
Abstract
Atrial myxomas are uncommon primary cardiac tumours, often detected incidentally. Their presence poses significant anaesthetic challenges during non-cardiac surgeries, especially emergencies, due to the risk of obstructive haemodynamics and embolic phenomena. We report the successful perioperative management of a 69-year-old male with an incidentally diagnosed left atrial myxoma posted for emergency orthopaedic surgery following trauma. With meticulous planning, vigilant monitoring, and tailored anaesthetic strategies focusing on preload optimisation and rhythm stability, the surgery was completed uneventfully. This case highlights key perioperative considerations for clinicians managing similar high-risk patients.
Keywords
Introduction
Primary cardiac tumours are rare, with a reported incidence of <0.3% at autopsy, among which atrial myxomas constitute nearly 50%–75% (Pinede et al 2001, Reynen 1995). These benign neoplasms commonly arise from the left atrium – typically the interatrial septum near the fossa ovalis (Keeling et al 2002). Their clinical manifestations range from being completely asymptomatic to causing life-threatening complications. The classical diagnostic description – Goodwin’s triad – includes embolic symptoms, intracardiac flow obstruction, and constitutional symptoms (fever, weight loss, fatigue) (Goodwin 1963).
Atrial myxomas can produce dynamic obstruction of the mitral valve orifice depending on body position, thereby causing syncopal episodes, pulmonary hypertension, or sudden haemodynamic collapse (Goswami et al 2004). In addition, friability of the tumour may predispose to systemic embolisation, including cerebrovascular events (Reynen 1995).
Anaesthetic management becomes particularly challenging when such a patient presents for emergency non-cardiac surgery, where delay for definitive cardiac surgery is not an option. Minor fluctuations in heart rate, rhythm, or preload can precipitate catastrophic obstruction or acute heart failure. Maintaining haemodynamic stability, sinus rhythm, and adequate preload are essential goals (Raja et al 2004, Serrano et al 2007).
Comorbidities such as atrial fibrillation and diabetes, along with emergency trauma-related factors (pain, blood loss, hypovolaemia), magnify perioperative risk. In these situations, a multidisciplinary approach involving cardiology and cardiothoracic surgical backup is strongly recommended (Gupta et al 2011).
This case report describes the comprehensive and successful anaesthetic management of a trauma patient with an incidentally detected left atrial myxoma, undergoing urgent wound debridement and orthopaedic fixation. The clinical course underscores vital considerations for safe anaesthesia in patients with intracardiac tumours. Written informed consent for the publication of the patient’s clinical details and images was obtained.
Case presentation
A 69-year-old male with known hypertension and type 2 diabetes mellitus presented to the emergency department following a road traffic accident, sustaining a fracture of the right tibia requiring emergency intervention. He also had a history of paroxysmal atrial fibrillation without ongoing treatment. He was posted for emergency wound debridement of the right upper limb with external fixator application for the right tibia.
On preoperative evaluation, transthoracic echocardiography (TTE) incidentally revealed a left atrial myxoma measuring 1.3 × 2.0 cm (Figure 1), arising from the interatrial septum, with normal ejection fraction (60%), concentric left ventricular hypertrophy, and Grade I diastolic dysfunction. No signs of mitral valve obstruction or embolism were observed. Considering the emergency nature of the surgery, the cardiology and cardiothoracic surgical teams were kept on standby. Antiarrhythmic agents and a defibrillator were prepared. The patient was categorised as American Society of Anesthesiologists (ASA) III (E).
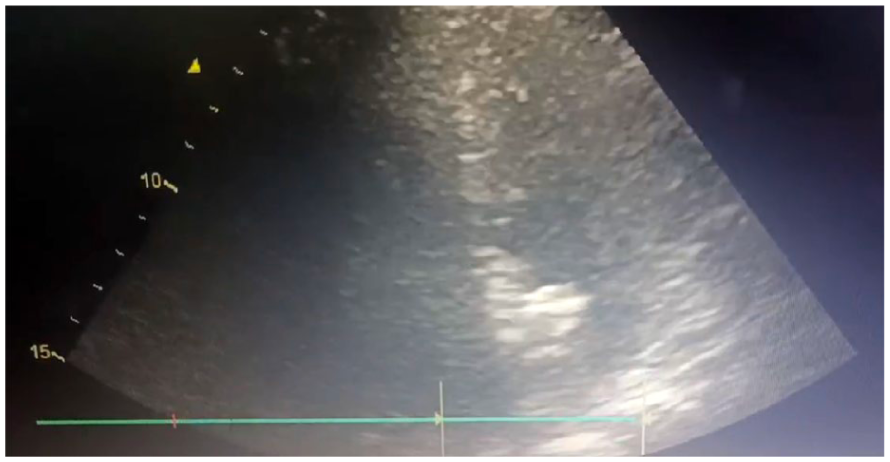
Transthoracic echocardiography showing left atrial myxoma
Standard monitors were applied, along with invasive arterial pressure monitoring, pulse pressure variation monitoring, bispectral index (BIS) monitoring, neuromuscular monitoring, and serial arterial blood gas analysis. The main anaesthetic goals were to avoid tachycardia and arrhythmias, maintain adequate preload and afterload, and avoid hypotension that may reduce coronary perfusion.
The patient was induced with intravenous (IV) fentanyl 2 mcg/kg, IV etomidate 0.3 mg/kg, and IV vecuronium 0.1 mg/kg. IV esmolol 0.5 mg/kg was administered 90 seconds prior to intubation. The patient was intubated with an 8-mm endotracheal tube fixed at 22 cm with controlled ventilation. Maintenance was achieved using sevoflurane with supplemental fentanyl. Mechanical ventilation ensured normocapnia and adequate oxygenation. Goal-directed fluid therapy was administered to maintain preload carefully without causing volume overload.
Intraoperatively, the patient developed intermittent episodes of hypotension, which were promptly managed with phenylephrine boluses and fluid adjustments. No arrhythmias or embolic manifestations occurred. Before extubation, IV esmolol 0.5 mg/kg was administered to prevent a sympathetic surge. The patient was extubated uneventfully and transferred to the PACU with stable vital signs.
Postoperative pain control was maintained using a buprenorphine transdermal patch, ensuring minimal haemodynamic fluctuation. Anticoagulation and beta-blockers were resumed postoperatively.
He recovered well without any postoperative complications and was referred to cardiothoracic surgery for definitive tumour excision.
Discussion
This case highlights critical perioperative concerns associated with atrial myxoma and the safe execution of emergency non-cardiac surgery when deferral for tumour resection is not feasible. The main clinical dangers include mitral valve obstruction, which may lead to reduced cardiac output and pulmonary oedema, risk of embolisation leading to stroke, myocardial infarction, limb ischaemia, and arrhythmias, especially atrial fibrillation (Goswami et al 2004, Reynen 1995).
Our patient exhibited Goodwin’s triad features only partially, with atrial fibrillation and diastolic dysfunction being relevant risks. TTE was performed as part of the preoperative assessment by the cardiologist due to the patient’s history of untreated paroxysmal atrial fibrillation. Current guidelines recommend cardiac evaluation in patients with arrhythmias to assess structural abnormalities, thromboembolic risk, and ventricular function (Fleisher et al 2022, Hindricks et al 2020). TTE serves as a non-invasive and readily available modality for detecting intracardiac masses, valvular pathology, and ventricular function, which are essential for perioperative risk stratification (Joglar et al 2024). The primary anaesthetic goal was to maintain adequate preload, which was achieved through careful goal-directed fluid administration. To preserve afterload and prevent sudden drops in systemic vascular resistance, phenylephrine was used as the vasopressor of choice during hypotensive episodes. Avoidance of tachycardia was crucial to prevent dynamic obstruction and was ensured using esmolol during both induction and emergence (Fleisher et al 2022). Efforts were also directed towards maintaining sinus rhythm, with antiarrhythmic drugs kept on standby for immediate intervention if required. The risk of embolisation was minimised by employing gentle ventilation techniques and maintaining stable haemodynamics throughout the procedure. In addition, adequate oxygenation and ventilation were ensured by serial arterial blood gas monitoring to detect and correct hypoxia or hypercarbia. Etomidate is associated with minimal cardiovascular depression compared to other induction agents, making it suitable for haemodynamically unstable patients (Forman 2011). Phenylephrine boluses were appropriately selected because tachycardia-inducing vasopressors, such as ephedrine and dopamine, may exacerbate dynamic obstruction (Gupta et al 2011, Serrano et al 2007). Continuous invasive monitoring with real-time perfusion indices ensured early recognition of preload-sensitive hypotension.
Cardiac team and resuscitation support availability enhanced the safety margin – particularly if acute obstruction had occurred. Although intraoperative transoesophageal echocardiography (TOE) is highly beneficial in patients with atrial myxomas due to its ability to provide continuous real-time assessment of tumour mobility, ventricular filling, mitral inflow, and abrupt haemodynamic deterioration, it was not utilised in this case (Practice Guidelines for Perioperative Transoesophageal Echocardiography 2010, Shah et al 2010). The decision was based on financial constraints and the emergency nature of the procedure, coupled with stable preoperative TTE findings. Postoperative analgesia minimised sympathetic surges, a crucial factor in preventing tachyarrhythmias and hypertension-mediated obstruction.
Conclusion
Patients with atrial myxomas pose significant haemodynamic challenges to the anaesthetists, especially during emergency non-cardiac surgeries. Incidentally discovered myxomas should not delay life-saving interventions when appropriate risk-mitigation strategies are implemented. Individualised anaesthetic planning focused on preload maintenance, rhythm control, and avoiding tachycardia or hypotension is key to preventing acute intracardiac obstruction and embolic events. This case reaffirms that multidisciplinary coordination, vigilant monitoring, and the use of cardiovascular stable anaesthetic agents ensure safe perioperative outcomes. Further reports and guidelines are needed to standardise anaesthetic management for such rare scenarios.
Footnotes
Acknowledgements
The authors would like to thank their colleagues in the Department of Anesthesiology at Sri Ramachandra Medical College and Research Institute (SRIHER), for their support and encouragement.
Authors’ note
The authors report that the material in this manuscript was not presented at any meeting or conference.
Author contribution
All authors contributed to the conceptualisation; helped with data collection and analysis plan; helped in the interpretation of the data and drafting of the paper; reviewed the article for important intellectual content; approved the final article version to be published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not required for anonymised single-patient case report.
Informed consent
Obtained.