
Abstract
Surgical adhesives are useful supplements in surgery, but their benefit in tendon repair is uncertain. The purpose of this study was to evaluate the effect of BioGlue™ on strength of flexor tendon repair. A total of 60 porcine flexor tendons were divided into three groups. In group one, a conventional core and peripheral suture repair was used. In group two, a core suture and BioGlue™ were used. In group three, a conventional core and peripheral suture repair and BioGlue™ were used. We performed static and cyclic axial load testing and measured diameter of the repair site. We found that BioGlue™ did not improve the tensile strength when added to a core and peripheral suture and that there was an increase in bulk at the repair site. We conclude that BioGlue™ application cannot replace a peripheral suture as tensile strength significantly decreases without a peripheral suture, and it does not benefit a tendon already repaired with a core and peripheral suture.
Level of evidence: n/a
Introduction
The primary repair of lacerated flexor tendons remains a challenge in hand surgery (Savage, 2014; Wu and Tang, 2014). Suture rupture, gapping of the repair zone, or knot unravelling may occur during postoperative early tendon motion (Strickland, 2005, Wu and Tang, 2013, 2014). The rupture rate after primary repair occurs with a frequency between 3%−6% (Dy et al., 2012, Elliot et al., 1994, Harris et al., 1999, Savage, 1985; Tang, 2005, 2013). There is a constant effort to improve the tensile strength. Different surgical adhesives for suture augmentation have been tested. For instance, fibrin glue is able to attenuate adhesions, but does not show a significant increase in tensile strength (Frykman et al., 1993, He et al., 2013).
BioGlue™ is another surgical adhesive, considered to have a higher biomechanical stability in comparison to fibrin glue (Schneppendahl et al., 2012). Surgical adhesives are useful supplements in different fields of surgery and the number of available products is persistently growing (Shah and Meislin, 2013). However, their role in flexor tendon surgery remains uncertain (Strickland, 2005). Currently, BioGlue™ is mainly used as a sealant in specializations like cardiac surgery, and there is a lack of information about a possible benefit of augmentation in flexor tendon repair. We hypothesized that augmentation with BioGlue™ would significantly increase the maximum tensile strength, decrease gap formation, and lower the displacement, thus allowing its use in the reinforcement of flexor tendon repair.
Materials and methods
A total of 60 fresh frozen porcine flexor digitorum profundus tendons were used. It is known that porcine flexor tendons have similar biomechanical properties to human flexor tendons and they are frequently used in biomechanical studies (Mao et al., 2011). Tendons from the forelimb were dissected between the A2 and A4 pulleys, where the tendon passes through the superficial tendon (Peltz et al., 2011). The harvested tendons were stored inside saline-soaked swabs and deep-frozen at −20 °C. Before testing, tendons were thawed at room temperature for 12 hours.
Tendon cut and measurement of cross-sectional area
A size 15 scalpel was used to carefully transect the flexor digitorum profundus at the middle of the harvested tendon segment. The height and width of the cross-section of the transected tendon was measured immediately after tendon transection. The cross-sectional area was calculated with a formula for the area of an ellipse (area = πab, where a equals one-half tendon height and b equals one-half tendon width).
Tendon repair
All tendons were randomly assigned to one of three groups of 20 tendons each. In group one, the control group, the tendons were repaired with a 4-strand locking Kessler suture with 3-0 Polydioxanone (PDS) (Johnson & Johnson, New Brunswick, New Jersey, USA) and a peripheral simple running suture, non-locking with 5-0 PDS. A core suture purchase of 0.7 cm and a 10% shortening was used in all groups to ensure the best tensile strength and gap resistance of the repair (Lee et al., 2010; Tang et al., 2003; Wu and Tang, 2012). In group two, the tendons were repaired with a 4-strand locking Kessler suture with 3-0 PDS without a peripheral suture; 1 ml BioGlue™ (CryoLife, Kennesaw, Georgia, USA) was applied circumferentially around the repair site. In group three, the tendons were repaired with a 4-strand locking Kessler core suture with 3-0 PDS and a peripheral simple running suture with 5-0 PDS; 1 ml BioGlue™ was applied around the repair site to cover the suture area (Figure 1). BioGlue™ is composed of purified bovine serum albumin and Glutaraldehyde. The components are preserved separately in a syringe until application, when they merge at the tip of the needle. The molecules react with each other and form a smooth coating at the repair site. The cross-sectional area was measured again after the suture and after application of BioGlue™ to evaluate tendon bulkiness caused by the use of BioGlue™.
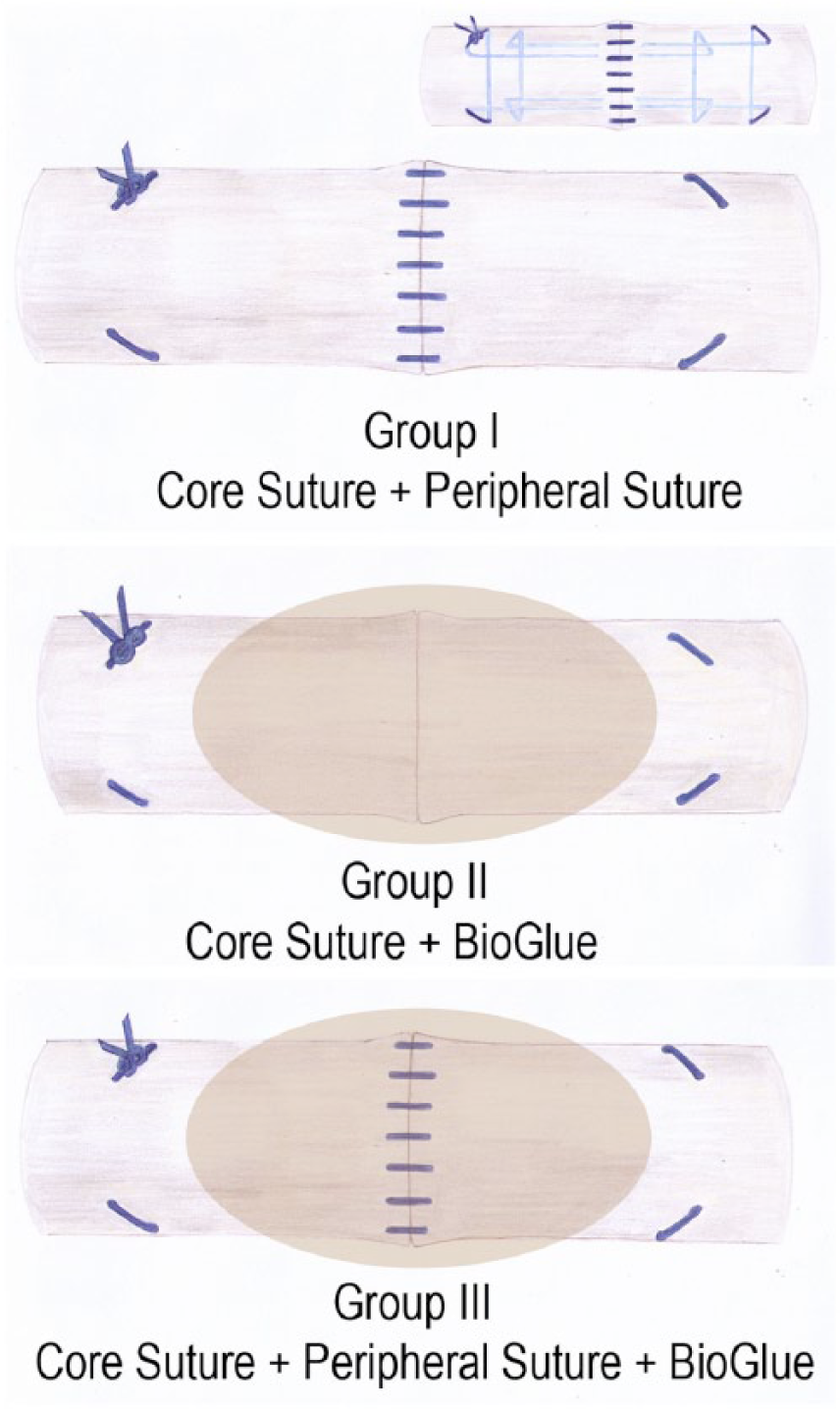
Experimental groups.
Tendons were repaired by a trained orthopaedic surgeon experienced in tendon repair techniques. Throughout tendon suturing and testing processes below, the tendons were kept moist using saline.
Biomechanical testing
Tests were conducted with a mechanical testing machine (Z020, Zwick/Roell GmbH, Ulm, Germany) and the test Xpert II software (Version 3.0, Zwick/Roell). Uniaxial testing was performed using a 100 N load cell and two stainless steel clamps (Figure 2). The distance between two clamps was 3 cm; 1.5 cm tendon length was clamped at each side. Static (10 tendons per group) testing and cyclic testing (10 tendons per group) were applied.
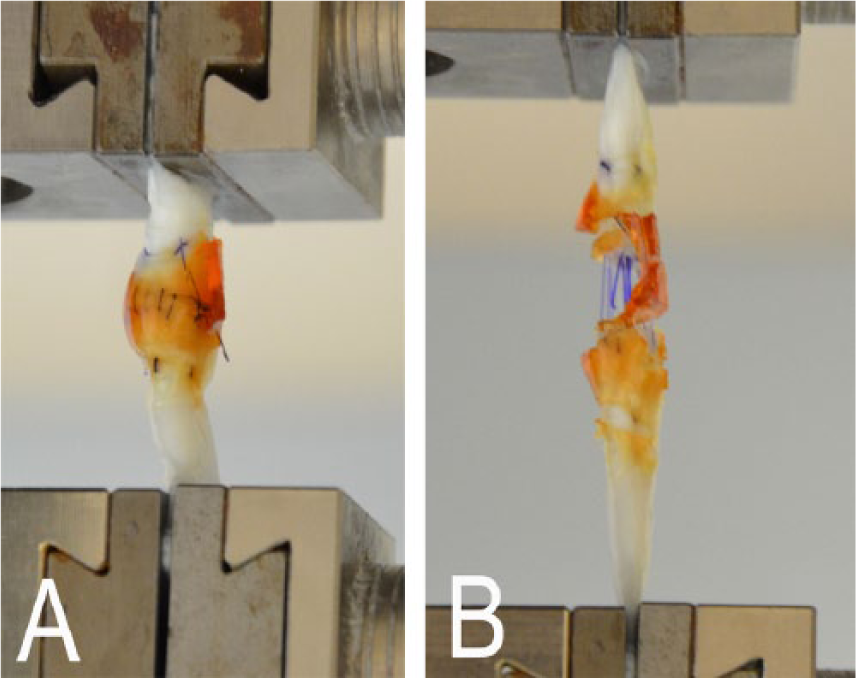
(A) Tendon repaired with core and peripheral suture and augmented with Bioglue™. (B) Axial tension tears the repaired tendon apart until the augmented suture ruptures.
The static test had a preload of 3 N, a tendon distraction rate of 20 mm/min until complete failure of the repaired tendon. A 2-mm gap formation force and maximum load were measured.
The cyclic testing had a preload of 3 N, a preconditioning loading to 10 N for 10 cycles. Subsequently, the tendon had three different maximal loads: 10 N, 20 N, and 30 N. Namely, the tendon was loaded up to 10 N, then increased to 20 N, and finally to 30 N, after 400 cycles at each of the above three loads at distraction rate of 20 mm/min. Load and displacement were continuously recorded to generate a load–displacement curve. The displacement was the length increase of the tendon segment between two clamps measured for each tendon from the curve at the final (400th) cycle of cyclic loading test compared with that at the first cycle.
Statistics
A power assessment using a significance level of 5% and a power of 80% indicated a sample size of 7. Primary endpoints were 2-mm gap formation force, maximum load, displacement, type of failure (pullout vs. rupture), and cross-sectional area. A Shapiro-Wilk test was performed to analyse the distribution. An analysis of variance and Tukey b post hoc test were used for comparison of the means. A p-value of less than 0.05 was considered statistically significant.
Results
Cross-sectional area at tendon repair site
The cross-sectional area of untreated tendons was 19.4 mm2 (SD 4.2). The cross-sectional area of core and peripheral suture repair was 38.2 mm2 (SD 6.7). The cross-sectional area of tendons repaired with a core suture and BioGlue™ was 62.5 mm2 (SD 8.9). The cross-sectional area of a core and peripheral suture in combination with BioGlue™ was 78.6 mm2 (SD 12.2). Compared with the tendon with standard core and epitendinous suture repair, the cross-sectional area at the repair site was significantly increased in the tendon with core suture plus glue repair (p < 0.01) and in the tendon with core and epitendinous suture and glue repair (p < 0.01). The mean increase were 64% and 106%, respectively.
A 2-mm gap formation force
A 2-mm gap formation force was significantly lower in group two where BioGlue™ was used (p < 0.001), but no peripheral suture compared with the other two groups (Figure 3). There was no significant difference between the tendons with core and epitendinous repair and those after adding BioGlue™ to the core and peripheral suture.
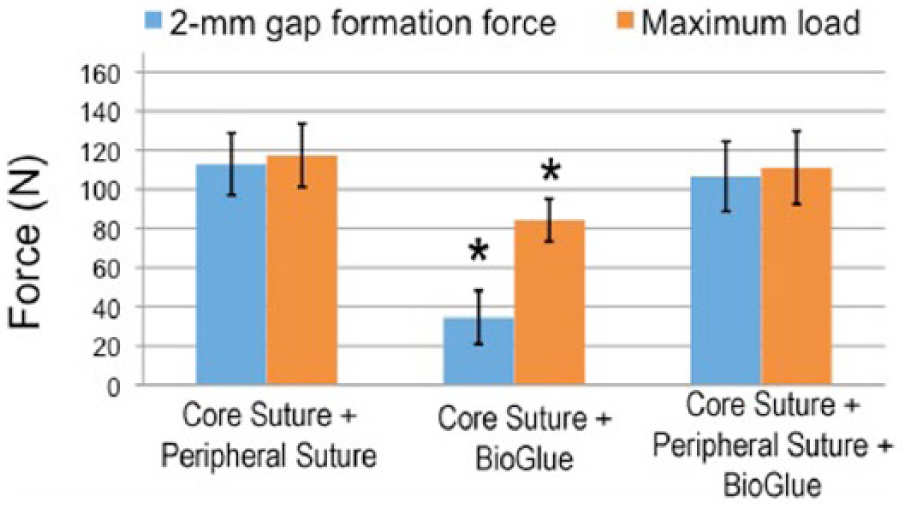
Flexor tendon repair using a core suture and BioGlue™ without a peripheral suture shows a significantly lower gap formation force (p < 0.001) and maximum load (p < 0.01). Tensile strength is not significantly increased in group 3 after augmentation with BioGlue™. The asterisk indicates data of significant differences compared with those in the other two groups.
Maximum load
Maximum load was significantly lower in group two where no peripheral suture but BioGlue™ was used for augmentation (p < 0.01). There was no significant difference between the tendons with core and epitendinous repair and those after adding BioGlue™ to the core and peripheral suture (Figure 3). All tendons failed by suture rupture in between the tendon ends.
Displacement
Displacement in group two was significantly higher than the other two groups at 10 N, 20 N, or 30 N maximal load (p < 0.05 or p < 0.01). Displacement of the tendons between other two groups had no significant difference (Figure 4).
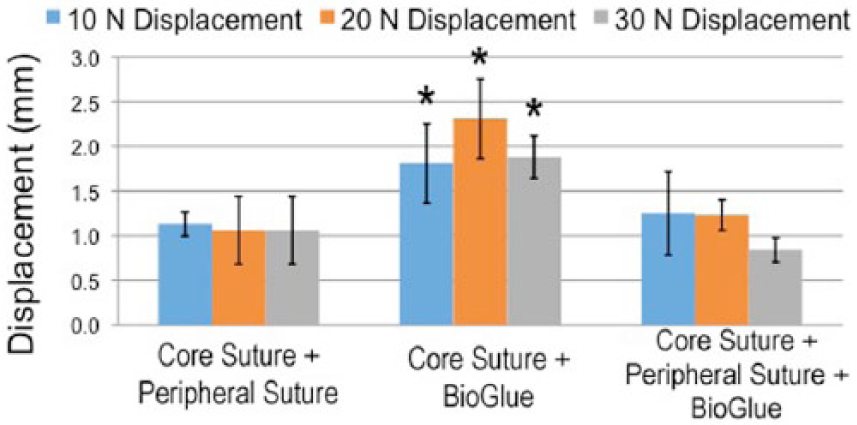
Tendon displacement was significantly increased in group two with only a core suture and application of BioGlue™(p < 0.05 or p < 0.01). The asterisk indicates the data of significant differences compared with those in the other two groups.
Discussion
In flexor tendon repair, different augmentation techniques using glues were studied (Frykman et al., 1993, Jones et al., 2002, Xu et al., 2013). Fibrin glue is one type of surgical adhesive that was evaluated for tendon repair in previous studies, particularly in Achilles tendons (Ambacher et al., 2001, Hohendorff et al., 2008). Frykmann et al. (1993) sutured lacerated flexor tendons in a rabbit model and covered the defect with fibrin glue for augmentation. They were able to show that fibrin augmentation prevented adhesions. He et al. (2013) used a similar in vivo model and confirmed the possible attenuation of adhesions. In addition, they showed that fibrin glue did not alter the biomechanical healing strength of the repaired tendons. Xu et al. (2013) found in cadaveric flexor tendons that the fibrin glue causes higher gliding resistance. In our study, reinforcement with a surgical adhesive BioGlue™ did not increase the tensile strength, but it increased the bulkiness of the repair site.
BioGlue™ is believed to have a higher stability than fibrin glue (Schneppendahl et al., 2012), therefore, it appeared reasonable to use it to augment flexor tendon repair. However, our biomechanical study shows no mechanical benefits of using this surgical adhesive. Our results show that BioGlue™ cannot replace a peripheral suture, nor does it increase the maximum load or resistance to gap formation after conventional core and peripheral suture in static or cyclic loading conditions. A 4-strand repair is used because multi-strand repair is the mainstay of flexor tendon repair in the last 10 years (Strickland, 2005; Tang et al, 2014; Wu and Tang, 2014). A 5-0 PDS was used for a peripheral suture, which is a bit stronger than a 6-0 suture that most surgeons used. We assume that our peripheral suture has been quite strong. With the application of BioGlue™ to a tendon with a core and peripheral suture, there was an increase in bulk at the flexor tendon repair site, but no gain in tendon repair strength. Currently, suture technique modification or use of innovative suture material might be a better approach to enhance flexor tendon repair strength (Wu and Tang, 2014) than application of glue or other additional substances (Lees et al. 2015).
Our study was limited to a pure biomechanical study that does not involve a tendon healing process. We also cannot evaluate adverse effects of BioGlue™, such as inflammation, foreign body reaction, or tissue necrosis (Furst and Banerjee, 2005, Lemaire et al., 2007, Witter et al., 2010). It is unknown how the separation from the synovial fluid affects tendon healing. These should also be considered in future investigations (Rodger et al., 2015). Bulkiness of the tendon repair site caused by applying a surgical adhesive can be a major concern, as the digital flexor tendon in the hand is confined in a narrow space by segmental rigid annular pulleys (Lowrie and Lees, 2014), which would greatly increase gliding resistance during early active tendon motion after surgery.
Based on our present ex vivo mechanical study, we conclude that the addition of surgical adhesive BioGlue™ does not increase surgical repair strength of a tendon already repaired with a core and peripheral suture, and that the glue increases diameter of tendon repair site, potentially increasing resistance to tendon gliding.
Footnotes
Acknowledgements
The authors thank Johannes Hain from the Institute of Mathematical Statistics for statistical support and Torsten Blunk for writing assistance. The work was done at the biomechanical laboratory in the Department of Trauma, Hand, Plastic and Reconstructive Surgery, University Clinics of Wuerzburg.
Conflict of interests
None declared.
Funding
The authors thank the IZKF (Interdisciplinary Center for Clinical Research), University Clinics of Wuerzburg, for support of our biomechanical studies.