
Abstract
Background
Postoperative ileus is a common complication of abdominal surgery, leading to prolonged hospital stay and associated costs. Gum chewing may be a safe, cheap intervention to reduce postoperative ileus.
Methods
The aim was to investigate the effect of gum chewing on postoperative ileus in open colorectal surgery patients. A literature search was conducted between December 2018 and March 2019 on CINAHL, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews, MEDLINE, Academic Search Complete, PubMed, Scopus and Google Scholar. The keywords used included ‘ileus’, ‘chewing gum’, ‘mastication’ and ‘sham feeding’. Papers had to include adults undergoing open colorectal surgery. The studies were appraised using Critical Appraisal Skills Programme tools and the results summarised using a narrative review.
Results
A total of three systematic reviews and three randomised controlled trials were included in the study. The studies show a significant to highly significant effect of gum chewing on postoperative ileus-related outcomes. The trials however in general utilised a weak design.
Conclusions
Gum chewing decreases postoperative ileus following colorectal surgery. More robust trials are required to confirm these findings. Due to the low risk of harm and cost of using gum chewing, its use is recommended even in the interim.
Introduction
Postoperative ileus is a common complication of abdominal surgery (Katrancha & George 2014, Keenahan 2014). It results in delayed passage of flatus and stool, with consequent abdominal pain and discomfort, leading to prolonged hospital stay and an increase in associated costs (Kehlet 2008). In the US, prolonged hospital stay and readmissions due to postoperative ileus was estimated to cost between $750 million and $1.46 billion yearly (Katrancha & George 2014, Keenahan 2014).
The pathophysiology of postoperative ileus is still not completely understood; however, literature suggests a multifactorial cause occurring during surgery (Katrancha & George 2014). It has been proposed that bowel manipulation during surgery leads to the activation of inhibitory reflexes and an inflammatory response, leading to generalised bowel dysmotility (Chapman et al 2018). Opioid administration and reduced patient mobility are believed to further precipitate postoperative ileus (Chapman et al 2018, Katrancha & George 2014).
It has been proposed that the initiation of sham feeding after surgery stimulates the production of saliva and increases vagal cholinergic stimulation, leading to increased peristalsis (Keenahan 2014, Meyer & Fawcett 2008). Gum chewing has been proposed as a safe, cheap and practical intervention to reduce postoperative ileus (Katrancha & George 2014, Keenahan 2014); however, individual studies reported inconclusive results (Chapman et al 2018, Liu et al 2017, Yang et al 2018, Zhang et al 2017).
The present review aims to investigate the effect of gum chewing on postoperative ileus in patients undergoing open colorectal surgery by appraising the most recent systematic reviews and any trials not included in these systematic reviews, to determine whether gum chewing can be safely implemented in postoperative colorectal care guidelines to reduce postoperative ileus.
The population included in this review is patients undergoing colorectal surgery. The intervention is gum chewing; the comparison is standard postoperative care. The review investigates the following postoperative outcomes: time to first passage of flatus, time to first bowel movement, time to first bowel sounds and length of hospital stay.
Methods
Eligibility criteria
This review includes only systematic reviews (with or without meta-analysis) and randomised controlled trials, since these provide the highest level of evidence about effectiveness (Straus et al 2018). To be eligible for inclusion in the review, papers had to: include adults, undergoing open colorectal surgery and focus on assessing gum chewing in comparison to standard postoperative care, have been published between 2017 and 2019, not have been included in previous systematic reviews. Studies among children and young adults were excluded. A search on the Medical Subject Heading (MeSH) database defines adults as over 19 years of age (MeSH Browser, 2019).
Studies with patients undergoing laparoscopic surgery were excluded because it is associated with a lower incidence of paralytic ileus and could, therefore, mask any effects of gum chewing (Gustafsson et al 2013). In other types of abdominal operations (eg: gynaecological, obstetric), the extent of bowel manipulation varies. This review was therefore limited to colorectal surgery to reduce heterogeneity. Eligibility was limited to papers published in English and Italian, based on the reviewers’ language comprehension.
Search strategy
The online search was conducted between December 2018 and March 2019 using the following databases and search engines: Cumulative Index of Nursing and Allied Health Litrature (CINAHL) Complete, Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews, MEDLINE Complete, Academic Search Complete, PubMed, Scopus and Google Scholar.
A search on the US National Library of Medicine’s (MeSH) browser resulted in the following terms being identified for use in the search: ‘ileus’, ‘chewing gum’ and ‘mastication’. The preliminary search also indicated the subject ‘sham feeding’, so it was included as a search term. The following search filters were applied: ‘English or Italian language’, ‘adults 19 years and over’, ‘exclude laparoscopy’ and ‘exclude caesarean’.
Study selection
Papers identified through the above search were imported to RefWorks, a web-based reference management software package. Duplicates were removed using RefWork’s ‘Find Duplicates’ feature. The remaining records were then screened on the basis of the title and abstract using the eligibility criteria provided in the Eligibility criteria section. Papers which did not fit the inclusion and exclusion criteria were excluded. The retained papers were then screened on the basis of their full text and any which did not fit the eligibility criteria were excluded. This process was conducted by two independent reviewers to enhance objectivity and reduce the possibility of excluding relevant records (Liberati et al 2009). Disagreement was managed by discussion until consensus was attained.
Data extraction process
Two reviewers independently extracted data from studies into a structured data extraction form. Extracted data included the author and year of publication, the type of colorectal surgery performed, the number of participants in the intervention and control groups, the frequency and interval between gum chewing, the type of care provided to the patients in the control group and the outcome indicators for paralytic ileus resolution.
Appraisal of individual papers
The Critical Appraisal Skills Programme tool for systematic reviews was used to assess the quality and validity of the selected systematic reviews. Assessment of risk of bias for randomised controlled trials was assessed using the Cochrane Risk of Bias tool (Higgins et al 2011). Two independent reviewers appraised the papers. Any discrepancies between results were discussed and consensus was achieved.
Summary measures and reporting of results
The effect of gum chewing on paralytic ileus-related outcomes was evaluated through the difference in means between comparison groups and the corresponding level of statistical significance. The results of the review are presented in tabular form and through a qualitative synthesis.
Results
Studies included in the review
The search on online databases described in the Search strategy section resulted in 549 records and another 43 records from Google Scholar. All of these records’ citations were uploaded to RefWorks. Through RefWorks, 406 duplicates were removed, retaining 186 records. These records were screened by reading through their title and abstract, resulting in 124 records being excluded (Figure 1). The remaining 62 records were screened by reading their full text. Thirty-one records were excluded for reasons summarised in Figure 1. The remaining 31 records consisted of 14 systematic reviews and 17 randomised controlled trials. The final number of studies selected for qualitative synthesis included three systematic reviews and three randomised controlled trials. Although the retrieved systematic reviews included patients undergoing laparoscopic surgery, these papers were still included since subgroup analysis was available.
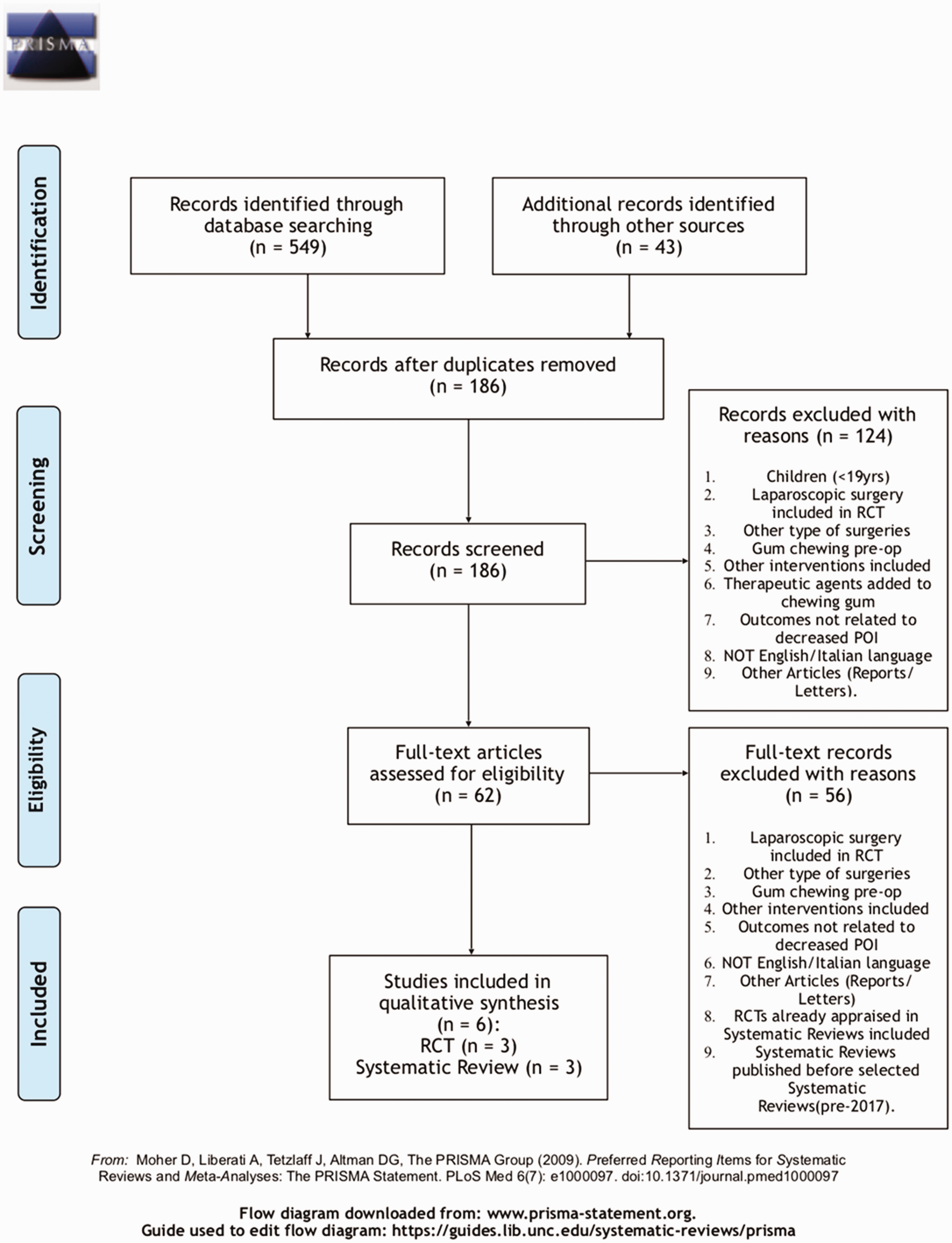
PRISMA 2009 flow diagram
Results and appraisal of recent reviews
The systematic review and two meta-analyses included in the present review included a similar number of randomised controlled trials and trial participants and focused on the same intervention and comparator (Table 1). Both meta-analyses reported positive effects of chewing gum postoperatively with a significant decrease in time to the passage of first flatus, early recovery of bowel movement and a reduction in the length of hospital stay (Liu et al 2017, Mei et al 2017). However, these systematic reviews had some important limitations. Binbin Mei et al’s (2017) review, for example, only included literature published in English and some of the outcomes, such as time to first defecation, were represented by only a small number of studies (n = 4), making it difficult to generalise the results of this review. Both reviews, however, assessed for the possibility of publication bias and there was no indication of this (Liu et al 2017, Mei et al 2017).
Summary of the included systematic reviews
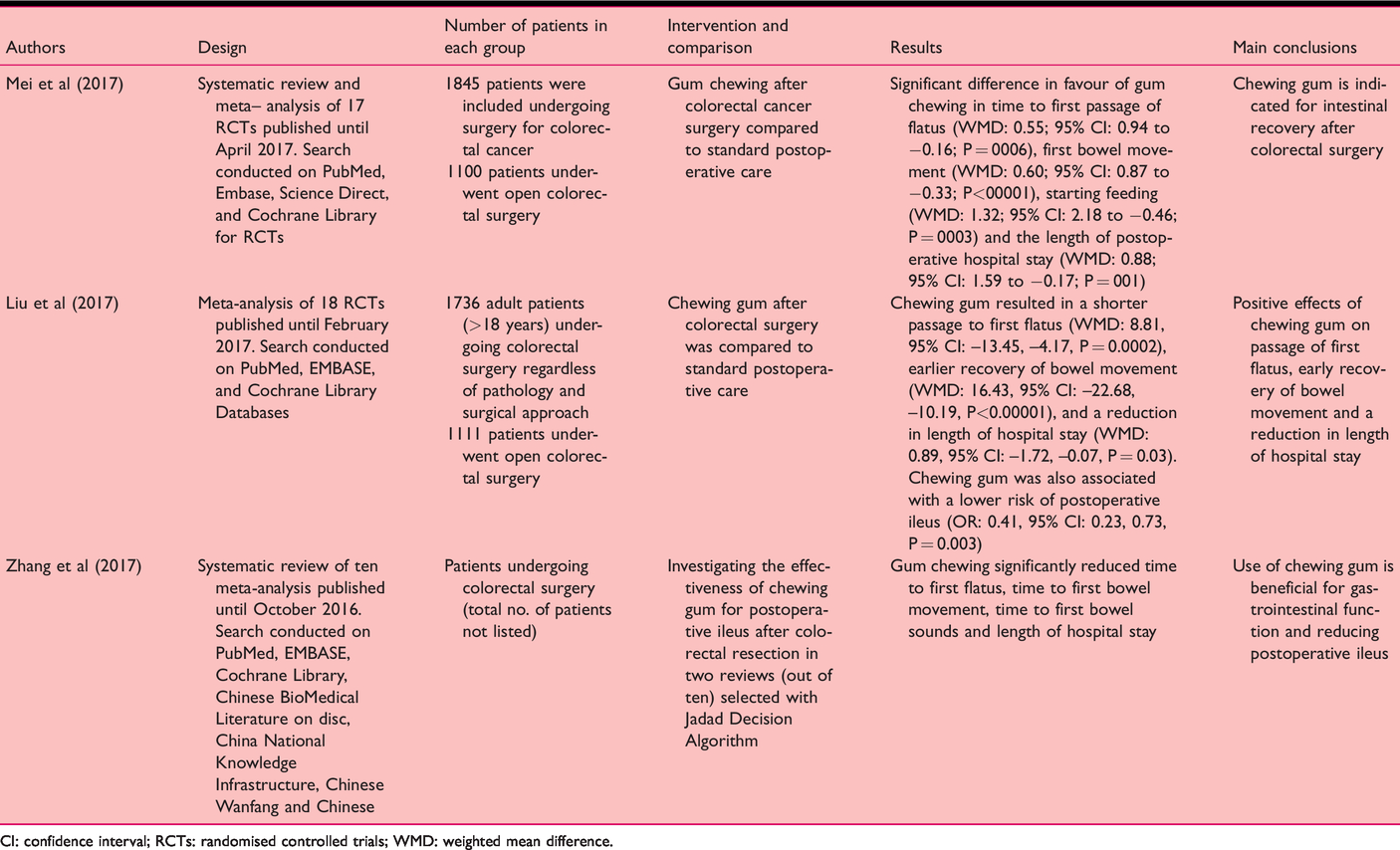
CI: confidence interval; RCTs: randomised controlled trials; WMD: weighted mean difference.
Hui Zhang et al (2017) conducted a review of existent meta-analyses; ten meta-analyses were included in this review. The results showed that chewing gum is useful in reducing postoperative ileus and returning bowel function to normal (Zhang et al 2017). This analysis included a number of strengths, including that the whole process was conducted by two independent reviewers.
Appraisal and results of trials
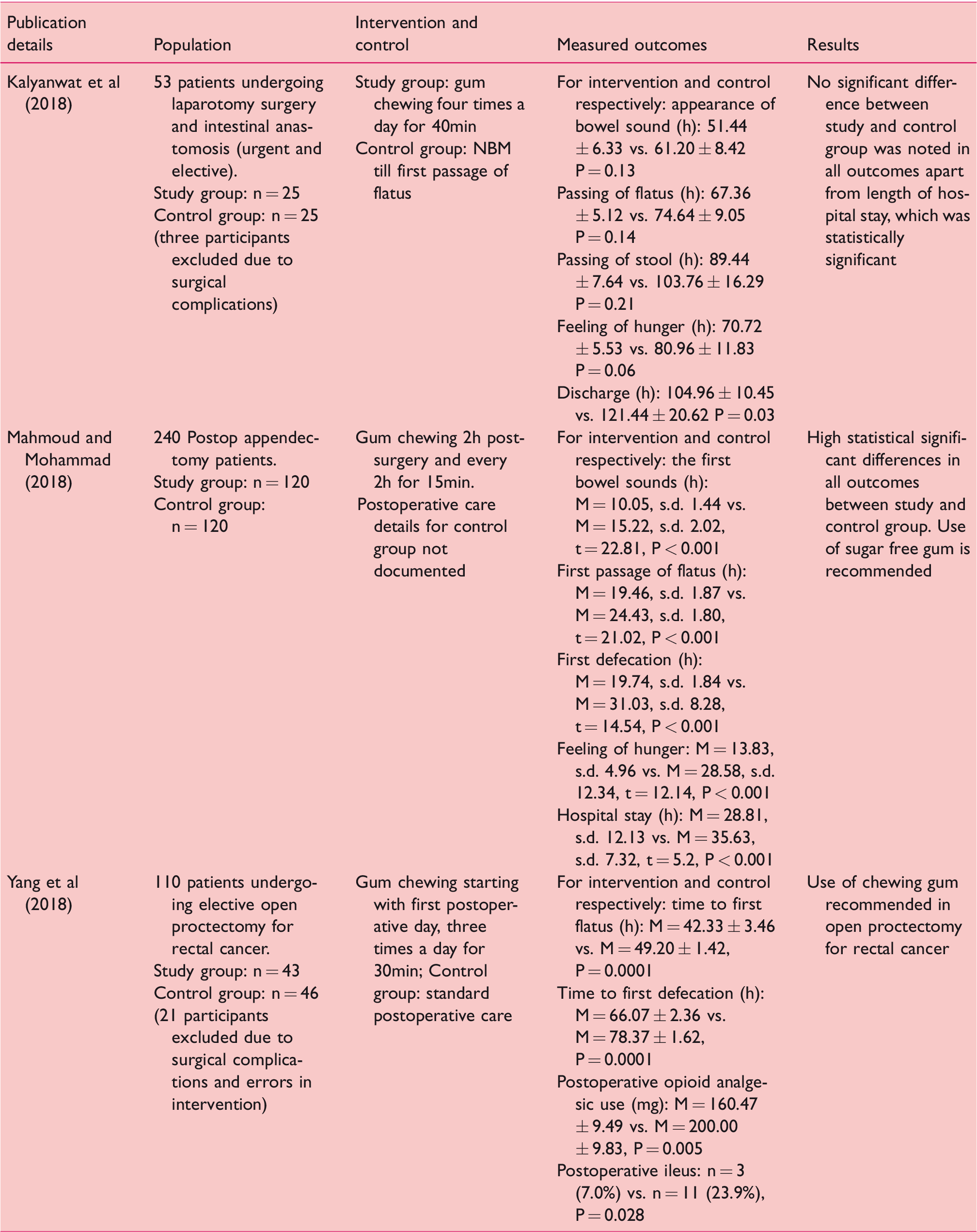
The primary studies included in this review were three randomised controlled trials; the studies are presented in Table 2 and a summary of their appraisal is presented in Table 3. These studies vary in the intervention implementation in relation to chewing gum. Kalyanwat et al (2018), for example, instructed participants to chew gum four times a day for 40min each time, whilst Mahmoud and Mohammad (2018) instructed their participants to chew gum every 2h for 15min every time. In the study by Yang et al (2018), participants chewed gum three times a day for 30min, which is the lowest duration and frequency of gum chewing among the included studies. Yang et al (2018) reported a significantly shorter period of time until resolution of paralytic ileus in the gum chewing group than in the control group (Table 2). Kalyanwat et al (2018) found no difference in the duration of paralytic ileus; the only difference reported was a significantly lower duration of hospitalisation for the intervention group when compared to the control. All three studies therefore suggest that gum chewing postoperatively is beneficial in resolving paralytic ileus at a faster rate than standard treatment.
Summary of the included randomised controlled trials
Risk of bias × other bias – limitations in measuring outcomes (eg: patient-reported outcomes and imprecision of outcome measurement were considered)

In both the studies by Kalyanwat et al’s (2018) and Mahmoud and Mohammad (2018), the main limitation was that the researchers and health care personnel were not blinded, possibly introducing risk of bias in treating participants and outcome measurement. In both cases, allocation to treatment and control group was carried out following surgery, and participant allocation was performed by alternate sequence, which is considered an inadequate type of randomisation, leading to selection bias (Higgins & Green 2006).
In the study by Yang et al (2018), these limitations were overcome by randomly allocating participants to intervention and control groups the day before surgery using the TenAlea random generation software. A sealed opaque envelope was used to conceal the random allocation of participants until the intervention was assigned.
Discussion
The appraised systematic reviews reported a significant reduction of paralytic ileus-related outcomes with gum chewing. These systematic reviews, however, reported unclear to high risk of bias in the included randomised controlled trials, mostly due to the improper random sequence generation and lack of allocation concealment and blinding of participants, personnel and outcomes. Moreover, the reviews include several randomised controlled trials with small sample sizes, which limits generalisation (Liu et al 2017, Mei et al 2017).
An earlier Cochrane Review by Short (2015), which was not included in this present review, did not identify a clear benefit with gum chewing for gastrointestinal recovery, mainly due to the poor study designs with high risk of bias of the included studies. The trials published after these reviews, and included in the present one, reported more positive postoperative outcomes with gum chewing. Kalyanwat et al (2018) reported a significant decrease in length of hospital stay, and Mahmoud and Mohammad (2018) and Yang et al (2018) reported a significant reduction in all paralytic ileus-related outcomes with gum chewing. The results of all three trials should, however, be interpreted with caution because they all include unclear to high risk of bias and other limitations.
The main paralytic ileus-related outcomes considered in most of the papers included in this review, to measure, were time to first flatus, time to first bowel movement/defecation, time to first bowel sounds and time to hospital discharge. Some of these outcomes are very difficult for the researchers to measure precisely; it is for example difficult to detect the time of first bowel sounds by auscultation. Moreover, observer error or inter-observer variation may influence recording of the time of first bowel movement or passage of stool. The time to hospital discharge may also be affected by other factors besides paralytic ileus. Measuring time to first flatus may also not be a reliable form of outcome detection, mainly because it is a patient-reported outcome (Guyatt et al 2011a, 2011b). In a Consolidated Standards of Reporting Trials (CONSORT) report, Calvert et al (2013) introduced a set of criteria for documenting patient-reported outcomes, including using a standard tool for data collection and providing a detailed report of how outcomes are assessed. Such criteria were not documented in any of the studies assessed in this review. Certainly, more precise outcome measures are required in order to increase the validity of the findings at the gum chewing outcomes.
Kendall (2003) points out that a large sample size is the ideal strategy to minimise random error of association between an intervention and an outcome. However, both the systematic reviews appraised and the trials included in this review included small population sizes (less than 100, less than 50). Considerable heterogeneity was observed across studies with regard to treatment applied. The frequency, time and interval of GC and postoperative care adopted (eg: patient ambulation) varied considerably between studies.
Limitations of the present review
The literature search in the present study was limited to studies published in English and Italian, and a search for grey literature and hand searching for articles was not performed, with the risk of missing important relevant studies.
This review is limited to colorectal surgery, excluding other abdominal surgeries with the aim of containing extensive heterogeneity. Several types of colorectal surgeries are performed, incorporating different approaches and bowel manipulation. The type of surgery affects the process of intestinal tract recovery and paralytic ileus (Mei et al 2017). Such heterogeneity presents limitations when results of different randomised controlled studies are combined in a systematic review.
Conclusions
Gum chewing may be considered as a safe, inexpensive and practical intervention in decreasing paralytic ileus following colorectal surgery. Due to its low risk of harm to patients, we can confidently recommend its application in future trials in order to enhance the validity of results of gum chewing on paralytic ileus in open colorectal surgery patients. The trials included in this review include unclear to high risk of bias, with uncertainties in the precision of outcome measurement and small population sizes. Studies with larger populations and more robust study designs are recommended. We also recommend a standardised protocol across studies for the frequency, time and interval of gum chewing, and standardised tools with detailed outcome measurements and reporting in order to increase confidence in results and ability to generalise findings.
No competing interests declared
Footnotes
ORCID iDs
Roberta Sammut https://orcid.org/0000-0002-2354-8808 Josef Trapani ![]()