
Abstract
Giant cell tumour of the distal radius is a locally aggressive lesion. In this study, we performed a wrist arthrodesis reconstruction with an ipsilateral double barrel segmental ulnar bone graft combined with a modified Sauve-Kapandji procedure for a giant cell tumour of the distal radius. From January 2007 to September 2013, we followed eight patients for a mean duration of 36 months. One patient developed a recurrence and was treated by amputation; the other seven patients achieved radiological union in about 8 months. There was no wrist instability, deformation or dislocation; the mean range of motion of the forearm achieved 75° of supination and 70° of pronation. The patients could recover reasonable grip strength. This new operative procedure can excise the tumour with a low rate of recurrence, fewer functional deficits and fewer complications than reported for other procedures.
Introduction
The prevalence of giant cell tumour (GCT) is higher in China and southern India, accounting for 5% of all primary bone tumours and 20% of benign skeletal tumours (Chakarun et al., 2013). Approximately 10% of all GCTs occur in the distal radius, which is the third most common location for a GCT (Harness and Mankin, 2004; Khan et al., 2004; Prosser et al., 2005). Treatment options include intralesional excision with or without adjunctive modalities (e.g. high-speed burring, cryotherapy and phenol, cementation with methyl methacrylate), en bloc resection followed by reconstruction or arthrodesis (Balke et al., 2008; Malek et al., 2006). For small lesions (Campanacci grade I) curettage and bone grafting or cementing is preferred, especially as it preserves the adjacent wrist joint. For grade II and III lesions or patients with a recurrence, these procedures are associated with high recurrence rates and en bloc resection is a better choice (Campanacci et al., 1987; Chadha et al., 2010).
There are several surgical procedures for wrist reconstruction following a wide resection, such as wrist arthrodesis or arthroplasty with an allograft, a vascularized or non-vascularized fibular autograft, ulnar translocation or a custom-made wrist prosthesis. However, reconstruction of the wrist after en bloc resection of the distal radius is still a challenging task with a high rate of complications, including donor site morbidity, non-union, fracture, wrist instability and dislocation (Damert et al., 2013; Legname et al., 2011).
The aim of this study was to report our experience with a relatively new surgical technique for wrist reconstruction following excision of a GCT.
Patients and methods
Patients
From January 2007 to September 2013, eight patients (five men, three women) underwent en bloc resection and reconstruction for a GCT of the distal radius. They had a mean age of 33 years (range 19–52). We treated five primary lesions and three recurrences. Two patients were classified with grade II tumours; and six were classified with grade III tumours, according to Campanacci’s radiological grading (Supplementary Figures S1 and S2). The diagnosis was confirmed by histological examination.
Surgical procedure
The key features were: an osteotomy approximately 3 cm proximal to the tumour; en bloc resection of the radius was done together with the surrounding soft tissues; preservation of 2 cm of the distal ulna; proximal to this distal segment, a segmental resection of the ulna, measured as twice the length deficit of the resected radius, was performed and a transverse osteotomy was made creating two equal lengths of ulna used as an intercalary bone graft from the proximal stump of the radial diaphysis to the proximal carpal row (Figure 1); the wrist was arthrodesed in about 20° and ulnar deviation of 10° with dorsal titanium reconstruction plate from the middle finger metacarpal to the radial diaphysis. Two cortical bone screws (Trauson Medical Instrument Co., Ltd, Jiangsu, China) were used to arthrodese the head of the ulna to the ulnar graft. An additional bone granule allograft (Anjiu Biotechnology Co., Ltd, Shanghai, China) was inserted at both ends of the ulna graft to enhance the fusion process. Postoperatively, the forearm was immobilized in a short-arm plaster cast for 6 weeks. All the operations were performed by surgeons of grade III.
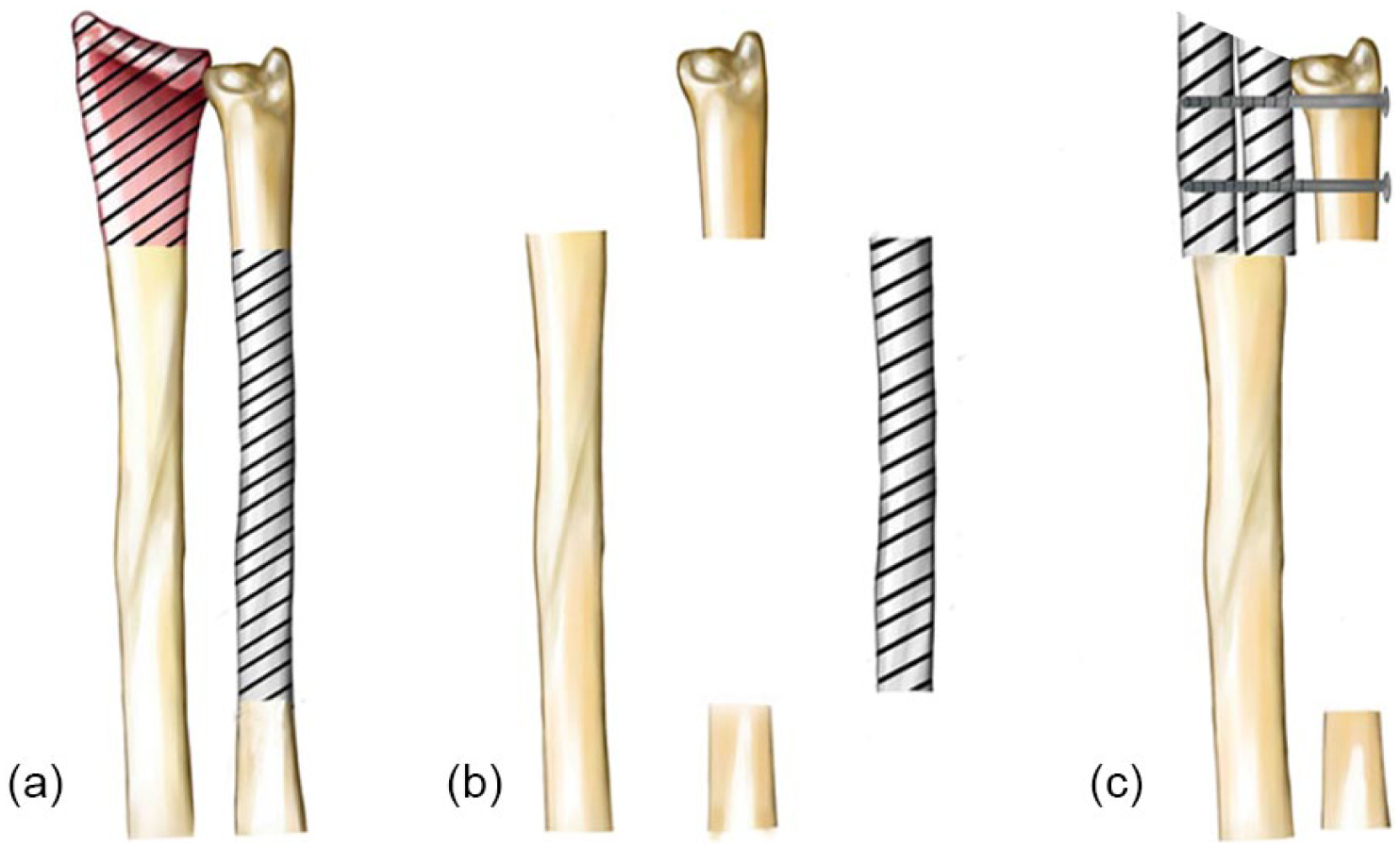
Schematic drawing of the wrist arthrodesis reconstruction of the distal ulna using an ipsilateral double barrel segmental ulna bone graft combined with the modified Sauve-Kapandji procedure. (a) The levels of radial and ulnar bone osteotomies are illustrated. (b) En bloc resection of the distal radius was performed together with a resection of a segment of the ulna about double the length of the distal radius resection. (c) This segment of ulna was divided into two sections of equal length and we placed them side by side to replace the distal radius we resected; they were fixed by two screws.
Postoperative management
Following removal of the plaster at 6 weeks, the patients were assessed for local recurrence by radiographs and magnetic resonance imaging (MRI) scan, complications, pain and the ability to work and perform daily activities every 3 months. Elbow assessment was performed through observing whether there were functional deficits and measuring ranges of flexion and extension. All measurements were compared with the opposite side. Functional evaluation of the patients was performed according to the most recent system of the Musculoskeletal Tumor Society. The Disabilities of the Arm, Shoulder, and Hand (DASH) score was evaluated for each subject preoperatively and 1 year postoperatively. In addition, chest computed tomography (CT) scans were performed every year postoperatively.
This study was approved by the Institutional Review Board of Shandong Provincial Hospital Affiliated to Shandong University.
Results
The patients were followed for a mean of 36 months (range 10–62). All patients regained full elbow movement. The mean range of motion of the forearm was 75° of supination and 70° of pronation (Figure 2). Grip strength was a mean of 31 kg (range 20–42), reaching a mean of 71% of the preoperative grip strength (mean 44; range 35–56 kg). The mean Musculoskeletal Tumor Society score was 25 (range 23–27). The mean DASH score was 39.2 of preoperatively and 48.9 postoperatively. None of the eight patients developed pulmonary metastasis. We did not observe any functional deficits in the elbow joints. One patient with tumour recurrence underwent amputation in the proximal forearm 2 years postoperatively. The other seven patients were evaluated and achieved radiological union (Figure 3) at a mean of 8 months (range 5–12).
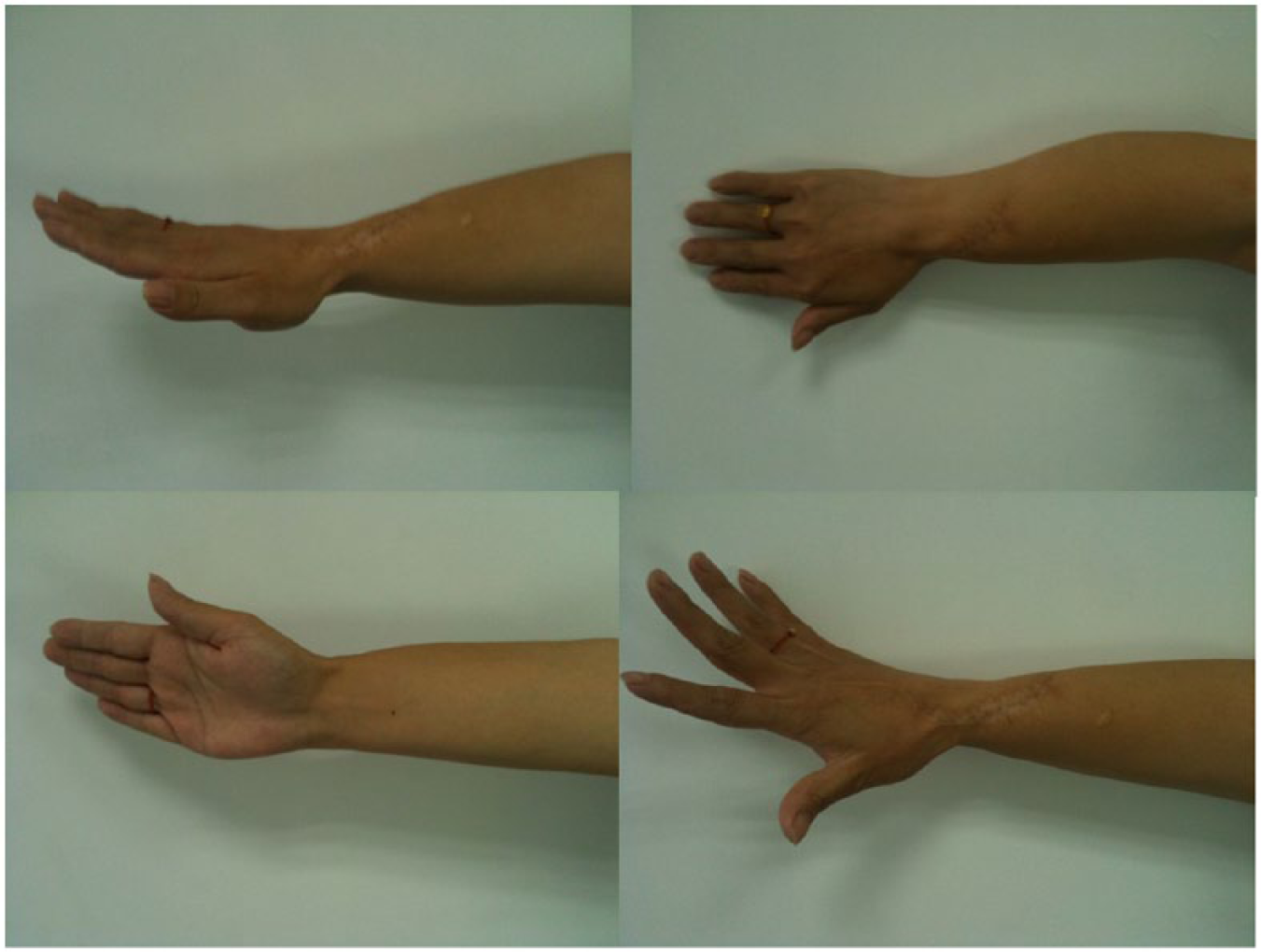
Excellent range of forearm rotation was observed postoperatively.
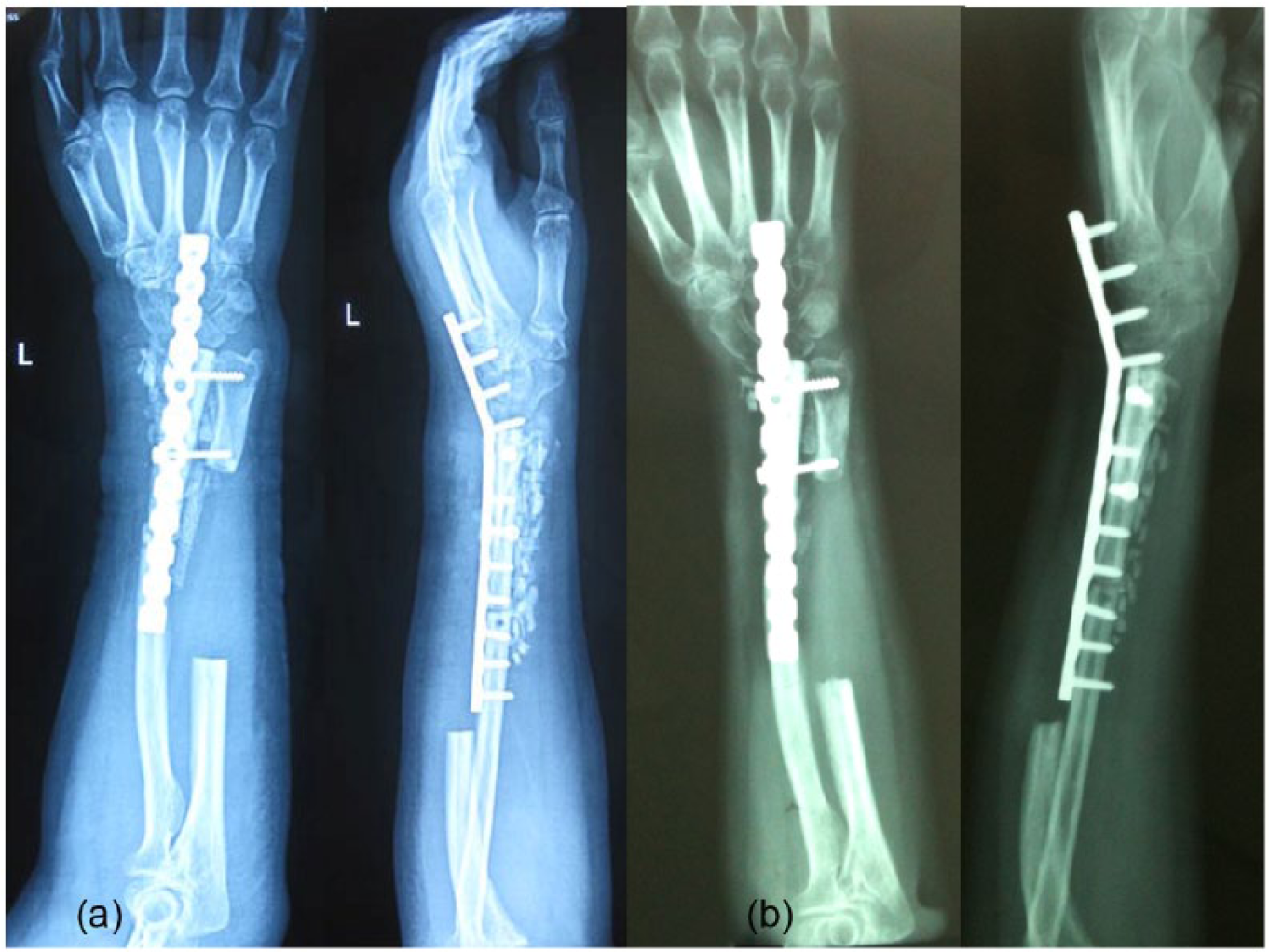
The anteroposterior and lateral radiographs of (a) one month postoperative (b) six months postoperative.
Discussion
A GCT of bone is a benign, locally aggressive disease with a high tendency for recurrence and a low rate of pulmonary metastasis (Humail et al., 2014; Kawamura et al., 2009; Oh et al., 2006). When the tumour is located in the distal radius, it has been reported to be more aggressive; the rate of recurrence is high (Liu et al., 2012). The primary aims of treating a GCT of the distal radius are to remove the tumour completely and to preserve forearm function.
Treatment by en bloc resection and reconstruction of the bone defect following tumour removal is challenging. The prime objective is cure; the secondary objective is the preservation of as much function as possible. A number of techniques have been used for reconstruction, such as a wrist arthrodesis or arthroplasty with an allograft, a vascularized or non-vascularized fibular autograft, ulnar translocation or a custom-made wrist prosthesis (Duan et al., 2013; Peng-Fei and Yu-Hua, 2011; Saikia et al., 2010; Zhu et al., 2013). Although the outcomes of these reconstructions are promising, complications have been described. Chadha et al. (2010) reported on nine patients who underwent autogenous non-vascularized fibula reconstruction. Two developed a fibular graft fracture following trauma, one developed postoperative tourniquet palsy, one developed subluxation of the wrist joint and one suffered a recurrence (Chadha et al., 2010). Zhu et al. (2013) reported on a partial wrist arthrodesis in seven patients and arthroplasty in seven other patients for a distal radius GCT using autologous proximal fibular grafts. All 14 patients reported no pain but had functional impairment with moderate activity. In the arthroplasty group, two patients developed wrist subluxation and four developed degenerative changes; in the arthrodesis group, only one patient suffered a radial fibula fracture following removal of the plate following an injury (Zhu et al., 2013).
Chalidis and Dimitriou (2008) reported an ulnar translocation technique for the treatment of GCTs of the distal radius to improve wrist stability and bone union, but the postoperative cosmetic result was poor and the translocated ulna was too thin to withstand the stresses of strenuous activities (Chalidis and Dimitriou, 2008). Nakagawa et al. (2003) noted that the Sauve-Kapandji procedure allowed the patients to achieve good forearm rotation and grip strength and satisfactory postoperative cosmetic results. Jakob et al. interpreted the wrist as consisting of three distinct columns (the radial column, the intermediate column and the ulnar column), each of which is subjected to different forces, and so must be addressed as discrete elements (Jakob et al., 2000). When three columns remain intact, the wrist can be more powerful (Supplementary Figure 3).
Our study also had some limitations: the number of patients was small owing to the rarity of the condition even in China; the follow-up was inadequate to report on the long-term results; and it was retrospective. Nevertheless, even with these limitations, we obtained good results. All eight patients achieved good bone union in an average of 8 months (except one patient who developed a recurrence) and none of them subsequently developed pulmonary metastases. There were no incidents of pain according to the patients’ description; no wrist instability, deformation or dislocation according to imaging. The patients achieved reasonable forearm rotation and 71% of preoperational grip strength. Although bone union would probably have been quicker with a vascularized bone graft, it is technically more demanding.
In conclusion, our study suggests that tumour resection and arthrodesis of the wrist and distal ulna using an ipsilateral double barrel segmental ulna bone graft combined with the modified Sauve-Kapandji procedure is an efficient and reasonably straight-forward technique for the treatment of a distal radius GCT.
Footnotes
Acknowledgements
We thank all patients participated this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board of Shandong Provincial Hospital Affiliated to Shandong University. Written informed consent was obtained from all patients.
Funding
This study was supported by grants from National Natural Science Foundation of China [No.81201441].