
Abstract
We evaluated the outcomes of ulnar translocation with T-locking plate fixation and ulnoscapholunate arthrodesis after distal radius resection for giant cell tumours. Eighteen patients (median age 33 years) were included, with a median follow-up of 72 months. The mean Musculoskeletal Tumour Society score was 27, demonstrating excellent function in all patients. The mean grip strength was 82% of the opposite hand. Supination and pronation were 77° and 76°, respectively. Wrist flexion and extension averaged 23° and 21°, respectively. The mean radial and ulnar deviations were 21° and 15°, respectively. Ulnoscapholunate union occurred in all patients within 3 months of surgery. Radioulnar union occurred in 17 patients within a mean of 4 months. One patient required revision surgery owing to plate breakage and radioulnar nonunion. Two patients had local recurrences. These results suggest that ulnar translocation is a reliable reconstruction method for giant cell tumour resection in the distal radius.
Introduction
Giant cell tumour (GCT) of bone is the third most common primary bone tumour, accounting for approximately 5% of all primary bone tumours (Jha and Chaudhary, 2023; Sullivan et al., 2023). Roughly 12% of GCTs of bones occur in the distal radius (Campanacci et al., 1987; Sullivan et al., 2023). Treatment typically involves intralesional curettage with defect filling using bone cement or bone graft, which helps preserve function (Jamshidi et al., 2018). However, compared with other locations, the distal radius has been associated with a higher incidence of local recurrence following the intralesional treatment. This is probably due to the bone’s shape and proximity to joints and critical structures (Wysocki et al., 2015), especially in Campanacci grade 3 cases, where cortical breakdown and soft tissue involvement are present (Srikanth et al., 2022; Sullivan et al., 2023), as well as in some grade 2 cases where the bony architecture and cortical thickness are inadequate following intracapsular curettage.
En bloc resection is a well-established procedure for the surgical treatment of aggressive GCT of bone, offering a lower incidence of local recurrence compared with intralesional approaches (Jamshidi et al., 2021b). Various methods have been developed for reconstructing the distal radius following tumour resection. These include reconstructing the resected distal radius by vascularized and nonvascularized fibular grafts, allografts, prosthetic or custom implants and hemiarthroplasty (Chobpenthai et al., 2023). Ulnar translocation is an alternative surgical approach that involves shifting the ulna towards the radius to fill the void left by distal radius resection. The proximal end of the ulna is fixed to the radial diaphysis, and a wrist arthrodesis is performed distally. This reconstructive procedure provides structural support without requiring bone grafts or prosthetic replacements (Agrawal et al., 2021; Kundu et al., 2025). Each method offers distinct advantages and challenges (Chobpenthai et al., 2023).
The technique of ulnar translocation is straightforward and provides stable support, making it a practical choice for patients with aggressive distal radius GCTs (Agrawal et al., 2021; Kundu et al., 2025). This approach uses the patient’s own bone, offering a biological solution that promotes timely union. Although this technique provides almost full rotation of the forearm, its main drawback is that it does not allow wrist flexion, extension and radial and ulnar deviation, which may be emotionally and functionally important to the patient. To address this limitation, ulnar translocation with ulnoscapholunate arthrodesis was introduced by Seradge (1982), using an intramedullary Steinmann pin for fixation of the translocated ulna to the carpus and proximal radius.
In patients with local recurrence previously treated by curettage via the palmar approach, we performed ulnolunate arthrodesis using a narrow locking plate through the same approach to minimize additional scarring. The outcomes of this technique were reported in our earlier study (Jamshidi et al., 2020). During the same period, for new cases of distal radius GCT that required en bloc resection, we used a dorsal approach to accommodate a T-plate, which provided additional fixation points to facilitate ulnoscapholunate arthrodesis. We hypothesized that ulnoscapholunate arthrodesis with a dorsal T-locking plate offers greater early and delayed stability, thereby reducing the risk of nonunion.
This study aimed to evaluate the functional outcomes, complications, and oncologic control after ulnar translocation and ulnoscapholunate arthrodesis via a dorsal approach, with fixation using a T-locking plate, following en bloc resection of GCT of the distal radius.
Methods
This study received approval from our institutional review board. We conducted a retrospective review of the medical records of patients who underwent surgical resection of a GCT of the distal radius with subsequent reconstruction using ulnar translocation between 1992 and 2022. Indications for this procedure included Campanacci grade 2 or grade 3 lesions (Campanacci et al., 1987) where intracapsular curettage was deemed unsuitable owing to compromised bony architecture and cortical thinning. Patients were included if they had primary GCT of the distal radius and were treated with translocated ulna and ulnoscapholunate arthrodesis stabilized with a T-plate through a dorsal approach with a minimum follow-up of 2 years. The eight patients with recurrent GCT were excluded from the study. Additionally, two patients who underwent total wrist arthrodesis and one patient who was lost to follow-up were also excluded. Eighteen patients were included in the final analysis (Figure 1). In all patients, the diagnosis of GCT was confirmed with a core needle biopsy via a dorsal approach.
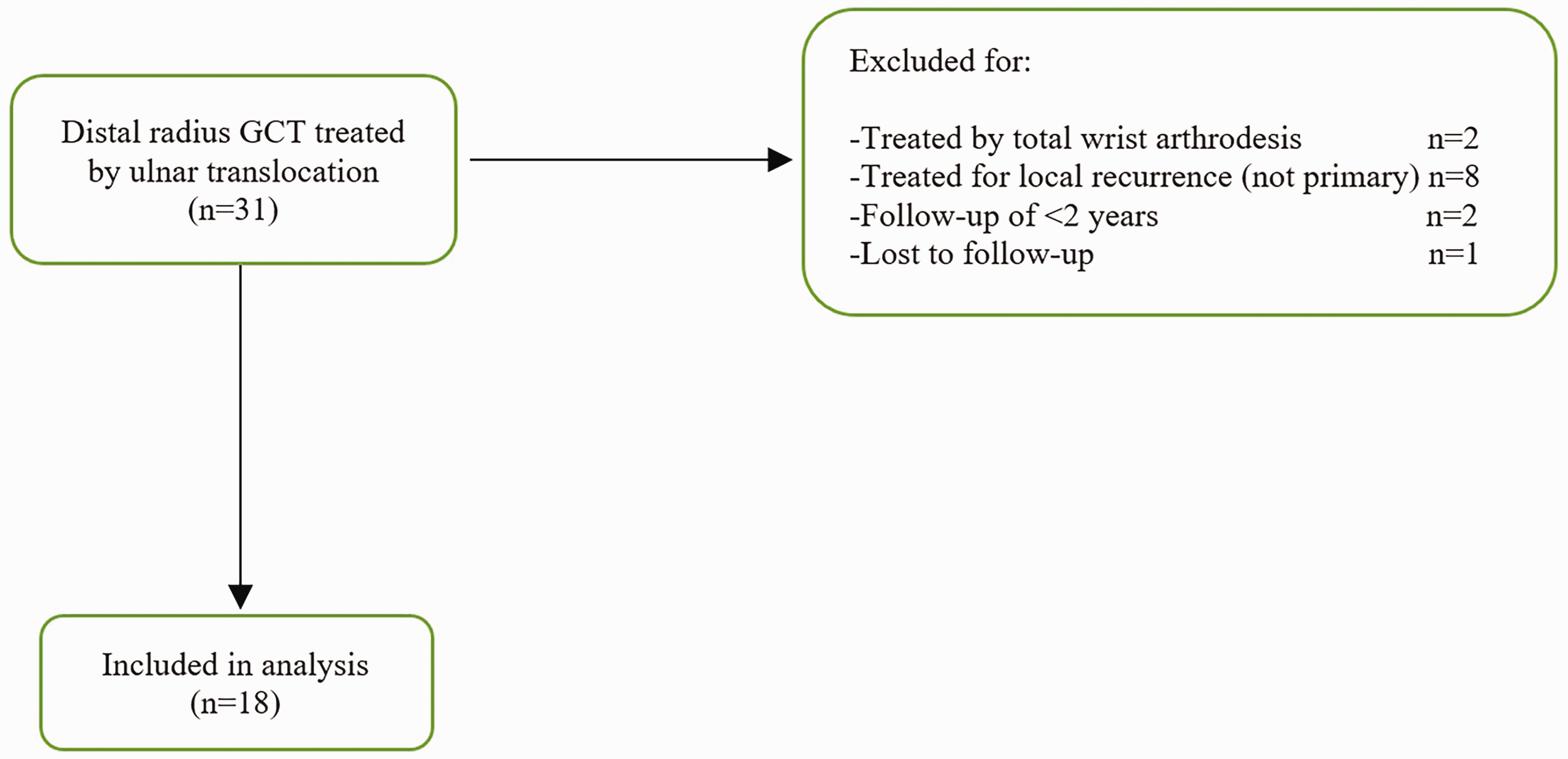
Flowchart illustrating the principles of inclusion and exclusion.
Surgical technique
All surgeries were performed by a musculoskeletal tumour surgeon (KJ) with level 5 expertise, as defined by Tang and Giddins (2016). Patients were positioned supine with the upper extremity on an arm board, and a pneumatic tourniquet was applied to the upper arm. The forearm was fully pronated, and a dorsal longitudinal incision was made, beginning 1 cm proximal to the base of the third metacarpal and extending across the wrist to 5 mm medial to Lister's tubercle. This incision encompassed the biopsy tract and continued proximally along the lateral border of the extensor digitorum communis tendon compartment, with the length determined by the planned resection of the distal radius.
To access the distal radius, the extensor retinaculum over the third and fourth compartments was incised longitudinally. The extensor pollicis longus tendon was retracted radially, and the extensor digitorum communis was retracted ulnarly. The centre of the dorsal radius was marked with cautery to maintain rotational alignment. Based on preoperative T1-weighted MRI, a proximal osteotomy of the radius was performed with a 1 cm margin. The distal radius was elevated, and dissection proceeded distally to ensure the complete removal of the interosseous membrane, surrounding soft tissue, and the pronator teres as needed to achieve clear margins. These structures were excised intra-articularly. Caution was taken to preserve the radial artery and the sensory branch of the radial nerve. The proximal portions of the scaphoid and lunate bones were excised with a narrow-blade oscillating saw, creating an appropriate bed for the translocated distal ulna. The ulna was cut distally at the midpoint of the radioulnar joint and proximally at the necessary level. To preserve wrist aesthetics and avoid wrist narrowing, the triangular fibrocartilage and distal ulna remnant within the radioulnar joint were retained without any surgical procedure. The wrist was positioned in 15° of extension. A 2.5 mm pin was drilled retrograde from the ulnar side of the scaphoid towards the third metacarpal, exiting through the palm of the hand (Figure 2(a)). The pin that protruded from the palm was then drilled proximally through the aligned ulna and into the radial shaft. The ulna was gently pulled laterally towards the radius with a towel clip to maintain its blood supply during translocation. After application of the T-plate, this alignment pin was removed.
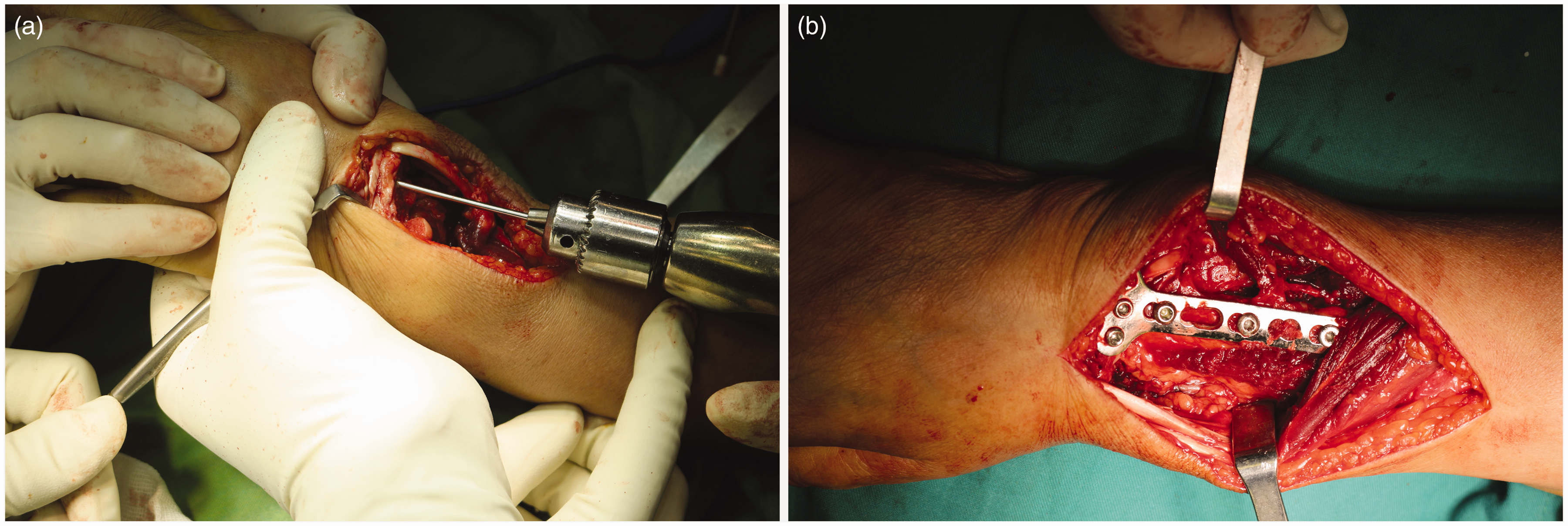
Intraoperative photograph showing (a) the retrograde insertion of the alignment pin and (b) the application of the plate.
A Safety Lock T-Plate 3.5 Right Angled (PEAK Surgical, Inc., Palo Alto, CA, USA) was used for dorsal fixation of both osteotomy sites. The initial locking screw was placed on the medial side of the scaphoid, followed by the alignment of the plate along the radial shaft to span the translocated ulna. A screw was inserted into the radius shaft, and the short arm of the plate was secured with two additional screws, one on the lateral side of the scaphoid and another on the lunate. Fixation was completed by inserting one or two screws into the translocated ulna and three or four additional screws into the radial diaphysis, depending on the bone quality (Figure 2(b)). The extensor retinaculum was repaired using a non-absorbable suture to avoid bowstringing.
Postoperative protocol and follow-up
The wrist and forearm were immobilized in an anterior splint. The day after surgery, patients were instructed to begin active and passive range of motion (ROM) exercises for their fingers. After 3 weeks, patients were asked to remove the splint and initiate active ROM exercises for the wrist, which were to be performed three times daily. The splint was completely removed once radiographic evaluations confirmed union at both junctions, at which point physical therapy was initiated. Radiographs were obtained every 6 weeks to monitor the union of both ends of the translocated ulna. Follow-up visits were scheduled every 3 months for the first 2 years, then every 6 months for the next 3 years, and annually for up to 10 years thereafter. During these visits, patients received clinical and radiographic evaluations of the chest and reconstructed area to assess any surgical or oncological complications.
Outcome measures
Outcomes were collected at the end of each follow-up visit. Functional outcomes were assessed using the Musculoskeletal Tumour Society (MSTS) score for the upper extremities, which consists of six subscales: pain, function, emotional impact, hand positioning, dexterity, and lifting ability, each scaled from 0 to 5. This yields a total score ranging from 0 to 30, where higher scores reflect better limb function (Enneking et al., 1993). The results were classified as excellent for MSTS scores ≥23, good for scores from 15 to 22, fair for scores from 8 to 14, and poor for scores <8 (Mohler et al., 2010). The total score can be transformed to a point scale of 0–100 (Rizzo et al., 2024). Additionally, patient-reported outcomes were recorded, including experiences of pain, return to previous employment and overall satisfaction with the appearance of the wrist. The wrist ROM was measured with a goniometer, while grip strength was assessed using a hand dynamometer, with results compared with those for the opposite wrist. Surgical complications were extracted from the patient’s records. Union was defined as the complete obliteration of the junction, the presence of periosteal sclerosis or the formation of callus at either end of the translocated ulna on radiographs (Jamshidi et al., 2021a). Bony union was independently evaluated by two fellowship-trained orthopaedic oncologists who had no involvement in the patient’s care. In cases where the two evaluators disagreed, the senior author resolved the issue.
Statistical analysis
The Kolmogorov–Smirnov test was employed to assess the normality of the distribution of descriptive data. Numerical variables following a normal distribution were reported as means and standard deviations (SD), while those with a non-normal distribution (age and follow-up) were presented as medians and interquartile ranges (IQR). Categorical variables were summarized as frequencies and percentages.
Results
Baseline characteristics
The patients included in this study consisted of 12 women and six men with a median age of 33 years (IQR 10.5; range 16–47). The tumour was located on the dominant side in 12 patients and on the non-dominant side in six. The lesion was Campanacci grade 2 in four and grade 3 in 14 patients. The mean resection length was 6 cm (SD 2; range 5–8). The pathology reports indicated free surgical margins for all specimens. The median follow-up of the patients was 72 months (IQR 40; range: 24–120).
Functional and oncologic outcomes
The mean wrist supination was 77° (SD 8; range 70–85) and pronation 76° (SD 7; range 70–85). The mean wrist flexion was 22° (SD 9; range 10–35) and extension 23° (SD 8; range 10–30). The mean radial deviation was 21° (SD 8; range 10–30) and ulnar deviation 15° (SD 7; range 10–25). The grip strength of the injured hand averaged 82% of the non-injured hand (range 70–90). The mean MSTS score of the patients was 27 (SD 1; range 26–28). On a score of 100, a mean MTS of 90 was obtained. Accordingly, all patients had excellent limb function. None of the patients reported pain in the last follow-up. All patients returned to their previous jobs. All patients, excluding two, were satisfied with the appearance of their distal forearm (Figure 3). All patients experienced limitations in vigorous recreational activities.

Photograph of both wrists of a 33-year-old woman comparing the reconstructed wrist to the normal side 2 years postoperatively.
None of the patients experienced lung metastasis. Two patients experienced local recurrences, both in the anterior soft tissue, 18 and 24 months after surgery. The recurrences were treated with excision.
Radiological outcomes and complications
Union at the ulnoscapholunate junction was achieved in all patients within 3 months. Radioulnar union occurred in 17 patients, with a mean duration of 16 weeks (SD 3; range 12–24) (Figure 4). One patient experienced radioulnar nonunion with plate fracture at 36 weeks. This complication was managed by inserting a new T-plate, strengthening the fixation with a narrow locking plate, and applying an autogenous bone graft harvested from the ilium (Figure 5). Patients generally did not report any issues with the remnant of the proximal ulna. However, one patient experienced a snapping sensation in the distal third of the forearm during supination and pronation. The patient tolerated this sensation without the need for intervention. Additionally, radiological examination in a different patient, 7 years after the operation, showed asymptomatic narrowing in the second, third and fourth carpometacarpal joints, while it was absent on preoperative radiographs. In four patients, two non-locking screws were palpable in the distal quarter of the dorsal side of the forearm. Despite the presence of protruding screws, patients reported no tenderness or tendon irritation and showed little desire to have the hardware removed.
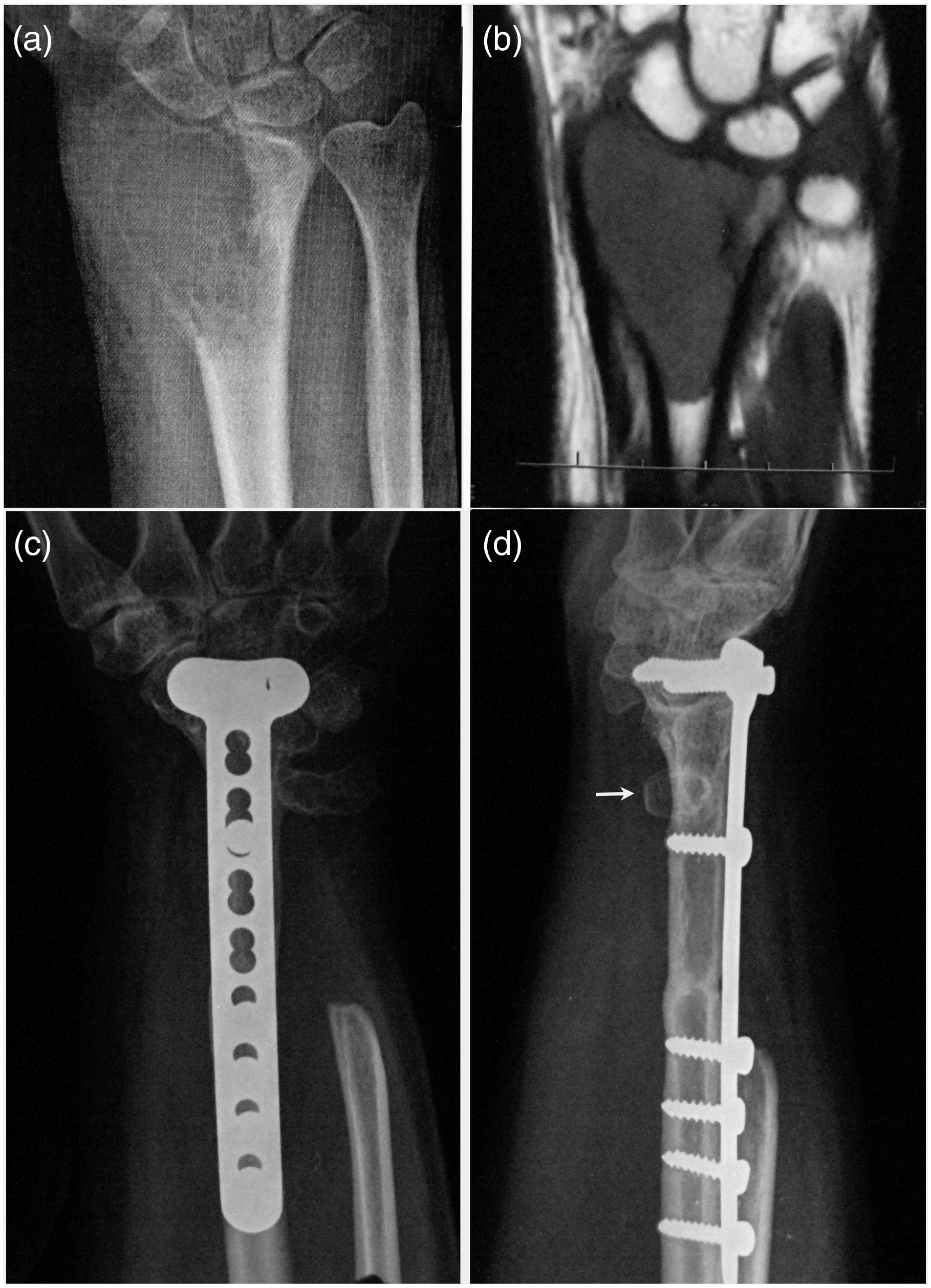
(a) Preoperative posteroanterior radiograph of the wrist of a 34-year-old woman with a stage 3 giant cell tumour of the distal radius; (b) preoperative T1-weighted coronal MRI displaying the medullary extension and (c, d) postoperative posteroanterior and lateral radiographs demonstrating solid union at the radius and ulnar junction, along with the remnant of the distal ulna (white arrow).
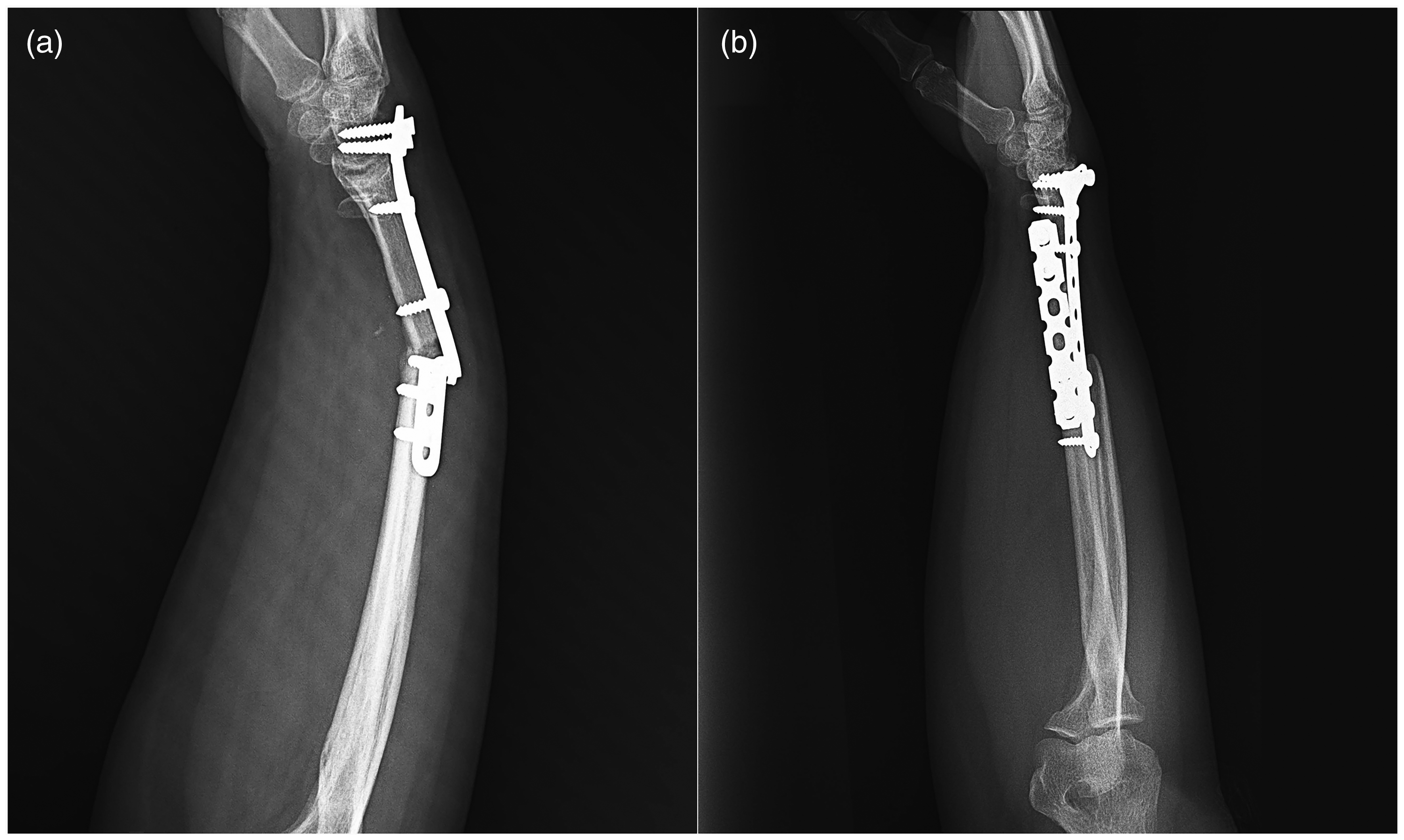
(a) Lateral radiograph of the distal radius 9 months after the resection of stage 3 giant cell tumour and reconstruction with ulnar translocation, showing evidence of nonunion and a fracture of the plate and (b) lateral radiograph of the same patient after application of a new T-plate, and a narrow locking plate, and autogenous bone graft.
Discussion
In this study, we evaluated the outcomes of reconstruction of the distal radius using ulnar translocation and ulnoscapholunate arthrodesis with a T-locking plate following en bloc resection for aggressive GCT. At a median follow-up of 72 months, all patients had excellent functional outcomes based on the mean MSTS score. Grip strength averaged 82% of that of the uninjured hand. The mean wrist range of motion included 77° supination, 76° pronation, 22° flexion, 23° extension, 21° radial deviation and 15° ulnar deviation. Notably, no patients reported experiencing postoperative pain. Two patients had local recurrences in soft tissue and one patient required revision surgery owing to radioulnar non-union.
Salunke et al. (2017) reported the results of ulnar translocation and total wrist arthrodesis in 25 patients with distal radius GCT with a mean follow-up of 23 months. The mean MSTS score was 24. Grip strength in the affected hand was reported as good in 17 patients, average in seven and not assessed in one patient when compared with the contralateral hand. One patient experienced non-union at the radioulnar junction. The mean time to bone union was 6.5 months at the ulna to radius junction and 4.5 months at the ulna to carpal junction. An excellent range of pronation and supination was observed in all patients. In the present study, the functional outcomes, including MSTS scores and grip strength, tended to be better than those reported by Salunke et al. (2017).
Kundu et al. (2025) treated 16 patients with GCT of the distal radius using ulnar translocation and total wrist arthrodesis. At 2 year follow-up, the mean MSTS score was 23. Grip strength exceeded 75% of the healthy site in seven of the 16 patients. The mean modified Mayo Wrist score improved from 21 before the operation to 61 after 2 years. Radioulnar nonunion was reported in two patients. The mean radioulnar and ulnocarpal union times were 23 and 18 weeks, respectively. The mean time to radioulnar and ulnoscapholunate union was less in the present study (16 and 12 weeks, respectively).
Seradge (1982) reported the functional outcomes of two patients with GCT of the distal radius who were treated by en bloc resection and reconstructed by ulnar translocation with partial wrist ulnoscapholunate arthrodesis fixed with Steinmann pins. In comparison with the opposite wrist, 85% of supination/pronation and 10°/20° flexion/extension of the wrist were obtained. Raju et al. (2021) reported five cases of ulnar translocation with ulnoscapholunate arthrodesis following the resection of GCT of the distal radius. They fixed the ulna to the scaphoid and lunate using multiple K-wires. At a mean follow-up of 60 months, the mean MSTS score for four patients was 83%, while one patient underwent amputation owing to extensive local recurrence. The average union time at the radioulnar junction was 4–5 months, and at the ulnocarpal joint, it was 3–4 months. This study did not report wrist ROM. We previously reported outcomes of ulnar translocation by preserving some degrees of wrist flexion and extension through ulnolunate arthrodesis in eight patients with recurrent GCT, using a narrow compression plate for fixation (Jamshidi et al., 2020). In that study, mean wrist extension and flexion were 30° and 10°, respectively. The mean wrist supination and pronation measured 74° and 78°, respectively. The mean grip strength was 64% of that in the contralateral hand. The mean MSTS score was 26. Ulnocarpal and radioulnar union were achieved in all patients at 5 and 7 months, respectively. In the present study, we used a T-shaped locking plate. The functional outcomes were comparable with the earlier study by Jamshidi et al. (2020). However, the ulnocarpal and radioulnar union times were shorter in the present study (3 and 4 months, respectively). This improvement could be attributed to the better biomechanical stability provided by the T-plate.
Wide resection and reconstruction with distal radial osteoarticular allografts, as well as various prostheses such as unipolar, complete wrist and 3-D-printed models, are the most commonly used surgical techniques for distal radius GCT (Zoccali et al., 2022). Reconstruction with allografts and custom-made prostheses has demonstrated pooled MSTS scores of 79 and 82%, respectively (Zoccali et al., 2022). However, these procedures were associated with a high number of surgical revisions (Chobpenthai et al., 2023). In the present study, partial wrist arthrodesis with T-plate fixation was associated with comparable rates of recurrence, revision and functional outcomes, along with reduced morbidity. Therefore, it may be considered a valuable alternative to allograft or prosthetic reconstruction in patients with aggressive GCT of the distal radius.
The current study has several limitations. Its retrospective design and relatively small patient population restrict the generalizability of the findings. There were no validated patient-reported outcome measures, such as the Disabilities of the Arm, Shoulder, and Hand score. Additionally, the exclusion of patients and lost to follow-up may introduce selection bias. Another limitation is the absence of a control group, such as patients receiving the traditional ulnar translocation technique with total wrist arthrodesis or another type of treatment. Therefore, in the future, prospective multicentre studies with larger patient populations are essential to validate these findings and further optimize the technical parameters.
Footnotes
Declaration of conflicting interests
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethics approval
This retrospective study was approved by the review board of Bone and Joint Reconstruction Research Center, Iran University of Medical Sciences.
Funding
None.