
Abstract
Introduction:
The operative management of distal radial fractures commonly requires inpatient admission, increasing the pressure on acute hospital capacity. Dedicated day case pathways and regional anaesthesia can reduce the length of stay but evidence remains limited.
Methods:
A retrospective service assessment was carried out at a large multisite NHS trust. Consecutive adults undergoing operative fixation of isolated distal radial fractures were identified across two control periods (2018–2019 and 2021–2022) and a post-implementation period following the introduction of the North Midlands Hand Centre (NMHC) (2023–2024). The primary outcomes were same-day discharge, length of stay and postoperative complications. Secondary outcomes included anaesthetic technique, hand surgeon involvement and bed-day utilization.
Results:
A total of 243 patients were included (Control n = 125; NMHC n = 118), with comparable baseline characteristics. Following NMHC implementation, same-day discharge increased from 66.4% to 98.3% (p < 0.001) and the mean length of stay decreased from 19.4 to 6.6 h (p < 0.001). The mean bed-day utilization per patient fell from 0.69 to 0.06, corresponding to an estimated reduction of approximately 74 inpatient bed-days over 1 year. The use of regional anaesthesia increased from 20.0 to 93.2% (p < 0.001) and hand surgeon involvement increased from 70.4 to 97.5% (p < 0.001). Overall complication rates remained stable (17.6 vs. 13.6%, p = 0.5).
Conclusion:
A bespoke day case pathway in a clean-air theatre for distal radial fracture fixation was associated with improved perioperative efficiency without increased complications.
Level of Evidence:
III
Keywords
Introduction
Open reduction and internal fixation (ORIF) is commonly indicated for unstable or displaced distal radial fractures (DRFs). Historically, however, many surgically managed DRFs in the UK were treated through inpatient pathways under general anaesthesia, often within mixed trauma operating lists and with variable access to subspecialist hand surgeons. This traditional model frequently necessitated overnight admissions and contributed to inpatient bed utilization within acute hospitals, particularly in high-volume trauma settings. The increasing national incidence of hand and wrist injuries has further intensified pressure on theatre capacity and inpatient resources, underscoring the need for more efficient, scalable models of care (Johnson and Dias, 2021).
Advances in perioperative practice have enabled a shift towards awake or regional anaesthesia (RA) led day case surgery for hand and wrist trauma. Randomized controlled trial evidence in patients undergoing distal radial fracture fixation has showed that RA is associated with improved early postoperative pain control and altered analgesic requirements compared with general anaesthesia, without adversely affecting longer-term functional outcomes (Rundgren et al., 2019). The safety of outpatient and ambulatory hand surgery has been further supported by evidence showing low complication and infection rates when procedures are carried out within modern clean-air theatre environments (Blessley-Redgrave et al., 2026; BSSH, 2022; Yu et al., 2019). Collectively, this evidence provides a strong rationale for RA-driven day case pathways to improve theatre efficiency and reduce inpatient bed occupancy while maintaining patient safety and clinical outcomes.
To support service transformation at scale, the NMHC was established in July 2023 to deliver dedicated day case surgery for elective and trauma hand procedures carried out by subspecialty-trained surgeons, with perioperative pathways centred on RA. The NMHC is configured as a stand-alone clean-air theatre with its own separate admission and discharge facilities, offering a range of day case procedures, including plate and screw fixation of DRFs. The University Hospitals of North Midlands NHS Trust serves a resident population of approximately 1.17 million and functions as a Level III major trauma centre for a wider regional population exceeding 3 million, providing a representative setting for assessing the system-level redesign of wrist trauma services.
This service assessment aimed to assess the clinical safety and operational impact of implementing a RA-led, day case ORIF pathway for DRFs within a dedicated hand surgery unit and to present a reproducible model that other UK trusts may adapt when undertaking similar service improvement initiatives.
Methods
Study design and setting
A retrospective service assessment of DRF management was conducted within a large, multisite NHS trust serving the North Midlands region. The assessment examined changes in practice before and after the introduction of the NMHC. Consecutive adults with operatively managed DRFs were identified over three discrete periods corresponding to different service configurations: October 2018 to August 2019 and August 2021 to August 2022, during which the legacy DRF pathway was delivered across two acute hospitals; and August 2023 to August 2024, the first full year in which the NMHC model was fully integrated within the trust. This project met NHS definitions for service assessment, used only routinely collected and anonymized clinical data, therefore formal research ethics approval was not required. The project was registered internally with reference CA11925.
Participants
Eligible participants were adults aged 18 years or older who presented to the trust with a DRF and underwent ORIF. Patients with polytrauma, bilateral and multiple significant injuries were excluded to ensure the cohort reflected isolated DRF management.
Data collection
Data were extracted from electronic health records and operative databases. Variables collected included demographic information (age and sex), treating hospital site (County Hospital, Royal Stoke University Hospital or NMHC), fracture characteristics (extra-articular vs. intra-articular pattern) and operative or perioperative details such as anaesthetic technique (general anaesthesia (GA), RA or combined GA–RA) and hand surgeon involvement.
Service performance metrics included length of stay, measured in hours and derived bed-day use, which is calculated as 0 for stays of up to 24 h and the ceiling of length of stay divided by 24 for longer admissions. Clinical outcomes comprised postoperative nerve-related symptoms, bleeding or haematoma, severe mobility limitation, infection, tendon complications, the need for re-operation and a composite measure of any complication.
Study periods
To assess the system-wide effect of the NMHC, analyses were conducted by study period rather than by individual case allocation. The Control period comprised 2 years, October 2018 to July 2019 and August 2021 to July 2022. The intervening years were excluded because complete data were unavailable and the COVID-19 pandemic led to unstable service configurations. The NMHC period covered August 2023 to July 2024. Grouping by period enabled the assessment of the whole-system transformation, including changes to anaesthetic practice, theatre scheduling and the structure of hand surgery provision.
Statistical analysis
Baseline characteristics were summarized descriptively and differences between study periods were assessed using appropriate statistical tests: t-tests for normally distributed continuous variables, Mann–Whitney U tests where distributional assumptions were not met, and χ² or Fisher’s exact tests for categorical variables. Primary outcomes were same-day discharge, length of stay and any postoperative complication. Secondary outcomes included individual complications, anaesthetic technique and the proportion of cases carried out by a hand surgeon. A sensitivity analysis compared NMHC-site cases with non-NMHC cases at the individual-case level to assess whether institutional differences influenced outcomes independently of period effects.
To illustrate longitudinal changes in practice, a year-by-year analysis from 2018 to 2024 was undertaken, plotting trends in same-day discharge, regional block use, hand surgeon involvement and postoperative complications. A separate horizontal faceted plot compared the length of stay and bed-day utilization between periods to show the operational impact of the NMHC model.
Results
Study population and baseline characteristics
A total of 243 adults underwent operative fixation for DRFs during the assessment period, comprising 125 patients treated during the 2 year Control period and 118 patients treated during the 1 year NMHC period (Table 1). Baseline characteristics were comparable between study periods. Mean age was similar in the Control and NMHC groups (55.6 vs. 55.1 years) and there were no significant differences in sex distribution or fracture pattern. Intra-articular fractures accounted for approximately 70% of cases in both groups.
Baseline characteristics.
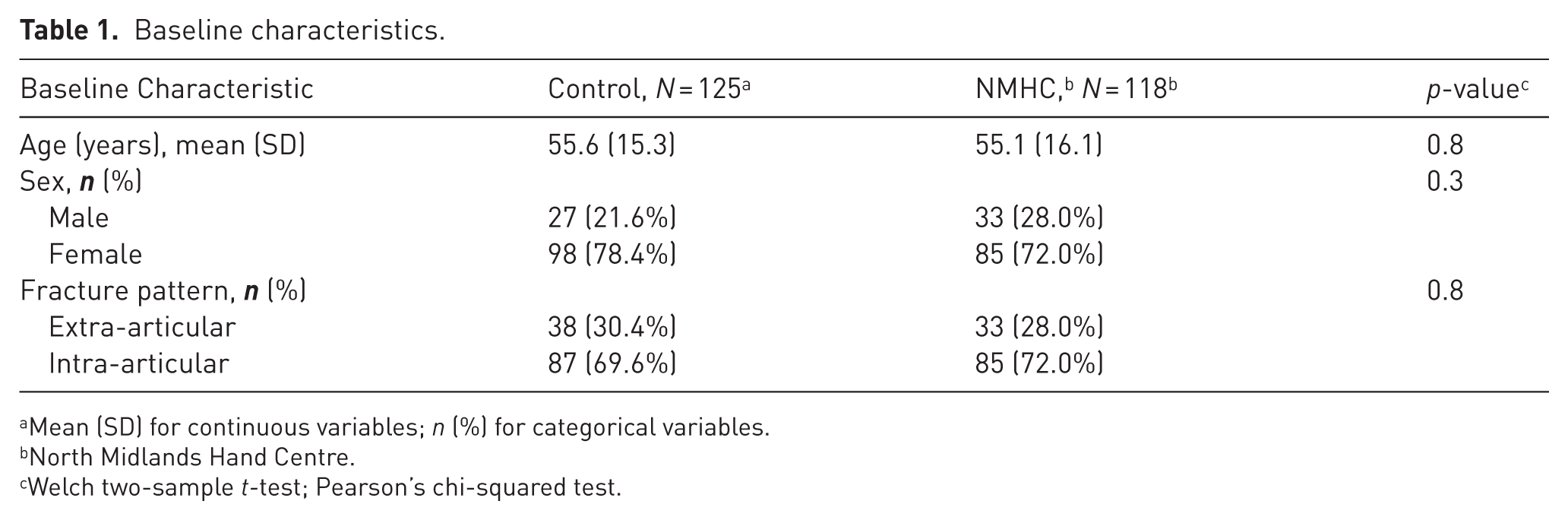
Mean (SD) for continuous variables; n (%) for categorical variables.
North Midlands Hand Centre.
Welch two-sample t-test; Pearson’s chi-squared test.
Primary outcomes
Primary outcomes are summarized in Table 2. Same-day discharge increased substantially following NMHC implementation, from 66.4% in the Control periods to 98.3% during the NMHC period (p < 0.001). Mean length of stay decreased from 19.38 to 6.55 h (p < 0.001).
Primary outcomes.
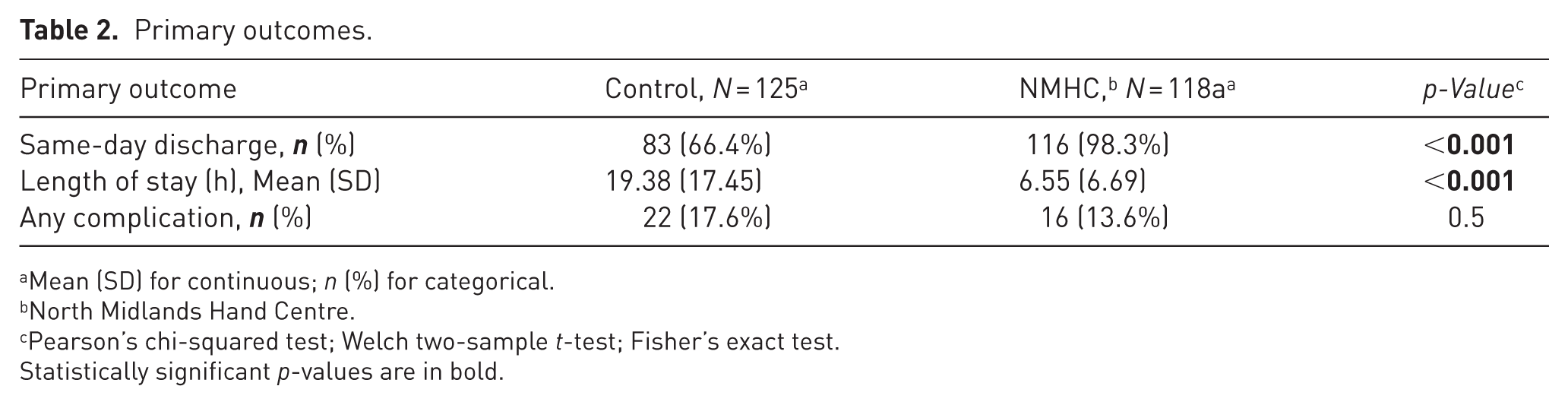
Mean (SD) for continuous; n (%) for categorical.
North Midlands Hand Centre.
Pearson’s chi-squared test; Welch two-sample t-test; Fisher’s exact test.
Statistically significant p-values are in bold.
The proportion of patients experiencing any postoperative complication did not differ significantly between periods (17.6% in the Control periods vs. 13.6% in the NMHC period; p = 0.5).
The distribution of length of stay and bed-day utilization showed a marked reduction in prolonged admissions during the NMHC period, with very few stays exceeding 24 h (Figure 1).
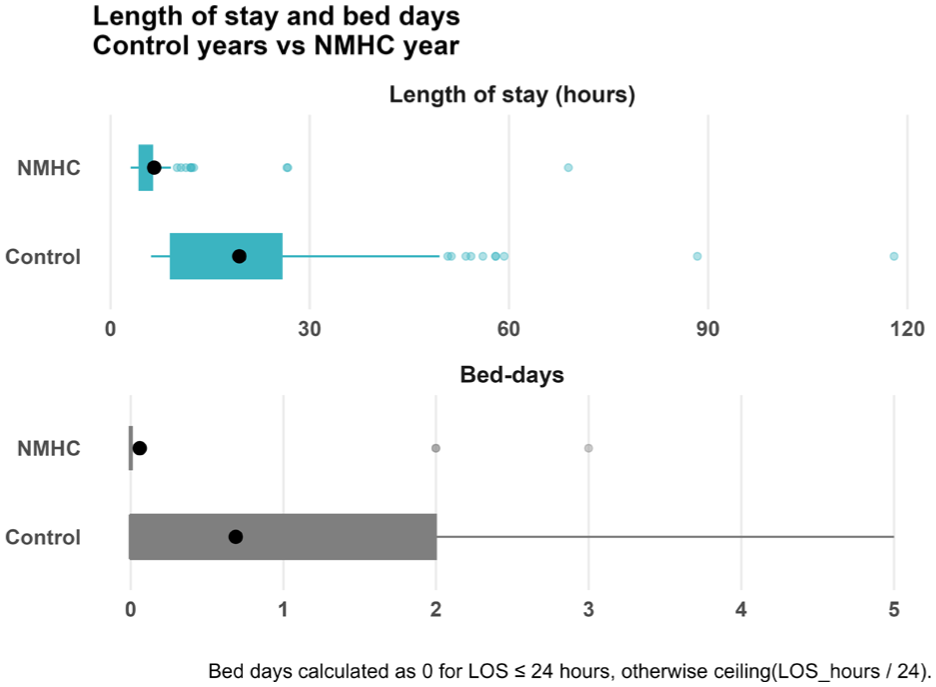
Length of stay (hours) and bed days utilization.
Perioperative and service delivery characteristics
Secondary outcomes are presented in Table 3. The use of RA increased markedly following NMHC implementation, from 20.0% in the control period to 93.2% in the NMHC period (p < 0.001). The proportion of procedures carried out by a subspecialist hand surgeon increased from 70.4% during the Control periods to 97.5% in the NMHC period (p < 0.001).
Secondary outcomes.
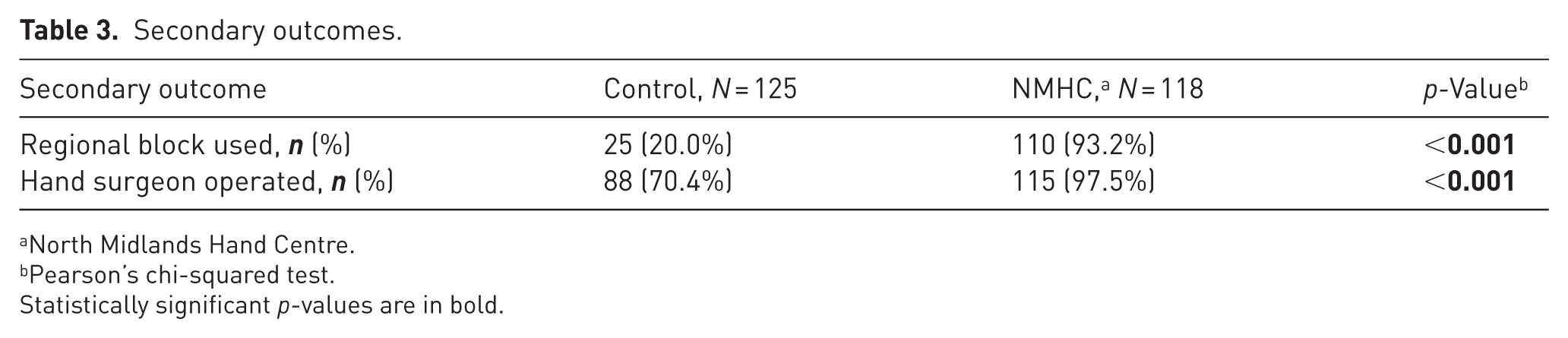
North Midlands Hand Centre.
Pearson’s chi-squared test.
Statistically significant p-values are in bold.
Year-by-year analysis showed progressive increases in the use of RA, same-day discharge and hand surgeon involvement, with stepwise changes coinciding with the introduction of NMHC (Figure 2).
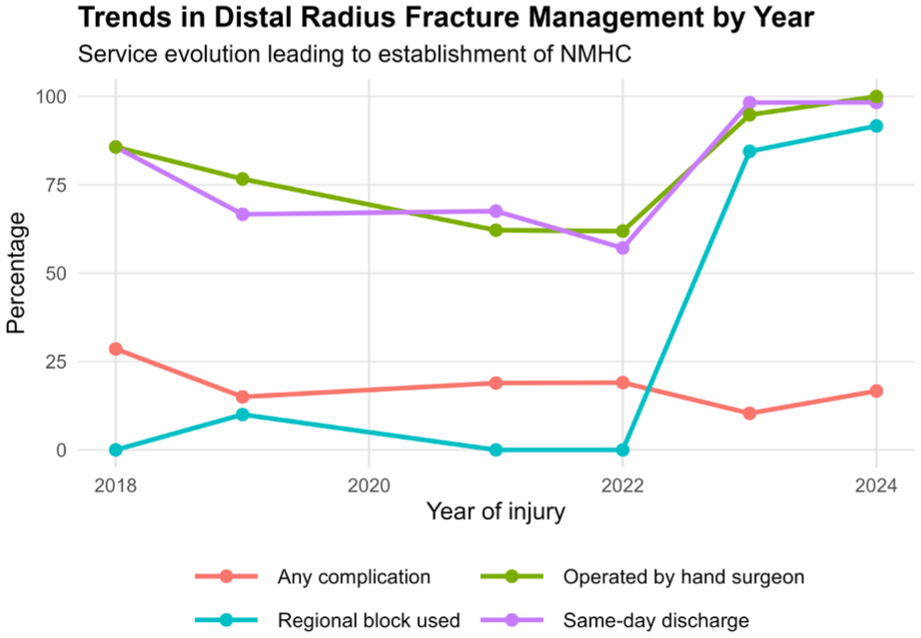
Trends in distal radial fracture management by year.
Complications
Postoperative complications are shown in Table 4. Individual complication rates were low in both study periods. There were no statistically significant differences between periods in nerve-associated symptoms, bleeding or haematoma, severe mobility limitation, infection, tendon complications or reoperation rates. Infection occurred in one patient during the NMHC period and none during the Control periods (p = 0.5). Reoperation rates remained low and comparable between groups (3.2 vs. 1.7%; p = 0.7).
Complications.
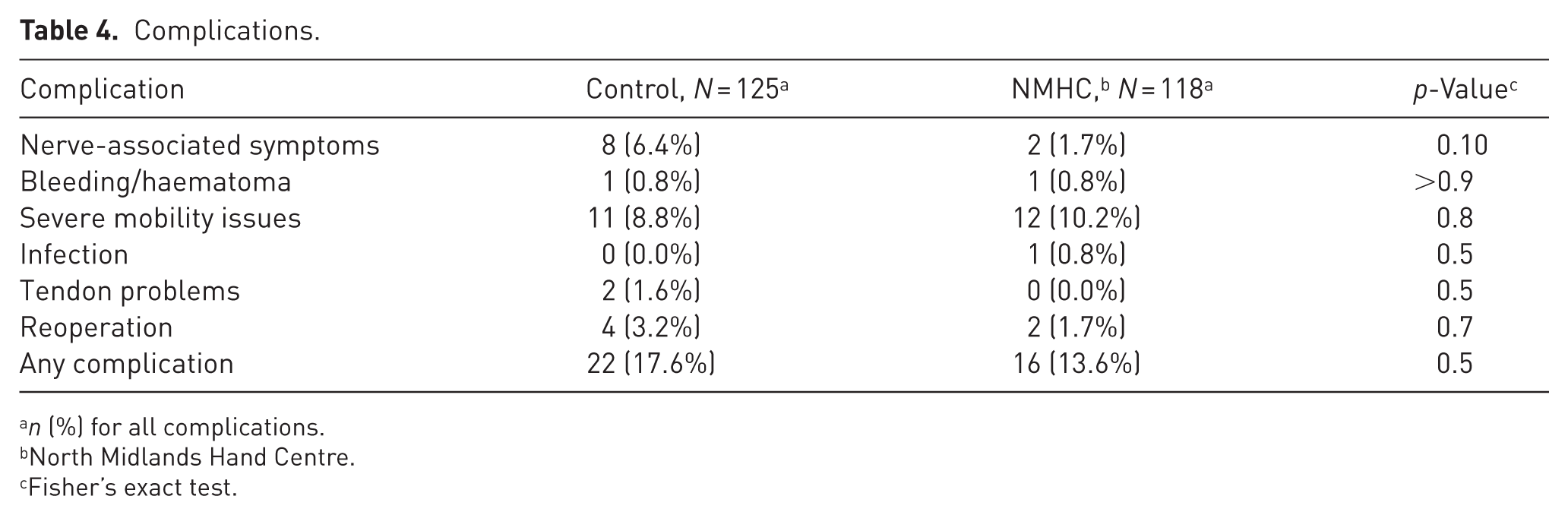
n (%) for all complications.
North Midlands Hand Centre.
Fisher’s exact test.
Overall complication rates remained stable across study periods (17.6% in the Control periods vs. 13.6% in the NMHC period; p = 0.5), with no increase observed following implementation of the NMHC model.
Sensitivity analysis
A sensitivity analysis comparing cases carried out at the NMHC site with non-NMHC cases at the individual-case level showed findings consistent with the period-based analysis, supporting the conclusion that the observed differences were associated with service configuration rather than case-mix variation.
Discussion
This service assessment shows that the NMHC enabled a safe, RA-led, day case, outside-the-main-theatre pathway for DRFs, achieving near-universal same-day discharge with low complication rates.
Bed-day cost analysis
NHS data measure acute bed-day costs at £400–600 (midpoint £530; with recent estimates at £527–562) (Guest et al., 2020; NHS England, 2025; UK Parliament, 2025). Bed-day use declined sharply from 0.69 to 0.06 per patient, saving ~74 bed-days per year across 118 cases and resulting in an estimated direct annual savings of £30,000–45,000 for 118 patients. These savings do not include the potential income from bed days saved and from moving these patients out of the main theatres, thereby vacating space for additional arthroplasty cases. Athar et al. (2019) analysed 229 trauma day cases (including 53 distal radius fixations), with 2.6% overnight stays, 94.5% satisfaction, no 48 h readmissions and £65,562 savings. These results highlight NMHC’s efficiency and cost-saving impact without compromising safety.
Regional anaesthesia benefits
Egol et al. (2012) retrospectively compared 187 DRF cases, finding that RA showed better 3 and 6 month pain, motion and DASH scores vs. GA. Lee et al. (2022) analysed 10,441 ORIF cases (1191 RA vs. 9250 GA) and found no differences in complications, reoperations, readmissions or mortality. In a randomized control trial, Rundgren et al. (2019) noted higher early opioid use and immediate postoperative pain with GA but RA had a later peak pain and post-discharge opioids; there were no 6 month Patient-Rated Wrist Evaluation (PRWE) or EuroQol-5 Dimension (EQ-5D) differences. NMHC’s RA rise boosted same-day discharge without raising complications, supporting RA as key to modern pathways.
Complications
Only one surgical site infection was observed during the NMHC period and none during the Control periods; there was no statistically significant difference between groups. The affected patient developed a stitch abscess, which resolved promptly with a short course of antibiotics. The introduction of this dedicated clean-air facility at the NMHC was not associated with a statistically significant change in infection rates, which remained low overall.
Strengths and limitations
This service assessment has several strengths. It includes consecutive patients managed across multiple service configurations within a large NHS trust serving a major regional population, allowing assessment of real-world practice rather than selected cohorts. The use of clearly defined pre- and post-implementation periods enabled assessment of the whole-system change associated with the introduction of the NMHC, rather than isolated pathway modifications. In addition, sensitivity analyses comparing NMHC and non-NMHC cases supported the robustness of the findings and reduced the likelihood that observed improvements were attributable solely to secular trends or case-mix variation.
However, several limitations should be considered when interpreting the results. The retrospective design limits causal inference and unmeasured confounding factors may have influenced outcomes. Fracture characteristics were recorded using binary classification (intra-articular vs. extra-articular), which may not fully reflect the spectrum of fracture complexity. As a result, residual confounding from underlying fracture severity cannot be excluded and differences in case complexity between study periods may have influenced the observed outcomes and the allocation of patients to inpatient or day-case pathways. Functional outcomes and patient-reported measures were not collected, precluding assessment of longer-term recovery, pain or patient satisfaction. The assessment reflects the experience of a single NHS trust, which may limit generalizability to centres with differing infrastructure, workforce availability or local service pressures. Finally, formal health-economic analysis was beyond the scope of this study, although the observed reductions in length of stay and bed utilization suggest potentially important resource implications.
Implications for practice and future service development
Despite these limitations, the findings have important implications for service delivery. Key transferable elements include subspecialist-led care, RA centred perioperative pathways and protected day case theatre capacity. The use of a clean-air theatre for fracture fixation did not increase the risk of infections or any other complications. Future work should incorporate prospective collection of patient-reported outcomes, assessment of long-term functional recovery and formal health-economic analyses to further define the value of such models.
The introduction of a dedicated, regional-anaesthesia-led day case hand surgery unit was associated with improvements in perioperative efficiency for operatively DRFs, including higher rates of same-day discharge and reduced length of stay. These changes were observed without an increase in postoperative complications during the assessment period. A retrospective service assessment of the findings showed associations rather than causal effects; however, it suggests that a structured day case hand surgery pathway may be feasible within a large NHS trauma service. Similar service development initiatives in other centres facing increasing trauma workload and pressure on inpatient capacity may benefit from introducing this bespoke pathway.
Footnotes
Acknowledgements
The authors would like to thank Mr Jaffar Ibrahim for his contributions to the study design.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Use of generative AI
The authors used generative artificial intelligence tools solely to assist with language editing, formatting and grammar refinement. All scientific content, analysis, interpretation and conclusions were conceived, drafted and verified entirely by the authors. The authors take full responsibility for the integrity and accuracy of the work and confirm that the use of generative AI complies with the journal’s guidelines.