
Abstract
We present our first cadaveric test results of a three-dimensional printed patient-specific scaphoid replacement with tendon suspension, which showed normal motion behaviour and preservation of a stable scapholunate interval during physiological range of motion.
Keywords
Introduction
Treatment options when the scaphoid cannot be reconstructed or preserved, for example after a multifragmentary fracture, avascular necrosis (Preiser’s disease) or failed reconstruction are limited to salvage procedures, such as partial and total wrist fusion or proximal row carpectomy (Herbert, 1991).
An alternative option is the implantation of partial or total scaphoid replacements that have been made of silicone, acrylate, metal or pyrocarbon (Pequignot et al., 2000; Picaud, 1953; Swanson, 1970; Swanson et al., 1997). Waugh and Reuling (1945) first reported on the short-term outcome after implantation of a scaphoid replica made of a cobalt–chromium–molybdenum alloy (Vitallium) as a placeholder in two patients. A 43-year follow-up after Vitallium replica implantation in one patient was reported by Leslie et al. (1991), with good pain relief during the first 5 years before carpal collapse and painful radio-carpal arthritis developed. The silicone replacement described by Swanson (1970) fractured and led to foreign body reactions in many cases (Kleinert et al., 1985). The titanium spacer introduced by Swanson et al. (1997) was stabilized by a distal pole beak placed in a bony channel in the trapezium and a trans-prosthetic suture to the lunate. However, dislocations occurred, and carpal collapse and progression of arthritis was not prevented (Spingardi and Rossello, 2011). Being pure spacers without any ligamentous suspension, none of these implants can be expected to prevent carpal collapse. Nor do they replicate the original individual shape of the scaphoid, which may have a negative influence on carpal kinematics and stability (Fogg, 2004).
This study reports on preliminary cadaveric testing results of a near anatomical patient-specific scaphoid replacement and with flexor carpi radialis tendon suspension to reconstruct the scaphotrapezial and scapholunate ligaments in an attempt to overcome some of the disadvantages of previous replacements.
Methods
Specimen and design of the prosthesis
A cadaveric Thiel-conserved wrist was provided by the local Department of Anatomy for testing. The specimen showed no evidence of radio- or intra-carpal pathology on computed tomography (CT). A three-dimensional (3D) model of the scaphoid was generated and modified using computer-aided design software (Mimics®, Materialise, Leuven, Belgium and 3DS Geomagic Freeform®, Rock Hill, SC, USA) (Figure 1). The technique used especially for the scaphoid has been recently described by ten Berg et al. (2018).
Palmar and dorsal view of the scaphoid prosthesis.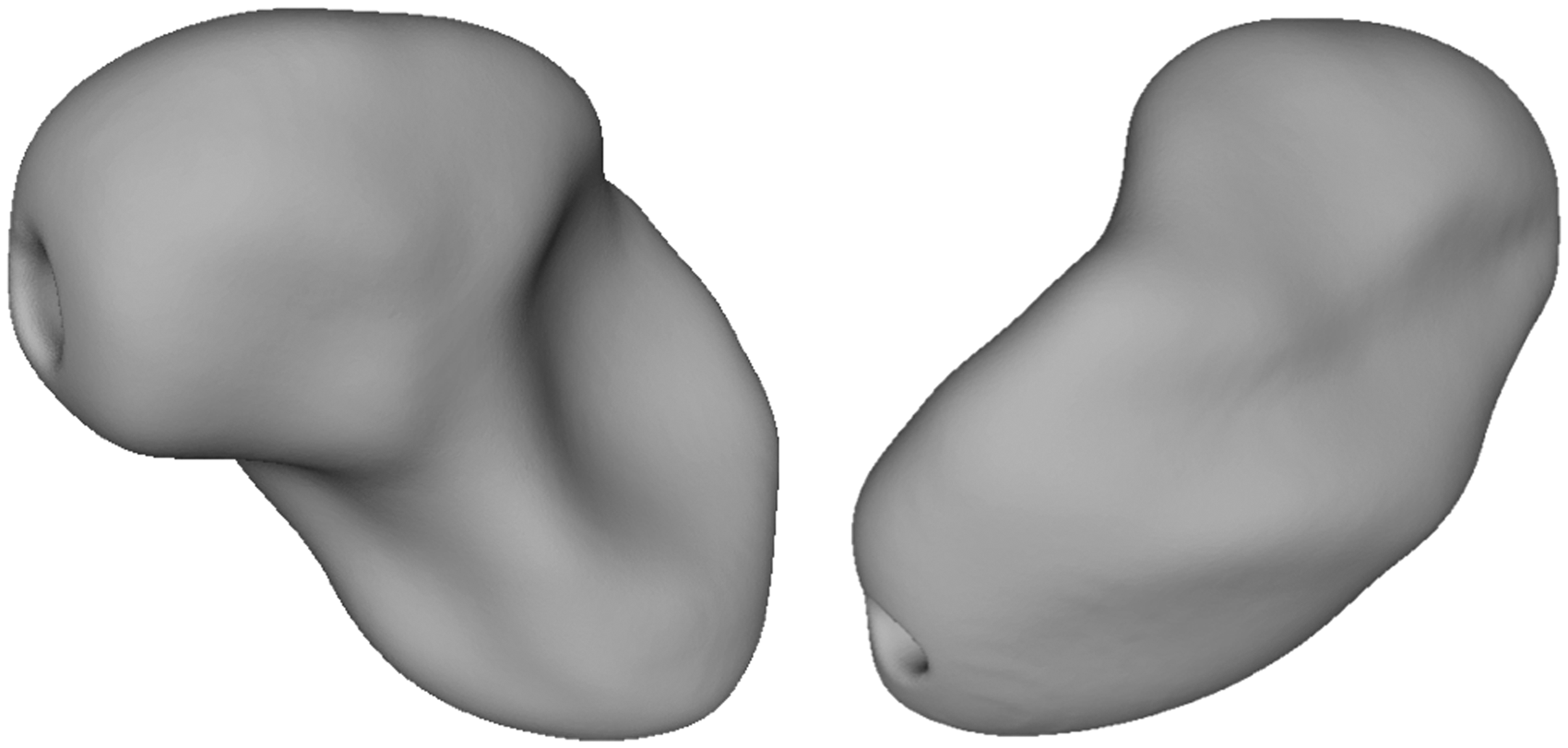
A channel was placed through the scaphoid based on the various techniques of scapholunate ligament (SLL) reconstruction (Brunelli and Brunelli, 1995). The channel was made in a curved fashion between the proximal and distal poles along the axis of the scaphoid to aid stability by providing the maximum amount of material between the channel and the outside surface (Figure 2). The distal palmar pole was flattened, and the edges of the inlet and outlet were smoothed to prevent tendon irritation.
The channel in the axis of the scaphoid.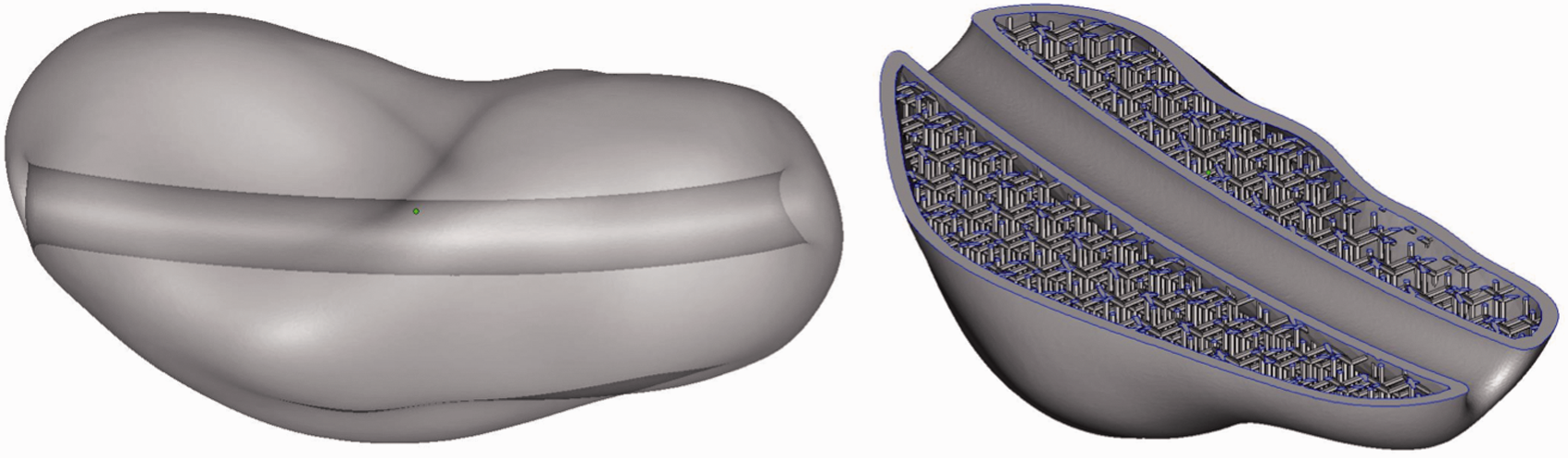
3D-printed aluminia ceramic has not been described for the use of patient-specific implants. However, Taniguchi et al. (2015) presented good clinical results for a talar replacement made of milled aluminia ceramic, which encouraged us to use the same material in a 3D-printed fashion (Figure 3).
Radial and ulnar views of the 3D-printed scaphoid prosthesis.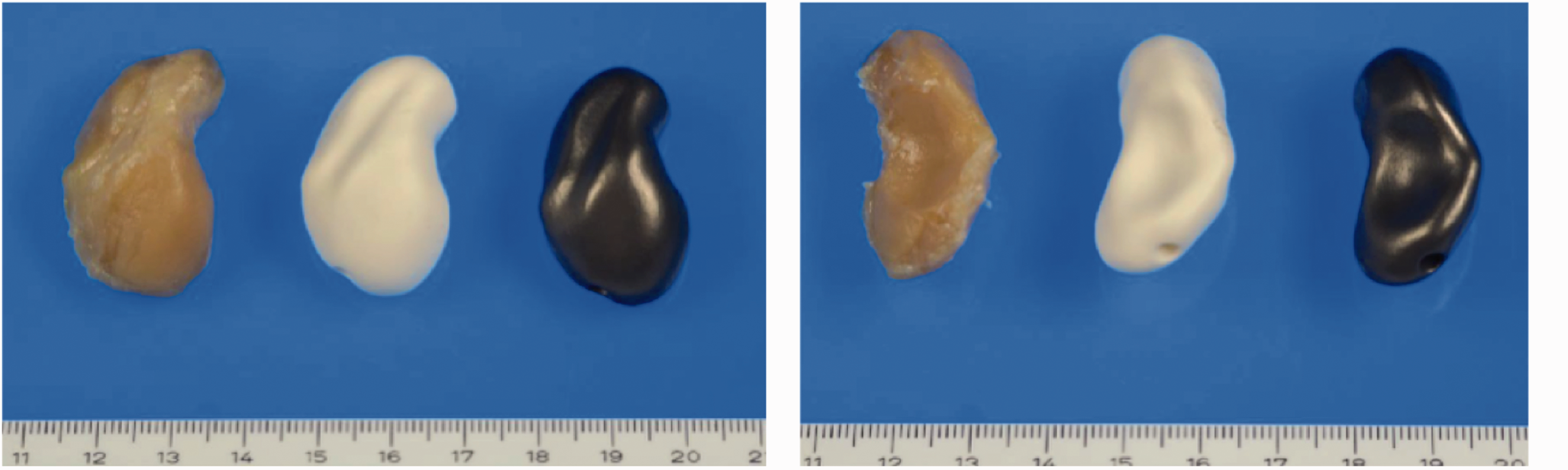
Quality assessment of the prosthesis
For quality assessment, the geometrical accuracy of the three-dimensional data of the implanted prosthesis was compared with the original scaphoid using the GOM Inspect 2016 freeware (GOM GmbH, Braunschweig, Germany). Differences between these three-dimensional surfaces are displayed in a colour-coded fashion.
Surgical technique
The original scaphoid was removed and replaced by the prosthesis. A distally based third of the flexor carpi radialis tendon was harvested and pulled through the tunnel in the prosthesis, then passed back to the palmar side through a sagittal drill hole in the lunate, where it was sutured back to its origin (Figure 4). This technique suspends the prosthesis and reconstructs the dorsal and palmar aspects of the SLL and the palmar scaphotrapezial ligaments (STL) (Corella et al., 2013; Henry, 2013).
Technique of implantation and fixation of the prosthesis with the flexor carpi radialis tendon.
Static CT motion analysis
Individualized thermoplastic splints (Ezeform®, Performance Health, Warrenville, IL, USA) in five predefined positions (neutral, maximal flexion, extension, radial and ulnar inclination) were made for the wrist by the chief occupational therapist (Figure 5). A CT scan of the wrist in each of the splints was then obtained to assess excursions of the original scaphoid and the prosthesis.
Cadaver forearm placed in the splint for CT scans.
Reproducibility of wrist positioning in the splints was assessed by comparing the angles of the longitudinal axes of the third metacarpal and the distal radius in the coronal and sagittal planes.
Motion patterns of the scaphoid and the prosthesis were assessed by comparing the 3D models of the wrist with the prosthesis to those of the original scaphoid in all positions. For this purpose, the 3D model of the wrist with prosthesis was compared with the one with the original scaphoid using the GOM Inspect 2016 freeware. This delineated any differences in the position of the carpal and metacarpal bones between the wrists.
Dynamic motion analysis (cinematography)
The behaviour of the prosthesis in flexion/neutral/extension and radial inclination/neutral/ulnar inclination was qualitatively assessed by one of the authors (P.H.) using fluoroscopy (Axiom Artis zee MP, Siemens Medical Solutions USA, Inc., Malvern, PA, USA).
Results
The accuracy of shape of the prosthesis was excellent, with maximal differences of 0.5 mm (Figure 6). Reproducibility of wrist positioning in the splints was satisfactory. In neutral position the wrist with the prosthesis showed 5° more flexion and similar radial inclination compared with that of the wrist before scaphoid excision and replacement. In flexion, it showed 3° more ulnar inclination and identical flexion. In extension, it showed 5° more ulnar inclination and similar extension. In radial inclination it showed 1° more radial inclination and 1° more extension. In ulnar inclination it showed 4° more ulnar inclination and 2° more extension.
Excellent accuracy in shape of the prosthesis with maximal differences of –0.05 to 0.5 mm to the original scaphoid.
Static motion analysis (CT scans)
Overlaying the 3D-models in the predefined positions pre- and post-operatively, showed similar motion patterns for the prosthesis and the original scaphoid (Figure 7). The prosthesis behaved in a physiological way with flexion in wrist flexion and radial inclination and extension in wrist extension and ulnar inclination. The biggest difference was found in ulnar inclination with a more extended prosthesis.
Correlation between the original and prosthetic scaphoids in neutral, flexion, extension and radial and ulnar inclination (blue, original wrist; grey, same wrist with scaphoid prosthesis).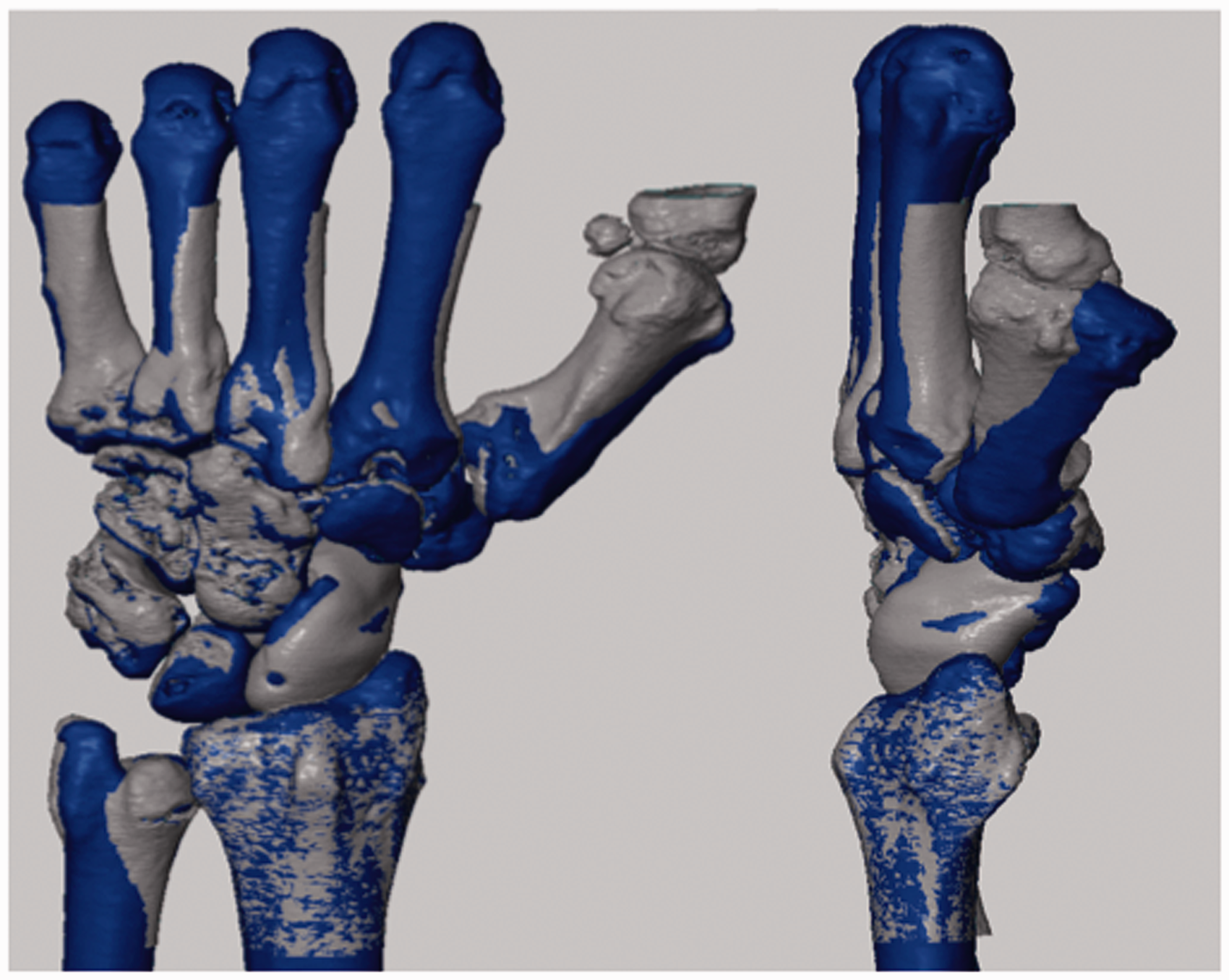
Dynamic motion analysis (cinematography)
The cinematography confirmed the anatomical position of the prosthesis in the wrist. The suspension used was stable and the prosthesis followed the movements of the wrist in extension and flexion as well as in radial and ulnar abduction in a physiological way. The scapholunate interval was stable throughout all physiological positions of the wrist (Videos S1 and S2, available online).
Discussion
The aim of this preliminary study was to test the feasibility of printing a replica of the scaphoid, and to test its motion behaviour when suspended with a tendon strip reconstructing the STL and SLL. The study delivered some promising results, which justify ongoing investigation.
Earlier scaphoid arthroplasties were complicated by dislocation and failure to prevent carpal collapse and arthritis (Carter et al., 1986; Kleinert et al., 1985; Spingardi and Rossello, 2011). We found that our prosthesis moved in a similar way to the original scaphoid, indicating that the suspension helps the implant to move in a natural way and possibly prevent carpal collapse and osteoarthritis. The fixation technique reconstructs the SLL and the STL as a secondary stabilizer to counteract the flexion moment of the scaphoid (Garcia-Elias et al., 2006; Henry, 2013). In a total replacement of the scaphoid, it is important to counteract flexion but also to stabilize the prosthesis in place. The design of the channel in the prosthesis reproduces the original anatomical distal and proximal–dorsal fixation points of the ligaments, which theoretically should help to obtain an anatomical reconstruction and physiological motion. These entry and exit points for the graft can be used with any other techniques, such as the use of synthetic ligament materials instead of autografts.
Several studies have shown substantial inter-individual differences in the shape of the carpal bones and motion patterns of the scaphoid (Craigen and Stanley, 1995; Fogg, 2004; Moojen et al., 2002; Nuttall et al., 1998; Viegas et al., 1993). Considering this and the fact that the scaphoid articulates with five other bones and shows rotational and also translational motion, we believe that any scaphoid prosthesis and any biological scaphoid reconstruction must replicate the original shape of the bone as precisely as possible to minimize non-physiological kinematics and wear. This requires a patient-specific implant. With the rapid progress in 3D printing of different materials during recent years, patient-specific implants have become a realistic option. 3D printing of titanium, ceramics and polyetheretherketone nowadays make it possible to produce patient-specific implants using materials that are already used for prosthetics in dentistry, fracture treatment and replacements of large joints. The decision about which kind of material will be used in a final version depends on long-term biomechanical tests and investigation on wear resistance.
Letta et al. (2014) found surface-to-surface size differences between right and left scaphoids in individuals to be between 0.73 and 1.9 mm and bigger in men than women. This must be taken into account when using the mirrored contralateral bone as a template for the pathological one by slightly reducing the size of the prosthesis to avoid ‘overstuffing’.
The implant remained stable in place and the scapholunate interval was found to be stable within a physiological range of motion. However, in the extension and ulnar abduction positions, the prosthesis was found to be more extended compared with the original scaphoid. As the position of the wrist with the prosthesis differed most in these positions compared with the original wrist, we believe that the hyperextension was mainly a result of the increased ulnar inclination of the wrist in the splints (Figure 7).
One limitation of our study is the lack of cyclic testing, which will be done in future and will include different suspension materials as well. Although there is some evidence that allograft can be reliably used for prosthesis suspension in the wrist (Henry, 2013), investigation of other fixation materials as synthetics or allografts will be of major interest to reduce the risk of suspension failure.
After implantation of the prosthesis, no bridges are burnt for the well-known salvage procedures if they should be required. We believe that a suspended prosthesis might become an alternative treatment option for very difficult or non-reconstructable conditions of the scaphoid.
Footnotes
Acknowledgement
We thank the Deutsche Arthrose-Hilfe e.V. for their support in the early phase of the project and Dr Johannes Homa as well as Manfred Spitzbart from Lithoz GmbH, Vienna, Austria, for the 3D manufacturing of the ceramic prosthesis. Special thanks to Professor Magdalena Müller-Gerbl, Head of the Anatomical Institute of the University of Basel, Matthias Hollinger, Head of the occupational therapy, and the team of the Department of Radiology of the KSBL for their support in the cadaver study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study has been financially supported by the Deutsche Arthrose-Hilfe e.V.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.