
Abstract
This is a case study of a 45 year old male patient who underwent an emergency laparotomy procedure. Perioperative risks and associated postoperative outcomes could occur from the complex interaction between the patient’s physical health status, the actual surgery performed, anaesthetic procedure and intra/postoperative events. The patient experienced renal compromise and physiological impairment during surgery. This article discusses his assessment and management as well as the various factors which have an impact upon his physiology.
Introduction
The Royal College of Anaesthetists (RCoA 2017) reiterated that all patients subject to anaesthetic procedures are exposed to potential risks of respiratory, circulatory or airway compromise and that inadequate management of such patients can result in complications. Deterioration in clinical manifestations of critically ill patients should prompt immediate intervention and intensive monitoring of the patient’s vital signs, to prevent an adverse event and to improve the patient’s outcomes (RCoA 2012).
Perioperative risks and associated postoperative outcomes can result from the complex interaction between the patient’s physical health status, the actual surgery performed, anaesthetic procedure and intra/postoperative events (Simpson & Moonesinghe 2013). In this case study, the systematic assessment and management of a 45 year old patient undergoing an emergency laparotomy will be discussed. There is a focus on care of the patient from arrival at the post anaesthetic care unit (PACU), until transfer to another unit.
The impact of actual pathology, anaesthetic and surgical inputs are highlighted by the RCoA (2012) as important factors which contribute to the patient’s physiology and thus their outcomes. Consequently, the levels of care provided in relation to monitoring (NICE 2011, 2017a), balanced fluid therapy (NICE 2017b), wound assessment, pain and postoperative nausea and vomiting (PONV) management would be explored in accordance with AAGBI (2015) guidelines.
Practice location and staff are anonymised and patients names have been changed for confidentiality reasons in compliance with Health and Care Professions Council (2016), trust policy and university regulations. The patient will be called Wilder, whose verbal consent was obtained in accordance with local trust guidelines. The local trust did not highlight any requirement to obtain ethical approval for the purposes of this case study provided that consent was given by the patient.
The Wilder case
Wilder arrived in theatre for emergency laparotomy for suspected peritonitis secondary to perforated peptic ulcer. His presenting symptoms included severe abdominal pain, abdominal distension, and nausea and vomiting. Laparotomy is a major abdominal surgery performed on patients presenting with the above symptoms, its purpose being to diagnose the cause and, in majority of cases, treat the condition (Azer 2016). It involves a complex clinical pathway for the patient, requiring inputs from clinicians across diverse specialties. Due to its high-risk nature, it is usually associated with significant mortality and morbidity as highlighted by Azer (2016).
The National Emergency Laparotomy Audit (NELA 2012) was established by a consortium of working parties in anaesthesia, surgery, research and quality improvement. This was in response to a call by the Healthcare Quality Improvement Partnership (HQIP 2011) to introduce audit proposals with the aim of providing reports on the existing variations in mortality and care provisions for varieties of surgical patients across England and Wales. This was also supported by Saunders et al (2012) in a report conducted on behalf of UK Emergency Laparotomy Network which indicated a high incidence of a non-risk-adjusted mortality of 14.9%, increasing to 24.4% in patients aged 80 and over. Since the establishment of NELA (2012), audit reports have been published over the years to highlight the status of care quality improvements for emergency laparotomy patients. However, the NELA (2016) audit report still portrays incidence of mortality ranging between 13–18% at 30 days postoperatively.
Related complications of laparotomy are:
postoperative hypoxaemia sepsis hypovolaemia hypothermia hypotension myocardial depression renal impairment pulmonary dysfunction and fluid imbalance (Schietroma et al 2013).
Wilder was preoperatively assessed in accordance with the NELA (2014) pathway and his expected risk of death pre and post surgery was documented as <5% hence the recommendation for PACU recovery prior to transfer to another unit. He was graded as American Society of Anesthesiologists (ASA II), a risk stratification metric for classifying patients based on their preoperative physical health state according to the American Society of Anesthesiologists (2014).
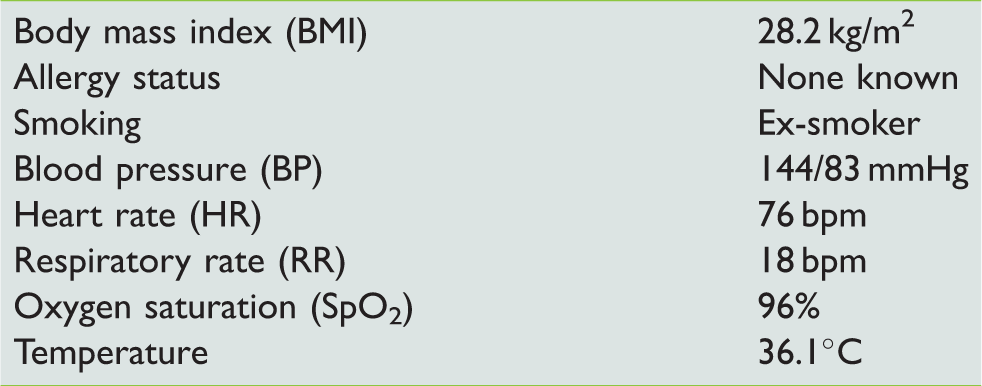
The patient’s history and pre-anaesthesia baseline parameters are presented in Tables 1 and 2.
Pre-anaesthesia baseline parameters for patient Wilder
Pre-anaesthesia pathology and blood gases
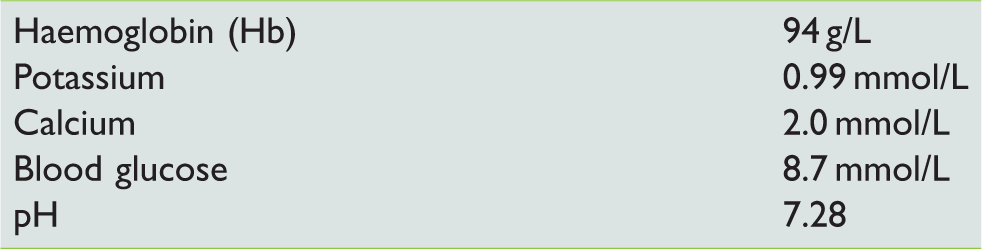
Initial pathology and blood gas results indicated are tabulated below (Table 2).
Wilder’s other comorbidity was noted as depression and he had been on fluoxetine 40 mg od, which he had not taken prior to admission. Fluoxetine is a potent inhibitor of certain hepatic cytochrome P-450 enzymes and may increase plasma concentration of drugs that are cleared via hepatic metabolism such as benzodiazepines (Attri et al 2012). Additional to an impaired biological response to stress, psychiatric patients are at increased risk of perioperative complications, including adverse responses during anaesthesia (Attri et al 2012). Some of these adverse responses may include arrhythmias, hypotension, prolonged narcosis, hyperpyrexia and postoperative confusion all of which ought to be considered by the anaesthetist and care givers.
Intravenous (IV) anaesthetic agents given included propofol (1% 180 mg), fentanyl (100 mcg), ondansetron (8 mg), rocuronium (120 mg) not only to facilitate smooth intubation but also to paralyse the patient’s diaphragm and abdominal wall muscles (Masden et al 2015) during surgery and closure of fascia. Closing fascia when muscles are not paralysed can adversely impact upon outcomes such as wound dehiscence, wound infection and incisional hernia (Masden et al 2015).
Administration of co-amoxiclav and tranexamic acid (2 g) was commenced at admission. Although there is no single physiological threshold defined, the use of tranexamic acid, according to Lamb et al (2014), may be indicated for patients suspected of:
physiological derangement significant haemorrhage requiring massive transfusion (>10 units packed RBC) severe metabolic acidosis (pH <7.30) hypothermia (<35°C) lactate >5 mmol/L or prolonged operative time (>90 minutes).
Damage control resuscitation
The past decade has seen an emergence of a paradigm known as damage control resuscitation (DCR) which focuses on preoptimization or initial resuscitation and early use of blood products including tranexamic acid among others, to prevent the lethal triad of acidosis, coagulopathy and hypothermia (Lamb et al 2014). The purpose is ultimately to stabilize biochemical and physiological reserve prior to anatomical or surgical repair, depending upon the degree of suspected physiological compromise (Schochl et al 2014).
Intraoperatively, the following were administered to Wilder:
Morphine (5 mg) Calcium Gluconate (10 mls) Actrapid (100units) 50% Dextrose Metaraminol (5 mg) Adrenaline (1:10,000 - 100 mcg) and Plasmalyte-148 commenced during anaesthesia.
A nasogastric tube, urinary catheter and other invasive monitoring were inserted, in line with NELA (2016) guidelines. An epidural catheter was inserted for analgesia purposes. Intraoperative average parameters included:
mean arterial pressure (MAP) 8mmHg HR: 88 bpm core temperature: 36.5°C SpO2: 97% on 55% FiO2 and stable cardiovascular status.
The perforation was repaired using an omental patch and the operation lasted 3.5 hours although requiring metaraminol boluses.
Wilder received paracetamol (1 g) and sugammadex (300 mg) prior to the procedure end-time. He was extubated in theatre and arrived at PACU with 40% O2 (10 L/min) via a venturi mask by a portable O2 cylinder to prevent de-saturation, in line with RCoA (2012) guidelines. This was changed to a wall outlet piped supply in PACU.
He was slightly hypotensive on arrival which was likely to have been induced by the sugammadex (Drugs 2017), although this improved with subsequent BP reading. All necessary airway adjuncts and monitoring equipment were readily prepared in compliance with AAGBI recommendations (2015). Wilder was systematically assessed using ABCDE-FG approach in line with local protocol and AAGBI (2013) guidelines. Monitoring included:
invasive BP (IBP) electrocardiogram (ECG) pulse oximetry tympanic thermometer and physical observations.
The NELA (2016) and RCoA (2012) publications pinpoint that intraoperative monitoring, effective pain control and perioperative normothermia can all aid recovery and improve outcomes.
A (Airway)
Wilder was conscious on arrival, able to respond to prompts and could maintain his airway and thus did not require capnography monitoring (AAGBI 2015). His saturation and verbal response indicated absence of obstruction and he appeared to have good protective reflexes.
B (Breathing)
Signs of respiratory distress were assessed in accordance with Resuscitation Council UK (RCUK 2015) guidelines:
use of accessory muscles nose-flaring or mouth-breathing see-saw abdominal movement.
None of the signs of respiratory distress were present and there was no increased work of breathing. The resting respiration rate (RR) was 16 bpm; the rhythm was assessed by looking, including depth and chest movements which were bilateral and symmetrical. Listening helped to assess for secretions, wheezing, stridor or crackles which may have indicated the presence of fluid in the small airways. Chest auscultation was performed to evaluate the pulmonary condition with regard to signs of pneumo/haemothorax.
Smoking and emergency surgery are among the risk factors for developing postoperative pulmonary complications, both of which applied in Wilder’s case. Another associated morbidity is postoperative hypoxaemia, partially due to pain preventing the patient from coughing effectively and breathing deeply (Hatfield 2014). Coughing and deep-breathing have been shown to aid in mobilizing secretions and re-expanding collapsed areas of the lungs for improved functional residual capacity postoperatively.
Abdominal wound pain, coupled with his previous smoking history, was suspected to have contributed to Wilder’s inability to cough effectively and to take deep breaths when his saturation transiently dwindled to 92%. However, he reported a pain score of 0 on assessment and thus deep breathing was encouraged. Cyanosis was absent (peripheral cyanosis was assessed via nail bed colour, central was assessed via lips colour and mucosa). His National Early Warning Score (NEWS) was 7. NEWS is an assessment tool developed by the Royal College of Physicians (RCP 2017) to identify acutely ill patients.
C (Circulation)
Warmed Plasmalyte-148, commenced intraoperatively, was titrated to a lower flow. Use of Plasmalyte-148 was indicated based on peritoneal irritation from initial assessment and for intraoperative fluid replacement (Baxter Healthcare 2017). Skin temperature was assessed for peripheral perfusion and felt warm to the touch; capillary refill was checked via finger-tip pressure raised to heart level and was 2 seconds.
Pulse (carotid and pedal) presence, rate and character/regularity were palpated and were acceptable; the rate corresponded with pulse oximeter and HR (ECG) readings. Skin pallor was checked and appeared pink/perfused, not diaphoretic. Core temperature was measured at 36.9°C. Heart rate (HR) was 70 bpm, and MAP was 65 mmHg.
IV cannula sites were assessed for bleeding, phlebitis and kinking and all appeared patent. Adequate perfusion was confirmed using ECG as recommended by RCUK (2015), to assess not only cardiac status but also to detect a return to spontaneous circulation.
Wilder became hypotensive with BP reading 90/57 but this was addressed by elevating his lower extremities above his heart level through a bed recline to increase venous return. The fluid flow-rate was slightly increased to address his hypotensive state since fluid imbalance can contribute to it (Vester-Andersen et al 2014). Epidural analgesia can also cause hypotension; thus, the pain score was ascertained to evaluate the adequacy of pain relief (AAGBI 2011). Wilder’s BP returned to acceptable values on re-positioning and fluid-flow adjustment. Catheter and drain were assessed for integrity, output, pus or blood which may indicate infection or injury, and although patent, urine output was poor (<0.5 ml/kg/hr seen on the catheter urometer). The wound was checked for bleeding and infection since bleeding can stimulate aldosterone to cause decreased urine output via water and sodium-retention.
D (Disability)
Wilder’s level of consciousness (LOC) was assessed using AVPU (Alert/response-to-Voice/response-to-Pain/Unresponsive) in concordance with local and national (AAGBI 2013) guidelines. Wilder was alert and responsive to all prompts. Pupils were assessed for size, symmetry and reaction to light and were acceptable. Epidural block levels were assessed using Bromage scale (AAGBI 2011) for motor which scored (0); sensory block was assessed using dermatome assessment and he felt cold sensations. He could move all his lower extremities in accordance with trust protocol guided by AAGBI (2011).
RR, HR, BP and sedation scores were monitored regularly and there was no sign of respiratory distress which can occur where block exceeds T6 (Nimmo & Harrington 2014). A benefit of epidural anaesthesia is the reduction of the neuro-hormonal input to a postoperative stress response thereby improving mobility (Nimmo & Harrington 2014). Blood glucose level also impact upon LOC, hence were measured (6 mmol/L).
E (Exposure)
Consent was verbally obtained for assessment of pressure areas while maintaining dignity and all appeared intact. The patient could shuffle independently. Adequate pillows and clean, fit-for-purpose linens were provided in accordance with Department of Health (DH 2013) requirements to provide comfort and maintain normothermia (NICE 2016).
F (Fluid)
Wilder received 3000 mls of warmed crystalloid intraoperatively. The last 1000 mls was continued in PACU and titrated over hours, as per instructions. Intraoperative blood loss was 2000mls and replacement included packed red cells (3 units), platelets (1 unit) and gelofusine (500 mls).
NELA (2016) guidelines reiterate that adequate pre/intraoperative resuscitation prior to and during emergency laparotomy is recommended as the key to improved outcome, since tissue hypoperfusion can result in organ failure which relates to prolonged length of stay and high mortality.
According to Sista et al (2013), the surgical stress response in laparotomy is usually overwhelmed by stress from potential intraabdominal sepsis and the associated systemic and immune responses. Intravascular volume depletion is a major complication and these losses can be through:
surgical site bleeding evaporation from exposed peritoneal structures sequestrated fluids in extra-cellular and intra-vascular spaces and potentially epidural dural puncture (Gravlee 2016).
Evidence/physiological response to stress
Evidence suggests that fluid type, volume and administration timing as well as the patient’s baseline physiology influence gastro-intestinal (GI) functional recovery and outcome (McConachie 2014). Fluid imbalance may be caused by fluid transudate into atonic bowel, reducing fluid availability for general circulation, thus rendering the patient hypovolaemic. This hidden fluid is termed third space losses.
Fluid overload is equally deleterious due to the intestinal fluid dynamics that are affected by several factors that cause a shift in the intestinal capillary Starling forces (fluid movement across capillary membranes) according to Woodcock (2017). These factors are:
the patient’s pathology hypovolemia alteration in microvascular permeability venous pressure among others.
The extracellular spaces around the intestines are prone to edema formation owing to the highly fenestrated capillaries. Hypo/hypervolemia and peritonitis may also cause intestinal oedema among other impairments and bowel manipulation and exposure can disrupt GI fluid balance (Pathway Medicine 2015). Intestinal circulation (IC) is vital in maintaining GI haemodynamic stability to support such functions such as absorption, peristalsis, faeces formation/excretion and crucially in sepsis and haemorrhage regulation, via protection of mucosal barrier. Anaesthetic agents impact upon IC, where propofol decreases mesenteric vascular resistance (MVR) (Baid et al 2016), increasing IC within the small intestine, despite its marked decrease in MAP. Inhalational agents (eg sevoflurane) also affect MVR through cardiovascular effects including BP and cardiac output as well as circulatory catecholamines (Baid et al 2016).
Stress causes adaptive responses which are fundamental for life as described in the general adaptation syndrome principle. The response comprises of three stages: alarm response, resistance and exhaustion (Lucille 2016, Tortora & Derrickson 2014). Physiological stress is induced by disease and other assaults such as haemorrhage. Haemorrhage decreases cardiac output and organ perfusion and elicits a reflexive decrease in vagal tone while increasing sympathetic response, thereby raising HR and systemic vascular resistance.
In the acute phase of the stress response, BP increases transiently to compensate before hypotension occurs due to exhaustion (Ryan et al 2012). Trans-capillary refill occurs following haemorrhage, to restore lost intravascular fluid by shifting interstitial albumin into the extravascular compartment via the capillary oncotic and hydrostatic pressure mechanism (Yartsev 2015). The renin-angiotensin-aldosterone pathway which is activated by haemorrhage or dehydration causes water-sodium retention and decreased urine output which may have played a role in Wilder’s low urine output. Haemopoietic response to haemorrhage is rapid as erythropoietin in bone marrow produces and releases erythrocytes into the circulation whilst the kidneys proliferate them. Pain also affects urine output by activating a noradrenergic response which decreases renal perfusion and output (Hatfield 2014).
Wilder’s preoperative low Hb concentration may have impacted upon his haemodynamics (pH, CO2, HCO3, H+, lactate) since metabolic activities require sufficient O2 supply (Yartsev 2015). Blood, vasculature and the heart facilitate supply and transport of O2 and other substrates into cells for energy (adenosine-triphosphate) production. Red blood cells (RBC) carry Hb which transports O2 with each Hb molecule binding four O2 molecules. Additional to surgery, sepsis, inflammation among others, O2 partial pressure (PO2) is a vital determinant of how much O2 -Hb affinity exists in RBC. In tissue capillaries where PO2 is low, Hb holds less O2 as it dissolves and diffuses into tissue cells (Otto et al 2013). Hence, low Hb concentration translates into a lower number of O2 molecules reaching the cells, thereby requiring increased O2 delivery/supply. This phenomenon might have contributed to Wilder’s previous hypoxic poor outcome. This was addressed by initially fluid-resuscitating Wilder hence improving cardiac output to hasten circulation, then increasing FiO2 and RBC transfusion to replace losses and boost Hb concentration.
An hourly fluid chart was commenced in PACU and poor urine output persisted (<0.5 ml/kg/hr) despite all the fluid-load. Urine retention is one of the myriad postoperative complications that may be triggered by transient or absolute hypovolemia and hypotension, which may indicate impaired renal perfusion. Absolute hypovolemia may be caused by surgical blood loss while transient hypovolemia may be due to intra-abdominal hypertension (IAH) which results from edema, or to haemorrhage that elevates abdominal pressure to the point of renal compromise (Chenitz & Lane-Fall 2012). Transient hypotension may be associated with neuraxial analgesia since renal perfusion can still be maintained with 20% of baseline MAP. Wilder’s bladder was scanned for content and a blood sample was sent for analysis of current trends in full blood count, creatinine, urea and electrolytes in line with NICE (2017).
G (Glucose)
Wilder’s pathology and surgery can cause glucose imbalance, hence the attention on his glycaemic status. As resistance to stress adrenocorticotropic-hormone (ACTH), which is secreted by the anterior pituitary, stimulates glucocorticoids release (eg cortisol) that forms glucose through gluconeogenesis (Scheiner 2016, Tortora & Derrickson 2014). Contrary to the insulin effect, the liver is stimulated to release glucose into the bloodstream. Wilder’s preoperative elevated blood glucose may have been due to the stress response which was addressed with the insulin, now measuring (6.0 mmol/L).
Venous thrombo-embolism
Mechanical venous thrombo-embolism (VTE) prophylaxis was commenced on admission (NICE 2015) through to PACU to increase venous flow, with prescribed daltaparin (5000 units). Whilst early mobilization is usually encouraged for adequate pulmonary function and to minimize venous stasis, an epidural catheter in-situ made this impracticable in Wilder’s case. Peripheral edema was absent on assessment. He was given instructions on leg movements to aid VTE prevention.
Pain and PONV management
Evidence supports the efficacy of epidural analgesia in providing effective pain relief in laparotomy procedures when safely and appropriately managed (Nimmo & Harrington 2014). There is a plethora of studies suggesting that block level, baseline systemic and mesenteric sympathetic activity (MSA), volume status and local anaesthetic concentration all impact upon its effectiveness within IC (Ahmed et al 2013). Evidence also suggests that vasodilatation of arterioles and venules would enhance micro and macro circulation if only T8-L1 (MSA occurs) is blocked. Paracetamol was prescribed and was due four hours postoperatively, having received a dose prior to the end of the operation.
Individualised care/hand over
Wilder was orally rehydrated but nil by mouth for 24 hours per postoperative instructions. Extra blankets were offered due to the cold ambient temperature, to maintain normothermia since hypothermia from such exposure can promote wound infection (NICE 2013, 2016). Deep-breathing exercise was encouraged. Wilder was regularly monitored in line with trust protocols and was assessed for pain and PONV to which he both scored 0 (although PONV prophylaxis was prescribed). Pressure areas were intact. Wilder was reassured regarding his surgeon’s visit for debrief. His relative was contacted and informed of where and when Wilder could be visited post transfer, since trust policy did not allow a carer's visit within PACU. Care given was documented.
Additional to his precarious renal function, his NEWS was 7 which was made up by: RR: 2, SpO2: 2, temperature: 0, O2 supplement: 2, MAP: 1, HR: 0. Prescriptions for paracetamol, ranitidine, fragmin (5000 units), naloxone and cyclizine were ascertained. He was transferred to high dependency unit (HDU) using situation background assessment recommendation (SBAR) as proposed by Davey and Cole (2015).
The following information was effectively communicated to the HDU staff: the patient’s NEWS score (which was 7) and observations of some physiological changes that had occurred in PACU. Details of drugs administered intraoperatively as well as in PACU were communicated. Also handed over were the due times for subsequent paracetamol doses, therapeutic antibiotics and ranitidine. Details of VTE prophylaxis and prescribed naloxone (in event of opioid toxicity from epidural) were all handed over to the staff in compliance with AAGBI (2013) guidelines.
Personal belongings, medical notes, prescription charts and health records were complete and handed over to HDU staff. Additional to postoperative instructions, early mobilization was recommended, or a physiotherapist’s attendance to assist with breathing exercises. His serum electrolyte level was recommended for regular monitoring if fluid replacement magnitude increased. It was advised that it may be prudent to assess his jugular venous pulse where CVP monitoring was not feasible as a raised value may suggest renal failure, in which case, hemofiltration would be indicated.
Conclusion
This case study explored a systematic assessment and management of a 45 year old male patient who underwent emergency laparotomy procedure. The primary focus was on the care of the patient from arrival to PACU until transfer to HDU. There is also a discussion of the patient’s pathology and comorbidity with reference to existing evidence relating to the possible impacts upon his physiology. Other factors contributing to the patient’s physiology and outcomes, such as anaesthetic and surgical inputs, have been discussed. The care provided was based on local trust policies as well as national guidelines and recommendations.
Wilder suffered renal compromise which was highlighted as one of the postoperative complications associated with the procedure he underwent. Further investigations and regular monitoring were recommended to ascertain his actual renal status and to plan for a further line of care for him.
No competing interests declared