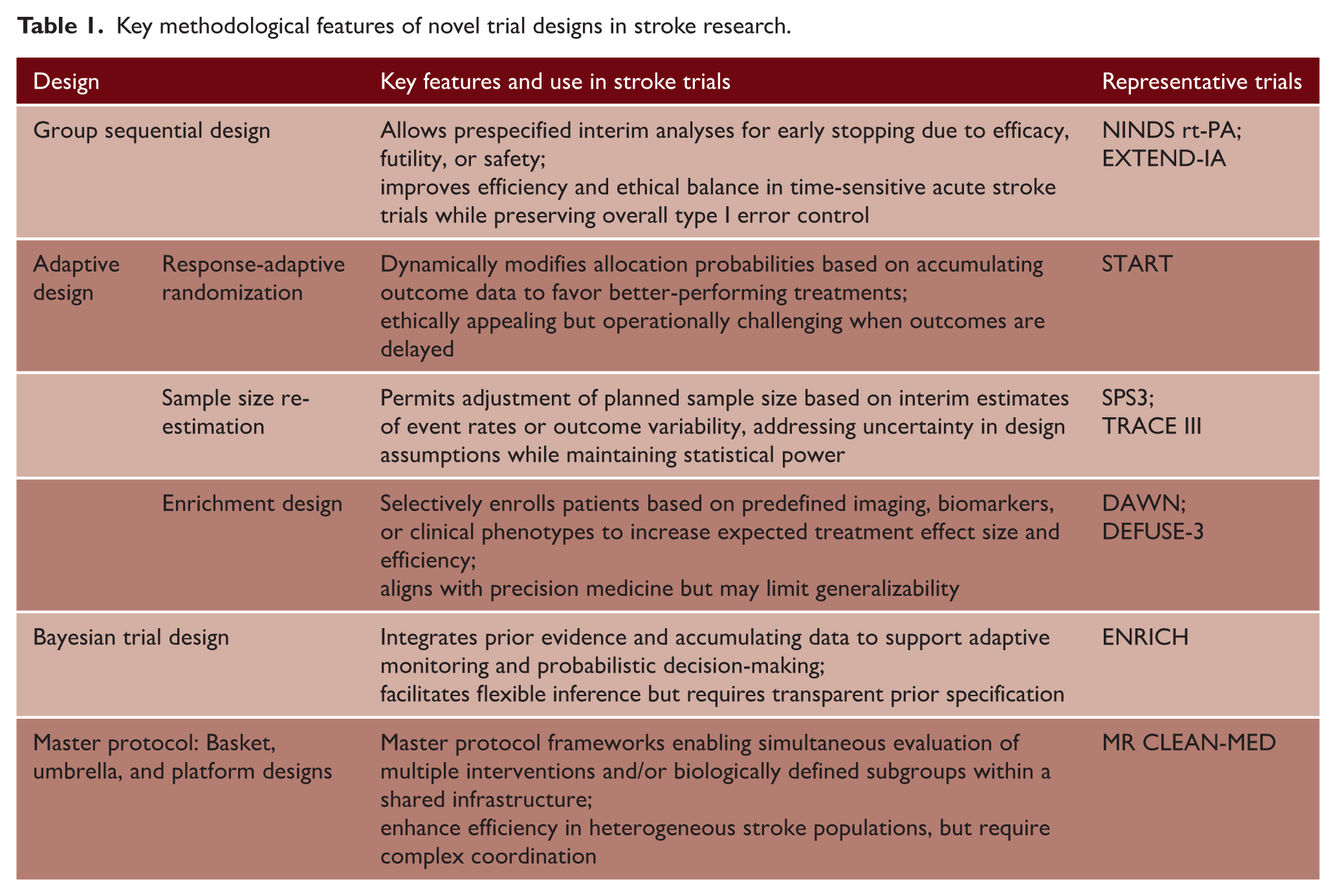
Group sequential designs have been incorporated into several stroke trials, including the NINDS rt-PA trial, in which prespecified interim monitoring was conducted for efficacy and safety, 25 and the EXTEND-IA trial, which was stopped early after interim analyses demonstrated substantial treatment benefit. 26 These examples illustrate the potential role of interim monitoring in supporting ethical trial conduct and facilitating early decision-making. However, despite their methodological appeal, there remain relatively few clear examples in acute stroke where group sequential monitoring substantially altered overall trial trajectory or duration. This may partly reflect the operational complexity of acute stroke trials, rapid recruitment in some large multicenter studies, and delayed ascertainment of functional outcomes, such as 90-day mRS. Group sequential approaches may, therefore, be particularly valuable in early-phase stroke studies for futility assessment and proof-of-concept decision-making before phase III evaluation.
Adaptive designs
Adaptive trial methodologies in stroke research may involve modifications to randomization procedures, sample size, and interim decision-making based on accumulating data, whereas other precision-oriented strategies rely on prospectively defined biomarker or imaging-based patient selection.
Response-adaptive randomization
Response-adaptive randomization (RAR) allocates participants to treatment arms based on probabilities calculated using outcomes that have been observed.27,28 An intuitive illustration is that participants have higher probabilities of being randomized to treatment arms with accumulating evidence of better efficacy. RAR design is appealing because it aligns trial conduct with patient benefit, potentially improving acceptability and ethical balance. However, RAR could introduce operational and statistical complexity. It is challenging to apply RAR to outcomes that may take a long time to evaluate, which is an important consideration in stroke, where functional endpoints may take months to ascertain. Nevertheless, evidence demonstrating clear superiority of RAR over conventional allocation strategies in acute stroke trials remains limited.
RAR has been explored in stroke-related studies, although not as widely used as in oncology trials. For example, in the START trial, which aims to determine the optimal delay time to initiate anticoagulation after atrial fibrillation-related stroke, RAR via interim analyses were conducted to favor allocation of participants to arms with better risk–benefit profile. 29 These experiences highlight both the promise and practical challenges of applying RAR in stroke trials, particularly when the primary outcomes are not immediately observable.
Sample size re-estimation
Sample size re-estimation (SSR) allows the trial to modify the prespecified sample size based on results from interim analyses, such as event rates or outcome variability, without unblinding treatment assignment.30,31 Although SSR is not a new statistical methodology, it remains an important adaptive design tool in contemporary stroke trials where initial assumptions regarding event rates, outcome variability, and treatment effect sizes are often uncertain. The outcome distributions and event rates in stroke trials can vary substantially across populations or disease subtypes, where SSR could offer a pragmatic tool to maintain adequate statistical power while saving patient resources. Limitations of SSR include increased logistical complexity and the need for careful regulatory and statistical oversight.
The Secondary Prevention of Small Subcortical Strokes (SPS3) study increased its planned patient enrollment from approximately 2500 to 3000 after interim analysis, when results showed that the event rate was lower than expected. 32 By using the promising zone approach at the prespecified interim analysis when 258 patients were evaluated, TRACE III tenecteplase reperfusion therapy trial allowed the expansion of the sample size to up to 808 to maintain enough statistical power. 33 These approaches show how SSR can be used in large, multicenter stroke trials to address uncertainty in key design assumptions while preserving trial integrity.
Enrichment design
Enrichment designs aim to increase the likelihood of detecting treatment benefit by selectively enrolling patients who are more likely to respond to an intervention based on predefined clinical characteristics, imaging features, biomarkers, or risk profiles.34,35 This strategy directly addresses patient heterogeneity by increasing the expected treatment effect size and improving statistical efficiency. Some enrichment strategies may also incorporate adaptive modifications during interim analyses, although many stroke enrichment trials have relied on prospectively specified selection criteria. However, enrichment approaches require strong biological rationale and prospectively defined selection criteria, as post hoc subgroup identification may increase the risk of false-positive findings and poor reproducibility. In addition, excessively narrow target populations may reduce recruitment feasibility and limit the commercial viability of therapeutic development.
Both the DAWN and DEFUSE-3 trials exemplified prospectively defined imaging-based enrichment strategies by selecting patients according to clinical–imaging mismatch and perfusion imaging criteria to identify those most likely to benefit from endovascular thrombectomy beyond the conventional 6-h time window. In DAWN, eligibility was enriched using a clinical–imaging mismatch defined by a combination of NIHSS score and infarct core volume on perfusion or diffusion imaging to enroll patients within 6–24 h of symptom onset. 36 In DEFUSE-3, enrichment was based on a target perfusion–core mismatch profile determined by automated perfusion imaging (e.g. infarct core <70 mL with a mismatch ratio ⩾1.8 and sufficient penumbra) to recruit patients within a 6- to 16-h window. 37 Notably, the success of these trials was supported by prospectively defined imaging criteria and strong pathophysiological rationale, distinguishing them from exploratory post hoc subgroup analyses that have historically shown limited reproducibility in stroke research.
Bayesian approach
Bayesian trial designs formally incorporate prior information, such as evidence from historical trials or expert opinions, into the design, analysis, and updating of treatment effects as data accumulate.38,39 Results are often presented as probabilities of benefit or harm, which are more intuitive for clinicians to understand compared with p values. Bayesian approaches naturally accommodate adaptive features, including early stopping and flexible decision rules. Although Bayesian methods are frequently incorporated into adaptive randomization procedures, Bayesian trial design principles extend beyond RAR to include posterior probability monitoring, borrowing of external information, adaptive stopping rules, and hierarchical modeling. Furthermore, Bayesian designs often require transparent justification of prior assumptions and may face regulatory or interpretational challenges when audiences are unfamiliar with Bayesian statistics.
Bayesian methods were prominently used in the
Master protocol (basket, umbrella, and platform trial designs)
Basket trials evaluate a single intervention across multiple patient subgroups defined by shared biological or imaging characteristics, instead of by clinical diagnoses.41,42 In stroke trials, this approach is particularly relevant when an intervention targets a common biological mechanism, such as collateral failure or inflammation, across heterogeneous stroke subtypes. Umbrella trials, on the contrary, evaluate multiple interventions within a single clinically defined stroke population, where treatment assignment is guided by distinct biological, imaging, or pathophysiological features. 43 At present, true basket or umbrella trial implementations remain uncommon in stroke research, and these frameworks may currently serve more as conceptual models for future precision stroke trials than widely established operational designs. Platform trials extend basket and umbrella concepts by providing a perpetual and adaptive trial framework in which multiple interventions and patient subgroups can be evaluated concurrently, with flexible addition or removal of treatment arms based on accumulating evidence.44,45 These flexible trial designs offer powerful tools to address biological heterogeneity in stroke by enabling mechanism-based patient selection and more efficient evaluation of interventions.
However, the application of these designs in stroke research remains limited, largely due to the absence of well-established biological stratification frameworks, rapidly evolving pathophysiology in acute stroke and substantial operational complexity associated with real-time patient characterization and treatment assignment. The MR CLEAN-MED trial illustrates how certain platform-like design features, including evaluation of multiple interventions within a shared infrastructure and common control framework, may be adapted to acute ischemic stroke research. 46
Novel outcome assessment
Win ratio for hierarchical composite endpoints
The win ratio is an analytical approach for composite endpoints that prioritizes clinically most important and relevant outcomes (Table 2).47,48 Instead of collapsing multiple outcomes in the hierarchical endpoint into a single binary composite, patients are first compared on the most severe outcome (e.g. death); and if tied, they are then compared on subsequent outcomes (e.g. recurrent stroke, disability, or safety events). This analytical framework is particularly attractive in stroke trials where outcomes vary widely in severity, and conventional analytical approaches may obscure clinically meaningful benefits of composite endpoints by weighting all components equally. The win ratio preserves clinical priorities and, at the same time, enhances efficiency when treatment effects differ across outcome components. However, the win ratio framework relies on prespecified hierarchical ranking of outcomes, and selection and ordering of endpoint components may introduce subjectivity and influence interpretation of treatment effects. Careful clinical justification and transparent pre-specification of outcome hierarchy are, therefore, essential. Furthermore, incorporation of clinician and patient perspectives into endpoint prioritization may improve the clinical relevance and acceptability of hierarchical composite analyses.
Key methodological features of novel outcome assessment approaches in stroke trials.
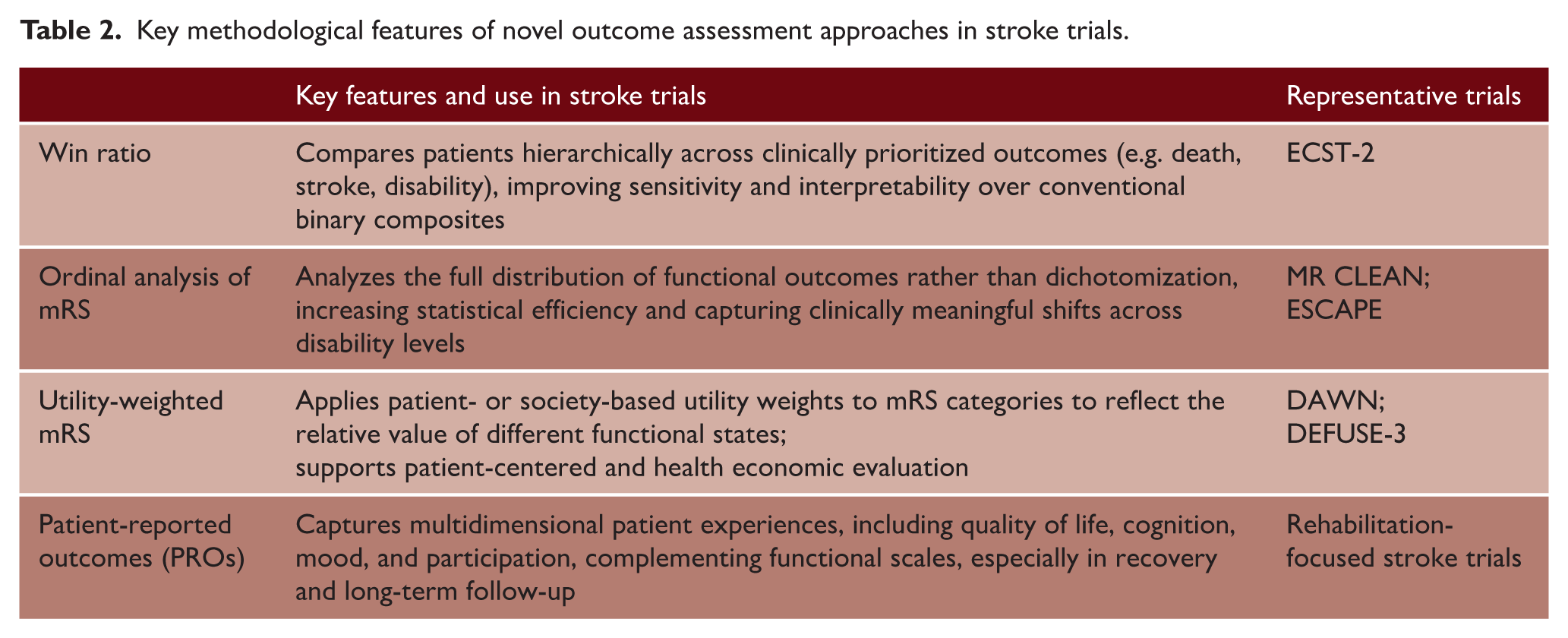
Although the win ratio has not yet been widely implemented in stroke trials, it has gained increasing methodological interest as a potentially attractive framework for hierarchical outcome assessment in cerebrovascular research. A recent methodological paper in Stroke illustrated the application of the win ratio using data from the ICSS and MR CLEAN trials and proposed its prospective use in the ECST-2 trial, where hierarchical outcomes, including fatal stroke, myocardial infarction, and nonfatal stroke, are prioritized according to clinical importance. 49 The win ratio may be particularly relevant in stroke prevention or neurovascular intervention trials involving clinically heterogeneous composite outcomes, whereas its role relative to conventional ordinal mRS analyses in acute stroke remains to be further established. Nevertheless, further empirical experience is needed to determine whether win ratio approaches provide substantial advantages over established ordinal or shift-based analyses in acute stroke trials.
Ordinal analysis and utility-weighted mRS
The modified Rankin Scale (mRS) is the most widely used functional outcome in acute stroke trials. Although highly relevant for global disability assessment after acute stroke, mRS may be less sensitive for evaluating cognition, participation, quality of life, or domain-specific recovery outcomes in rehabilitation and prevention-focused studies. Conventional statistical analyses often adopt the dichotomization of mRS (e.g. mRS 0–2 vs. ⩾3), which leads to substantial information loss. An alternative analytical method is to treat mRS as an ordinal outcome, which will improve statistical power by utilizing enough information about the full distribution of mRS. Utility-weighted mRS further extends this concept by assigning weights to each mRS level, which allows the investigator to incorporate different weights to different mRS levels based on patient- or societal-valued health states. These approaches align closely with the clinical perspective that shifts across mRS levels contain more clinical meaningfulness than across a dichotomous mRS threshold.
Ordinal analysis of the full mRS distribution has become standard in contemporary acute stroke trials, including landmark endovascular thrombectomy studies such as MR CLEAN and ESCAPE, where proportional odds models were utilized to evaluate potential treatment effects across the entire mRS spectrum.50,51 However, interpretation of the common odds ratio or shift estimate may be less intuitive for clinicians to understand, particularly because the estimated effect does not directly correspond to a specific change in functional category at the individual patient level. To improve clinical interpretability, ordinal analyses are increasingly accompanied by graphical distributional displays, absolute category-specific risk differences, utility-weighted summaries, or responder-based interpretations. Utility-weighted mRS has been used in the primary and secondary analyses of reperfusion trials, including DAWN and DEFUSE 3, to quantify potential treatment effects in terms of patient-valued functional outcomes.36,37 These analyses showed that ordinal analysis and utility-weighted approaches can reveal clinically relevant treatment benefits that may be underestimated using conventional binary dichotomization. In practice, maximizing statistical efficiency must be balanced against the need for clinically interpretable treatment estimates that can meaningfully inform bedside decision-making and guideline development.
Patient-reported outcomes
Patient-reported outcomes (PROs) capture multi-dimensions of health, such as quality of life, cognition, mood, fatigue, and social participation, that cannot be fully reflected by conventional functional endpoints such as mRS.52,53 In stroke trials, particularly rehabilitation-focused studies, PROs complement conventional disability scales by capturing dimensions of recovery that are insufficiently reflected by the mRS, including cognition, fatigue, participation, emotional well-being, and health-related quality of life. As patient survival and functional independence continue to improve, PROs are increasingly recognized as particularly important tools to evaluate patient-centered benefit, particularly in trials targeting rehabilitation, secondary prevention, and post-acute recovery. 54
Validated PRO instruments, such as the Stroke Impact Scale (SIS) and EQ-5D, have been incorporated in several stroke trials as secondary or exploratory outcomes. For instance, rehabilitation and recovery-focused stroke trials have increasingly adopted SIS domains and other multidimensional outcome measures to detect clinically meaningful improvements in participation, mobility, upper limb function, and quality of life that may not be adequately captured by conventional mRS-based analyses.55,56 In acute interventional studies, PROs have been applied at long-term follow-ups to evaluate patient-perceived treatment-related benefits beyond early functional outcomes, reinforcing their role in comprehensive outcome assessment.57,58 However, the extent and complexity of PRO assessment in acute stroke trials should be balanced against trial feasibility, participant burden, and the incremental clinical information gained beyond established functional outcome measures. In many acute intervention trials, focused or targeted PRO assessments may be more practical and informative than comprehensive multidomain quality-of-life batteries. In rehabilitation-focused stroke trials, more targeted patient-reported outcome measures (PROMs) may be particularly important when interventions aim to improve specific dimensions of recovery, such as communication, cognition, fatigue, emotional well-being, or social participation, which may not be adequately captured by global disability scales such as the mRS. In such settings, domain-specific PROMs may serve not only as complementary outcomes but also as clinically meaningful primary endpoints.
Methodological challenges and opportunities
Despite substantial methodological advances in the design and analysis of clinical trials, the implementation of innovative and adaptive trial methodologies in stroke research remains relatively limited compared with other therapeutic areas such as oncology and cardiovascular medicine. Acute stroke trials are often faced with narrow therapeutic time windows, high clinical urgency, and logistical complexity, all limiting opportunities for extensive baseline assessment, real-time biomarker evaluations, and complex adaptive randomization. The marked heterogeneity of stroke in terms of disease etiology, vascular territory, collateral status, and comorbidities further makes it complicated for patient selection and treatment effects evaluation, making conventional fixed designs inefficient, time-consuming, and financially costly. In addition, many biologically relevant stroke phenotypes, such as penumbral viability, inflammatory response, and neuroplasticity, lack standardized, rapidly assessable biomarkers suitable for trial enrichment. Furthermore, under-recruitment, increasing regulatory complexity, and growing pressure on healthcare systems further challenge the feasibility and scalability of stroke trials in real-world settings. Regulatory conservatism and variability in clinical practice across the globe also pose barriers to the adoption of adaptive designs, Bayesian decision rules, and novel endpoints analytical methods, particularly for global multicenter stroke trials where simplicity and interpretability remain critical. Methodological challenges may also differ substantially between acute intervention and rehabilitation-focused stroke trials, particularly regarding endpoint selection, longitudinal follow-up, and sensitivity to functional recovery.
To date, only a limited number of stroke trials have incorporated Bayesian adaptive frameworks, platform structures, or RAR, highlighting substantial opportunities for future methodological expansion. The increasing availability of advanced imaging, digital health records, and longitudinal outcome assessments enables more precise patient phenotyping and supports the use of enrichment strategies, adaptive randomization, and platform trial infrastructures. Novel outcome analytical methods, such as ordinal and utility-weighted functional scales, hierarchical composite endpoints, and PROs, offer greater sensitivity to clinically meaningful benefits across the recovery continuum. Bayesian frameworks provide a coherent approach for integrating prior evidence, borrowing information across disease subgroups, and enabling flexible interim decision-making, which is particularly valuable in heterogeneous stroke populations. Moreover, platform and master protocol designs allow multiple interventions to be evaluated efficiently within a shared infrastructure, accelerating evidence generation while reducing patient and resource burden. It is noteworthy that although innovative trial methodology can improve efficiency and precision, it cannot compensate for interventions lacking sufficient biological rationale or therapeutic efficacy.
Among the innovative methodologies discussed, some approaches may be more immediately applicable to future stroke trials than others. In particular, adaptive enrichment strategies, platform trial infrastructures, ordinal outcome analyses, and Bayesian interim monitoring appear especially well aligned with the biological heterogeneity and operational realities of stroke research. In contrast, RAR may face more substantial practical limitations in acute stroke settings due to delayed functional outcome ascertainment and the need for rapid treatment allocation. Future methodological development in stroke should, therefore, prioritize designs that balance statistical efficiency, operational feasibility, interpretability, and regulatory acceptability.
Looking ahead, future stroke trials are likely to evolve beyond traditional site-based models toward more integrated, data-driven, and patient-centered research ecosystems. Decentralized trial designs are emerging as a promising approach to address challenges in recruitment, retention, and trial delivery, particularly in the primary and secondary prevention of stroke. By leveraging remote consent, digital follow-up, and integration with electronic health records, decentralized trials may improve accessibility and reduce the burden on overstretched healthcare systems. For example, pragmatic studies such as ADAPTABLE have demonstrated the feasibility of large-scale, low-cost, remotely conducted trials. 59 However, issues related to data quality, endpoint validation, and digital inequalities remain important considerations. Emerging approaches using synthetic or externally derived control groups based on real-world data and stroke registries may further improve trial efficiency and reduce recruitment burden, particularly in early-phase or rare stroke subtype studies. However, these approaches require careful adjustment for selection bias, confounding, temporal drift, and data quality to ensure validity and regulatory acceptability.
In addition, machine learning algorithms applied to imaging, electronic health records, and data obtained from wearable devices enable real-time risk prediction, automated phenotyping, and dynamic treatment assignment regimes, facilitating truly personalized and adaptive trial designs. AI-assisted outcome assessment, including automated mRS scoring and continuous functional monitoring, has the potential to reduce measurement variability and capture recovery trajectories with greater granularity. When combined with Bayesian adaptive frameworks and platform trial structures, these technologies could transform stroke trials from static, population-averaged trials into learning systems that continuously update evidence and optimize treatment strategies. However, the implementation of AI-driven methodologies in stroke trials also raises important challenges regarding transparency, reproducibility, regulatory oversight, and external generalizability across diverse healthcare systems, imaging platforms, and patient populations. AI models developed in highly selected data sets may not maintain performance across broader clinical settings, highlighting the importance of robust external validation, algorithm interpretability, and prospective evaluation before widespread adoption in stroke research. Furthermore, such flexibility must be embedded within well-calibrated inferential frameworks to safeguard trial integrity and prevent inflation of false-positive conclusions. This will require close collaboration among clinicians, statisticians, data scientists, regulators, and patients to ensure methodological rigor, transparency, and clinical relevance. Greater familiarity with these innovative methodologies among clinicians and emerging stroke trialists will be important to facilitate broader adoption and effective implementation in future stroke research.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received support from the National Natural Science Foundation of China (No.82304241).