
Abstract
We retrospectively reviewed the outcomes of flexor tendon repairs in zones 1, 2 and 3 in 356 fingers in 291 patients between 2005 and 2010. The mean (standard deviation) active ranges of motion of two interphalangeal joints of the fingers were 98° (40) and 114° (45) at 8 weeks postoperatively and at the last follow-up (mean 7 months, range 3–98), respectively. Using the Strickland criteria, ‘excellent’ or ‘good’ function was obtained in 95 (30%) out of 322 fingers at 8 weeks and 107 (48%) out of 225 fingers at the last follow-up. A total of 48 (13%) fingers required reoperation because of rupture, adhesion, contracture or other complications. The prevalence of rupture was 4%. We carried out multiple linear regression analysis to identify the predictors of the active digital motion. The following variables were found as negative predictors: age; smoking; injury localization between subzones 1C and 2C; injury to the little finger; the extent of soft tissue damage; concomitant skeletal injury; delay to surgery; use of a 2-strand Kessler repair technique; attempted suture or preservation of the tendon sheath–pulley system; and resecting or leaving the concomitant superficial flexor tendon cuts untreated. Analysing the 8 weeks results of tendon repairs in zones 1 and 2, early active mobilization was found to be superior to Kleinert’s regime.
Introduction
The treatment of flexor tendon injuries in the fingers is challenging and the functional results are not always optimal. Ruptures and adhesions around the repaired tendon needing tenolysis are found in approximately 5% each (Dy et al., 2012a; Elliot, 2002). Further surgery for rupture or adhesions is required in around 6% of cases (Dy et al., 2012b). Age, smoking, zone of injury, multiple finger injuries, associated flexor digitorum superficialis (FDS) tendon injury, nerve injuries and delayed treatment have previously been reported to adversely affect outcomes (Elhassan et al., 2006; Kasashima et al., 2002; McFarlane et al., 1968; Silfverskiöld et al., 1993; Trumble et al., 2010).
The aim of this study was to identify predictors for poor outcomes in a large series of flexor tendon repairs.
Methods
Patients
A total of 736 patients were operated on in Oslo University Hospital with primary or delayed primary flexor tendon repair between 1 January 2005 and 31 May 2010. Data were collected retrospectively from the medical records. We included flexor digitorum profundus (FDP) injuries in zones 1, 2 or 3. The exclusion criteria were: thumb injuries (74 patients); proximal injuries, i.e. zones 4–5 (66); distal injuries needing tendon reattachment to the distal phalanx (37); concomitant replantation or revascularization (68); post-operative immobilization in children or because of concomitant unstable skeletal injuries (116); partial FDP laceration (16); referrals from other hospitals (15); and patients with insufficient documentation or follow-up (53).
Inclusion and injury characteristics
A total of 291 patients with 356 injured fingers were included. The mean age was 35 years (range 7–88). The patient characteristics and the injury-related variables are shown in Table 1.
Characteristics of the included 291 patients and 356 finger injuries.
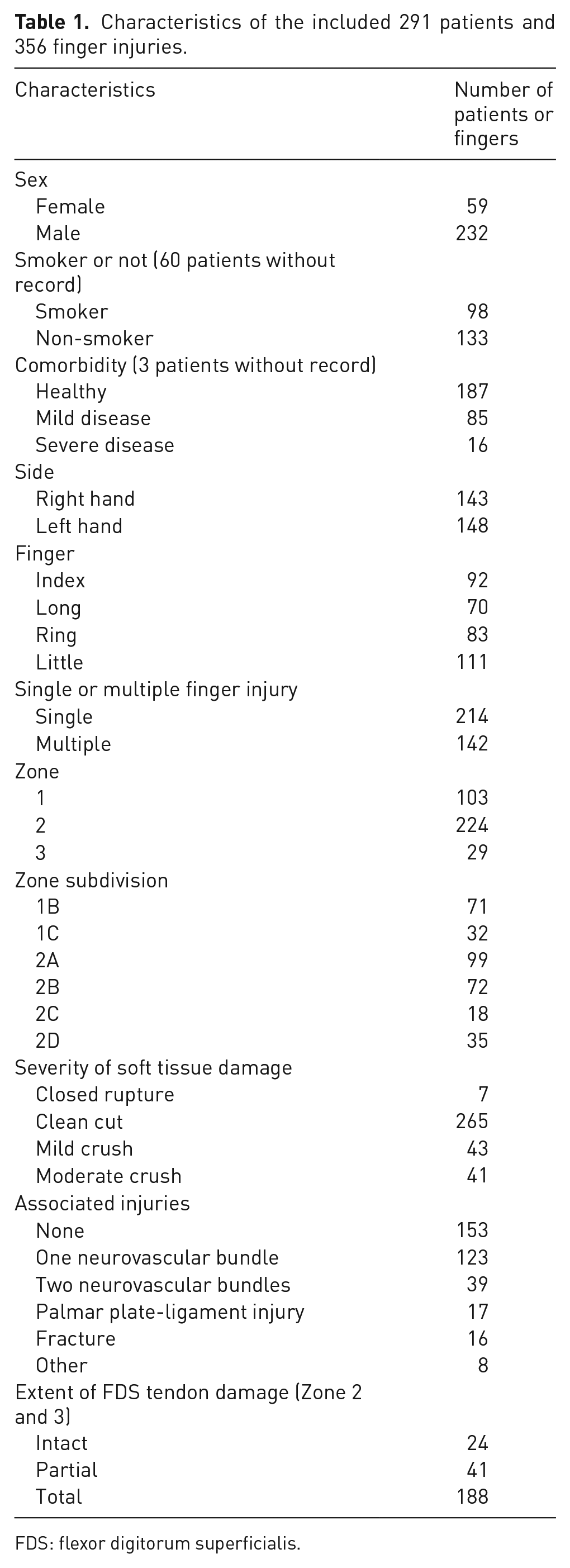
FDS: flexor digitorum superficialis.
We subdivided the injuries in zones 1 and 2 using Moiemen and Elliot’s (2000) and Tang’s (1994) criteria: the relation of the distal FDP stump to the main pulleys and joints defined the localization, i.e. FDP lacerations under the A4 and A2 pulleys were subzone 1C and 2C, respectively. The original laceration of the tendon sheath is usually proximal to the distal tendon stump in the extended finger. The localization of the FDS tendon injury was also subdivided: detachment from the insertion – zone 2A; distal to the A2 pulley –2B; under the A2 pulley – 2C; and proximal to the A2 pulley, but still within the tendon sheath –2D.
Fingers with crush injuries were included as long as flexor tendon repair and early mobilization were possible. Lacerations by knives or glass were defined as clean cuts, irregular sharp objects (e.g. metal plates) as mild crush and motorized tools (e.g. circular saws) as moderate crush injuries.
Surgical techniques for tendon repairs
Surgery was mostly performed within 3 days. In 42 patients the repair was postponed for 3–14 days. In 23 patients the delay was more than 14 days, but direct end-to-end tendon repair was still possible.
A total of 287 FDP tendons were repaired with a traditional 2-strand modified Kessler technique completed with a simple running suture. A side-locking loop repair (Yotsumoto et al., 2005) combined with interlocking horizontal mattress epitendinous suture (Dona et al., 2003; Rigó et al., 2012) was performed on 61 FDP tendons, and a double Kessler (Smith and Evans 2001) repair in eight. The material of the core suture was braided polyblend polyethylene (FiberWire; Arthrex Co., Naples, FL, USA) in the Yotsumoto-Dona repair; otherwise monofilament polypropylene (Prolene; Ethicon, Sommerville, NJ, USA) in 107, monofilament nylon (Dermalon; Covidien Ltd., Mansfield, MA, USA) in 78, and polydioxanole (PDS; Ethicon, Somerville, NJ, USA) in 10 FDP repairs. In 101 fingers the suture material was not recorded in the operation notes. The dimension of the core suture was always 3-0; the peripheral sutures were carried out with 5-0 or 6-0 monofilament polypropylene.
Simple opening without attempting to close the tendon sheath or partial pulley release as suggested by Tang (2007) was performed in 137 fingers. In 65 fingers we attempted to close the sheath, to reconstruct or suture the pulley, or to avoid opening the overlying pulley despite making the repair more difficult. The treatment of the sheath or pulley was not documented in 125 cases.
The FDS tendon was uninjured or nearly normal with no need for treatment in 34 of the 253 fingers in zones 2 and 3. In 11 fingers the injured FDS slip was resected back to the chiasma, while the other slip was preserved in continuity. Only one slip was sutured, while the other was resected in 24 fingers and both slips sutured in 34 fingers with a complete FDS laceration through the chiasma; these repairs were carried out with either a Becker or a modified Kessler technique. In 40 fingers the injury was in the subzone 2D or zone 3, where the same technique was used as in the FDP tendon. A total of 92 lacerated FDS tendons were resected proximally and 18 were left retracted within the sheath.
The operating surgeon’s experience was ranked as proposed by Tang (2009); however the surgeons often carried out the operations with the assistance of a colleague with a higher level of experience. Non-specialist surgeons (level 1) performed tendon repair in 78 fingers, less experienced specialists (level 2) in 81, experienced specialists (level 3) in 83 and highly experienced specialists (level 4) in 114. The total number of surgeons was 16.
Postoperative care and motion protocols
After surgery, a short forearm splint up to the proximal interphalangeal joints was applied, with 10°–30° of wrist flexion and 50°–80° of metacarpophalangeal joint flexion. Rubber bands were attached to the injured fingers. A total of 263 patients were instructed to carry out 30 repetitions of passive flexion and active extension per hour (Kleinert’s regime). Twenty-eight patients were allowed to carry out ten non-resisted active finger flexions per hour (early active mobilization programme) after warming up with 10 repetitions. The splint and rubber bands in these 28 patients were the same as in those with Kleinert’s regime. All patients started finger motion on the first or second postoperative day. After 4 weeks, splint protection was removed and unrestricted finger motion started. Injuries in zones 1, 2 or 3, concomitant nerve injuries and stable fractures were mobilized using the same protocol.
Follow up and assessment criteria
The active ranges of motion (AROM) of the proximal and distal interphalangeal joints were measured by the therapists with a goniometer placed dorsally on the fingers during the follow-up consultations. The data were collected retrospectively from the medical records at 8 weeks post-operatively and at the last consultation; the mean follow-up was 7 months (range 3–98). The functional outcome was graded according to Strickland and Glogovac (1980). Reoperations were also recorded from the medical notes.
Statistical analysis
The statistical analyses were performed in six series after allocating the fingers into the following groups: all zones; pooled zone 1 and 2 injuries for assessment of the effect of the tendon sheath and pulley treatment; pooled zone 2 and 3 injuries for assessment of the variables associated with the FDS tendon; with AROM as the dependent variable at 8 weeks; and at the last follow-up with a minimum of 3 months. Multiple linear regression analyses were carried out to predict the AROM using the following explanatory variables: age, gender, smoking, side, injured finger, single or multiple finger injury, zone and subzone of injury, extent of soft tissue damage, associated injuries, extent of FDS injury, surgical delay, surgeon’s experience, FDP suture technique, type of rehabilitation, treatment of the tendon sheath/pulley system and treatment of the FDS tendon; these variables were chosen based on clinical judgment. The models were accomplished with backward analysis; the Akaike Information Criterion (AIC) was used to select the best models. In order to gain the best model fit and minimize the amount of residuals, some variables with insignificant effects (p ⩾ 0.05) were kept. The statistical analyses were carried out using IBM SPSS Statistics 22 program and methodical advice was gained from a statistician.
The adjusted R-squared values of the regression models indicate the proportion of variances in observations that the models could explain. The intercept represents the optimal predicted AROM, which is changed by the sum of effects from the different predictors in each case; the 95% confidence interval (95% CI) represents the uncertainty of the estimations. The regression coefficient is the mean value of the changes in AROM when the value of the particular explanatory variable changes with one unit; in case of a linear variable, such as age or delay to surgery, the coefficient should be multiplied by the value of the variable.
We merged the multinomial categorical variables into binary ‘dummy variables’ as required by the regression models, to distinguish the values with significant and insignificant effects, e.g. injury between subzones 1C and 2C or an associated fracture. The treatment of the FDS tendon was merged into new variables, ‘condition of FDS’, with the following categories: FDS tendon in continuity, repaired or not repaired. We excluded comorbidity as an explanatory variable because of the strong collinearity with smoking, which had a larger effect on the results. The suture material was excluded as well because of the large proportion of missing data and the excessive collinearity with repair technique. The effect of the sheath or pulley treatment was analysed only in zone 1 and 2 injuries, while the extent of FDS tendon damage and FDS treatment were analysed only in zone 2 and 3 injuries.
Results
Functional recovery and prevalence of reoperation
A total of 332 fingers were available for functional analysis at 8 weeks; 225 had a minimum of 3 months follow-up. The mean (SD) AROM was 98° (40) and 114° (45) at 8 weeks and at the last follow-up, respectively. ‘Excellent’ or ‘good’ function was achieved in 95 (30%) and 107 (48%) fingers at 8 weeks and at the last follow-up, respectively. A total of 15 digits (4%) suffered rupture of the repair, 12 in zone 2, two in zone 1 and one in zone 3. Four ruptures occurred during the first 4 weeks while still using the splint, seven within 2 weeks of removal of the splint and four after more than 6 weeks post-operatively. A total of 48 (13%) of 356 fingers required revision surgery, including 15 (4%) re-repairs of ruptured tendons, 14 (4%) tenolyses including two joint releases, eight (2%) tenodeses or arthrodeses, five (1%) corrections of finger scars, five (1%) excisions of granulomas, two carpal tunnel releases and one amputation. Four fingers underwent more than one reoperation.
Factors affecting the outcome
A significant regression equation was found in all models (Tables 2 and 3); however, the adjusted R-squared values of the models were relatively low, e.g. the adjusted R-squared of 0.227 in model 1 means that the model can explain only 22.7% of the deviations from the expected values. Assessing all zones of injury, age, smoking, injury localization between subzones 1C and 2C, associated fracture, and using traditional Kessler or double-Kessler suture instead of Yotsumoto-Dona suture, were the significant negative predictors for AROM at both 8 weeks (Model 1) and at the last evaluation (Model 4); these variables were also significant predictors in all subgroup analyses (Figure 1). The delay to surgery had no significant effect; however, including it into the analyses improved the statistical model, implying it was also a predictor. The predicted final AROM was 163°. The Yotsumoto suture increased the AROM by 36°. An associated fracture, injury localization between subzones 1C and 2C and smoking decreased AROM by 34°, 29° and 29°, respectively. The final AROM decreased 0.7° for each additional year of age and 0.3° for each additional day of delay to operation. These effects are relatively low but represent a reduction of 21° in a 50-year-old patient compared with a 20-year-old, and a further 4° of reduction for a delay to surgery of 14 days. The AROM at the last evaluation correlated significantly with the AROM at 8 weeks (Figure 2).
Summary of the multiple linear regression models for AROM at 8 weeks.
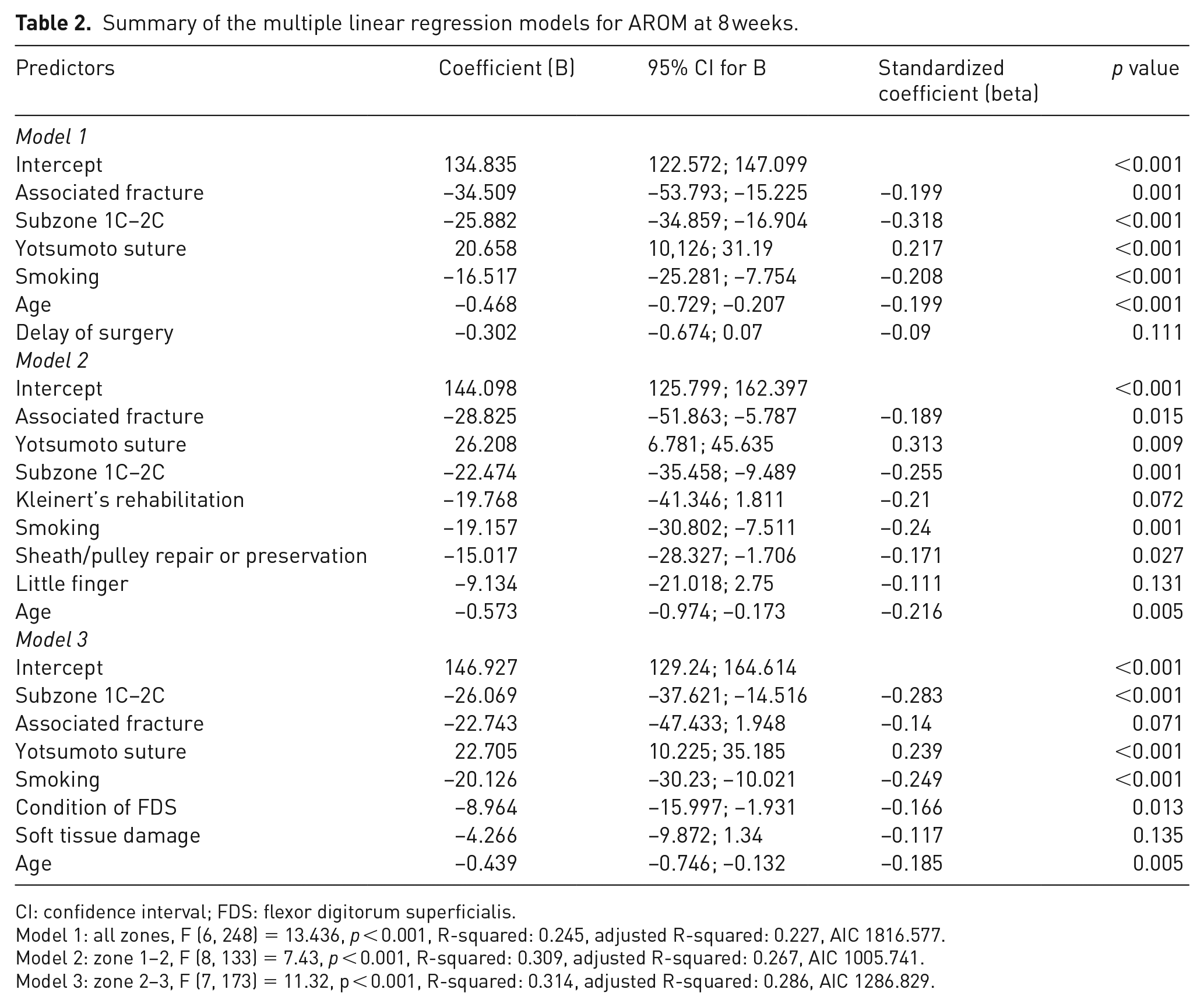
CI: confidence interval; FDS: flexor digitorum superficialis.
Model 1: all zones, F (6, 248) = 13.436, p < 0.001, R-squared: 0.245, adjusted R-squared: 0.227, AIC 1816.577.
Model 2: zone 1–2, F (8, 133) = 7.43, p < 0.001, R-squared: 0.309, adjusted R-squared: 0.267, AIC 1005.741.
Model 3: zone 2–3, F (7, 173) = 11.32, p < 0.001, R-squared: 0.314, adjusted R-squared: 0.286, AIC 1286.829.
Result of the multiple linear regression models for AROM at last consultation.
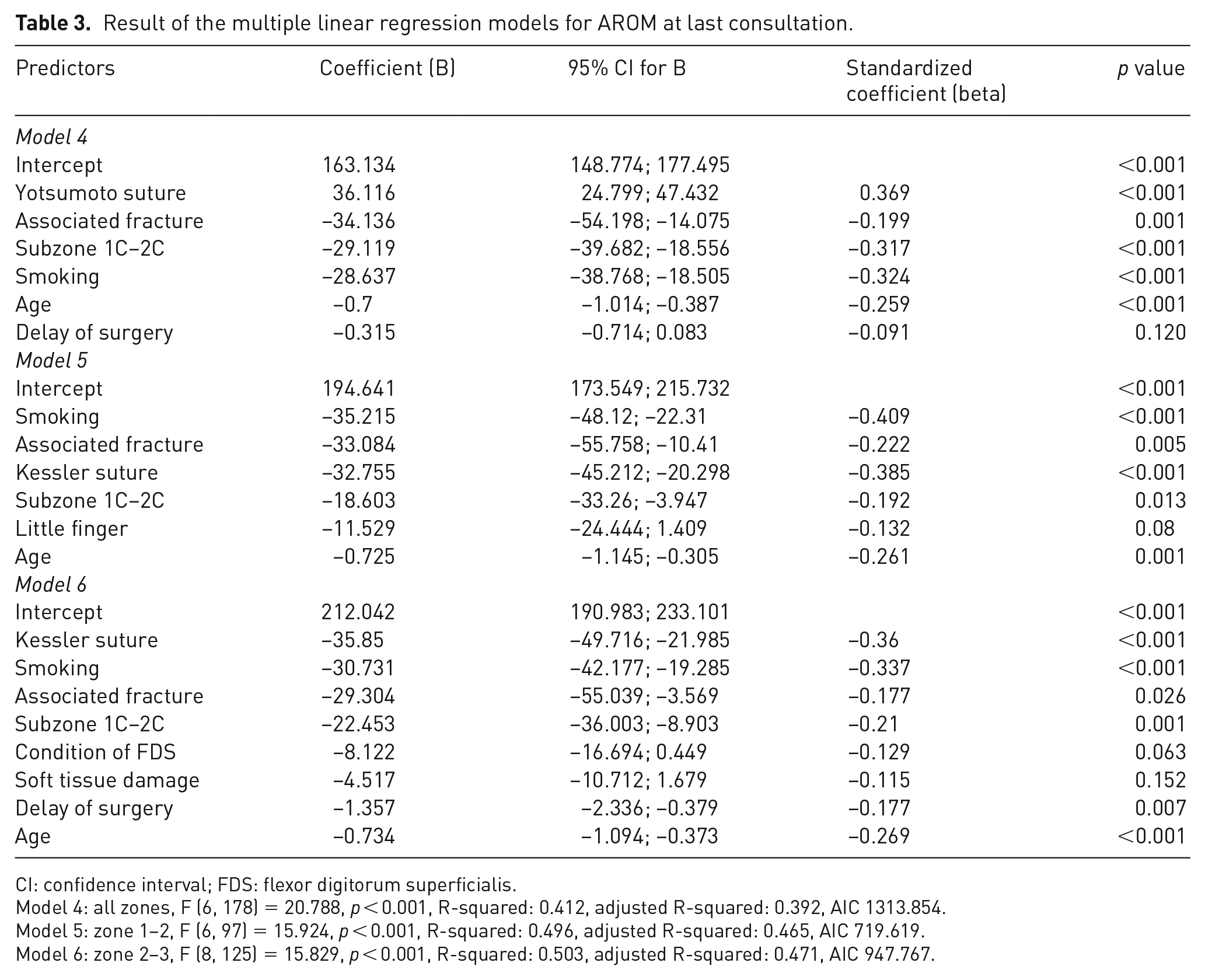
CI: confidence interval; FDS: flexor digitorum superficialis.
Model 4: all zones, F (6, 178) = 20.788, p < 0.001, R-squared: 0.412, adjusted R-squared: 0.392, AIC 1313.854.
Model 5: zone 1–2, F (6, 97) = 15.924, p < 0.001, R-squared: 0.496, adjusted R-squared: 0.465, AIC 719.619.
Model 6: zone 2–3, F (8, 125) = 15.829, p < 0.001, R-squared: 0.503, adjusted R-squared: 0.471, AIC 947.767.
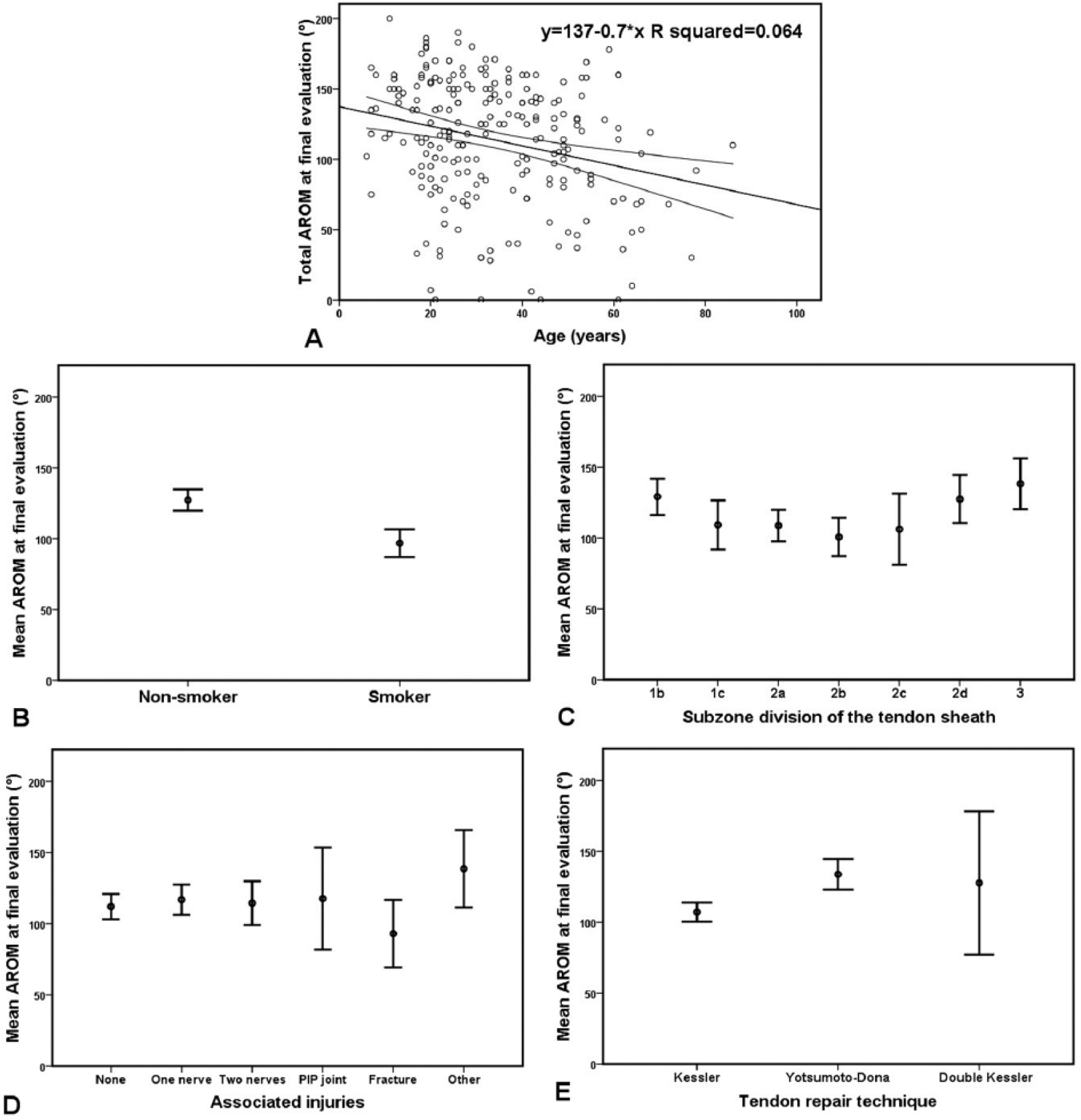
Predictors of AROM at the final evaluation, assessing all zones. Error bars represent 95% confidence interval of the mean. (A) Significant negative correlation between age and AROM. (B) Significant negative effect of smoking. (C) Significant negative effect of injury localization between subzones 1C and 2C. (D) Significant negative effect of an associated fracture. (E) Significant negative effect of modified Kessler repair.

Significant positive correlation between the 8 weeks’ and the final AROM.
In the subgroup analysis of zone 1 and 2 injuries, repair or preservation of the tendon sheath/pulley was an additional negative predictor, causing 15° reduction of AROM at 8 weeks (Model 2). Injury of the little finger and the use of Kleinert’s rehabilitation regime instead of early active motion reduced the 8 weeks’ AROM by a mean of 9° and 20°, respectively; however, the effects were statistically insignificant. Assessing the late results (Model 5), age, smoking, injury localization between subzones 1C and 2C, associated fracture and suture technique were the significant predictors as mentioned above; however, the double Kessler repair was no longer a risk factor compared with the Yotsumoto-Dona technique. The little finger was included as an insignificant predictor in the late model as well. The treatment of the sheath–pulley system and the rehabilitation could no longer be included in the statistical model, probably due to the small sample sizes.
The ‘condition of the FDS tendon’ was an additional significant predictor of the AROM at 8 weeks in pooled zone 2 and 3 injuries (Model 3): repaired and unrepaired total FDS tendon injuries decreased the AROM by 9° and 18°, respectively. The ‘condition of the FDS tendon’ was also included as a predictor in the statistical model for the late results; however, the effect was no longer significant (Model 6). Delay to surgery became a significant predictor. Double Kessler and Yotsumoto-Dona sutures were both superior to Kessler sutures. The extent of soft tissue damage was incorporated in both the 8 weeks’ and the late statistical models, but had an insignificant effect.
Our statistical analysis was unable to show any effect of other patient or injury-related variables on the functional results, including gender, side, single or multiple finger injuries, association with injuries other than fractures or extent of FDS tendon damage. Among the assessed treatment-specific variables, the surgeon’s experience was not proven to be a predictor.
Discussion
Excellent or good function has been reported in 70%–80% of digits after primary flexor tendon repair (Baktir et al., 1996; Cullen et al., 1989; Elliot, 2002; Elliot et al., 1994; Moriya et al., 2015; Tang, 2005, 2013). Complications or the need for further treatment lead to longer follow-up compared with the successful cases. The function of injured fingers can improve for up to 1 year after surgery because of the gradually increasing motion (Elliot, 2002; May and Silfverskiöld, 1993; Moriya et al., 2015). Our patients with satisfactory results at 8 weeks were often not called back for further follow-up, so the last recorded active range of motion may have been poorer than what would have been recorded later. This may be one reason why our functional results are inferior to other reports, where all the patients were called back for late evaluation.
One reason to evaluate the functional results at 8 weeks is the larger sample size, improving the statistical models. The other reason is that the long-term outcome is significantly correlated to the early results. Silfverskiöld et al. (1993) found the range of motion at 3 weeks to be a significant predictor of the final function. We found significant correlation between the AROM at 8 weeks and at final review. Several predictors at 8 weeks were no longer significant at the later analyses, probably because of the smaller sample sizes.
Age, smoking, soft tissue damage, zone 2 injury, multiple finger injuries, delay to surgery and associated FDS and nerve injuries are established risk factors for suboptimal functional results after flexor tendon surgery (Elhassan et al., 2006; Kasashima et al., 2002; McFarlane et al., 1968; Silfverskiöld et al., 1993; Trumble et al., 2010). The effect of operative technical details were not analysed in these studies (Table 4). We investigated a considerably larger number of fingers (patients) and also included crush injuries in the analyses. Moderate crush injuries and concomitant stable phalangeal or metacarpal fractures do not contraindicate flexor tendon repair as long as early mobilization is possible; however less favourable results can be expected in these cases (Tang, 2007). An accompanying phalangeal fracture and smoking have been linked to poor functional results of tendon surgery (Slattery, 1988; Trumble et al., 2010); both findings were confirmed by our study.
Comparison of publications on risk factors for suboptimal functional outcome.
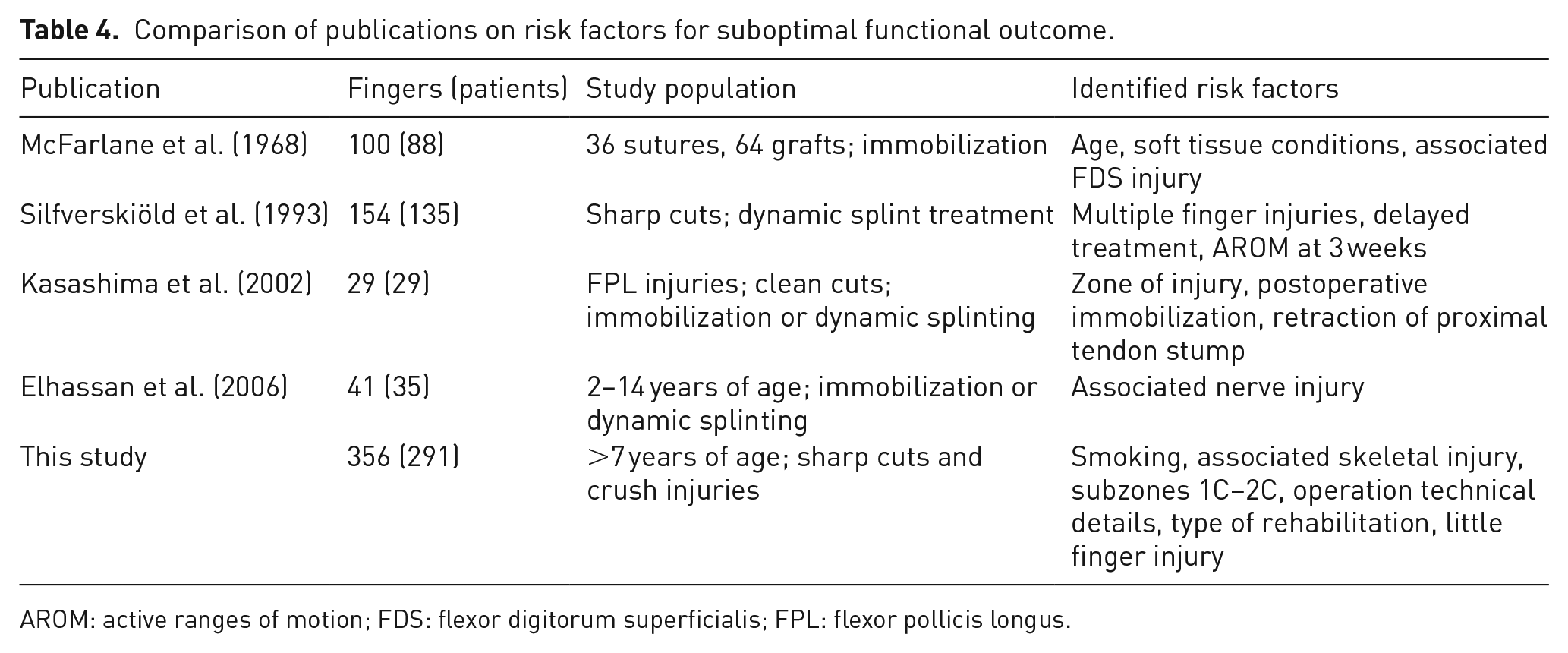
AROM: active ranges of motion; FDS: flexor digitorum superficialis; FPL: flexor pollicis longus.
It is widely accepted that zone 2 injuries have poorer functional outcome than injuries in other zones. Subzone 2C, which is the narrowest part of the sheath, is considered the most problematic. Our subgroup analyses revealed most functional problems with injuries localized between the A4 and A2 pulleys (subzones 1C to 2C). Possible explanations may be simultaneous injury to the FDS chiasma, digital nerve(s) or proximal interphalangeal joint capsule; these correlations were not proven by our data. The pulleys could increase the resistance to gliding of the repaired tendon, especially if the surgeon tried to avoid releasing the A2 or A4 pulleys. The oedematous tendon could catch at the edge of the pulleys and hinder gliding, leading to adhesions or ruptures.
The results of flexor tendon repair in the little finger have been found to be inferior to other fingers (Elliot, 2002; Gault, 1987; Moriya et al., 2015). Orkar et al. (2012) compared zones 1 or 2 flexor tendon repairs in 60 index and 108 little fingers. They found significantly more proximal interphalangeal contracture in the little fingers in zone 1 injuries. Our results confirm that injury to the little finger is a negative predictor for the AROM in zone 1 and 2 injuries.
The use of stronger suture materials, stronger repair techniques, limited pulley release or ‘venting’ are widely recommended in the literature based on experimental evidence and clinical work (Amadio et al., 2005; Elliot and Giesen, 2013; Tang, 2007; Tang et al., 2014). We confirmed the role of these factors in the clinical setting. In our patients, the Yotsumoto-Dona suture and double Kessler suture gave better AROM than the standard modified Kessler suture. Two-strand sutures are generally considered mechanically insufficient (Wu and Tang, 2014); however, a biomechanical study found the Yotsumoto-Dona suture was strong enough for early active motion both for gapping and ultimate strength (Rigó et al., 2012). Other suture configurations were not used in our department.
The treatment of concomitant injured FDS tendons is controversial: three comparative studies have shown significantly better outcomes with simultaneous repair of both the FDP and FDS tendons (Lister et al., 1977; Moriya et al., 2015; Nielsen and Jensen, 1984), whereas others have not (Brunelli et al., 1983; Ikuta and Tsuge, 1985; Tang, 1994). We found resected or untreated complete division of the FDS tendon to be a significant negative predictor of the functional results.
Recent attention has been focused on the surgeon’s experience, which has been accepted as an important factor influencing the outcome of tendon surgery (Tang, 2009, 2013). In our department, the less experienced surgeons carried out the operations with the assistance of more experienced surgeons until judged sufficiently skilled. Hence, the highest level of experience in the operating team often exceeded the experience of the operating surgeon. We did not find the operating surgeon’s experience to be a significant predictor of the outcome.
Dy et al. (2012b) found 6% reoperations of 5229 flexor tendon repairs in a register study. They concluded that patients with increasing age and workers’ compensations were more likely to need reoperation, while those with concomitant nerve repair were less likely to undergo reoperation. Painful nerve injuries can interfere with mobilization and theoretically protect against rupture; however, we were unable to identify a correlation between concomitant nerve injury and the functional results.
Early active mobilization of the sutured tendon has become popular in recent years. Many therapists and patients find it easier to perform than the Kleinert-type rubber band mobilization (Amadio et al., 2005; Elliot and Giesen, 2013). Our subgroup analysis of pooled zone 1 and 2 repairs showed early active motion as a positive predictor of AROM at 8 weeks. However, our other models showed no superiority of early active motion with the method that we used. The early active motion in our patients in this report may be criticized as not being a true early active regime as there were rubber bands in place. Therefore, we cannot rule out that other early active motion protocols could be more effective. We also noted that the rates of excellent and good results in our series are generally lower than in many other recent reports (Moriya et al., 2015; Trumble et al., 2010). We assume the difference may relate to the use of rubber band traction, which prevent a true early active motion of the repaired digits. Many units no longer use rubber band traction (Tang et al., 2013).
Treatment of flexor tendon injuries requires teamwork and active participation of the patient in rehabilitation is mandatory. Cooperation is difficult to define and measure, so we could not include this important factor in our analysis.
The statistical method we used has limitations. An assumption for regression analysis is the independence of observations. We cannot assume that the results for each finger are totally independent in case of multiple finger injuries. However, we often observed different function or need for reoperation in different fingers in the same patients, implying some degree of independence. One should be cautious with generalization of the findings; it is difficult to apply the results on methods that were not used in our department. There is a distinction between including a variable in a statistical model and it having any clinical importance. For example, delay has a regression coefficient of −1.357 in model 6, which is statistically significant; the effect of delay was to decrease range of motion by 1° per day against the intercept of 212°. What it means for clinicians is that even when the delay is statistically significant, it is outweighed in importance by other variables, such as smoking, the type of tendon suture or patient age. The adjusted R-squared values of our statistical models are relatively low; there are other unknown predictor variables or interactions that could influence the models. As the highest R-squared value of our models was 0.471, we could not explain more than 47% of the variations in the observations; we have still much to learn.
We conclude that increasing age, smoking, injury localization between subzones 1C and 2C, injury to the little finger, the extent of soft tissue damage, concomitant skeletal injury, delay to surgery, repair technique, treatment of the tendon sheath/pulley system, treatment of the concomitant superficial flexor tendon injuries and the rehabilitation are the predictors of functional results after flexor tendon repair in zones 1, 2 and 3. We are unable to influence all of these factors, but based on our findings, we recommend patients stop smoking and surgeons use stronger surgical repair techniques than the Kessler repair, repair concomitant FDS tendon injuries, perform limited release of the pulleys if necessary and undertake early active motion rehabilitation to optimize the results of FDP tendon repairs.
Footnotes
Acknowledgements
The authors would like to thank the hand therapists of the Department of Physiotherapy and Occupational Therapy, Rikshospitalet, Oslo University Hospital for the thorough follow-up of the patients and the precise registration of the finger function.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved in advance by the local Ethical Committee.