
Abstract
Blood management is a critical aspect of patient care during surgical procedures. In the United Kingdom, there is a growing recognition of the need to integrate intraoperative cell salvage into blood management protocols, especially for invasive surgeries where significant blood loss is anticipated. While donated blood (allogeneic blood) is traditionally used in such cases, it carries risks and potential complications. Consequently, intraoperative cell salvage presents itself as an appealing alternative, particularly in hip and knee arthroplasty procedures. Intraoperative cell salvage involves the collection and reinfusion of a patient’s own blood (autologous blood) lost during surgery. Studies have consistently shown that autologous blood collected via intraoperative cell salvage has fewer complications and greater benefits compared to donated blood. However, despite these advantages, the widespread adoption of intraoperative cell salvage in UK hospitals remains limited, primarily due to associated costs. While the integration of intraoperative cell salvage into blood management services may incur initial expenses, research suggests that it could ultimately prove to be cost-effective. This is because improved patient outcomes associated with intraoperative cell salvage may lead to reduced postoperative complications and shorter hospital stays. Thus, there is a growing imperative to overcome financial barriers and promote the implementation of intraopertive cell salvage as a standard practice in perioperative care across UK health care settings. The purpose of this scoping literature review is to consolidate the available information on the current use of intraoperative cell salvage and to identify intraoperative cell salvage techniques and devices described for use in an arthroplasty setting.
Introduction
Donor blood, while invaluable, is facing increasing scarcity and cost, notwithstanding its potential life-saving properties, it carries inherent risks such as wrong blood incidents, infection transmission and immunosuppression (Lloyd et al 2023). Managing the supply of donor red cells is a critical concern in the United Kingdom. Due to worries about the potential risk of variant Creutzfeldt–Jakob Disease (vCJD) transmission through blood transfusions, donor selection criteria have been revised to exclude individuals who received transfusions after 1 January 1980. These measures, alongside other donor eligibility restrictions, have exacerbated the decline in blood donor numbers (Ashipala & Joel 2023). The potential introduction of a vCJD test in the future could further impact donor willingness. Such shortages may necessitate restricting transfusions to cases of active major bleeding, emergency operations and life-threatening anaemia. In response, intraoperative cell salvage (ICS) has emerged as a well-established alternative to allogeneic blood in many UK hospitals, endorsed by recommendations outlined in the Health Service Circular–Better Blood Transfusion–Safe and Appropriate Use of Blood. In many cases, the implementation of ICS encounters obstacles, particularly in areas where there is insufficient infrastructure to adequately train staff (Ashipala & Joel 2023). Recognising this challenge, the UK Cell Salvage Action Group, which operates as part of the NHS Blood and Transplant Appropriate Use of Blood Group, was formed. Its primary objective is to bolster the broader adoption of ICS as a substitute for donor blood and to foster a unified approach to its utilisation across the United Kingdom (Ferguson et al 2024).
This paper aims to delve into the significance of ICS within the perioperative setting, examining its merits and demerits, as well as its clinical utility in both primary and revision hip and knee arthroplasty procedures. A scoping review of the literature has been undertaken to identify common themes and insights on this subject matter. The resulting themes encompass the use of ICS, its advantages and disadvantages and its application in total hip and knee arthroplasty. Moreover, tailored recommendations including training for perioperative staff will be provided, with the overarching goal of augmenting patient health outcomes during and after operations.
Brief history of the origins of cell salvage
The inception of cell salvage and autologous transfusion traces back to 1818, when Blundell, a pioneering gynaecologist, initially employed these methods in managing post-partum haemorrhage (Grainger & Catling 2018). In this early application, blood-soaked swabs underwent saline washing before reintroduction into patients, albeit yielding notably high mortality rates. The exploration of cell salvage and autologous transfusion endured into subsequent centuries. Notably, in 1931, salvaged blood from a haemothorax was directly infused back into patients (Davidson & UK Cell Salvage Action Group 2015). This progression culminated in 1943 with the development of the initial cell salvage autotransfusion device by Arnold Griswald (Davidson & UK Cell Salvage Action Group 2015). This device facilitated the collection of suctioned blood in a bottle, subsequent straining through cheesecloth and reintroduction into patients. These foundational principles laid the groundwork for the design of contemporary cell salvage devices. By the 1960s, several commercial devices had become available. The advent of the first ‘modern’ cell saver occurred in the 1970s, however, it was accompanied by various complications including haemolysis, air embolism and coagulopathy (Godfrey 2020).
Principles of ICS
Cell salvage encompasses three distinct phases: collection, washing and re-infusion (Figure 1). The collection of red blood cells (RBCs) from the operative site necessitates the utilisation of a dedicated double-lumen suction device. One lumen extracts blood from the surgical field while the other introduces a predetermined volume of heparinised saline into the salvaged blood (Ashworth & Klein 2010, Klein et al 2018). Following anticoagulation, the blood undergoes filtration and is collected in a reservoir. Component separation is achieved via centrifugation. Subsequently, the RBCs undergo washing and filtration across a semi-permeable membrane, effectively removing free haemoglobin, plasma, platelets, white blood cells and heparin. The salvaged RBCs are then suspended in normal saline, resulting in a haematocrit range of 50%–80%. These salvaged RBCs can be transfused immediately or within a 6-hour timeframe (Allam et al 2008, Amand et al 2002). Although the current standard storage time for cell salvaged blood is 6 hours, a recent prospective study involving 101 paediatric patients undergoing cardiac surgery demonstrated that extending the storage time to 18 hours resulted in minimal microbiological contamination or chemical deterioration (Hishon et al 1995).
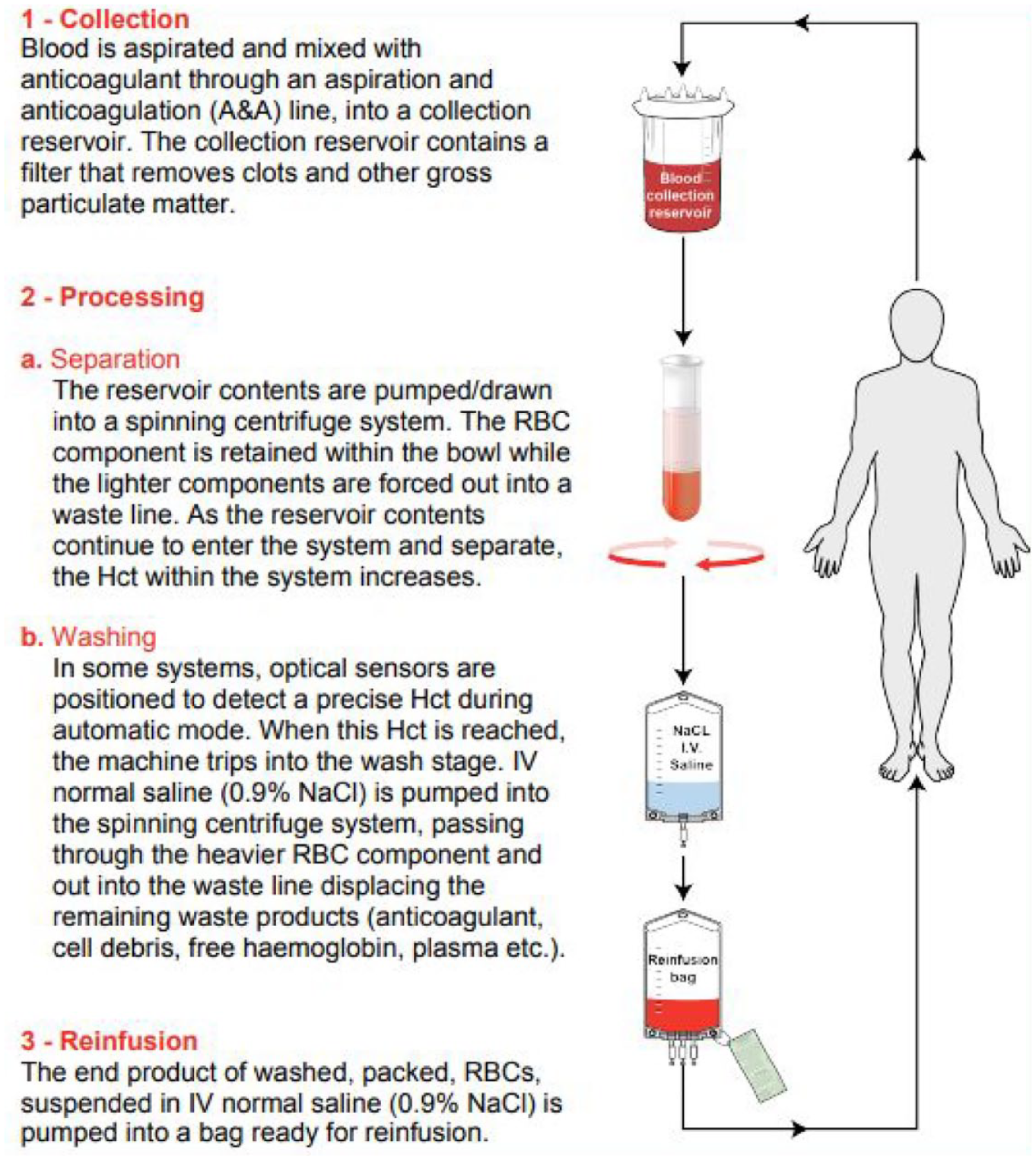
Stages of the ICS process. Image from the UK Cell Salvage Action Group ICS Education Workbook
Advantages of ICS
The benefits associated with ICS pertain to the availability and biochemical properties of donor blood, as well as the potential complications linked to transfusion. One investigation revealed that ICS reduced the reliance on allogeneic blood by 39% and preserved an estimated 0.68 units for every elective adult perioperative patient (Forrest et al 2019). In addition, another study highlighted several advantages of ICS, including the reduction in the necessity for allogeneic blood transfusions, avoidance of restrictive transfusion practices dictated by blood management principles, superior oxygen delivery compared to allogenic blood and mitigation of immune-related adverse effects (Carroll et al 2020, Choi et al 2019). The ICS method facilitates the maintenance of RBCs’ elliptical profiles, elevated concentrations of 2,3-diphosphoglycerate and adenosine triphosphate (ATP) and physiological pH balance, resulting in enhanced oxygen distribution and delivery to tissues (Carroll et al 2020, Roets et al 2019). In contrast, allogeneic blood can induce transfusion reactions, leading to haemolytic reactions and immunosuppression, potentially increasing post-operative infection rates (Klein et al 2018). Autologous blood may serve as a culturally and religiously accepted alternative to donated blood (Murphy & McConnell 2022). Research has also shown that ICS is more cost-effective for health care organisations, particularly when collecting more than one unit of blood (Forrest et al 2019). Moreover, using the patient’s own blood reduces the risk of viral illnesses and maintains potassium levels (Klein et al 2018). In addition, the risk of transfusing incompatible blood types is eliminated with ICS, making it an ideal choice for unforeseen major blood loss situations (Klein et al 2018). Advances in cell salvage technology have resulted in smaller programmable units, with reasonably priced consumables and straightforward instructions for operation (Grace & Lawler 2020). Overall, the benefits of ICS encompass reduced morbidity, improved recovery and earlier mobilisation and discharge.
Disadvantages of ICS
The limitations associated with ICS primarily concern financial aspects and resource allocation, alongside potential procedural complexities (Rawlings et al 2021). Initial setup costs for hospitals procuring a salvage machine can be substantial, compounded by ongoing expenditures for disposables (Miller et al 2022). Furthermore, the perioperative unit must allocate additional resources, not only for training specific nursing staff to operate and supervise the ICS device, but also to ensure comprehensive training and yearly competency assessments (Carroll et al 2020). In addition, processing autologous blood can be slow, which is a critical issue in urgent situations like trauma cases with heavy bleeding and major haemorrhage (Carroll et al 2020).
Although the exact etiology remains uncertain, reinfusion hypotension may manifest in certain instances, possibly attributed to the release of bradykinin and abrupt declines in calcium levels (Carroll et al 2020). Addressing hypotension may necessitate discontinuation of the transfusion and administration of vasopressors (Carroll et al 2020). Other potential complications include haemolysis, haematuria, micro-embolism and the risk of contamination with pharmaceuticals or infectious agents (Choi et al 2019). Furthermore, substances such as alcohol, hydrogen peroxide and specific hypotonic compounds may induce RBC degeneration and breakdown, thus rendering ICS contraindicated under such circumstances (Akonjom et al 2019).
Complications with the utilisation of cell salvage
Complications associated with the utilisation of cell salvage are infrequent, and research has indicated no escalation in complications among patients undergoing cell salvage procedures. Nevertheless, when patients are autotransfused significant volumes, it frequently leads to coagulopathy, as the washing process eliminates all platelets and clotting factors, leaving only the red cells suspended in normal saline (Carless et al 2010). Conducting patient assessments (including thromboelastography), laboratory tests (including prothrombin time, fibrinogen and platelet count), or both, and consider blood product replacement in accordance with local protocols is important in patient care. A randomised trial involving 213 cardiac surgery patients demonstrated no elevation in bleeding or coagulopathy in the group where the volume of blood processed by the cell saver was relatively small (342 [194] ml) (Tachias et al 2022).
Indications and contraindications of cell salvage
Indications and contraindications
ICS presents both indications and contraindications crucial for clinical decision-making. Indications for ICS include cases with anticipated blood loss exceeding 500 ml or 10% of estimated blood volume, especially in patients with low haemoglobin levels or heightened risk factors for bleeding (Lloyd et al 2023). In addition, patients with multiple antibodies or rare blood groups benefit from ICS. For individuals who decline donor blood products due to ethical, religious beliefs or personal choice, ICS becomes a vital option during surgeries where blood loss is expected (Carroll et al 2021). Moreover, in cases of operative massive haemorrhage, ICS should be readily available as standard equipment. However, several contraindications must be considered. These include the absence of trained personnel to collect or process aspirate and patient refusal, which may arise from various factors, including religious beliefs, as seen in some Jehovah’s Witnesses who may have differing views on ICS usage (Klein et al 2019). Some may allow the use of a closed-circuit system, while others may decline blood salvaged from swab washing. Thus, while ICS offers significant benefits in specific scenarios, careful assessment and consideration of both indications and contraindications are imperative for its appropriate application (Reijngoud et al 2009).
Precautions and special considerations
When collecting samples via intracavitary sampling (ICS), it is imperative to refrain from aspirating certain substances, including (Everhart et al 2018):
Antibiotics that are not licenced for intravenous (IV) use
Iodine-based skin preparations
Chlorhexidine
Topical clotting agents
Fibrin-based adhesives
Unset orthopaedic cement.
These substances pose risks such as cardiovascular collapse, haemolysis of RBCs, potential systemic reactions if administered intravenously or are compounds not authorised for parenteral injection. In addition, avoiding aspirating body fluids like urine and heavily contaminated blood with faecal matter prevents complications (Reijngoud et al 2009).
Utilisation of ICS in total hip and knee arthroplasty
The utilisation of ICS in total hip and knee arthroplasty has undergone extensive examination. A study by Forrest et al (2019), conducted in 2019 at a tertiary hospital, indicated that orthopaedic surgery was the specialty most frequently employing ICS, accounting for 22.9% of cases (Forrest et al 2019) Moreover, the National Institute for Health and Care Excellence (NICE) recommends considering ICS in surgeries expected to involve significant bleeding, such as cardiac, open abdominal, complicated urology, obstetric and orthopaedic surgeries (NICE 2015).
In a meta-analysis by Kim et al (2017), it was found that allogeneic blood transfusions may increase the risk of surgical site infections (SSIs). Everhart et al (2018) echoed these findings, noting an elevated risk associated with the transfusion of multiple units of allogeneic blood. Despite the relatively low percentage of patients developing SSIs post-arthroplasty, the frequency of these cases remains notable, underscoring the importance of blood management practices (Kim et al 2017).
An audit conducted by Grace & Lawler (2020) reported promising outcomes associated with ICS usage in orthopaedic surgeries. The study revealed an average return volume of 148 ml in 86 patients who received ICS, with only 6% requiring allogeneic blood transfusion (Grace & Lawler 2020). However, it is essential to note the associated costs, estimated to be approximately £400 per patient for allogeneic blood transfusion alone, excluding ancillary expenses (Grace & Lawler 2020). While the initial setup costs for ICS implementation can be significant, the expense can be mitigated over time through its widespread use (Grace & Lawler 2022).
In a multicentre audit of UK tertiary hospitals, Forrest et al (2019) found orthopaedic surgery to be the leading specialty utilising ICS, followed closely by urology and cardiothoracic surgery. Interestingly, revision total hip arthroplasty (THA) ranked highest among procedures utilising ICS, suggesting significant benefits from its application in such cases (Forrest et al 2019). However, Miller et al (2022) observed that combining ICS with tranexamic acid (TXA) did not yield significant improvements in blood loss or transfusion outcomes compared to TXA alone.
In the context of revision arthroplasty, metal-on-metal hip arthroplasty (MoMHA) revision surgery is performed for adverse reactions to metal debris known as metallosis, in these cases ICS should ne used with careful consideration (Walker et al 2023, Walton et al 2023). Despite this, studies have shown that ICS can be safely utilised in revision surgeries, contributing to reduced rates of allogeneic blood transfusion without an increased risk of reinfection (Walker et al 2023).
A systematic review and meta-analysis of the revision arthroplasty literature identified 283 studies, 11 were included in the review and 9 in the meta-analysis (Walton et al 2023). A notable discrepancy (p < 0.001) in the requirement for allogenic transfusion was observed between groups, with an odds ratio of 0.331 (95% CI: 0.165–0.663) linked to cell salvage utilisation. Among 561 patients undergoing revision hip arthroplasty treated with cell salvage, 247 (44.0%) necessitated allogenic transfusion, compared to 418 out of 643 patients (65.0%) treated without it. For those receiving cell salvage, the average allogenic blood volume required was 1.95 units (390 ml) per patient (0.7 to 4.5 units), versus 3.25 units (650 ml) per patient (1.2–7.0 units) without cell salvage. Moreover, the meta-analysis indicated a significant mean difference of −1.91 units (95% CI −4.0 to 0.2) (p = 0.003). In conclusion, this systematic review underscores a substantial reduction in allogenic blood transfusion necessity with the implementation of cell salvage in patients undergoing revision hip arthroplasty, advocating for its routine adoption in this demographic. Nonetheless, further investigation is warranted to ascertain whether this effect varies across different complexities of revision arthroplasty (Dusik et al 2014, Walton et al 2023).
Training for practitioners
The UK Cell Salvage Action Group has created online tools to support training in cell salvage utilisation. They advocate for competency-based training and education (UK Cell Salvage Action Group). An ‘Intraoperative Cell Salvage Competency (ICS) Assessment Workbook’ is available for download from http://www.transfusionguidelines.org.uk. Manufacturers can provide initial training, which can be arranged during the purchase negotiation phase. Additional training options include in-house sessions, e-learning modules, the ICS workbook or the ICS competency assessment workbook (Grainger et al 2008).
Recommendations for members of the perioperative team
Hospitals undertaking major surgeries are encouraged to assemble a team of blood management champions who can collectively determine and establish a set of protocols for the effective implementation of patient blood management strategies (UK Cell Salvage Action Group).
Carroll & Young (2020) recommend discussing the use of ICS during the WHO surgical team huddle. Therefore, it is suggested that this be included in the set of protocols being developed.
As part of patient blood management strategies, it is advised to review the use of TXA used alongside ICS. Increasing evidence indicates that allogeneic blood transfusion may result in prolonged hospitalisation and significant morbidity in certain patient groups (Akonjom et al 2019).
When using ICS, it is recommended that the scrub practitioner and assistant assist the surgeon to ensure that antibiotics and other haemostatic agents are not suctioned during ICS (Grainger et al 2008).
Carroll and Young also propose prompt reinfusion due to the potential deterioration of rescued oxygen-carrying capacity and deformation of RBCs over time. Therefore, it is recommended to minimise the time between blood removal and reinfusion (Carroll & Young 2020).
It is recommended that only trained personnel operate the ICS machine. An auto-transfusionist, whether an anaesthetist, anaesthetic practitioner, perfusionist or theatre practitioner with appropriate training, should conduct blood collection and recycling using the ICS device (UK Cell Salvage Action Group).
An ongoing training and evaluation programme, alongside continued data gathering and routine reviews, needs to be implemented to ensure the currency of practice, including updated learning about new information and changes to ICS technique (Grainger et al 2008).
Conclusion
While allogeneic blood is indeed crucial, its availability can be limited, particularly in cases of unexpected major blood loss. Despite its benefits, such as its potential to transmit viral illnesses and cause complications like haemolysis and transfusion reactions, there are concerns regarding its accessibility and safety, particularly in arthroplasty procedures. In this context, ICS emerges as a crucial tool in patient blood management, offering potential to enhance patient outcomes. However, the setup costs for ICS can be substantial, encompassing expenses for equipment, consumables and staff training. Nonetheless, financial analyses comparing these upfront costs with potential savings from reduced complications and shorter hospital stays over time suggest that the benefits of ICS outweigh the initial investments. Given the prevalence of knee and hip replacements in the UK ageing population, often with accompanying comorbidities, it becomes imperative for hospitals to adhere to national standards and establish comprehensive patient blood management practices.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.