
Abstract
The wide-awake hand surgery (WAHS) technique involves injecting lidocaine with adrenaline for hand surgical procedures that are done without the use of tourniquets, sedation, regional or general anaesthetic. This is a retrospective review of the first 100 consecutive patients who underwent operations using this technique at our centre. The operations included carpal and cubital tunnel decompression, trapeziectomy, tendon transfer, and tenolysis. A questionnaire adapted from Lalonde’s previous work on wide-awake surgery was used to assess patients’ experiences. Sixty-five percent of the patients responded to the postal questionnaire, the majority reporting a high satisfaction level. Ninety-one percent of responders reported that the operation was less painful or comparable with a procedure at the dentist; 86% would prefer to be wide-awake if they needed to have hand surgery again, and 90% stated they would recommend WAHS to a friend.
Keywords
Introduction
The wide-awake hand surgery (WAHS) technique was first introduced by Lalonde in 2007 (Bezuhly et al., 2007) and is characterized by the following features: use of local anaesthetic with adrenaline into the operative field including digits; use of larger volumes of local anaesthetic to achieve a tumescent effect; avoidance of regional anaesthesia, general anaesthesia, sedation, or use of a tourniquet; intraoperative involvement of the physiotherapist to assess range of movement.
There are advantages to this technique: it eliminates the risks associated with general or regional anaesthesia and also the discomfort associated with tourniquets. Patients who would have otherwise been denied surgery because of comorbidities can have an operation. Finally, potential cost savings can be achieved by providing a day-case service without the need for anaesthetists, pre-assessment visits, and pre-operative investigations (Bismil et al., 2012; Lalonde, 2011; Nelson et al., 2009).
The birth of WAHS followed a reassessment of the safety consideration of local anaesthesia with adrenaline in digital surgery and also the introduction of clear guidelines to treat digital ischaemia (Chowdhry et al., 2010; Denkler, 2001; Fitzcharles-Bowe et al., 2007; Lalonde et al., 2005; Mustoe et al., 2010; Nodwell and Lalonde, 2003). Strict contraindications against the use of adrenaline in finger blocks stem from reports of digital gangrene; to date there have been 48 reported cases. On closer examination however, all of these cases involved the use of cocaine or procaine with or without adrenaline (Denkler, 2001). There have been no reports of digital gangrene using commercial lidocaine with adrenaline since its introduction in 1948. Not only is adrenaline safe in the hand and digits, it allows for adequate haemostasis without the use of a tourniquet (Thomson and Lalonde, 2006; Thomson et al., 2007).
With WAHS, tourniquet time is no longer a determining factor of whether a procedure requires a local or general anaesthetic. In addition, a non-sedated, comfortable patient is able to cooperate with the surgeon, allowing the operator to perform a real-time, dynamic assessment of hand function during the operation itself. This is particularly beneficial in surgery for fracture fixation, joint fusions, tendon repairs, tendon transfers, and tenolysis (Higgins et al., 2010; Lalonde, 2009). Operative findings can be discussed with the unsedated awake patient and post-operative instructions delivered and emphasized towards the end of the procedure.
The aim of this study was to assess the outcome after the introduction of WAHS in a UK hand centre. We focused on surgery-related outcomes and patient satisfaction. The surgical factors assessed were the feasibility of this technique, conversion rates from WAHS to tradition anaesthetic techniques, and complication rates. Patient satisfaction and experience were evaluated by questionnaire.
Methods
WAHS has been used in our department since 2009. After counselling, the option of WAHS was offered to all suitable hand surgical patients seen by the senior author (JGM) either in the clinic or presenting acutely. Patients deemed unsuitable were those with potential vascular compromise or those who had specifically declined any procedures under local anaesthetic.
Our method of WAHS is a slight modification of the technique described by Lalonde (Mustoe et al., 2010). All procedures are carried out with an infiltration of 1% lidocaine with 1:200 000 adrenaline. Sodium bicarbonate (8.4%) is added to comprise one-tenth of the volume. This buffers the acidic local anaesthetic solution to make it work faster and causes less pain (Davies 2003; McKay et al., 1987). In addition, hyaluronidase is added (to make up a dilution of 50 IU/ml) to facilitate tissue spread (Nevarre and Tzarnas, 1998). Cold ethyl chloride spray is used to minimize the initial pain from the needle piercing the skin (Selby and Bowles, 1995).
For procedures on the digits, 2–5 ml of infiltrate is used. For more proximal procedures involving the wrist or forearm, larger volumes are necessary. Volumes of 30 ml are recommended for the wrist and hand, and up to 200 ml for the forearm. For procedures involving the joint and bones, we inject into the joint capsule as well as the soft tissues around the joint. If the procedure involves significant manipulation of bones, for example in joint replacement, we inject into the medullary canal intra-operatively. The concentration of lidocaine is diluted if very large volumes are required, bearing in mind the maximum recommended dose of 7 mg/kg of body weight. A minimum of 20 minutes is required to allow for maximal anaesthesia and haemostasis.
Data from the first 100 consecutive patients who underwent hand surgery using the WAHS were assessed using a newly developed 19 question survey adapted from Lalonde’s previous work (with permission). The questions concentrated on four main areas: the patient pathway, pain, anxiety, and overall WAHS experience. Eighteen questions were provided in options available for the patient to circle or tick, and one question provided a line to be filled in about analgesia taken post-operatively for pain. The questionnaires were posted to the 100 consecutive patients at a minimum of 3 (range 3–22) months after surgery. Ethical approval was granted by the local audit/ethics committee.
In addition to analysis of the responses in general, we were also keen to find out if the period of time between surgery and answering the questionnaires had any bearings on the outcomes, particularly relating to memory of the experience, pain, and anxiety levels. Patients were grouped into two categories: those who replied to the questionnaire 3–12 months after surgery were placed in the ‘early’ category, and those who replied 13–22 months after surgery were placed in the ‘late’ category.
Finally, we wanted to assess the effect of different procedures on patients’ responses. Procedures involving bones and joints (Darrach’s procedure, trapeziectomy, joint replacement, excision of bony lesions, and K-wire fixation) were grouped together, and procedures involving soft tissues only (carpal tunnel decompression, cubital tunnel decompression, excision of soft tissue lesion, Dupuytren’s fasciectomy, tendon surgery, nerve transfer, and soft tissue trauma) were placed in another group.
Responses from the late group were compared with the early group, and responses from the ‘bone/joints’ group were compared with the ‘soft tissue’ group. Categorical data were analyzed using Fisher’s exact test, and continuous data were analyzed using an unpaired Student’s t-test.
Results
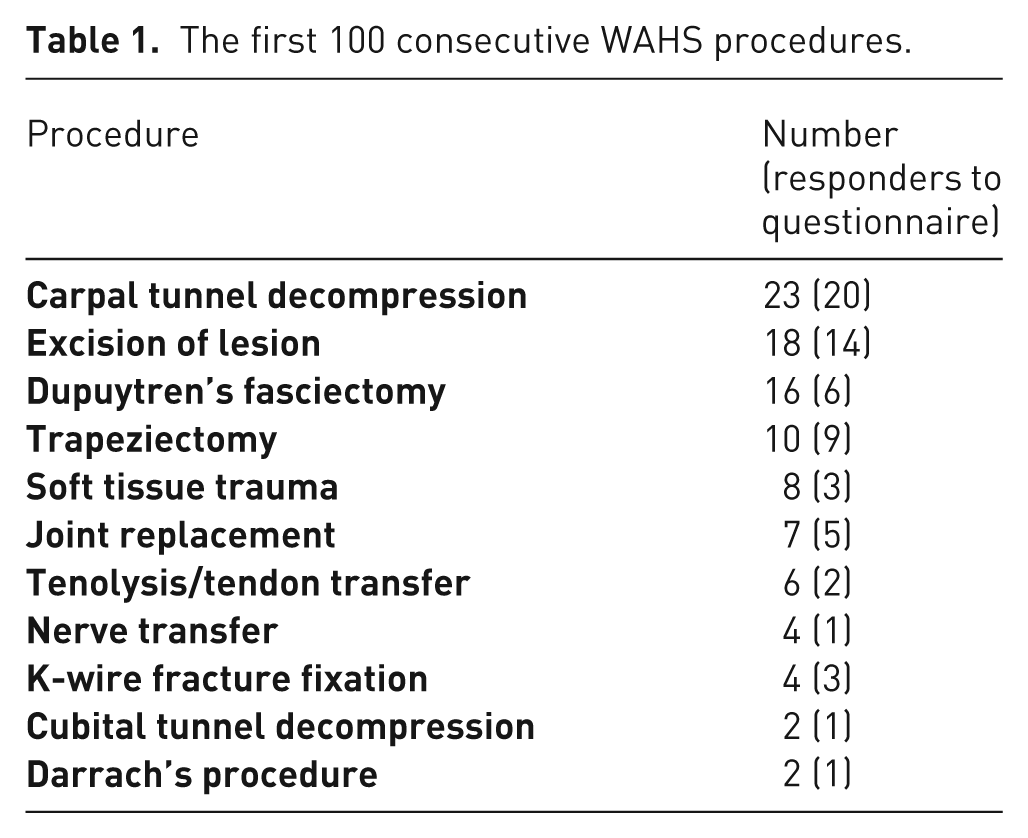
Fifty-two patients were female and 48 male with a mean age of 55 (range 19–83) years. The case mix for the 100 procedures included 91 elective and nine trauma cases. Sixty-five patients responded to the questionnaire, and the number of responders per procedure is shown in Table 1.
The first 100 consecutive WAHS procedures.
Patient pathway
Sixty-two percent of respondents did not need any pre-operative assessment visits before the day of surgery, while the rest (38%) had one or more pre-operative visits.
Ninety-seven percent of patients felt they were given sufficient information about the WAHS procedure. The remainder left this question unanswered. Eighty-eight percent felt they were given sufficient information about options other than WAHS. Eleven percent felt they were not given sufficient information about other options, and one patient left this question blank.
Pain
Patients were asked to rate the level of pain experienced at three stages: during the injection of local anaesthetic, during the operation, and their worst pain experienced after surgery, with 0 being no pain and 10 being the worst pain imaginable. Eighty-seven percent reported a pain score of 5 or less during the injection of local anaesthetic. The pain scores during injection of local anaesthetic are shown in Figure 1. Sixty-eight percent reported a pain score of 0 during their WAHS operation (Figure 2). There was a wide range of reported pain levels for the worst pain experienced after surgery shown in Figure 3. Patients were asked about what analgesia they took post-operatively. Twenty percent did not require any post-operative analgesia (Table 2).
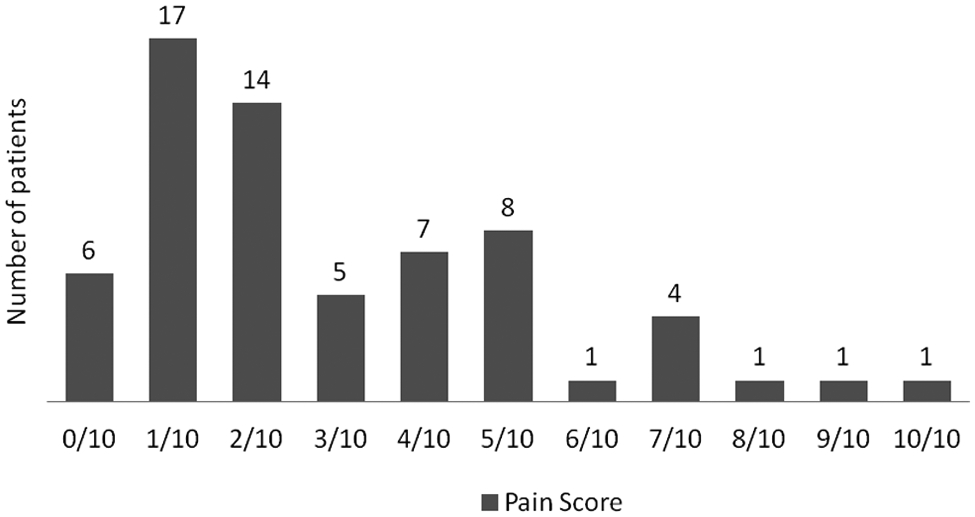
Pain scores during injection of local anaesthetic.
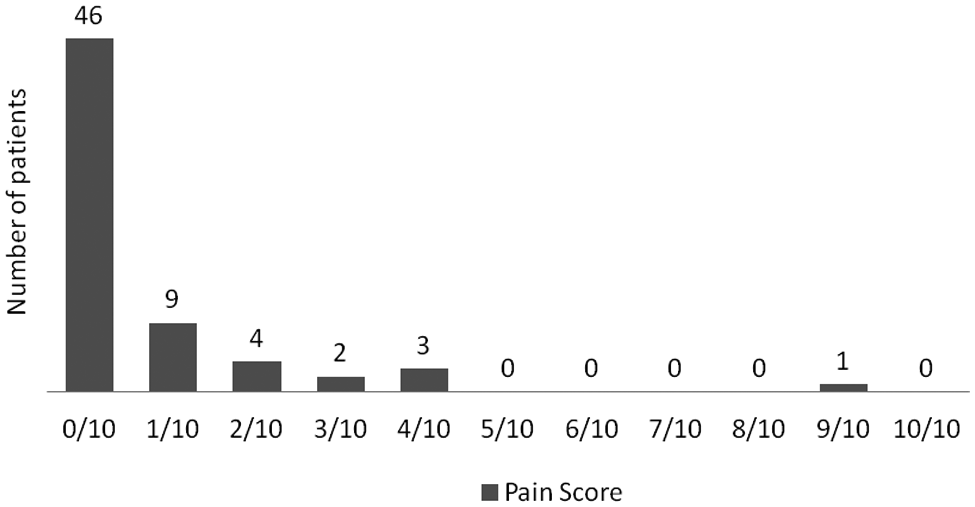
Pain scores during WAHS.
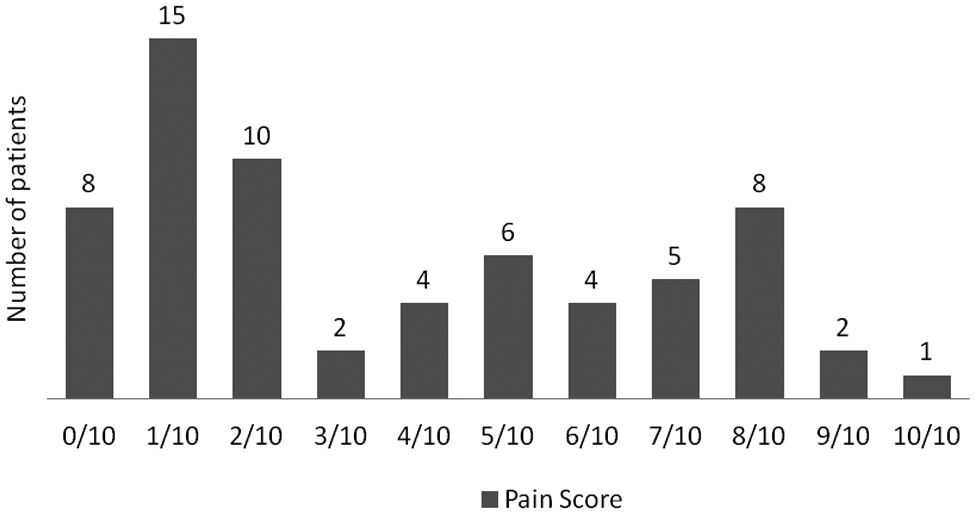
Worst pain reported after WAHS.
Analgesia taken after WAHS by responders to questionnaire.
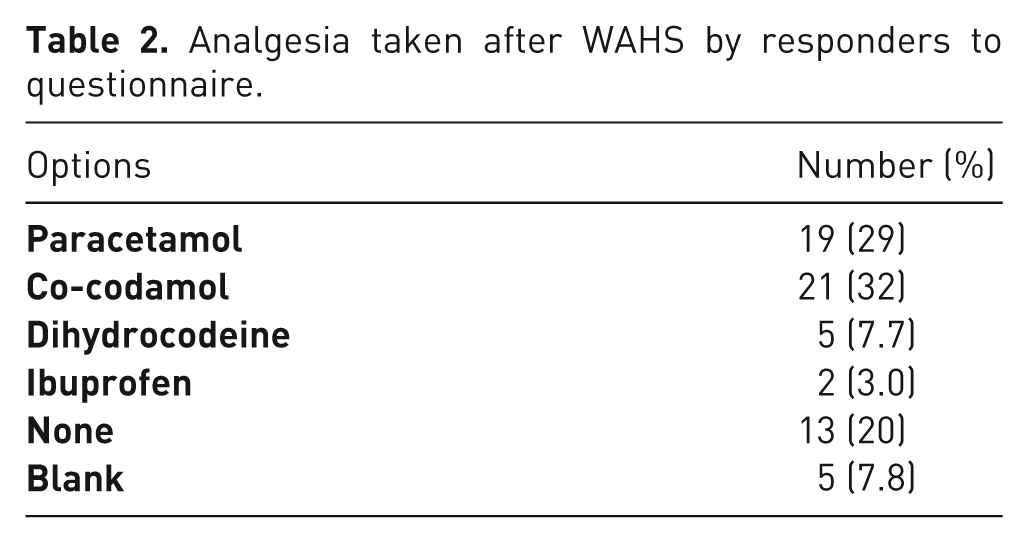
Sixty-six percent of patients felt that their analgesic medications were good enough to handle their pain satisfactorily, 7.7% felt their analgesics were not strong enough, and 6.2% left this question blank. Seventy-six percent of patients stated that the hand was numb/pain-free for at least 3 hours post-operatively (Figure 4).
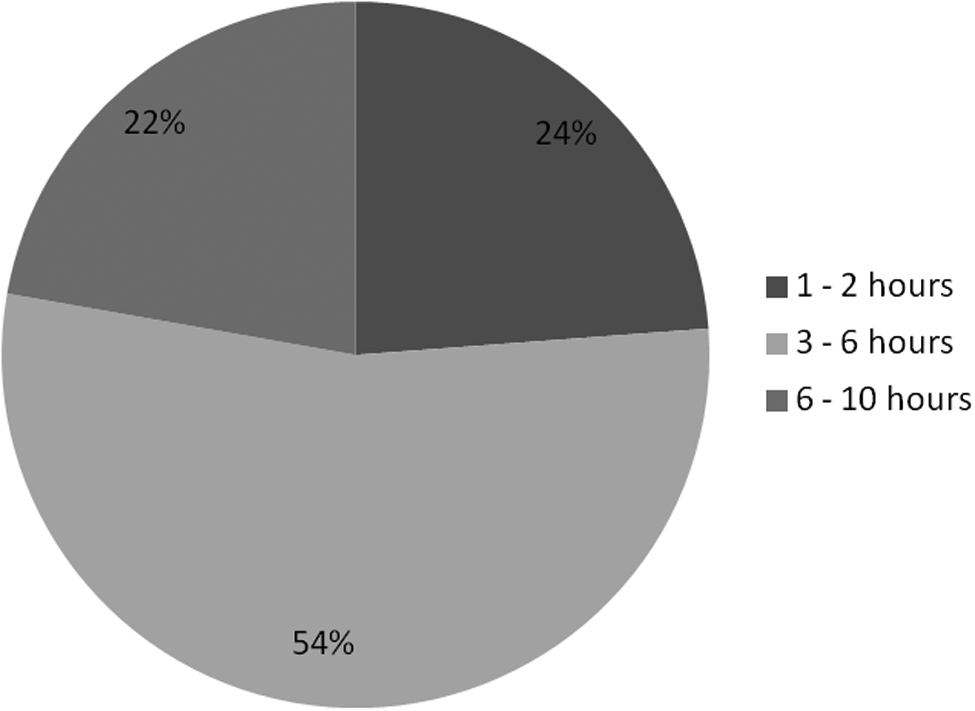
Reported length of time hand was numb/pain-free post-operatively.
The majority (91%) of patients felt that the pain they experienced with WAHS was much the same or less than having a dental procedure such as a tooth extraction.
Postoperatively, 89% stated they did not have any nausea or vomiting, and 11% reported some nausea and vomiting.
Anxiety
We asked patients to rate their level of anxiety before, during, and after surgery, with 0 being not anxious at all to 10 being extremely anxious. The levels of anxiety were generally low and shown to fall sequentially from the pre- to intra- to post-operative periods as shown in Figure 5.
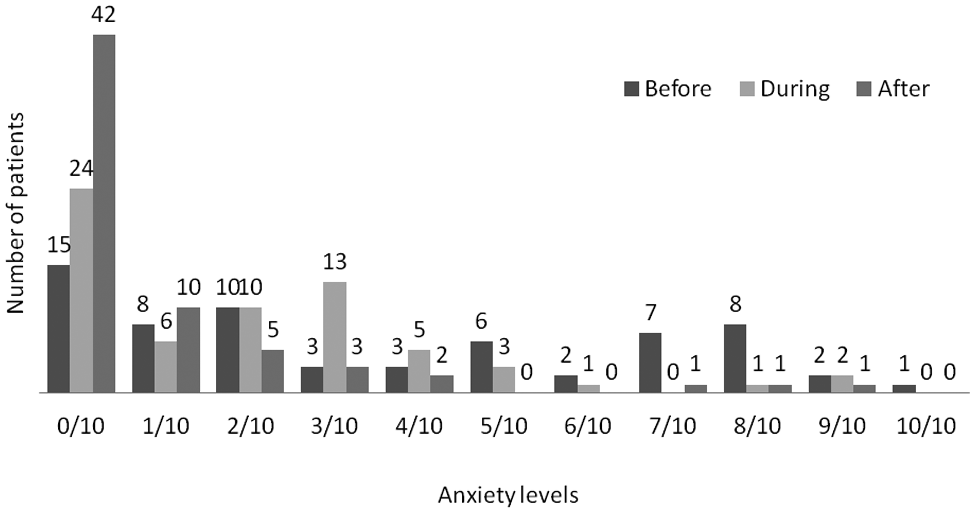
Reported anxiety levels before, during, and after WAHS.
Overall WAHS experience
Eighty-six percent of respondents felt that, if they needed to have hand surgery again, they would prefer to be wide-awake, 4.6% would prefer to be sedated, and 9.2% would like to be completely asleep. When asked about their overall experience of WAHS, 59% felt it was better than what they had expected, 34% felt it was about what they had expected, and 7.7% felt it was worse. Figure 6 shows how the respondents felt regarding recommending WAHS if they had a friend needing hand surgery. All respondents felt well supported by the surgical/nursing team.
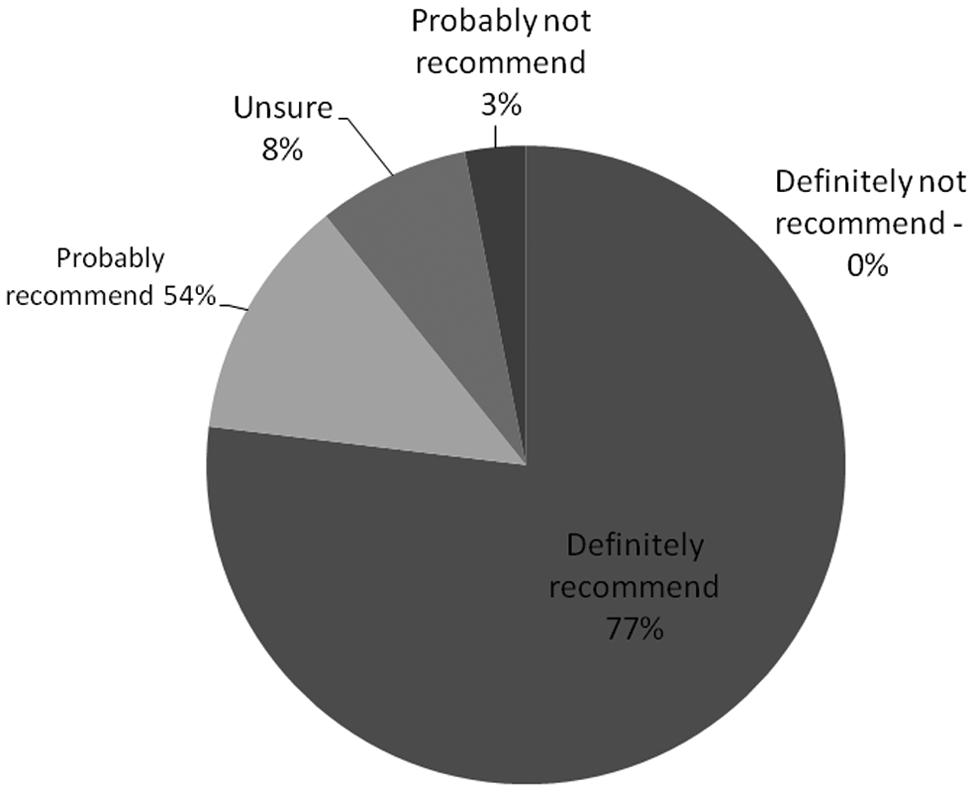
Recommendation of WAHS to a friend.
Effect of timing and type of surgery on responses
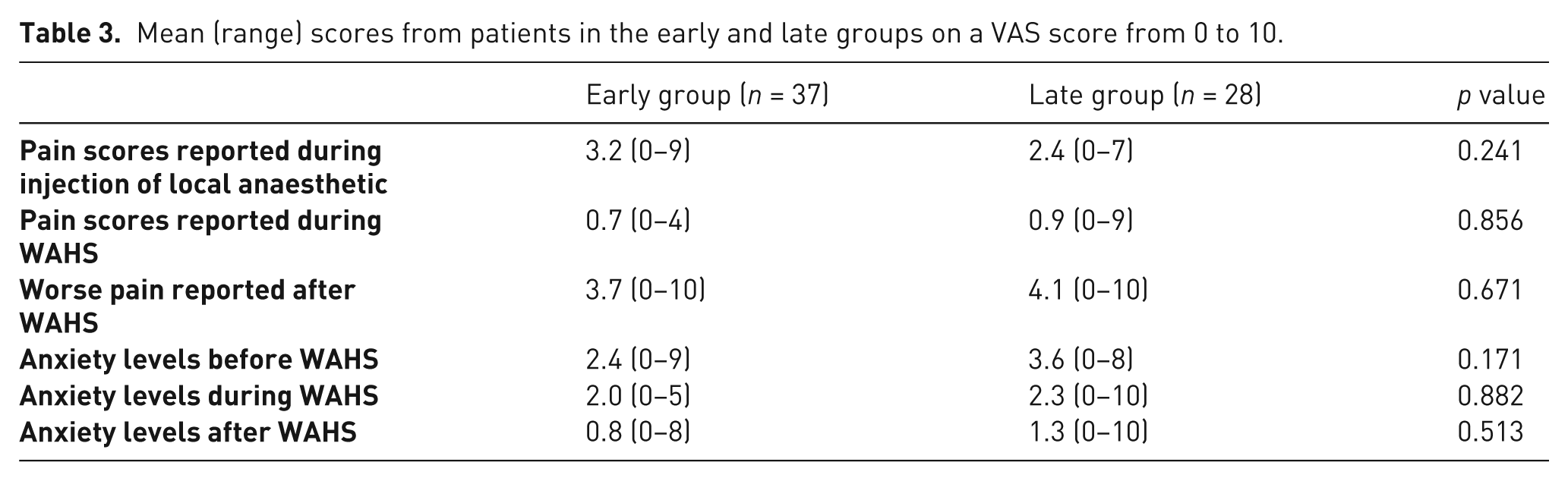
The timing of questionnaires ranged from 3 to 22 months after surgery, with a mean of 7.8 months and median of 6 months. As described, patients were in the early or late group, depending on the time after surgery when they responded. There were 37 patients in the early group and 28 in the late group. We found no statistical difference in pain scores or anxiety levels (Table 3).
Mean (range) scores from patients in the early and late groups on a VAS score from 0 to 10.
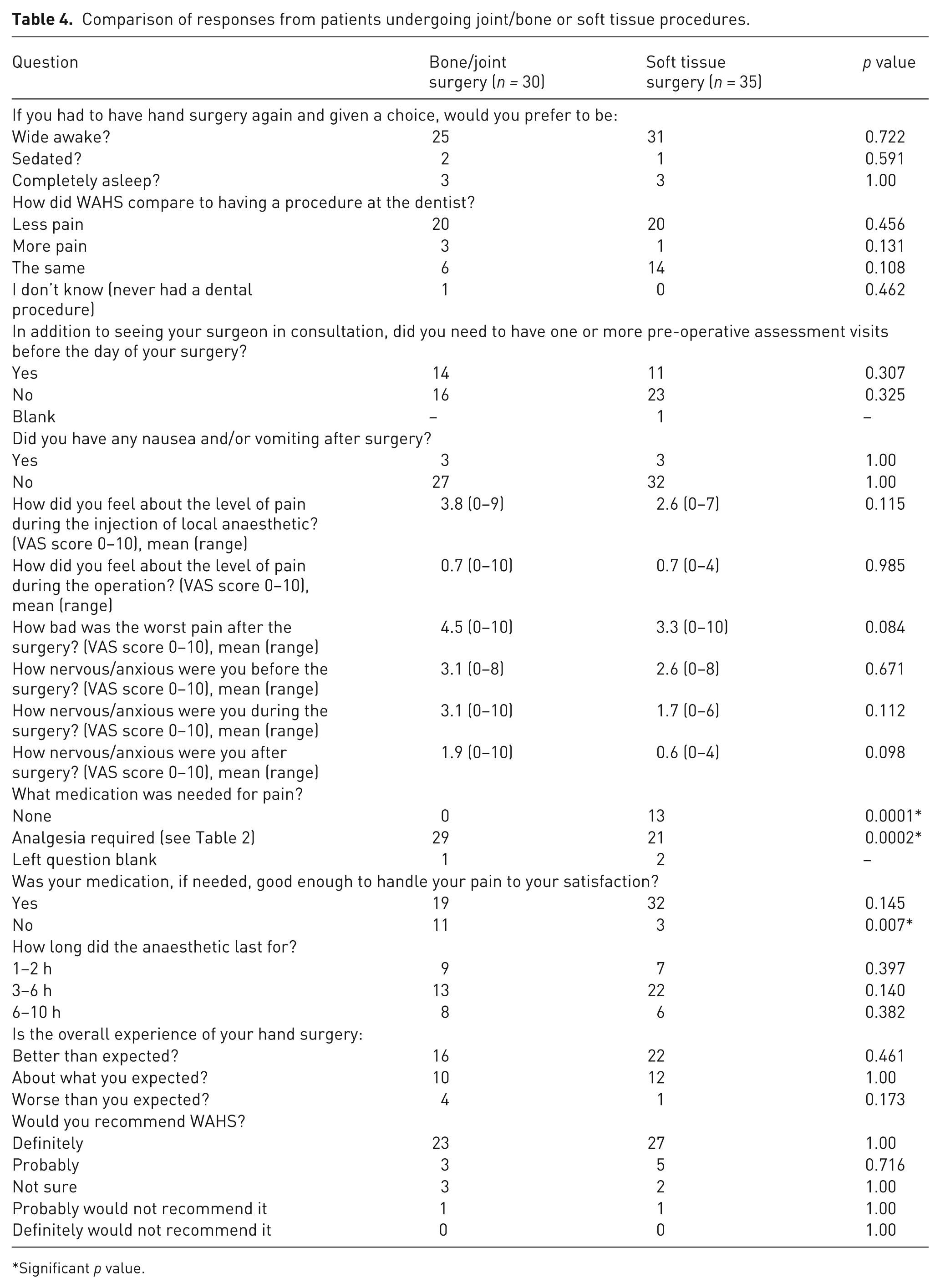
Responses were compared for patients who had bone/joint procedures and those with soft tissue procedures. This demonstrated a statistically significant increase in the number of patients requiring analgesia after bone/joint surgery (p = 0.0001). A higher proportion of patients in the bone/joint surgery group felt that the analgesia they took was unable to provide pain relief to a satisfactory level (p = 0.007). All other areas assessed were not found to be significantly different (Table 4).
Comparison of responses from patients undergoing joint/bone or soft tissue procedures.
Significant p value.
Complications
The procedures in all 100 cases were completed without the need for conversion to a regional or general anaesthetic. No tourniquets were used. One patient who underwent a trapeziectomy developed complex regional pain syndrome. This patient had experienced some pain during the operation with traction on her thumb. In retrospect, the infiltration in or around the base of the thumb and trapezium had not spread enough to anaesthetize the digital nerves, so that the thumb tip was still sensate. There were no cases of skin necrosis or digital ischaemia.
Discussion
Our results show that the majority (88%) of patients reported a score of 5 or less during the injection of local anaesthetic in WAHS, and 68% reported a pain score of 0 during the operation. One patient had had a trapeziectomy done on the left hand with regional anaesthesia and sedation, and subsequently a right trapeziectomy using WAHS. She stated that she preferred WAHS as she did not require a cannula or tourniquet, was not drowsy, and her arm “did not feel dead” after the procedure. In our experience, patients often complain about tourniquet pain, whether under regional block or local anaesthesia. Most feel that tourniquet pain was the worst part of their hand surgery. Patients who have had previous procedures without WAHS have reported that they preferred surgery without a tourniquet. A recent paper (Smith et al., 2012) compared pain perceived from pneumatic and silicone ring tourniquets on the upper limb in 30 healthy volunteers. They concluded that the silicone ring tourniquet “would not be suitable for local anaesthetic procedures due to the severe pain experienced on application.” These volunteers experienced considerable pain with both pneumatic and silicone ring tourniquets, and in fact commented that they “would not feel comfortable on the operating table after such a painful experience.” A big advantage of the WAHS technique is the elimination of tourniquets and its associated pain, therefore reducing the overall discomfort of surgery.
Some patients undergoing WAHS have found the pressing and pulling of tissues outside the wound field to be unpleasant, while not actually experiencing any pain. We now routinely inject into areas outside the surgical site. For example, in Dupuytren’s surgery, we block the dorsal digital nerves proximal to the metacarpophalangeal joints so that hyperextension of the digit at the end of the procedure does not cause discomfort. For trapeziectomies, we block the digital nerves on the palmar aspect of the thumb so that traction of the thumb can be tolerated during the operation.
There was a wide range of scores reported for the “worst” pain experienced after surgery (Figure 3). Only eight patients (12.3%) reported a pain score of 0. Forty-three percent reported a pain score of 1–3, 21% reported scores of 4–6, and 25% reported scores of 7–10. These scores are higher than we expected; however, there is evidence that hand surgery patients experience significant post-operative pain. A survey that analyzed post-operative pain after ambulatory surgery found that 37% of hand surgery patients suffer from moderate to severe pain (Rawal et al., 1997). A controlled study comparing the efficacy of oral analgesics in 120 patients after day-case hand surgery under regional block showed that post-operative pain could not be adequately controlled with a single analgesic drug, and up to 40% of patients felt that their analgesia was inadequate (Rawal et al., 2001). Our findings show that 20% did not need any painkillers, and only 7.7% found that their analgesia was not strong enough to handle their pain. A recent paper (Sorensen et al., 2012) that compared local anaesthetic versus intravenous regional anaesthesia in endoscopic carpal tunnel release in 38 patients found that local anaesthesia significantly reduced post-operative pain and significantly fewer patients in the local anaesthetic group required analgesics during the first 2 hours after surgery. This provides further support to the WAHS technique compared with regional anaesthesia.
A statistically higher number of patients did not require any analgesia in the soft tissue procedure group (13/35) compared with the bone/joint procedure group (0/30), and a higher proportion of patients in the bone/joint group (11/30) felt their analgesia was not satisfactory. This is not surprising, given that those in the bone/joint surgery category would have had greater manipulation of tissues and, hence, greater pain and subsequent analgesic requirements. Greater emphasis needs to be placed on post-operative analgesia, especially for those undergoing surgery involving the bones or joints.
WAHS should prevent the nausea and vomiting patients may encounter with general anaesthesia. A prospective, randomized study involving 100 patients found that nausea and vomiting was significantly less in patients undergoing regional anaesthesia than those having general anaesthesia (McCartney et al., 2004). These authors reported that 15% of patients undergoing regional and general anaesthetic for hand surgery procedures suffered from nausea and vomiting, which is similar to our finding of 11%.
Our results show that patients’ anxiety levels were generally low and fell sequentially from pre- to intra- to post-operative periods. The number of respondents reporting no anxiety at all increased from 26% before surgery to 40% during surgery to 60% after surgery. It is reasonable to assume that patients’ level of anxiety would be less after surgery, regardless of the type of anaesthesia; nonetheless, the falling anxiety levels are a positive reflection of the experience of WAHS.
Although we did not carry out a formal analysis of the cost-effectiveness of WAHS compared with alternatives, we believe there are potential savings with this technique, as it eliminates the costs associated with anaesthetists. In addition, patients would not need a routine pre-operation clinic assessment and time to discharge should be shortened. A retrospective study that analyzed the cost-effectiveness of 1000 cases of orthopaedic WAHS over 10 years found that a wide-awake service, based on a day-case facility, saved the National Health Service approximately £750,000 (€929,550/US$120,1800) for the 1000 cases (Bismil et al., 2012). The national tariff for an operation is the amount paid to the service providers for any admission episode based on a defined procedure. The authors quoted savings of 50–75% of the national tariff using WAHS.
Our results show that this technique is acceptable to patients. The majority of respondents felt the level of pain experienced during surgery was comparable with a dental procedure. Eighty-six percent would prefer to be wide-awake if they had to have hand surgery again, and 90% would recommend WAHS to a friend. Koegst et al. (2011) analyzed 151 patients who had undergone wide-awake carpal tunnel release, release of the first extensor compartment, or trigger finger release. A questionnaire was sent with a 78.8% (119/151) return rate. The authors found that 83% of respondents would choose the WAHS technique again, and only 9% would prefer another form of anaesthetic. Our results are comparable with these findings.
Surgery using the WAHS technique requires some adjustments on the part of the surgeon. The operative field is not bloodless, as one would expect from complete tourniquet control. However, the bleeding is usually minimal and largely confined to the skin edges of the initial incision. In addition, the bleeding slows considerably and is completely manageable if sufficient time has been given to allow the vasoconstrictive effects of adrenaline to work. It is the experience of the senior surgeon (JGM) that operating in this controlled manner does not slow down the surgery to any appreciable extent. The surgeon must become accustomed to the ‘wetness’ of the field. Tumescence with large volumes of local anaesthetic may mean that in some cases the operating field is constantly wet. This can initially be aggravating to a surgeon but easily dealt with by regular compression of the wound with a dry swab.
Although traditional teaching advocates against the use of adrenaline in digits, we have not observed any incidents of ischaemia from using the WAHS technique. However, in general adrenaline should still be avoided if there are concerns about the vascularity of the hand or digit. Phentolamine should always be available in the event of adrenaline-induced ischaemia and a phentolamine ‘rescue’ injection given if necessary (Lalonde et al., 2005). There have been reports of adrenaline injection into digits after accidental auto-injection from EpiPens™ (Mylan Inc., Canonsburg, Pennsylvania, USA) resulting in cold, white digits. Phentolamine has been shown to be effective in reversing the vasoconstrictive effect of adrenaline-induced ischaemia in these circumstances (Velissariou et al., 2004). Phentolamine is available in phentolamine mesylate ampoules in 10 mg/ml strengths and should be injected subcutaneously into the site in question and titrated until the skin becomes pink.
This study confirms the safety, efficacy, and patient popularity with WAHS shown in previous studies from North America. We feel WAHS is a useful concept that deserves greater popularity in hand surgery.
Footnotes
Acknowledgements
We would like to thank Dr D. H. Lalonde for his contributions and permission to adapt his questionnaire for use in our study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent has been obtained from patients whose opinions are presented in this paper.
Conflict of interests
None declared.