
Abstract
Introduction:
Barn-integrated operating rooms represent an emerging model in surgical education, offering open-plan layouts designed to enhance efficiency and learning. Despite growing use across United Kingdom centres, limited data exist on their impact on surgical training. This primary aim of this study is to explore the perceived benefits and challenges of barn-integrated operating rooms among orthopaedic surgeons in the context of the multidisciplinary team.
Methods:
A prospective mixed-methods study was conducted using a pilot-tested questionnaire distributed to 93 orthopaedic theatre personnel, including consultant and trainee orthopaedic surgeons, operating department practitioners, and scrub nurses, assessing satisfaction, supervision, and educational value.
Results:
Of 54 respondents (58% response rate), 81.5% preferred barn-integrated operating rooms to conventional theatres. Of the total, 78.3% of surgeons reported visiting adjacent barn-integrated operating rooms theatres for learning, and 67.4% agreed supervision was superior. Thematic analysis revealed improved accountability, communication, and support. Concerns included potential infection risk (33%), radiation exposure (33%), and noise disturbance (46%).
Conclusion:
Barn-integrated operating rooms provide a promising environment for surgical training, promoting supervision, learning frequency, and teamwork. Addressing perceived risks through structured safety protocols will be essential as adoption expands. Further multicentre research is warranted to evaluate long-term outcomes. Findings should be interpreted within the constraint that perspectives were limited predominantly to surgeons.
Introduction
The evolving landscape of surgical education has led to the exploration of alternative models for training environments, including the implementation of barn-integrated operating rooms (BOR). BOR are open-plan surgical facilities, with ultra clean air canopies overlying each operating station (Sykes et al 2024). A barn theatre can be characterised by an open-plan layout without the conventional partition walls or barriers used to separate traditional operating theatres. Each theatre unit in the barn complex has its own specialised air canopy with ultraclean ventilation systems to prevent infection spread (Sykes et al 2024).
The first documented BOR was implemented in the Robert Jones and Agnes Hunt Orthopaedic Hospital and described in 1991 (Donnelly & Greaves 1991). Since then, more hospitals have incorporated this theatre setup across the United Kingdom (UK), with a typical layout illustrated in Figure 1. The use of BOR has subsequently been expanded across multiple surgical units and sub-specialities; however, their use in orthopaedics is predominantly within the elective setting. There is evidence to support that these open theatres are highly effective in reducing the number of airborne bacteria, with no increased risk of deep infection in orthopaedic surgery (Jentzsch et at 2021).
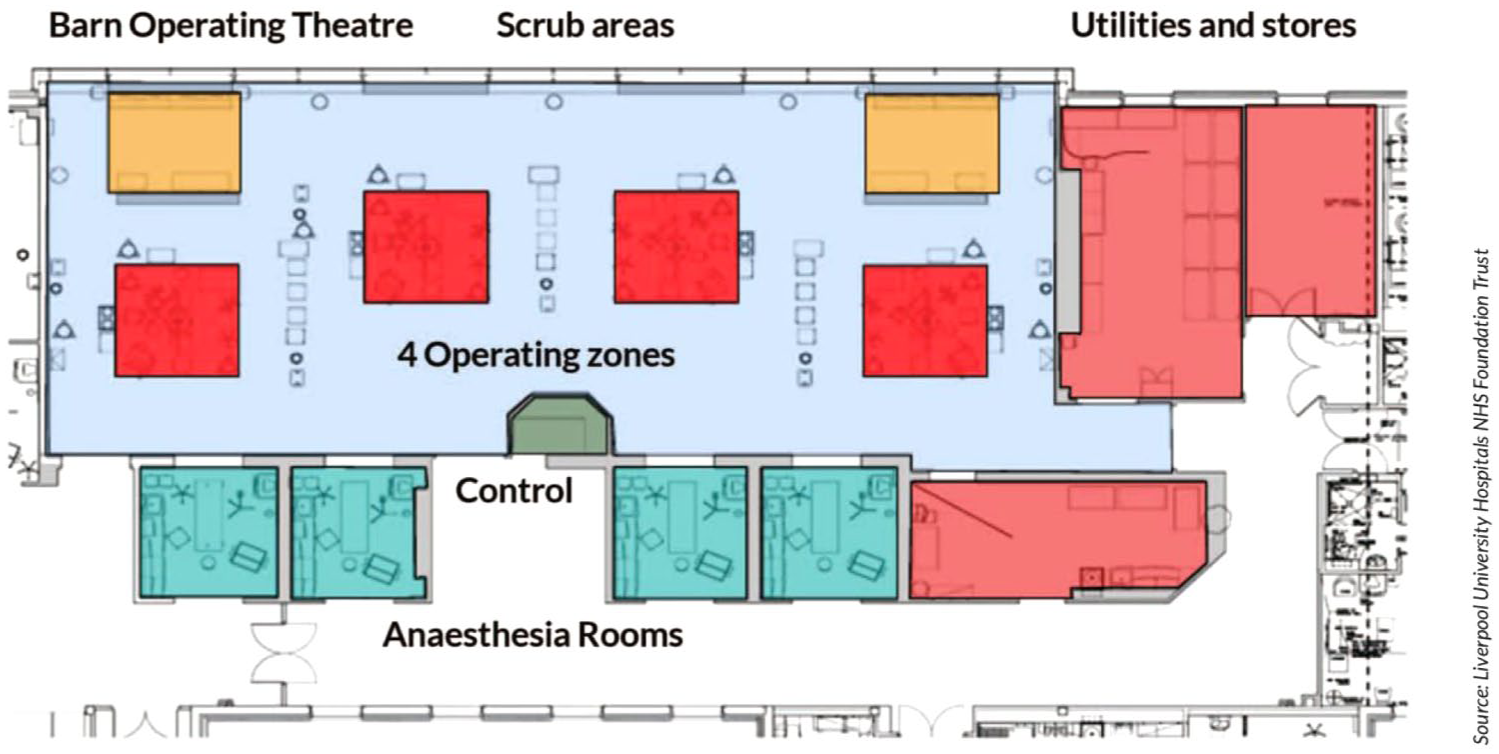
Barn-integrated operating room layout
Reduced theatre efficiency in the aftermath of the COVID-19 pandemic has raised multiple issues for orthopaedic trainees, with attainment of surgical curriculum requirements and reduction in training opportunities representing topical issues at national meetings (Stambough et al 2020). The Get It Right First Time (GIRFT 2022) review suggested that BOR could be used to optimise theatre efficiency, while simultaneously creating an environment for training opportunities, multidisciplinary collaboration, and sharing of best practice.
Despite the huge potential of BOR in orthopaedic training, there is currently no published evidence detailing trainee and wider theatre staff experience within this novel learning environment. This study aims to identify, analyse, and discuss the current concerns, benefits, and training experience of surgeons and theatre staff operating in BOR.
Methods
This is a prospective cohort study, using a mixed qualitative, quantitative questionnaire. Following a literature review, three of the authors established a draft questionnaire (RG, HI, KG) focusing on prevalent issues within orthopaedic training. The content validity was evaluated by the wider authorship group. It was pilot tested with local orthopaedic trainee grade doctors prior to its distribution.
The final questionnaire was disseminated via email to 93 orthopaedic theatre personnel working within a trauma unit. Eligible participants included consultant and trainee orthopaedic surgeons, operating department practitioners (ODPs), and scrub nurses routinely working within the BOR environment. While the primary focus of the questionnaire related to surgical training and supervision, participation was not restricted to surgeons, and responses from perioperative practitioners were included where received. Our unit runs three adjacent trauma theatres per day within the BOR and a separate conventional operating room (COR) list.
Prior experience operating in a COR environment was a prerequisite for inclusion. Supervising surgeons were defined as independently operating associate specialist doctors or consultants.
Baseline demographic data were collected including gender, age, training status, and grade. The survey aimed to gauge the positive and negative aspects of participants’ experience with barn theatre operating, in the context of orthopaedic surgical training and working environment. The data was anonymised, analysed, tabulated, and displayed as proportions of the final results. The questionnaire included ‘free text’ answers, from which the authors derived and collated major paraphrased themes. Reflexive thematic analysis was performed using standardised methodology (Braun & Clarke 2019).
In accordance with the NHS Health Research Authority (HRA 2022) ‘Is My Study Research?’ decision tool, this project was classified as a service evaluation and did not require formal Research Ethics Committee review. As participant eligibility was defined by NHS employment, local governance approval was obtained prior to questionnaire distribution, including departmental permission and registration with the Trust quality improvement framework. All participants were recruited in line with local organisational policy, and responses were anonymised prior to analysis.
Results
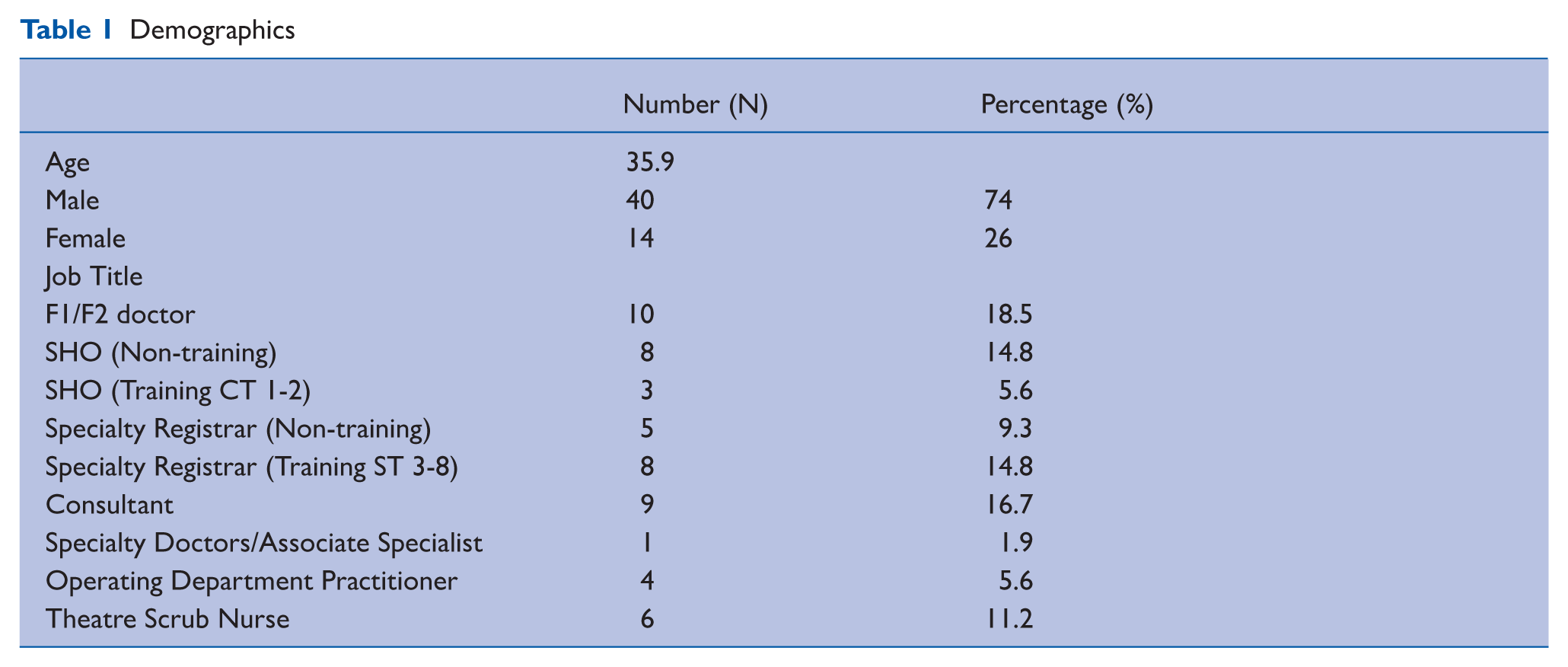
Questionnaires were distributed within the orthopaedic department to 93 personnel. Response rate was 58% (54/93). There were 40 (74%) male and 14 (26%) female participants. Average age of respondents was 35.9 years (range 22–61). Consultants and associate specialists comprised 18.6% (10.54) of respondents. Of the 54 respondents, 44 were consultant or trainee orthopaedic surgeons, and 10 were perioperative practitioners (ODPs or scrub nurses). The distribution of participating operating room personnel is given in Table 1.
Demographics
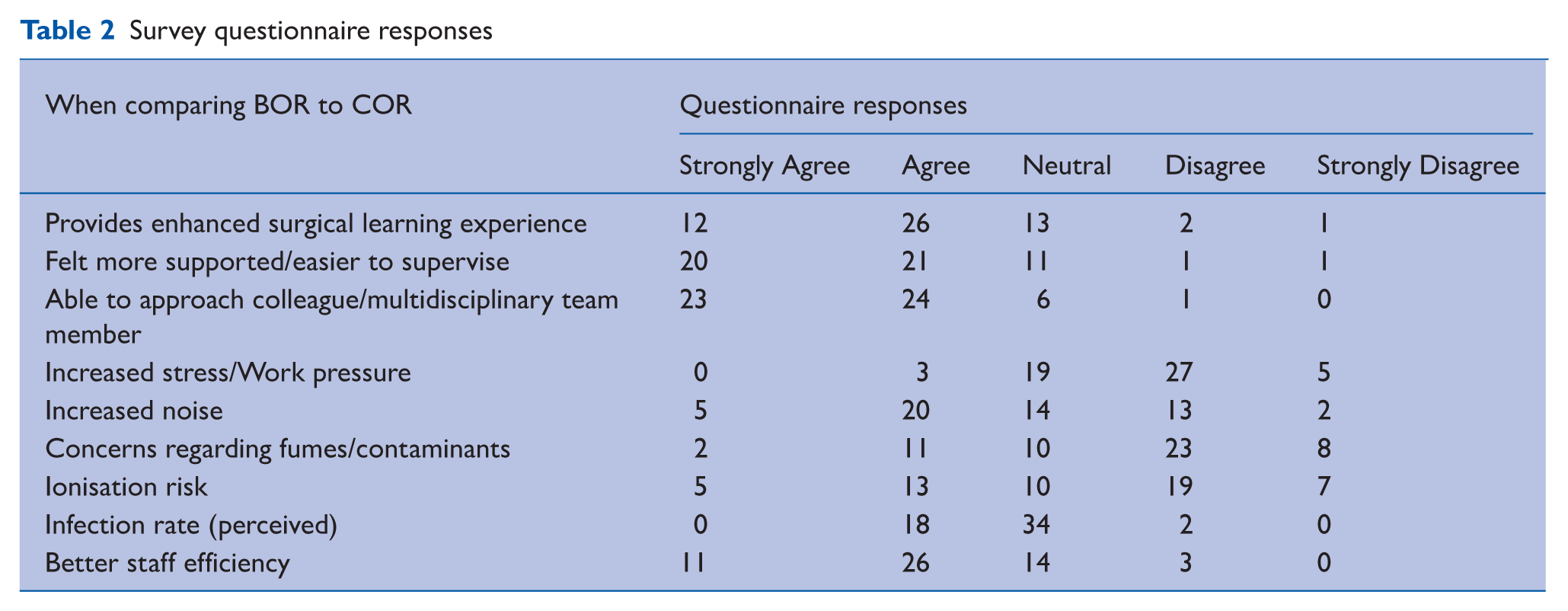
Seventy percent (n = 38) of the respondents reported BOR provided an enhanced surgical learning experience compared to COR, while 24% (n = 13) had an equivocal opinion, with only 6% (n = 3) preferring COR. Seventy-six percent (n = 41) reported they felt easier to supervise/felt better supervised in BOR, while 20% (n = 11) were neutral about this question, with 4% (n = 2) felt COR were better in this regard.
Sixty-seven percent (n = 36) of respondents had crossed between one and three times to a neighbouring theatre for a learning opportunity, while 13% (n = 7) took four or more such trips. In terms of being able to approach a colleague for advice and communication among multidisciplinary team members, 87% (n = 47) preferred BOR, with 11% (n = 6) being neutral and 2% (n = 1) preferring COR.
Regarding stress and work pressure, only 6% (n = 3) felt BOR was a higher stress environment, with 35% (n = 19) feeling comparable amounts of stress in both, while 59% felt working in COR was more stressful than BOR. Forty-six percent (n = 25) reported higher noise in BOR, with 24% (n = 13) of respondents feeling there was higher exposure to fumes and contaminants from neighbouring rooms in the BOR. Over 33% of respondents felt there was a higher risk of ionising radiation and infection rate while working in BOR.
Two thirds (69%) of the respondents felt staff efficiency was better in BOR, with 82% of staff preferring to work in this theatre setting. The questionnaire responses are given in Table 2.
Survey questionnaire responses
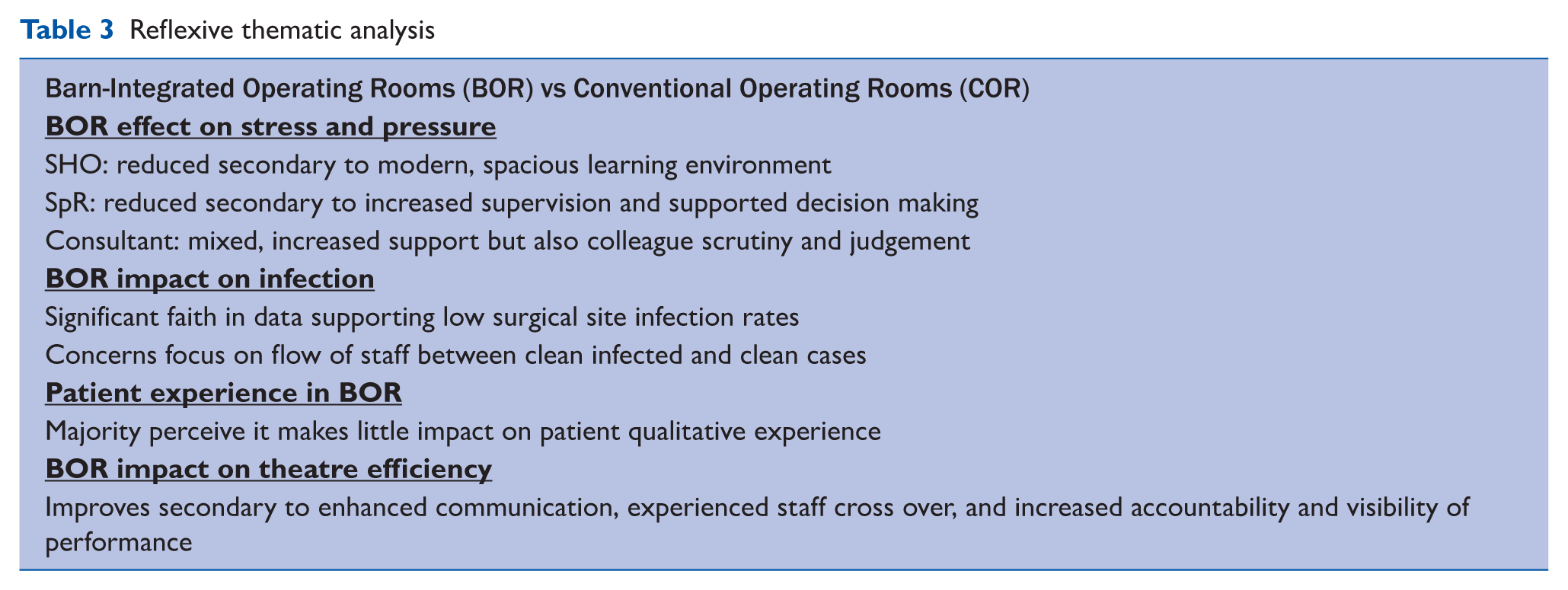
Reflexive thematic analysis was performed for the subjective responses, and these are delineated in Table 3.
Reflexive thematic analysis
Discussion
To our knowledge, this article presents the only currently available data analysing the perspectives of orthopaedic trainees, trainers, and operating room personnel working in a BOR setting. Our study demonstrates the potential for BOR as an enhanced surgical learning environment for orthopaedic trainees, with widespread preference for this model among all staff groups involved.
Although surgeons comprised the majority of respondents, this study also included perspectives from perioperative practitioners, specifically ODPs and scrub nurses. These staff groups play a critical role in theatre workflow, environmental control, and non-technical performance within BOR settings. However, representation across the MDT was uneven, with anaesthetists, radiographers, and recovery staff perspectives not captured. Consequently, the findings should be interpreted as reflecting predominantly surgical and selected perioperative viewpoints rather than a comprehensive MDT evaluation.
Evidence from the literature indicates that operating models comparable to BOR are associated with markedly reduced mean operative times while maintaining similar complication rates for elective orthopaedic procedures (Waly et al 2020). Such efficiencies could contribute to addressing the substantial elective backlog that has persisted since the COVID-19 pandemic (UK Parliament 2021).
Post-COVID health care constraints have fundamentally altered how surgical trainees gain operative experience. The pandemic led to reduced case volumes and fewer training opportunities, negatively impacting progression and skill acquisition. The BOR model offers a means to counteract this by increasing the frequency of both observed and assisted procedures. The authors conclude that the BOR removes barriers to progressive, graduated responsibility, providing an ideal environment for indirect supervision, especially for senior trainees with evolving autonomy.
Several United Kingdom (UK) centres have already adopted the Barn-Integrated Operating Room model, including Chase Farm Hospital (London), Wrightington Hospital (Lancashire), Broadgreen Hospital (Liverpool), Salford Royal Hospital, and the Royal Orthopaedic Hospital (Birmingham) (Buildingbetterhealthcare.com 2024). Data from Broadgreen suggest that infection control rates have improved, accompanied by positive behavioural changes within the theatre environment. In line with Get It Right First Time (GIRFT) recommendations (2022), an increasing number of NHS trusts are now considering transitioning to BOR configurations to help address the elective orthopaedic backlog (Buildingbetterhealthcare.com 2024).
The study findings indicate that BORs are perceived as an optimal environment for both teaching and supervision, benefitting learners and educators alike. A systematic review of 23 studies has shown that insufficient mentorship in orthopaedic training detrimentally affects the overall educational experience (Enson et al 2022). The BOR model may address this issue through an open operating room configuration, enabling senior surgeons to move between adjacent theatres to provide real-time oversight and guidance to multiple trainees, thereby enhancing the quality and consistency of mentorship. While most respondents in this study were surgeons and surgical-grade theatre personnel, BOR workflows also involve anaesthetic teams, scrub and circulating practitioners, radiographers, and recovery staff. Their roles influence team communication, environmental control, and non-technical performance within BOR. The absence of their perspectives limits the completeness of MDT interpretation in this study.
Although respondents expressed concern about potential infection risks within the BOR environment, existing evidence indicates that infection rates are not directly linked to the number of personnel present in the operating theatre (Montiel et al 2021). Instead, they are more strongly influenced by behavioural and environmental factors, such as staff movement patterns, door-opening frequency, and overall theatre traffic (DiBartola et al 2019, Humphreys et al 2023). These factors can disrupt ultraclean airflow and increase the risk of airborne contamination. Consequently, infection prevention in BORs should prioritise behavioural discipline, strict adherence to aseptic protocols, and minimisation of unnecessary movement between stations. The authors theorise that with appropriate workflow management and staff education, the open-plan BOR model can maintain infection risk levels comparable to conventional theatre setups.
The non-technical skills highlighted, including communication, situational awareness, and teamwork, are shared across the entire theatre team. Because this study captured only surgical viewpoints, it cannot establish how BOR affects these competencies for non-surgical MDT members. Therefore, this should be viewed as a first step in wider BOR analysis, requiring future inclusion of perioperative practitioners.
Noise pollution, surgical smoke, and ionising radiation exposure represent key occupational hazards that must be carefully managed if BORs are to be widely adopted as future theatre models. The survey highlighted staff concerns regarding these environmental factors, reflecting well-documented issues within orthopaedic practice. Studies have demonstrated that persistent noise exposure in operating theatres can contribute to distraction, communication difficulties, and even permanent noise-induced hearing loss (NIHL) among staff (Jeyaraman et al 2024). Similarly, elevated exposure to surgical fumes in open-plan settings may increase inhalation risk, though this can be mitigated through the installation of physical partitions or optimised air filtration systems at supply inlets (Cheng et al 2023).
Radiation exposure in BORs is likely to remain comparable to that in conventional theatres, provided the principles of ALARA: time, distance, and shielding, are rigorously followed. However, evidence suggests that radiation safety awareness remains suboptimal within orthopaedics, with only 19% of surgeons in a national study reporting adequate formal training (Raza et al 2021). As BOR configurations involve greater staff mobility and inter-theatre crossover, structured radiation safety education and regular dosimetry monitoring should be integral to local governance to minimise occupational exposure.
The most significant limitation of this study is that it captures surgeon centric perspective on the BOR, under-representing perioperative practitioners who form a major part of the operating theatre MDT. Wider MDT perspectives remain essential to understanding how BOR affects the full perioperative pathway. Participation was voluntary, introducing the possibility of selection bias and reducing representativeness of the wider orthopaedic theatre workforce. Consequently, the external validity of these findings, particularly when extrapolated to the broader population of orthopaedic trainees, may be limited. In addition, while the questionnaire provided valuable insights into training experiences, its categorical design may have oversimplified the complex range of factors influencing educational quality and professional development.
Future research should employ multicentre recruitment across institutions using BOR models, while also focusing on perioperative practitioner perspectives to complement these findings. Such an approach would enhance the reliability and generalisability of findings, allowing more robust evaluation of the BOR’s impact on surgical training, supervision quality, and theatre efficiency.
Conclusion
These findings indicate that the Barn-Integrated Operating Room model has considerable potential as an addition to surgical training curricula, fostering both technical proficiency and non-technical competencies such as communication, teamwork, and situational awareness. Future studies incorporating larger sample sizes, multicentre participation, and longitudinal follow-up will be essential to determine the long-term sustainability, educational value, and overall impact of BOR on surgical trainee performance and patient outcomes. These conclusions should be viewed considering the limited respondent group, and future work must integrate the perspectives of perioperative practitioners to establish the wider MDT impact of BOR.
Implications for practice
BOR may enhance supervision, communication, and team dynamics in the perioperative environment.
Structured use of BOR could improve trainee learning encounter frequency and confidence.
The MDT implications of BOR cannot be fully interpreted from this dataset, and future evaluations must include perioperative practitioner perspectives.
Noise, infection, and radiation risks must be addressed with local safety governance.
Supplemental Material
sj-docx-1-ppj-10.1177_17504589261421002 – Supplemental material for Barn theatres: A novel learning environment for orthopaedic surgeons
Supplemental material, sj-docx-1-ppj-10.1177_17504589261421002 for Barn theatres: A novel learning environment for orthopaedic surgeons by Richard Galloway, Hassan Imtiaz, Louise Nordin, Michael Kent and Kieran Gallagher in Journal of Perioperative Practice
Footnotes
Acknowledgements
The authors would like to thank the theatre and perioperative teams at University Hospital Dorset for their assistance in the data-collection process and for their commitment to surgical education and innovation.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. The data are anonymised and stored securely in accordance with institutional governance policy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
Formal ethical approval was not required, as confirmed by the NHS Health Research Authority online decision tool. Participation was voluntary, and all respondents provided informed consent when completing the anonymous questionnaire.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.