
Abstract
Recreational cyclists often participate in events that exceed their usual activity levels, increasing the risk of musculoskeletal discomfort. Reduced flexibility is a contributing factor, yet no studies have examined mobility interventions to address this issue. This randomized controlled trial investigated the effects of a 6-week pre-event mobility intervention on musculoskeletal discomfort scores, the number of participants reporting discomfort by body region, and active flexibility in recreational cyclists participating in a two-day, 250-km ride. Fifteen participants were allocated to a control group (n = 7), maintaining their usual training, or an intervention group (n = 8), completing the mobility intervention. All participants completed questionnaires and flexibility tests before and after the intervention. The intervention group showed a significant reduction in musculoskeletal discomfort scores (12 [4.3] pre vs 4.5 [3.5] post; p = 0.029), whereas no significant change was observed in the control group (10 [13.0] vs 12 [11.0]; p = 0.446). The number of participants reporting discomfort by body region increased in the control group but remained stable in the intervention group, with no significant between-group difference (MD = 1.2; p = 0.052). Greater improvements in active flexibility were observed in the intervention group for the posterior chain (MD = −8.6; t = −2.663; p = 0.013), while flexibility of the soleus decreased in both groups but declined less in the intervention group (MD = −2.8; t = −2.146; p = 0.041). These findings suggest that adding mobility intervention before a recreational cycling event may reduce discomfort and support flexibility.
Introduction
Recreational cycling has become a lively and inclusive activity that unites all kinds of riders, from beginners discovering the joys of two wheels to experienced enthusiasts of road, gravel, or mountain biking. It encompasses a wide range of activities, including bike touring, physical training, and casual group rides with friends or family. All these activities are rooted in the simple pleasures of exploration, well-being, and spending meaningful time outdoors in good company. 1 In 2020, Vélo Québec reported that more than 4.5 million people in the province of Quebec, over half the population, were engaged in cycling, highlighting its cultural and social importance. 2
Recreational cycling also builds its community through organized cycling events. These long-distance group rides focus on personal challenge and shared experience rather than competition. 1 Despite their growing popularity, recreational cycling events remain underexplored in the scientific literature. To our knowledge, only two studies have examined cyclists in the context of a recreational cycling event.3,4 One of these studies, conducted by Dannenberg et al. (1996), noted that the physical demands of these events can greatly exceed what recreational cyclists are accustomed to, highlighting the importance of proper conditioning to reduce musculoskeletal discomfort and the risk of overuse injury. 4 The second study, by Du Toit et al. (2020), specifically investigated gradual onset injuries, defined as symptoms of a chronic (non-traumatic) cycling injury severe enough to interfere with cycling, require treatment, or necessitate medical advice from a health professional. 3 Using this definition, they reported a prevalence of gradual onset injury of only 1.1% at the time of registration to Cape Town Cycle Tour in 2016, a notably low rate. 3 This might be attributable to several factors: recreational cyclists may not recognize musculoskeletal discomfort as a symptom of chronic cycling injury, may not accumulate enough cycling volume to perceive their symptoms as severe enough to warrant changes in their cycling habits, and consequently may be less likely to seek medical advice.
Given the limited research on musculoskeletal discomfort and overuse injuries among cyclists during recreational cycling events, we rely on existing studies conducted with professional cyclists. De Bernardo et al. (2012) examined the prevalence of overuse injuries among professional cyclists participating in major European cycling competitions, reporting a rate of 62.7%. 5 The lower limb was the most affected area, accounting for 67.9% of all overuse injuries. 5 However, elite and recreational cyclists differ substantially in both age (elite cyclists are typically younger) and training volume (recreational cyclists generally train less). These differences may influence both the type and frequency of cycling overuse injuries. Therefore, findings from elite populations may not directly apply to recreational populations.
Among the factors contributing to musculoskeletal discomfort and overuse injuries in cycling, the literature frequently highlights reduced flexibility as a key determinant.6–11 Therefore, stretching and other mobility-related interventions are commonly recommended to prevent these issues. Yet, to our knowledge, no studies have investigated chronic mobility interventions among recreational cyclists. Mobility interventions, which are intended to enhance flexibility, can take various forms, including static stretching, dynamic stretching, proprioceptive neuromuscular facilitation (PNF), yoga, tai chi, whole-body vibration, foam rolling, resistance training and others. However, evidence regarding their long-term effects on flexibility is mixed, with some interventions providing minimal benefits12–14 while others are well documented as effective.12,14–20 Among them, foam rolling and proprioceptive neuromuscular facilitation (PNF) stretching are well-known for their effectiveness.14,19 Combining foam rolling with PNF stretching may therefore represent an innovative and more engaging alternative to traditional static stretching, potentially enhancing cyclists’ interest and adherence. There is no research specifically addressing the impact of a mobility intervention combining foam rolling and PNF stretching on musculoskeletal discomfort and flexibility among recreational cyclists.
Thus, this study aims to investigate the effects of a 6-week mobility intervention combining foam rolling and PNF stretching of the lower limb implemented prior to a two-day, 250 km recreational cycling event. Using a randomized controlled trial design, we will examine three primary outcomes: (1) musculoskeletal discomfort scores, (2) the number of participants reporting discomfort by body regions, and (3) active flexibility. These measures will be assessed 6 weeks before and 1 week after the event to determine the intervention's impact on recreational cyclists. This study hypothesizes that a 6-week mobility intervention will lead to significant improvements in musculoskeletal discomfort scores, a reduction in the number of participants reporting discomfort by body region, and enhanced active flexibility among recreational cyclists participating in a recreational cycling event.
Materials and methods
Study design
A randomized controlled trial was conducted to assess the effects of a mobility intervention implemented prior to a recreational cycling event on cyclists’ musculoskeletal discomfort scores, the number of participants reporting discomfort by body region, and their active flexibility. Road cyclists registered for this two-day, 250-kilometre event were randomly assigned to either the control group or the intervention group. The control group maintained their usual training, whereas the intervention group completed a six-week mobility intervention prior to the event. All participants completed a series of questionnaires and underwent a battery of tests pre- and post-intervention (after the cycling event).
Participants
A call for study participation was posted on the event's social media platforms, and the organization sent an email to registered cyclists. All interested cyclists meeting the inclusion criteria were included, specifically those participating in the recreational cycling event who were 18 years or older and had no restrictions on engaging in regular physical activity. A sample of 20 cyclists volunteered for the study; five participants did not complete the study due to various circumstances (work-related musculoskeletal issues, an inappropriate bike size and fit, a bike accident, an injury unrelated to cycling and a lack of interest). The final sample included 15 cyclists randomly assigned to either a control group (n = 7; 3 females; 42.4 ± 12.5 years old) or an intervention group (n = 8; 3 females; 46.9 ± 14.4 years old). Although no predetermined sequence or formal stratified randomization was used, participants were randomly allocated to groups, with efforts made to balance sex distribution. As the study was based on voluntary participation, no a priori power analysis was conducted. Consequently, the final sample size reflects the maximum number of participants that could be recruited within the available timeframe and resources. Before taking part in the study, all participants were informed of the aims and procedures and signed an informed consent form. The study received approval from the institutional Research Ethics Committee (2026-801). Figure 1 shows the participant flow in the study, covering recruitment, group assignment, exclusions, and the final sample sizes for both the intervention and control groups.
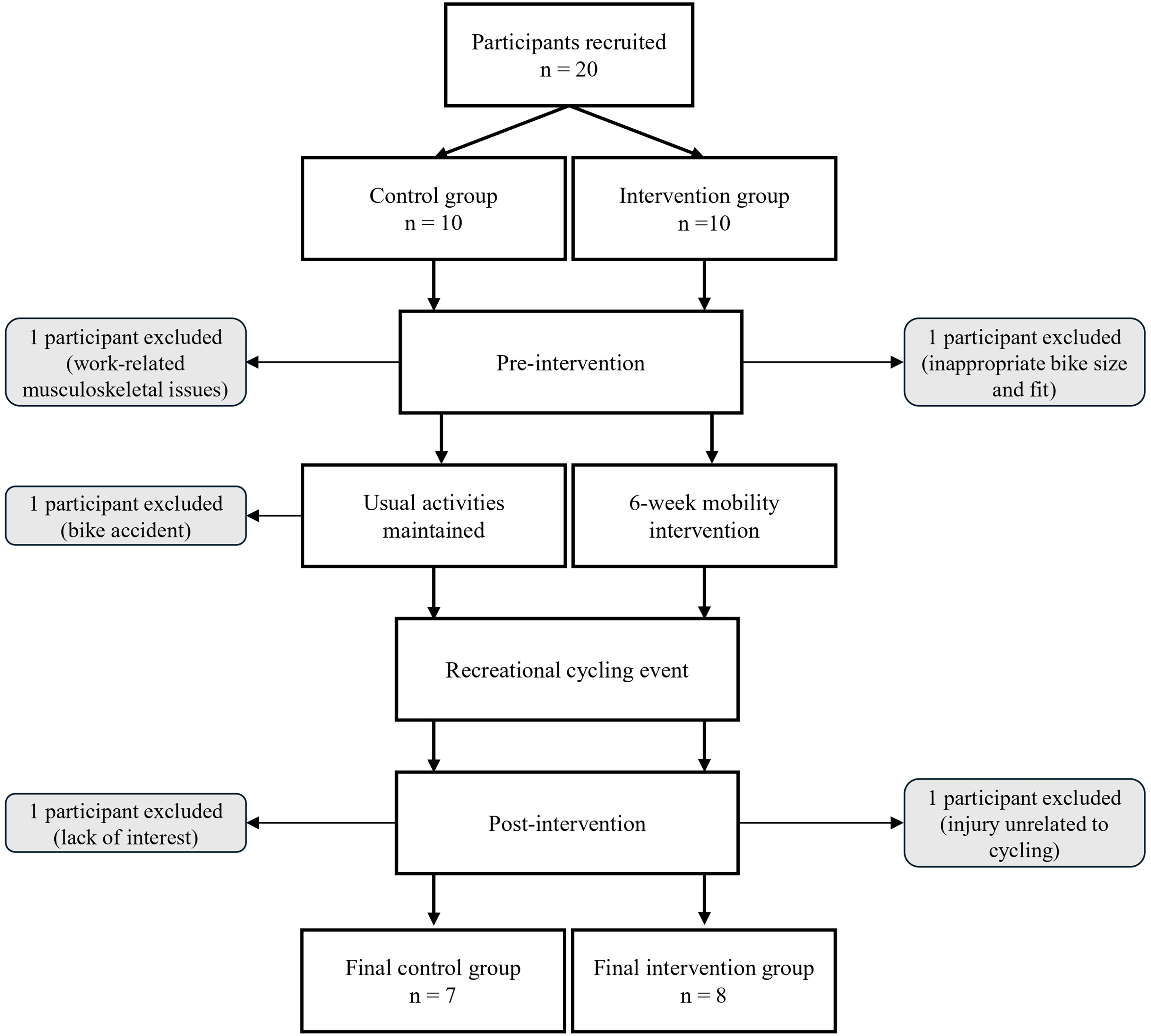
Flowchart of the study.
Protocol
Each participant attended the university kinesiology clinic individually on two occasions: pre- and post-intervention. The pre- and post-intervention visits occurred 6 weeks before and 1 week after the recreational cycling event, respectively. The post-intervention visit was scheduled one week after the recreational cycling event to ensure that fatigue, pain perception, and flexibility were not affected by the event. These visits were scheduled around the same time of day to ensure consistent timing and minimize potential effects on flexibility measurements. Forty-eight hours before each visit, participants received an email reminding them not to engage in any physical activity within 24 h and to avoid consuming caffeine, alcohol, or muscle relaxants within 12 h beforehand. They were also instructed to wear their usual cycling gear for the tests. The consent form was sent by email before the pre-intervention visit; however, it was signed at the clinic, allowing participants to read it and ask the research assistant questions if necessary. During each visit, participants completed a series of questionnaires administered through interviews and performed a battery of active flexibility tests. The first questionnaire was the “Get Active Questionnaire” from the Canadian Society for Exercise Physiology, which was used to determine whether participants had restrictions on engaging in physical activity. 21 The second and third questionnaires included participants’ demographic characteristics and training habits. These questionnaires covered sex, age, cycling experience, training history, future training plans, injury history, bike fitting (professional or proshop), occupation type, and participation in complementary sports. The fourth questionnaire was a modified version of the Cornell Musculoskeletal Discomfort Questionnaire. 22 During the pre-intervention visit, the questionnaire assessed musculoskeletal discomfort experienced during the past week, whereas at the post-intervention visit, it assessed discomfort experienced since the previous visit (pre-intervention visit). All four questionnaires were completed at the pre-intervention visit, while only the training habits questionnaire and the modified version of the Cornell Musculoskeletal Discomfort Questionnaire were administered at the post-intervention visit. Then, the battery of active flexibility tests targeted the lower limbs, including the posterior and anterior chains, hamstrings, gluteus maximus, soleus, and quadriceps, bilaterally. At the end of the pre-intervention visit, the research assistant presented, demonstrated and practiced the mobility intervention with each participant of the intervention group. Then, to ensure standardization, all participants in the intervention group were provided with the same foam roller.
Mobility intervention
The mobility intervention includes a sequence of foam roller exercises and proprioceptive neuromuscular facilitation (PNF) stretches. Inspired by Sharman et al. (2006), participants in the intervention group performed the routine two to three times per week over the six weeks preceding the recreational cycling event. 23 The routine typically takes about 15 min, with each exercise done once on each side (right and left). 23 These exercises, inspired by Isidro et al. (2021), Wanich et al. (2007), and Sanner and O’Halloran (2000), can be done alone and with minimal equipment (see mobility intervention in Appendix 1).6,8,11 Using a foam roller (model 8858864, Corength, Decathlon, France), participants performed five back-and-forth rolls on muscles including the hip flexors, adductors, iliotibial band, glutes, hamstrings, and calves, applying pressure that may be perceived as mild discomfort. This foam rolling method was adapted from Pagaduan et al. (2022). 13 Following this, PNF stretches targeted the quadriceps, gluteus maximus, hamstrings, and soleus. Based on Sharman et al. (2006) and Weerapong et al. (2004), participants first performed a passive stretch to the point of mild tension or slight discomfort, without pain.23,24 Next, they performed an isometric contraction against resistance for 5–8 s at approximately 30–50% of their maximal effort. After a 3-s relaxation phase, another passive stretch was applied for 5 to 8 s, again to the point of mild tension or slight discomfort. Participants were instructed to keep a journal of each time they performed the intervention and to bring it to the research assistant at the post-intervention visit.
Musculoskeletal discomfort score
The musculoskeletal discomfort score was calculated using a modified version of the Cornell Musculoskeletal Discomfort Questionnaire. 22 This questionnaire gathered information on the frequency and intensity of discomfort, whether it disrupted their physical activity routine, and, if applicable, whether the discomfort affected one or both sides of specific body regions. Certain body regions were grouped in the questionnaire to simplify the interview and to focus on regions commonly reported for musculoskeletal discomfort among cyclists. A musculoskeletal discomfort score was obtained by multiplying the scores for frequency, intensity, interference, and the number of sides affected for each body region. More specifically, the discomfort frequency was rated on a four-point scale: “several times a day” (3), “once a day” (2), “only occasionally” (1), or “never” (0). Discomfort intensity was rated on a three-point scale: “very uncomfortable” (3), “moderately uncomfortable” (2), or “a little uncomfortable” (1). Regarding interference with physical activity routines, a “yes” response was scored 2, and a “no” response was scored 1. For the number of sides affected by body region, a score of 1 was assigned if only one side was affected, and 2 if both sides were affected. For regions that cannot be divided into sides, a score of 1 was assigned. These scores were then summed across all regions to produce each participant's musculoskeletal discomfort score. 25 Thus, a higher score indicates greater musculoskeletal discomfort, whereas a lower score reflects less musculoskeletal discomfort. The pre- and post-intervention scores were used for statistical analysis.
Number of participants reporting musculoskeletal discomfort by body region
The number of participants reporting musculoskeletal discomfort by body region was derived from the modified Cornell Musculoskeletal Discomfort Questionnaire. This represents the number of participants in each group (intervention and control) who reported discomfort in each body region assessed by the questionnaire. To evaluate changes over time, the difference between pre- and post-intervention counts was calculated for each body region. These differences were then used in the statistical analyses. For each body region, prevalence was calculated as the proportion of participants reporting discomfort within each group (intervention or control).
Active flexibility assessment
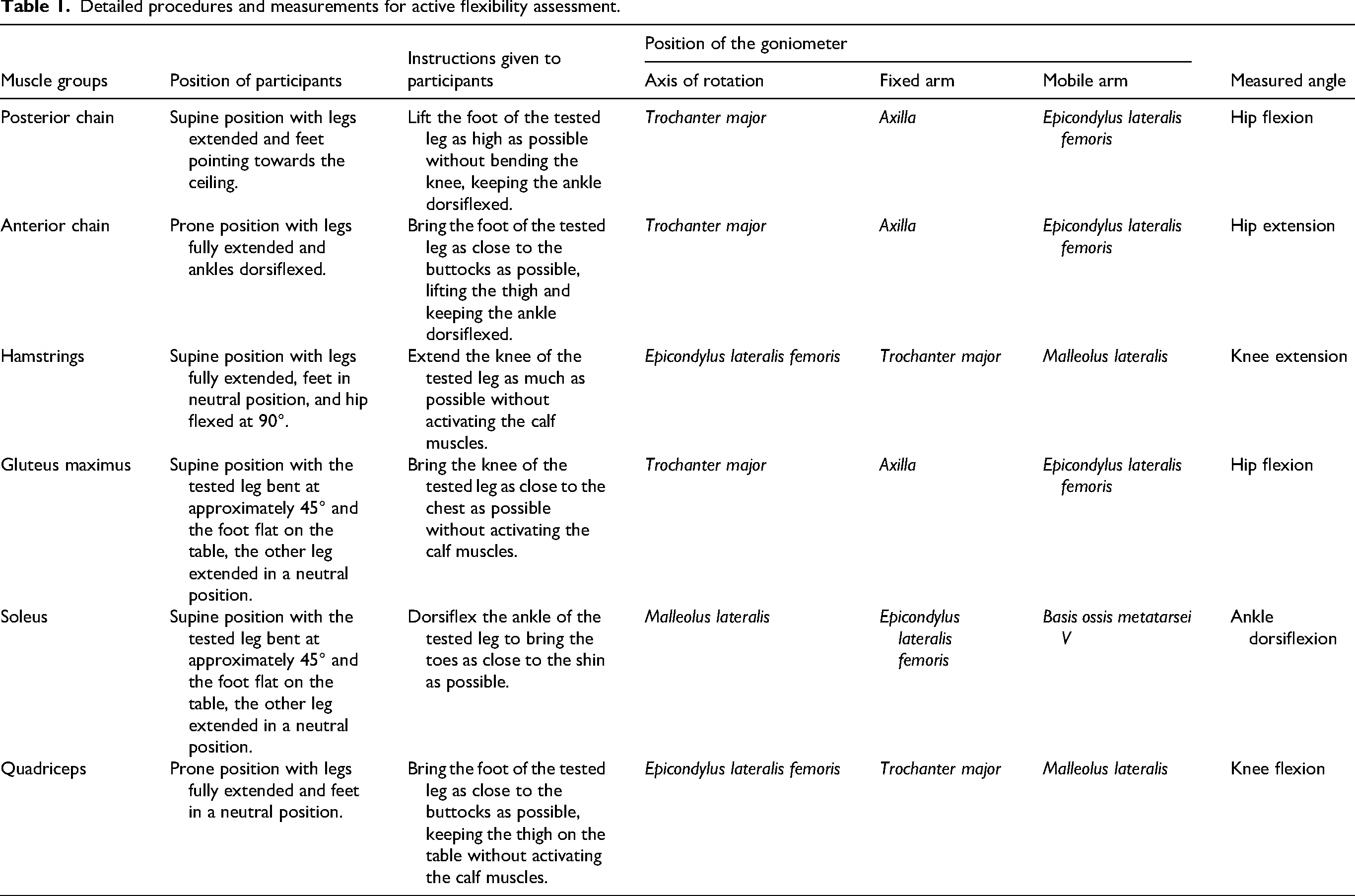
Active flexibility assessment is particularly relevant for cyclists, as it captures the muscles’ ability to stretch during antagonist contraction, a process that happens while pedalling and directly influences its mechanics. It is assessed by active range of motion, which is the maximum joint angle achieved during voluntary contraction of the antagonist muscle, causing the target muscle to stretch. Goniometry was used to evaluate the active range of motion, as it is considered the gold standard. 26 Only one research assistant performed all tests, both pre- and post-intervention, to minimize inter-professional errors. Each test was conducted on a massage table using a digital goniometer (model 35-310, iGaging, USA). Participants wore their usual cycling clothing, which allowed accurate identification of anatomical landmarks and proper placement of the goniometer. The participants’ positions, the instructions provided, the goniometer placements, and the angles measured for each test are detailed in Table 1. The procedures for all tests were inspired from Clarkson (2020), except for the soleus protocol, which was adapted from Witvrouw et al. (2003).26,27 Participants followed the instructions and maintained each position until the angle was taken. Tests were first performed on the left side, then repeated on the right side. For each side, three measurements were taken within a 5-degree range, and the average was calculated to provide a result for each side. If a value exceeded the 5-degree range, the researcher's assistant repeated the measurements. It is important to note that each result was adjusted so that higher angles reflected greater flexibility. Finally, the differences between pre- and post-intervention results were calculated to evaluate changes in active flexibility. These data were then used for statistical analysis.
Detailed procedures and measurements for active flexibility assessment.
Statistical analysis
Descriptive statistics were presented as mean ± standard deviation (SD) for parametric variables. Non-parametric variables were expressed as median [interquartile range] (IQR) for continuous data and as frequencies (%) for categorical data. Inferential statistics were used: i) to confirm that the two groups (intervention and control) were similar in demographic and training habits characteristics, and ii) to evaluate the hypotheses that the mobility intervention would lower musculoskeletal discomfort score, reduce the number of participants reporting musculoskeletal discomfort by body regions, and increase active flexibility.
For the demographic and training habits comparisons, variables such as the number of rides per week, average intensity, and weekly distance were analyzed using independent samples t-tests when the assumptions of normality (Shapiro–Wilk test) and homogeneity of variances (Levene's test) were satisfied (p > 0.05). When these assumptions were violated, the non-parametric Mann–Whitney U test was applied to compare age, cycling experience, and average ride duration. Chi-square tests were used for categorical variables, including sex, current training status, injury history, bike fitting, occupation type, terrain ridden, type of training cycle, use of progressive training, and multisport participation.
To evaluate the hypotheses, data were initially assessed for normality and homogeneity of variances using frequency histograms, Shapiro-Wilk tests, and Levene tests. Non-parametric analyses were used when data were not normally distributed or when variances were unequal. Musculoskeletal discomfort score was analyzed with pre-post within-group comparisons using Wilcoxon signed-rank tests. Changes in the number of participants reporting musculoskeletal discomfort by body region and in active flexibility between groups were compared using independent-samples t-tests. The significance level for all inferential tests was established at p < 0.05. All descriptive and inferential analyses were performed with JASP version 0.95.1 (JASP Team, University of Amsterdam, The Netherlands).
Results
Participants’ demographic and training habits characteristics are summarized in Tables 2 and 3. The study population was predominantly male (60.0%), with a median age of 43.0 years [15.5] and a median cycling experience of 5.0 years [9.0]. Nearly half of the participants (46.7%) reported at least one traumatic injury in the last five years, and 6 (40.0%) had experienced a musculoskeletal injury in the past five years. In the week preceding the visit, 14 (93.3%) reported musculoskeletal discomfort. Thirteen participants (86.7%) reported having a sedentary occupation, whereas only two (13.3%) had an active occupation.
Participants’ demographic characteristics.
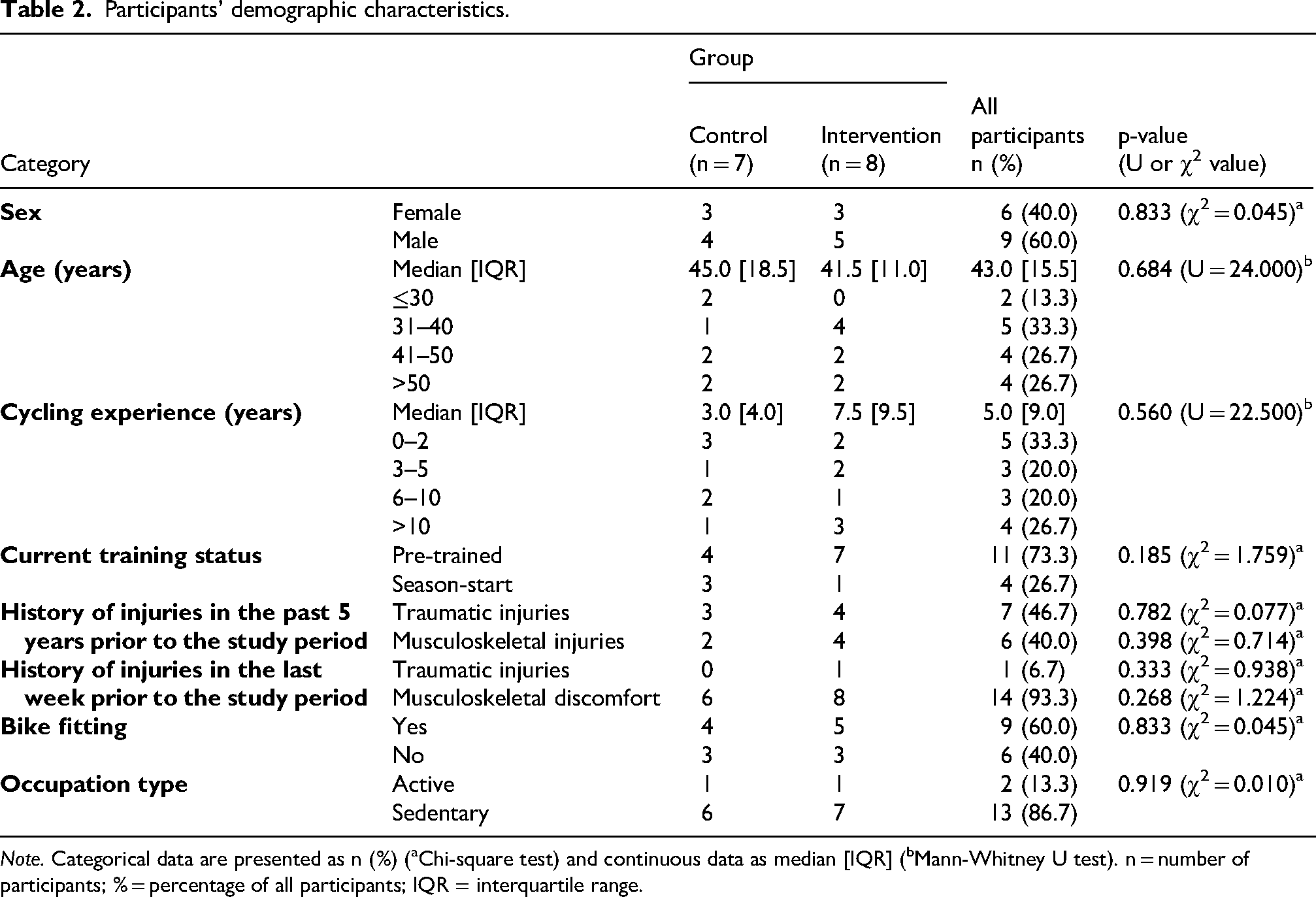
Note. Categorical data are presented as n (%) (aChi-square test) and continuous data as median [IQR] (bMann-Whitney U test). n = number of participants; % = percentage of all participants; IQR = interquartile range.
Participants’ training habits.
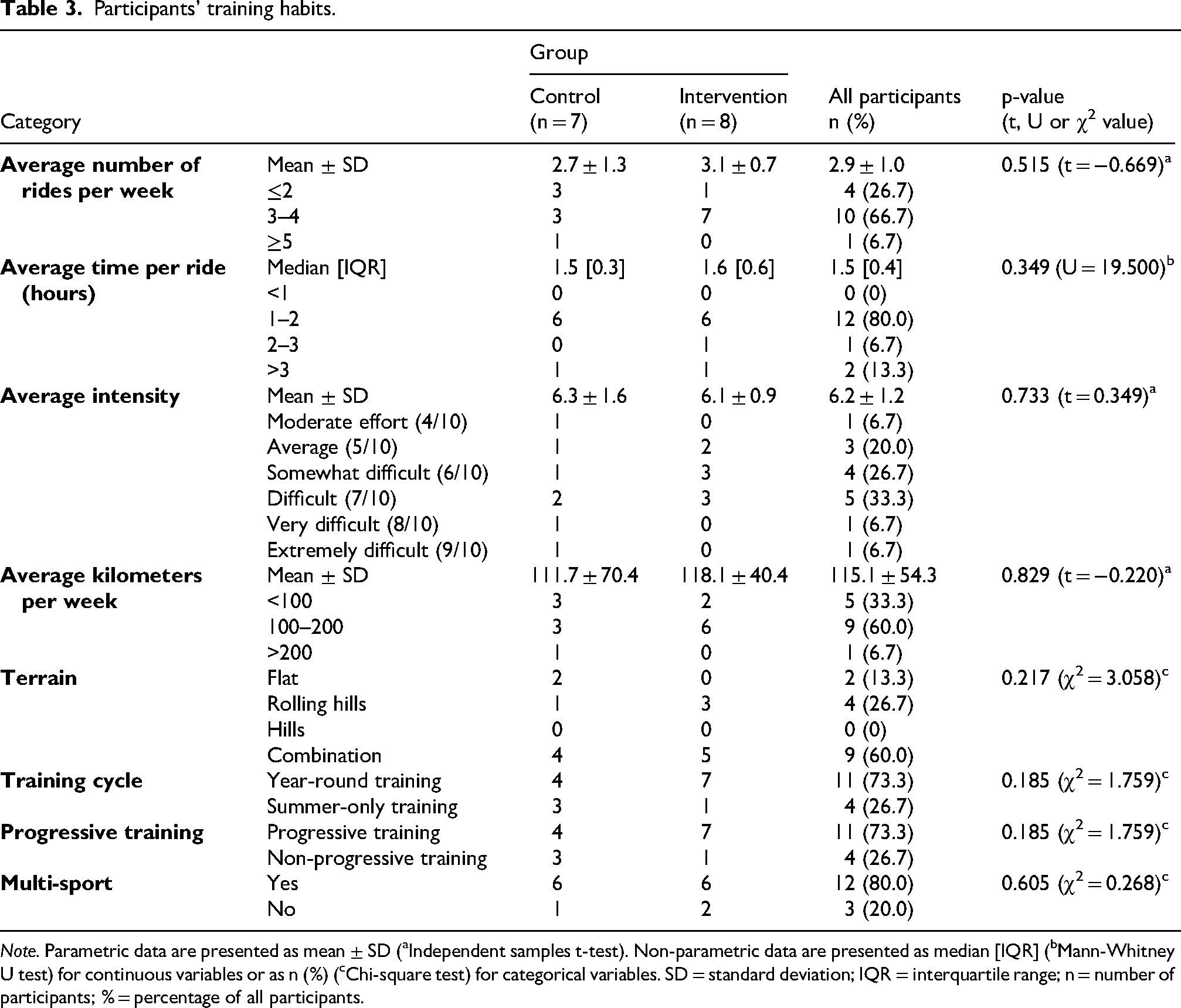
Note. Parametric data are presented as mean ± SD (aIndependent samples t-test). Non-parametric data are presented as median [IQR] (bMann-Whitney U test) for continuous variables or as n (%) (cChi-square test) for categorical variables. SD = standard deviation; IQR = interquartile range; n = number of participants; % = percentage of all participants.
Regarding training habits, at the pre-intervention visit, 11 participants (73.3%) were already trained, while 4 (26.7%) participants were at the start of their season. Eleven participants (73.3%) reported using a progressive training approach, and the same number also trained year-round, while four (26.7%) did not follow a progressive approach or train year-round. Participants reported an average of 2.9 ± 1.0 rides per week, with a median ride duration of 1.5 h [0.4], a mean intensity of 6.2 ± 1.2 out of 10, and a weekly distance of 115.1 ± 54.3 km. Nine participants (60.0%) rode on a combination of terrain (flat, rolling hills, and hills). Most participants (80.0%) engaged in multiple sports, whereas only three (20.0%) focused exclusively on cycling. Nine participants (60.0%) had previously undergone a professional bike fitting (performed by a bike shop or an expert). When comparing both groups, no significant differences were identified in demographic and training habits characteristics.
Table 4 presents musculoskeletal discomfort scores for all participants in each group before and after the intervention. The control group showed a non-significant increase of 2 points in the post-intervention score (p = 0.446; w = 9.000; z = −0.845). In contrast, the intervention group show a significant decrease of 7.5 points in the post-intervention score (p = 0.029; w = 34.000; z = 2.240).
Participants’ musculoskeletal discomfort scores pre- and post-intervention.
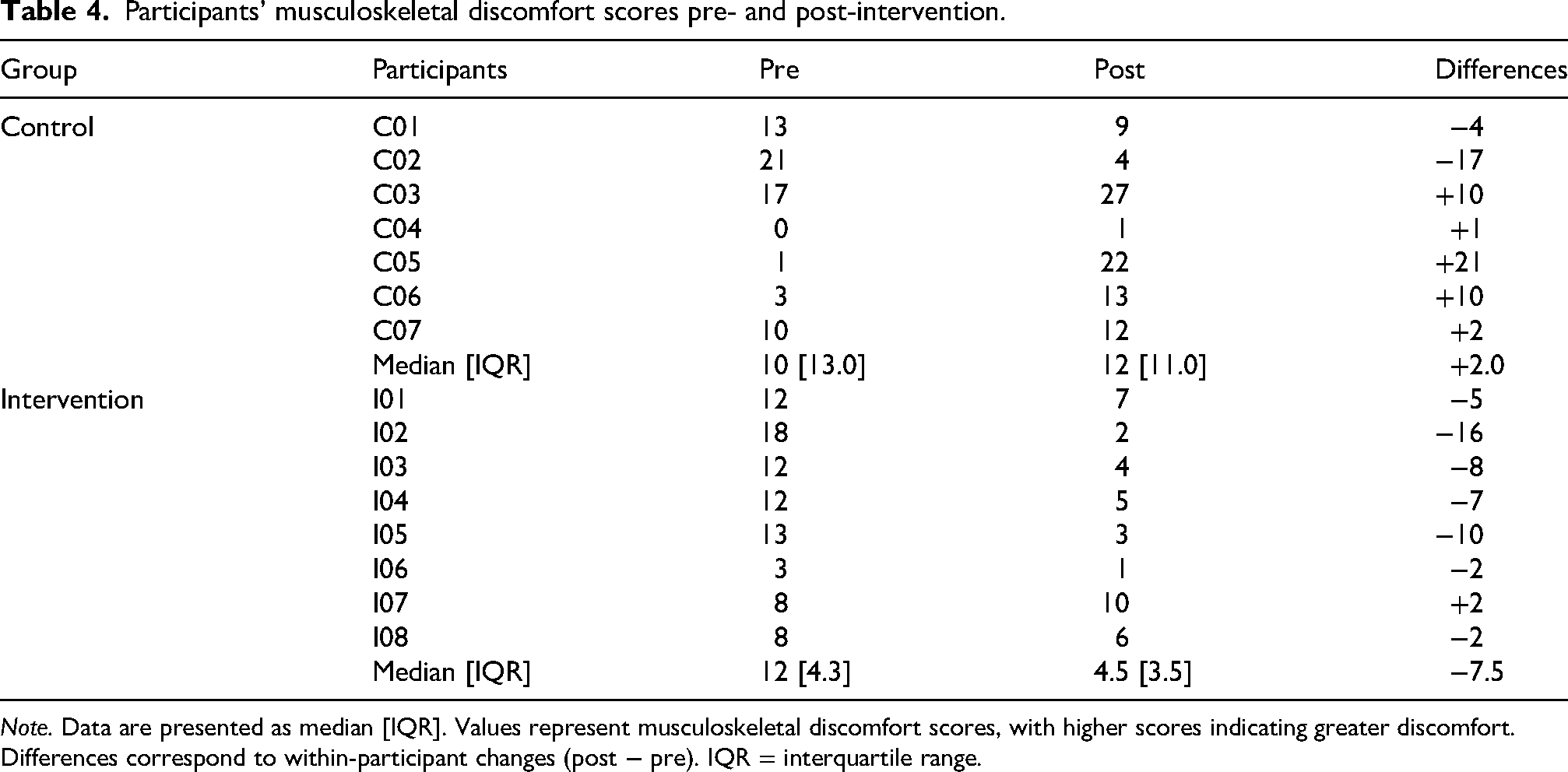
Note. Data are presented as median [IQR]. Values represent musculoskeletal discomfort scores, with higher scores indicating greater discomfort. Differences correspond to within-participant changes (post − pre). IQR = interquartile range.
Table 5 presents the number of participants reporting musculoskeletal discomfort by body region before and after the intervention in both groups. The control group showed an increase in the number of participants reporting musculoskeletal discomfort by body region (1.1 ± 1.5), whereas the intervention group remained relatively stable (−0.1 ± 1.2). Although the difference between both groups was not statistically significant, a tendency was observed, with a mean difference of 1.2, a t-value of 2.071, and a p-value of 0.052. Additionally, a greater number of participants in the control group reported musculoskeletal discomfort across multiple body regions at post-intervention, particularly in the lower back and wrist/hand. In the control group, the number of participants experiencing lower back discomfort increased from 2 (28.6%) pre-intervention to 6 (85.7%) post-intervention, representing an increase of 4 (57.1%). In contrast, no change was observed in the intervention group, in which 3 (37.5%) participants reported lower back discomfort at both time points. A similar pattern was observed for the wrist and hand region. In the control group, affected participants increased from 1 (14.3%) to 4 (57.1%), while the intervention group saw wrist/hand discomfort decrease from 6 (75%) to 5 (62.5%), a reduction of 1 participant (12.5%). In the intervention group, musculoskeletal discomfort decreased, with buttock discomfort declining from 2 (25%) to 0 (0%), although upper back discomfort increased from 0 (0%) to 2 (25%).
Number of participants reporting musculoskeletal discomfort by body regions pre- and post-intervention.
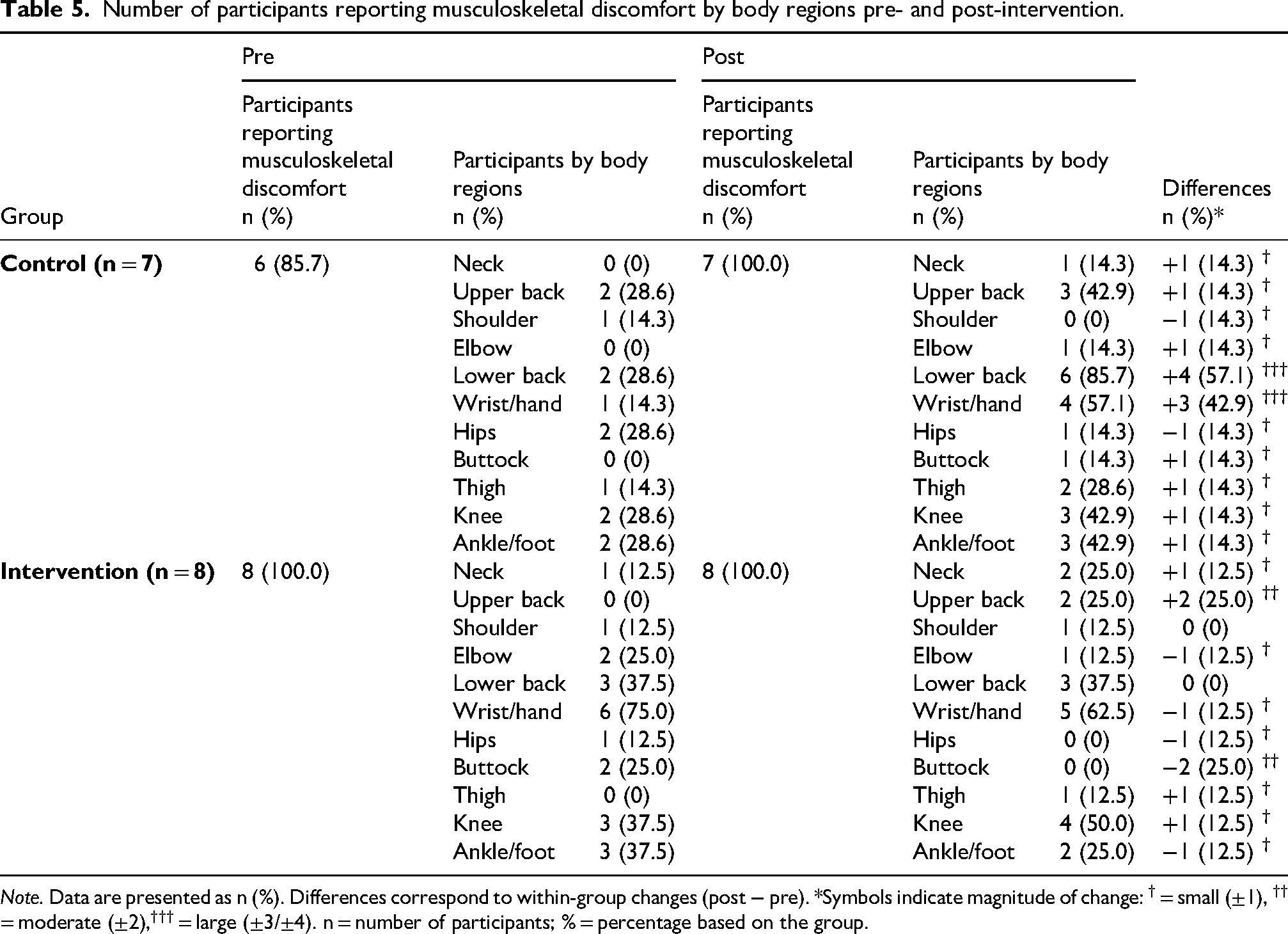
Note. Data are presented as n (%). Differences correspond to within-group changes (post − pre). *Symbols indicate magnitude of change: † = small (±1), †† = moderate (±2),††† = large (±3/±4). n = number of participants; % = percentage based on the group.
Regarding active flexibility results, pre- and post-intervention differences within each group are expressed in degrees (°) and presented in Table 6, along with the results of independent-samples t-tests. Significantly greater improvements in active flexibility were observed in the intervention group compared to the control group for the posterior chain (mean difference = −8.6; t = −2.663; p = 0.013) and soleus tests (mean difference = −2.8; t = −2.146; p = 0.041). A tendency toward larger improvements in active flexibility was observed in the intervention group compared to the control group for the hamstring and gluteus maximus tests (mean difference = −4.2; t = −1.746; p = 0.092 and mean difference = 3.9; t = −1.754; p = 0.090, respectively).
Comparison of mean flexibility differences (°) before and after the intervention period between control and intervention groups.
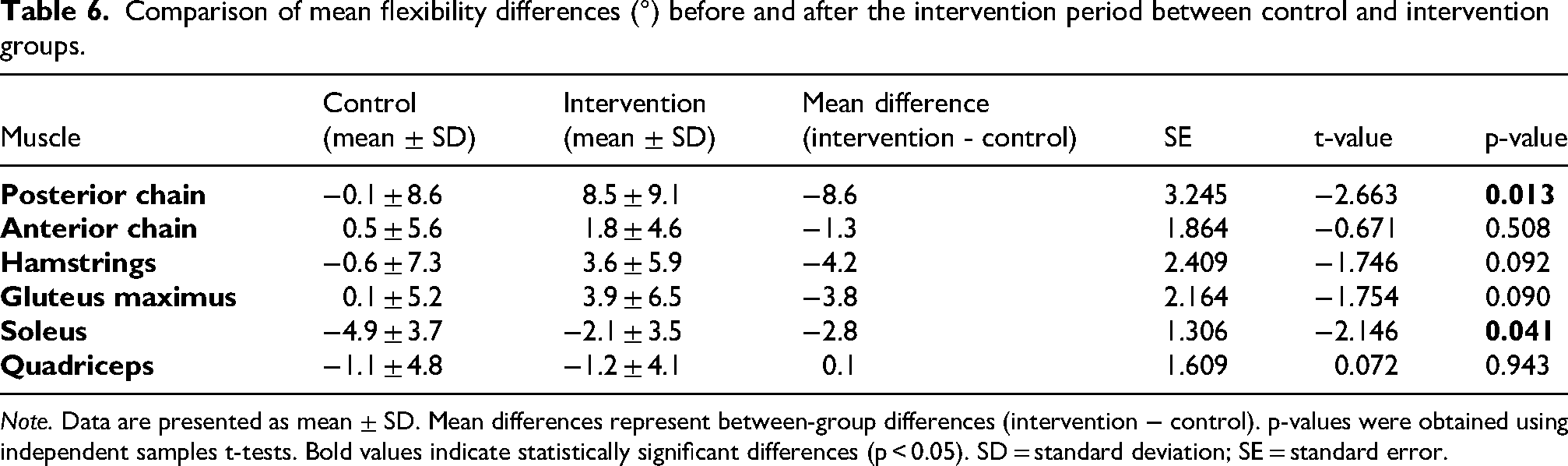
Note. Data are presented as mean ± SD. Mean differences represent between-group differences (intervention − control). p-values were obtained using independent samples t-tests. Bold values indicate statistically significant differences (p < 0.05). SD = standard deviation; SE = standard error.
Discussion
The study examined the effects of a six-week mobility intervention combining foam rolling and PNF stretching of the lower limbs in recreational cyclists prior to a two-day, 250-kilometre recreational cycling event. Results showed that the intervention significantly reduced the musculoskeletal discomfort score and tended to prevent increases in the number of participants reporting musculoskeletal discomfort by body region. Additionally, the intervention group showed greater improvement in posterior chain active flexibility than the control group. Although active flexibility of the soleus decreased in both groups, the decrease was smaller in the intervention group than in the control group. Participants in the intervention group demonstrated high adherence to the mobility intervention. All participants reported completing the intervention at least twice per week between the pre- and post-intervention assessments. These results provide valuable insights into the potential benefits of incorporating foam rolling with PNF stretching into the training routine for recreational cyclists.
The scientific literature addressing the prevalence of musculoskeletal discomfort among cyclists, whether professional, amateur, or recreational, is extensive.3–5,28–34 A frequently cited study by Wilber et al. (1995) reported that, in their cohort of recreational cyclists, the most affected regions were the neck (48.8%), knees (41.7%), groin/buttocks (36.1%), hands (31.1%), and back (30.3%). 28 These findings partially align with those observed in our cohort. At post-intervention, musculoskeletal discomfort in the control group was most frequently reported in the lower back (85.7%), followed by the hands/wrists (57.1%) and the upper back, knees, and ankles/feet (42.9% each). Although the anatomical distribution of discomfort generally aligns with the literature, the prevalence in our sample was markedly higher, particularly in the lower back. Differences in bike type in Wilber's cohort (mountain vs. road) may partly explain this discrepancy, as our participants used only road bikes. Even though the literature examines the prevalence of musculoskeletal discomfort, to our knowledge, no previous studies have specifically examined the effects of a mobility intervention on musculoskeletal discomfort or flexibility (passive or active) among cyclists, regardless of performance level.
Moreover, no study has combined foam rolling and PNF stretching modalities to reduce musculoskeletal discomfort. Nevertheless, the significant reduction in musculoskeletal discomfort score observed in our intervention group aligns with broader evidence supporting mobility interventions, such as stretching, foam rolling, or yoga, for reducing musculoskeletal discomfort. 35 Notably, a 2025 systematic review by Konrad et al. reported beneficial effects of chronic stretching interventions (static, dynamic) lasting 4 weeks to 6 months on musculoskeletal discomfort. 36 Across six studies involving 658 predominantly sedentary and inactive participants (i.e., truck drivers, office workers, and students), five studies reported significantly greater reductions in discomfort in intervention groups compared with controls. As in Konrad's study, our sample consisted mainly of office workers and students, reflecting predominantly sedentary occupations. Despite their sedentary work, our participants were physically active, which could influence the intervention's outcomes due to greater physical demands.
Only a limited number of studies have examined mobility interventions for musculoskeletal discomfort in athletic populations.37,38 Among them, the study by Iranmanesh et al. (2025) investigated the effects of a stretching intervention on several outcomes, including low back discomfort, in male professional football (soccer) players. 39 Football is not a cyclic sport; however, it involves repetitive movement patterns that share biomechanical demands with cycling. In contrast to cycling, football is intermittent and characterized by frequent changes in speed and direction. Furthermore, in Iranmanesh's study, participants were professional athletes who were younger and trained at higher volumes and intensities than recreational athletes. In that study, participants performed dynamic stretching before practice and static stretching afterward, five times per week for 8 weeks, resulting in reduced lower back discomfort.
From pre- to post-intervention, the intervention group showed a trend toward a more similar number of participants reporting musculoskeletal discomfort by body region, whereas the control group showed a greater increase. Specifically, in the control group, four additional participants reported lower back discomfort and three more reported wrist/hand discomfort at post-intervention, while the number of affected participants in the intervention group remained similar in these regions. Although the between-group difference did not reach statistical significance, these findings may suggest that the mobility intervention helps limit the development of discomfort in specific body regions. This interpretation is consistent with the systematic review by Konrad et al. mentioned above. 36 In Konrad's review, two studies assessed musculoskeletal discomfort by prevalence across body regions or the total number of body regions the participant reported as painful.40,41 Significant reductions in these parameters were observed, indicating fewer body regions and fewer participants affected in the intervention groups.
The group that underwent the mobility intervention achieved greater gains in posterior chain active flexibility than the control group. Both groups showed a decrease in soleus active flexibility, but the decline was significantly smaller in the intervention group. The intervention group also showed a trend toward greater gains in active hamstring and gluteus maximus flexibility. These findings suggest that integrating foam rolling with PNF stretching into recreational cyclists’ routines offers benefits for active flexibility. While both PNF stretching alone 42 and foam rolling alone19,43 are generally recognized to enhance active flexibility, combining foam rolling and PNF stretching within the same intervention to enhance active flexibility is relatively uncommon in the literature. Nevertheless, a meta-analysis by Konrad et al. (2021) evaluated the effect of combining foam rolling with stretching (either static or dynamic) on range of motion, comparing it to stretching alone, foam rolling alone, and control conditions. 44 Importantly, the studies included in this review focused exclusively on acute effects, with single-session interventions, rather than chronic effects of the interventions. Their analysis demonstrated that the combined treatment produced greater improvements in range of motion than control conditions, but no additional benefit was observed compared with stretching or foam rolling alone. Notably, PNF stretching was not included in the protocols analyzed in the meta-analysis, leaving a gap in understanding its effects within combined interventions. Our study addresses a gap in the literature by examining the long-term effects of a combined PNF stretching and foam rolling intervention on active flexibility. While our results provide new insights into the effectiveness of this combined method, future research should compare its effects with those of other intervention strategies to determine whether combining these techniques truly offers additional benefits over using each one individually.
Limitations
This study has several limitations that should be considered when interpreting the results. First, the sample was small and heterogeneous, comprising participants from a convenience sample at a recreational cycling event. Thus, the external and internal validity of the findings were limited. As a result, the findings cannot be generalized to other populations, and the participants may have responded differently to the mobility intervention. Second, the recall period for the Cornell Musculoskeletal Discomfort Questionnaire was inconsistent across assessment points: participants reported discomfort from the previous week at the pre-intervention visit and from the previous seven weeks at the post-intervention visit. This discrepancy in reporting periods reduces the comparability of pre- and post-intervention musculoskeletal discomfort scores and may affect the validity of the conclusions. In addition, because the questionnaire relies on self-report, responses may be influenced by recall bias, omissions, or individual differences in pain perception. Furthermore, psychosocial variables such as stress and anxiety, which are known to affect pain perception and the development of chronic symptoms, 45 were not measured and should be incorporated in future studies to provide a more comprehensive understanding of musculoskeletal discomfort. Third, bike fit, another key factor associated with cycling-related discomfort, 6,29 was reported in Table 2, but the effect was not evaluated or controlled, and may have significantly influenced the outcomes of cycling-related discomfort. Future research should include an assessment of bike fitting. Lastly, participants’ training habits were not standardized, and variations in training volume or intensity, as well as exposure to prolonged cycling effort, could have influenced or altered the reported discomfort. Greater control over training-related variables would strengthen the design of future studies.
Practical implications
This study's findings have important practical implications for coaches, kinesiologists, athletes, and sports medicine experts. Adding foam rolling and PNF stretching to recreational cyclists’ training routines has the potential to reduce musculoskeletal discomfort and benefit active flexibility throughout the season. Because musculoskeletal discomfort is common among recreational cyclists, targeted interventions such as foam rolling and PNF stretching might help prevent cycling-related discomfort. These methods should be part of a comprehensive program that also includes strength training, conditioning, and proper bike fitting. A holistic approach is necessary to meet the varied physical needs of recreational cyclists.
Conclusion
A 6-week mobility intervention involving foam rolling and PNF stretching of the lower limb implemented prior to a two-day 250-km recreational cycling event significantly reduced musculoskeletal discomfort and tended to limit the development of discomfort in recreational cyclists. The mobility intervention also appears to increase active flexibility in the posterior chain and preserve soleus active flexibility, which declines more when no mobility intervention is performed. These findings suggest that adding foam rolling and PNF stretching to the routines of recreational cyclists before a cycling event may help reduce musculoskeletal discomfort and benefit their active flexibility. To enhance understanding, future research should investigate psychosocial factors, bike fitting, and training periodization while incorporating biomechanical and neuromuscular aspects of cycling-related discomfort. By clarifying the relationship between active flexibility and musculoskeletal discomfort, sports medicine professionals can develop more effective protocols to improve cyclists’ comfort and support healthier lifestyles.
Supplemental Material
sj-pdf-1-spo-10.1177_17479541261459672 - Supplemental material for Pain-free pedalling: A pre-event mobility intervention reduces musculoskeletal discomfort in recreational cyclists
Supplemental material, sj-pdf-1-spo-10.1177_17479541261459672 for Pain-free pedalling: A pre-event mobility intervention reduces musculoskeletal discomfort in recreational cyclists by Laurence Michaud, Martin Lavallière and Mathieu Tremblay in International Journal of Sports Science & Coaching
Footnotes
Acknowledgements
The authors would like to thank all participants for their time and dedication to this study. We would also like to extend our sincere gratitude to the organizing committee of the Défi Vélo Plein Air 2025 for their collaboration and support, which made this research possible.
Laurence Michaud received scholarships from the Canadian Institutes of Health Research (CIHR) (BESC M) and from the Collectif de recherche sur la santé en région (CoRSeR) at UQAR, Rimouski, Canada.
Ethical considerations
The study received approval from the institutional Research Ethics Committee (CER-2026-801).
Consent to participate
All participants provided written informed consent before taking part in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The student co-researcher was employed by the Association du Cancer de l’Est du Québec to organize the 2025 Défi Vélo Plein Air. This affiliation did not give rise to any conflict of interest regarding the conduct, authorship, or publication of this study.
Data availability
Although the data supporting this study's findings are not publicly available, they can be provided upon reasonable request from the corresponding author. This is necessary to protect research participants’ privacy and prevent the disclosure of confidential information. The detailed mobility program is included in the supplementary materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.