
Abstract
Why do people with psychopathology use less adaptive and more maladaptive strategies for negative emotions if such usage has self-destructive consequences? Although researchers have examined the reasons for people’s engagement in maladaptive “behaviors,” such as nonsuicidal self-injury, surprisingly little attention has been paid to the reasons why people might endorse maladaptive emotion regulation (ER) strategies. This article addresses this question, focusing on the case of depression, evaluating an array of 10 possible explanations. After considering the existing evidence, we provide a blueprint to help the field reach stronger conclusions about depression and other forms of psychopathology. Better understanding of the origins of healthy/unhealthy ER has implications for clinical science, clinical practice, as well as their integration.
Many researchers postulate that difficulty in emotion regulation (ER) is a trans-diagnostic construct that explains why people develop mental disorder(s) (see Kring & Sloan, 2009). A key idea is that people with mental disorder(s) employ faulty ER strategies with respect to their negative feelings. A major meta-analytic review concluded that increased endorsement of problematic ER strategies is associated with multiple psychological problems, including depression, anxiety, and eating disorders (Aldao, Nolen-Hoeksema, & Schweizer, 2010). Further, Sloan et al.’s (2017) systematic review showed that endorsement of maladaptive ER strategies decreases following psychological treatments across different kinds of treatments and clinical problems, including depression, anxiety, eating disorders, borderline personality disorder, and substance use problems.
Why do people with psychopathology use less adaptive and more maladaptive strategies for negative emotions if such choices have self-destructive consequences? Although researchers have examined the reasons for people’s engagement in maladaptive “behaviors,” such as binge-eating, smoking, drug or substance use (see e.g., Tice & Bratslavsky, 2000), and nonsuicidal self-injuries (see Nock, 2009, for review), surprisingly little attention has been paid to the reasons why people might endorse maladaptive ER strategies. This article evaluates several possible explanations for why people might make seemingly poor ER decisions, as well as key recommendations to guide future research on this topic.
To address this topic in a cohesive fashion, we focused on the case of depression. We consider depression because it is an important form of psychopathology and one of the most researched, especially in the area of ER (e.g., Aldao et al., 2010). Even with this high degree of interest, we will see the empirical record on addressing some of these explanations is scanty. Perhaps for this very reason, this is a critical moment to take stock of the field. We view the main novelty and strength of this article is to clearly envision possibilities for why depressed persons show a putatively problematic pattern of ER strategy usage. We identified the most plausible hypotheses for why such a pattern exists, evaluating what we know and do not know about each hypothesis. After taking stock, we propose five future directions to enhance our understanding of ER, including the benefits that will redound to depression research and treatment, and the understanding of psychopathology more broadly. Indeed, we identify clear thinking about the big picture as necessary for further meaningful progress in understanding depression and other forms of psychopathology. Rather than focusing on a single mechanistic explanation for why people with depression deploy maladaptive ER strategies (e.g., cognitive biases and inhibition difficulty; Joormann & Stanton, 2016), our goal is a comprehensive review of what is known regarding several plausible explanations.
In tackling these issues, we focus on ER strategies for negative emotions because (a) the clinical literature overwhelmingly focuses on the regulation of negative emotions; (b) we wanted to make our review both tractable and coherent; and (c) explanations for depression-related differences in the regulation of positive emotions are likely to be quite different. Also, to make our review tractable, we follow a broad distinction between putatively maladaptive (maladaptive hereafter) and putatively adaptive (adaptive hereafter) ER strategies rather than focusing on individual ER strategies (Aldao et al., 2010). Among the most frequently studied adaptive ER strategies are cognitive reappraisal, problem-solving, and acceptance (see Liu & Thompson, 2017, for review). Among the most frequently studied maladaptive strategies are expressive suppression, avoidance, and rumination (see Liu & Thompson, 2017, for review). We used the adaptive/maladaptive ER distinction for three main reasons. First, we wanted our review to have historical continuity with work on emotion regulation: for over 10 years, ER strategies have been classified as either adaptive or maladaptive based on expert consensus about their effects on mood (Aldao et al., 2010; Liu & Thompson, 2017; Schäfer, Naumann, Holmes, Tuschen-Caffier, & Samson, 2017). Second, there is considerable empirical evidence that depressed people generally use more of the maladaptive strategies and less of the adaptive ER strategies, compared to nondepressed persons (Aldao et al., 2010; Visted, Vøllestad, Nielsen, & Schanche, 2018). We believe it would serve the field to arrive at sounder interpretations of these findings. Third, many clinically evidence-based treatments for depression have focused on reducing maladaptive ER strategies and enhancing adaptive ones (e.g., cognitive behavioral therapy [CBT] fosters cognitive reappraisal through thought challenges; Jacobson et al., 2000). Thus, use of this distinction would help make this review relevant to considerable existing work on intervention.
One reason for focusing on depression is that it has a particularly well replicated relationship to problematic ER strategy endorsement. Aldao et al.’s (2010) meta-analysis was influential in establishing that greater endorsement of maladaptive (with a medium to large effect), and lesser endorsement of adaptive, ER (with a small to medium effect) strategies predicted greater depressive symptoms (see also, Kovacs, Rottenberg, & George, 2009). We should note that extant research, almost exclusively, uses retrospective self-report methodology to assess emotion regulation strategy choice. One concern is that this methodology may inflate effect sizes because of depressed persons’ response biases, tendencies to endorse negative self-relevant characteristics (e.g., Smith, Ingram, & Roth, 1985), or tendency to reject positive self-relevant characteristics (see Orth & Robins, 2013, for review). Importantly, a small body of work using alternative methodology provides some independent corroboration, as similar results have been obtained in studies using self-reports of state ER strategy usage in a lab setting (e.g., Quigley & Dobson, 2014) and in studies that collect contemporaneous self-reports of ER in daily life (e.g., Brans, Koval, Verduyn, Lim, & Kuppens, 2013; Silk, Steinberg, & Morris, 2003). Thus, there is reason to believe that, even if retrospective self-report methods inflate depression-related effect sizes, the data obtained from such methods still reflect real-world differences in use.
Finally, we think this review is timely as a corrective. That is, because the pattern of maladaptive ER strategy endorsement is well replicated in depression, it has been tempting to use it as a basis to draw broad, often unfounded, conclusions about the nature of ER in depression. For example, some commentators infer from this finding that participants make less use of adaptive ER because they lack skill in adaptive ER strategies (e.g., Freudenthaler, Turba, & Tran, 2017; Klemanski, Curtiss, McLaughlin, & Nolen-Hoeksema, 2017; van Beveren, Harding, Beyers, & Braet, 2018). With a second inferential leap, it is then asserted that teaching or training depressed people in adaptive ER skills will in itself improve depression: “youth low in positive emotionality will benefit from learning different adaptive ER skills” (van Beveren et al., 2018, p. 33); “prevention and intervention programs teaching strategies to promote adaptive emotion regulation skills and reduction in RNT may reduce both social anxiety and depression” (Klemanski et al., 2017, p. 216); and “the training of mindfulness and of emotion regulation skills may be also beneficial for the prevention of symptoms of depression and anxiety in the general population” (Freudenthaler et al., 2017, p. 1343). Although these implications sound plausible, they also seem premature. Is it right to call for teaching people with depression adaptive ER strategies without first demonstrating that ER knowledge or skill is impaired? We think the time is ripe to carefully evaluate explanations for why persons with depression report such an ER pattern, to have more clarity about what we do not yet know. Such a reckoning is needed if we are to improve descriptive psychopathology or, ultimately, to identify the most promising treatment target(s).
Why, then, do persons with depression utilize more maladaptive and less adaptive ER strategies than nondepressed persons? In this article, we address 10 possible explanations for either excessive use of maladaptive ER strategies and/or lack of use of adaptive strategies. Each explanation hypothesizes a possible reason why depressed persons show a pattern of using less adaptive and more maladaptive ER strategies, compared to nondepressed individuals. Given the complexity of human behaviors, the list of potential hypotheses was virtually limitless. To winnow the list of explanations, we chose hypotheses that have been previously discussed by researchers as plausible. We also valued explanations that could be readily tested. To locate our list of explanations within a wider conceptual space, we nested our explanations within Tinbergen’s (1963) framework. Tinbergen’s framework considers four levels of explanation relevant to understand a behavior: mechanism, function, development, and evolution. Our explanations were connected to all levels of Tinbergen’s (1963) framework, with the exception of the phylogenetic level because that level is less readily tested (see Table 1). These 10 explanations, as we will discuss, are not necessarily mutually exclusive. For each explanation, we will consider both its theoretical plausibility and level of empirical support. We begin with five explanations that focus on depressed persons’ decreased implementation of adaptive strategies, followed by two explanations that focus on increased implementation of maladaptive strategies, and finally three explanations regarding possible mechanisms that apply to both adaptive and maladaptive ER patterns.
Regulation of negative emotions in depression.
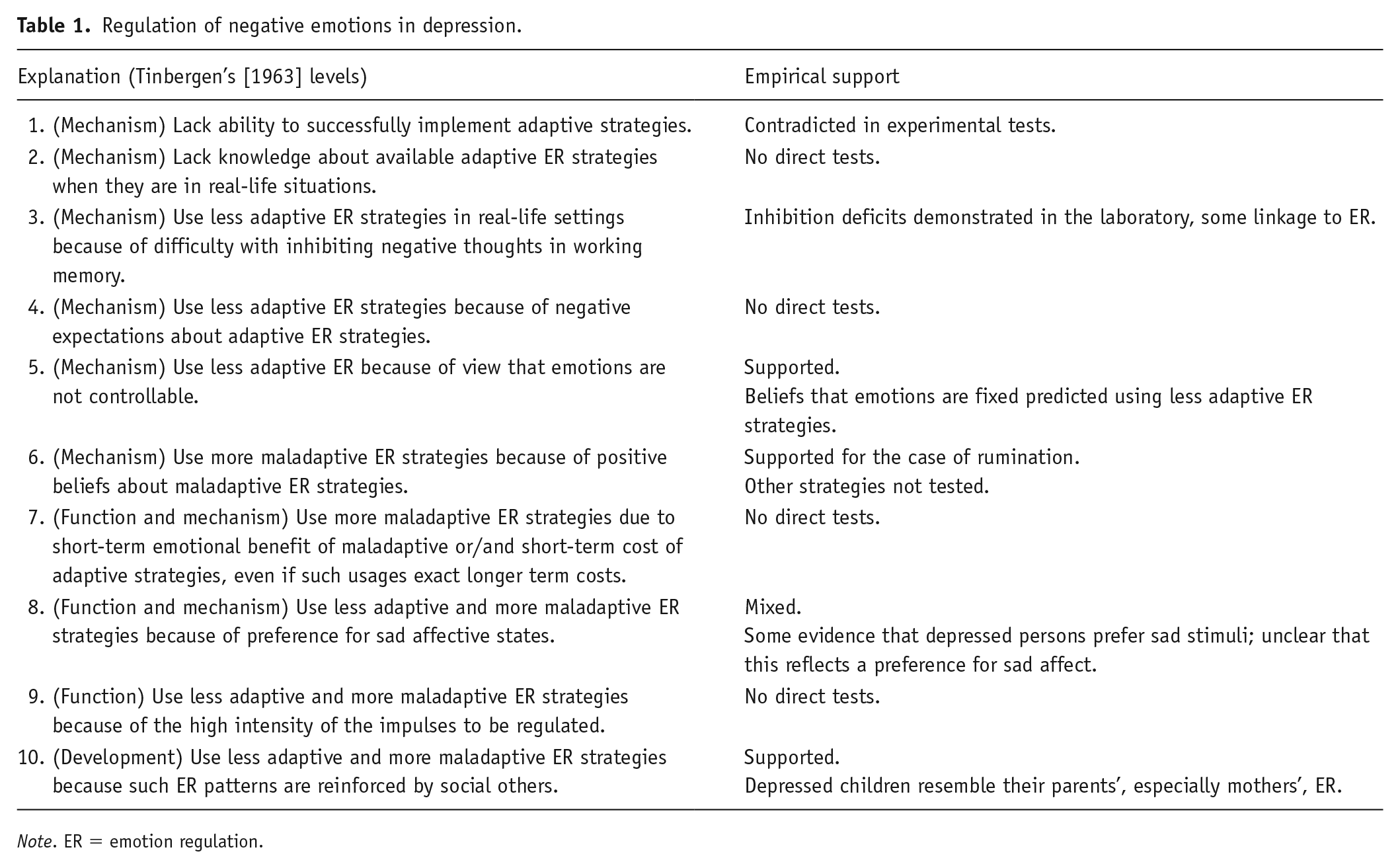
Note. ER = emotion regulation.
Explanations for Depression-Related Differences in ER Strategy Choice
Explanation 1: People With Depression Do Not Have the Ability to Successfully Implement Adaptive Strategies
It is possible that persons with depression use adaptive ER strategies less frequently because they are not capable of implementing these strategies. Implementation of ER strategies means “the short-term execution of a particular regulation strategy” (Sheppes, Suri, & Gross, 2015, p. 383). Although this explanation is initially plausible, Liu and Thompson (2017) carefully reviewed a significant body of work directly examining instructed ER in the laboratory and concluded that, when so instructed, depressed persons are just as able to implement adaptive ER strategies, as indicated by similar reductions in negative affect after strategy use, as nondepressed persons. These null findings undercut the explanation that depressed persons lack ability to implement adaptive ER strategies.
Despite this negative evidence, we do not see the issue of ER ability in depression as entirely settled. One limitation of work on ER ability in the laboratory is that only mild or moderate levels of negative emotion were aroused via emotional images (Millgram, Joormann, Huppert, & Tamir, 2015), discussion of negative personal events (Smoski, LaBar, & Steffens, 2014), or performing a frustrating task (Ellis, Vanderlind, & Beevers, 2013). One key unresolved question, then, is whether people with depression would break down in their efforts to implement adaptive ER strategies in circumstances where more intense emotional impulses are regulated.
Explanation 2: People With Depression Lack Knowledge About Available Adaptive ER Strategies in Real-Life Situations
Even though there is reasonable evidence that depressed persons can implement adaptive ER strategies in the laboratory, it appears that they do not choose these strategies in real life. This might occur if available adaptive ER tactics do not spontaneously come to mind when they are most needed in real-life settings. Each ER strategy requires knowledge concerning specific tactics that can be used to implement it (Sheppes et al., 2015). For example, to implement cognitive reappraisal, it is helpful to hold in mind diverse ways the strategy can be realized, such as “I can think of other possible positive interpretations” or “I can think of positive lessons from a negative situation.” Individuals with depression might not hold enough knowledge concerning available adaptive tactics, which can discourage them from selecting an adaptive ER strategy. If this is the case, providing depressed persons with a stock of adaptive ER tactics might increase their use in real-life settings. Unfortunately, to our knowledge, this proposition is as yet untested.
Explanation 3: People With Depression Use Less Adaptive ER Strategies in Real-Life Settings Because They Have Negative Cognitive Biases and Difficulty With Inhibiting Negative Thoughts in Working Memory
A related hypothesis is that persons with depression might not use adaptive ER strategies in real-life settings because maladaptive strategies are more accessible to them when ER is needed. Joormann and Stanton (2016) provide an extensive theory consistent with this hypothesis. Specifically, these authors articulate how cognitive biases towards negative information (e.g., attentional disengagement difficulty, negative interpretational and memory bias) and deficits in inhibiting mood-congruent negative thoughts from accessing and remaining in working memory may lead to difficulty in accessing adaptive ER strategies—such as cognitive reappraisal—and increased accessibility of maladaptive ER strategies, such as rumination. Additionally, Joormann (2010) theorized that depressed individuals are prone to use maladaptive strategies because they have difficulty with inhibiting mood-congruent negative thoughts from working memory. As a consequence of these inhibition deficits, a person is more likely to rehearse or ruminate about negative material, and/or to have trouble accessing mood-incongruent thoughts, which again could decrease access to adaptive ER strategies, such as reappraisal or problem-solving. In addition, the appraisal bias model (Mehu & Scherer, 2015) theorizes that cognitive bias may serve as a risk factor for depression because it plays into problematic patterns of ER strategy use. The model postulates that rigid and extreme cognitive biases tend to elicit intense emotions in many situations; the inflexible emotional responses in turn make it hard to use adaptive ER strategies, and therefore renders a person more vulnerable to developing depression (Mehu & Scherer, 2015).
Despite the strength of this theoretical work, no research has directly examined how specific cognitive biases alter the subsequent selection of ER strategies. There is correlational work showing that persons with depression have difficulty with inhibiting negative stimuli in working memory and that the extent of this difficulty is related to higher endorsement of rumination and lower endorsement of reappraisal in depressed people (see Joormann & Stanton, 2016, for review). This correlational work is an important preliminary step in showing how inhibition difficulty may change or impact the choice of ER strategies in people with depression (see Joormann & Stanton, 2016).
Explanation 4: People With Depression Use Less Adaptive ER Strategies Because They Hold Negative Expectations About Adaptive ER Strategies
Even if depressed people were just as able to implement adaptive ER or were equally knowledgeable about adaptive ER tactics, depressed people might be deterred from selecting such strategies due to their beliefs. Belief has been theorized as an essential driving factor for behavior (see Eccles & Wigfield, 2002, for review) and correlates with conscious and automatic usage of ER strategies (e.g., Taku, Cann, Tedeschi, & Calhoun, 2015). Thus, we propose several beliefs that might influence conscious or unconscious processes underlying ER strategy use in depression.
The first regards negative expectations about adaptive ER strategies. Expectancy refers to a belief on whether a certain task or behavior will lead to a certain result. For example, depressed persons might hold negative expectations that adaptive strategies will not be effective for mood enhancement in general (i.e., including both self and others) or will not work for their individual case. Surprisingly, to our knowledge, no study has yet examined what kinds of expectancies depressed persons hold regarding adaptive strategies. Although not specifically about adaptive strategies, we have studies of generalized expectancies for negative mood regulation (NMR), which concern the degree to which a person believes his or her coping strategies will enhance negative mood (e.g., Catanzaro & Mearns, 1990). Importantly, higher levels of NMR expectancies are inversely related to depression (e.g., Flett, Blankstein, & Obertynski, 1996; Kassel, Bornovalova, & Mehta, 2007), as well as being positively associated with adaptive coping (e.g., Catanzaro & Greenwood, 1994; Kassel et al., 2007).
Another theoretical basis for considering the negative beliefs about the adaptive ER explanation comes from the expectancy of motivation theory (e.g., Atkinson, 1957), which maintains that a person’s expectancy about whether a certain behavior will help them achieve a goal, further motivates the behavior. Thus, depressed persons’ expectation that adaptive ER strategies will not be effective for them might lead to diminished motivation to use the strategies. In addition, mood-congruent theory (e.g., Mayer, Gaschke, Braverman, & Evans, 1992) argues that negative mood is often accompanied by negative judgments. It is possible that depressive mood leads people to maintain beliefs that “active” adaptive strategies might not work, which may bias them away from selecting those strategies.
Explanation 5: People With Depression Use Less Adaptive ER Because They Do Not Believe Emotions Are Controllable
Depressed people’s beliefs about emotion and its controllability might discourage them from identifying the need to change their mood using adaptive ER strategies. One distinct kind of belief concerns the malleability of emotion. Tamir, John, Srivastava, and Gross’s (2007) implicit theory of emotion considers the importance of individual differences in beliefs about the malleability of emotions: those who believe that emotions are fixed (not controllable; entity belief) are less likely to use active ER strategies, compared to those who believe emotions are malleable. Consistent with this idea, previous studies found that entity beliefs predicted lower usage of adaptive ER strategies (De Castella et al., 2013; Ford, Lwi, Gentzler, Hankin, & Mauss, 2018; Gutentag, Halperin, Porat, Bigman, & Tamir, 2017) and higher usage of avoidance as a strategy (De Castella, Platow, Tamir, & Gross, 2018). Ford et al. (2018) found that entity belief predicted greater depression 2 years later, and the relationship was mediated by the lower level of adaptive ER usage. In sum, there is preliminary support for the idea that the tendency to hold entity beliefs about emotion could help explain why depressed persons tend not to utilize adaptive ER strategies.
Explanation 6: People With Depression Use More Maladaptive ER Strategies Because They Hold Positive Beliefs About Maladaptive ER Strategies
It is possible that depressed people might hold inflexible positive beliefs about maladaptive strategies, which leads them to select and implement such strategies. Research in this area to date has primarily considered rumination. Consistent with this proposition, Papageorgiou and Wells (2001a) found that depressed people tend to have positive beliefs about rumination, including the belief that rumination will help them learn from the past, find solutions, and understand their depression. Moreover, the degree to which positive beliefs were endorsed predicted increased use of rumination (Papageorgiou & Wells, 2001a; Watkins & Moulds, 2005).
Although empirical work regarding positive beliefs about other maladaptive strategies has lagged, it is plausible that patterns similar to those observed for rumination will hold for other maladaptive strategies. Again, the concept of expectancy in motivation theory supports links between beliefs and motivations to behave (e.g., Atkinson, 1957). It is logical that depressed persons would be motivated to utilize strategies like avoidance or expressive suppressions because they believe they are beneficial across most contexts. These inflexible beliefs can lead depressed persons to overuse maladaptive strategies across situations. Avoidance might, for example, be seen as helpful to cope with anxiety across social situations, which can motivate a person to typically avoid social events. Expressive suppression might be seen as useful in every relationship context, which may influence a person to use it, even when it worsens mood.
Explanation 7: People With Depression Use More Maladaptive ER Strategies Because They Value Short-Term Emotional Benefits Provided by Maladaptive ER Strategies, Even if Such Usage Exacts Greater Longer Term Costs
It is plausible that depressed persons unconsciously or consciously prefer using maladaptive ER strategies because maladaptive strategies provide short-term emotional benefit, even though they may be harmful in the longer run, relative to adaptive strategies. For example, avoiding uncomfortable social situations might produce short-term relief from emotional discomfort; however, a pattern of avoidance may prolong one’s depression due to social isolation. Indeed, previous studies showed that expressive suppression results in greater initial reduction in negative affect to negative stimuli than using reappraisal (Yuan et al., 2015) and acceptance (Liverant, Brown, Barlow, & Roemer, 2008; Yuan, Liu, Ding, & Yang, 2014). Depressed persons might place a premium on short-term emotional benefits, compared to nondepressed persons, which leads them to implementing more maladaptive ER strategies. Relatedly, evidence in the domain of delay discounting suggests that depressed persons value small immediate rewards over large delayed rewards, although this is not universally found (see Forbes & Dahl, 2012, for review; see Schweighofer et al., 2008, for relation to biological dysfunctions). Finally, in repetitive self-harm, a clinical problem commonly seen among people with depression, those who engage in the behavior report short-term emotional relief as one reason for such behavior, even though its longer term consequences are adverse (see Klonsky, 2007, for review). Despite the plausibility of the valuing short-term benefits explanation, to our knowledge, there are no clear and direct empirical tests of this idea in depressed persons.
Another equally possible explanation is depressed persons might prefer maladaptive ER strategies due to the short-term cost of using adaptive strategies. Some adaptive strategies (e.g., cognitive reappraisal) may require substantial initial cognitive resources (Muraven, Tice, & Baumeister, 1998). For example, use of adaptive strategies may be disadvantageous for depressed people because they drain their already limited cognitive resources (see Rock, Roiser, Riedel, & Blackwell, 2014). Future research is imperative to examine the costs and benefits of each ER strategy, and whether the patterns of these costs and benefits differ for depressed persons.
Explanation 8: People With Depression Use Less Adaptive and More Maladaptive ER Strategies Because They Prefer Sad Affective States
Another possible explanation for why depressed persons might use less adaptive and more maladaptive ER strategies is because they prefer sad affective states. Specifically, Millgram et al. (2015) argued that depressed people have a stronger preference for sadness than do nondepressed controls. Three studies have shown that, when provided a choice between different affective stimuli, clinically depressed participants preferred to engage with sad stimuli more than nondepressed participants (Millgram et al., 2015; Yoon, Verona, Schlauch, Schneider, & Rottenberg, 2019). Further, in Study 3 of Millgram et al. (2015), the depressed group chose to increase sadness to sad pictures when trained to both increase and decrease emotions using a cognitive reappraisal, more often than nondepressed controls. With these findings, Millgram et al. (2015) argued that depressed persons use strategies to upregulate sadness because they want to feel sad. This position is also in line with self-verification theory and the idea that depressed persons might seek emotional stimuli or emotions that match or confirm their negative internal states (e.g., Giesler, Josephs, & Swann, 1996). Although researchers tended to view such pattern as maladaptive (e.g., Millgram et al., 2015), some researchers argued that depression (Andrews & Thomson, 2009; Nesse, 2000) or sad mood (Forgas, 2003) may serve positive functions. For example, depression may help a person cease making futile efforts in the face of an unachievable goal (Nesse, 2000) and depressive rumination may promote more focused analytical reasoning regarding life dilemmas that triggered the depression (Andrews & Thomson, 2009).
Although these findings are intriguing, one key caveat is that most work does not directly measure preference for emotional experiences, instead measuring preference for emotional stimuli that likely produce emotional states. The distinction between preference for emotional experiences and preference for emotional stimuli is important because putatively sad emotional stimuli can potentially generate a range of affective experiences, including positive emotions such as calmness (see Yoon et al., 2019). In fact, when we provided participants with free responses to explain their choices of emotional stimuli, depressed persons frequently said that they selected sad music because they found it relaxing or calming (Yoon et al., 2019). Moreover, we also found that after listening to their chosen music, depressed persons reported improved mood (i.e., decreased sadness and increased happiness) even though, again, sad music was most often chosen as preferred (Yoon et al., 2019). Thus, depressed persons’ apparent preference for sad stimuli might not necessarily reflect a preference for sad mood. Indeed, such a finding would also run against some findings in metaemotion, where having symptoms of depression is associated with a higher fear of experiencing sad mood states (see e.g., Yoon, Dang, Mertz, & Rottenberg, 2018, for review). Future studies are needed to reconcile these tensions.
Explanation 9: People With Depression Use Less Adaptive and More Maladaptive ER Strategies Due to the High Intensity of Their Negative Emotions
Given that depression often entails strong negative affective states, the intensity of emotions regulated by depressed persons is likely to be more intense than nondepressed people’s. One possibility is that high levels of intense negative emotion may “pull for” maladaptive ER strategies to a greater extent than do low levels of negative emotion. This could be the case if intense negative emotions are experienced as overwhelming and uncontrollable, which could short-circuit the selection of adaptive strategies, such as seeing the situation in a positive light, finding solutions, or accepting the situation as it is. With more intense negative emotions, a person might be inclined to keep ruminating about the trigger or seek other strategies that do not involve active processing, such as avoidance or expressive suppression. Indeed, Sheppes, Scheibe, Suri, and Gross (2011) found that healthy individuals chose disengagement-related ER strategies over cognitive reappraisal when in high-intensity negative situations (i.e., highly intense negative pictures and unpredictable electric shock), whereas cognitive reappraisal was preferred in low-intensity situations. Given that depressed persons report more intense daily stress compared to nondepressed individuals (e.g., Bylsma, Taylor-Clift, & Rottenberg, 2011), intense negative emotions that depressed persons experience might lead them to use less adaptive and more maladaptive ER strategies. This explanation is as yet untested with clinical samples.
Although empirical research is scanty, the affect intensity explanation remains plausible. For example, it is clinically well observed that when people are subjected to extreme adversity, initial reactions of avoidance or denial are virtually a normative response (Bonanno, 2004; Kübler-Ross, 1973), including to bereavement (e.g., Bonanno, 2004), major surgery (e.g., Bracken & Shepard, 1980), and to career adversity (e.g., Blinde & Stratta, 1992). Rumination was also commonly reported by putatively resilient individuals within 6 months after the loss of a spouse (Bonanno, Wortman, & Nesse, 2004). Thus, one possibility is that depressed persons gravitate towards “maladaptive” strategies like avoidance-based coping in part because they are more likely to be faced by the kinds of intense stressors (Monroe & Harkness, 2005) that generate intense negative affective states. This explanation brings up the fundamental question of whether depressed persons’ usage of maladaptive ER strategies is truly maladaptive or could overlap considerably with how healthy individuals regulate high-intensity stressors. Future study is imperative to address this question.
Explanation 10: People With Depression Use Less Adaptive and More Maladaptive ER Strategies Because Such ER Patterns Are Reinforced by Social Others
ER and the need for ER often occurs in the context of social interaction (Zaki & Williams, 2013). A person’s need to regulate emotion can occur in response to a social interaction, and also people can influence each other’s emotion regulation. Environmental reinforcement (e.g., attention) can increase or decrease behavior (e.g., Hull, 1943) through patterns of rewards or punishments, including observational learning (i.e., via watching others be reinforced; Bandura, 1986). Depressed people might use less adaptive and more maladaptive ER strategies via reinforcement from social others, such as family or friends. For example, a person might use expressive suppression or avoidance of negative emotion because the person’s family members provide attention contingent on displays of positive emotions only. Or a depressed person might simply learn maladaptive strategies because people around them frequently use such strategies.
Indeed, previous literature showed that children’s ER is socialized by adopting parental beliefs about emotion and ER (e.g., emotions are irrational and are to be avoided) and mirroring parents’ own ER strategies (see Thompson & Meyer, 2007, for review). In the context of depression, ample evidence exists on children, especially girls, modeling mothers’ negative affect, self-concepts, and behaviors (see Gotlib & Goodman, 1999, for review). Further, Katz and Hunter (2007) showed that higher level of mothers’ usage of acceptance for their own emotions was associated with lower levels of depression in their adolescent children. In sum, previous literature supports the interpersonal influence of use of ER strategies on depressed individuals, especially between mothers and daughters. However, it remains untested how ER choices in depressed adults are influenced by close relationships, such as spouses.
What Is Needed to Reach Stronger Inferences About ER Strategy Choice in Depression
It is time to reevaluate what we actually know about why people with psychopathology use more maladaptive and less adaptive ER strategies. Fitting this theme, our review of findings in the depression literature makes it clear that the often repeated claim that depressed persons need to be taught adaptive ER strategies (e.g., Freudenthaler et al., 2017; Klemanski et al., 2017; van Beveren et al., 2018) is unfounded. The major assumption—that depressed persons lack knowledge about ER tactics—is itself unproven. This underscores the need for specific research designs that will allow us to confirm (or disconfirm) particular explanations.
Therefore, in the following sections, we offer concrete suggestions for research that are grounded in what we already know, and which are designed to better test the explanations we have thus far considered. Our hope is that this work will help researchers and clinicians move forward in the most productive directions. For example, one ultimate goal is that by better understanding depressed persons’ motives for using faulty ER strategies, future research can help persons with depression achieve healthier emotions, either through formal interventions or less formal self-help procedures. Alternatively, we might learn, perhaps surprisingly, that there are cases in which depressed persons’ choices of ER strategy are adaptive and are not in need of change. Thus, in the next section, we suggest five research directions to potentially advance understanding.
We prioritize these directions for their incremental value in helping us gain closure on the explanations we have just evaluated, making no pretense that our list is exhaustive. For instance, we seek directions that will help clarify when and where depressed persons’ endorsement of maladaptive ER strategies represents a dysfunction versus a normative pattern (i.e., that would be observed among healthy nondepressed individuals undergoing stress). We seek designs that can help us reach firmer conclusions regarding depressed persons’ knowledge about available adaptive ER strategies (or lack thereof). We seek designs that tackle multiple explanations at once, knowing that some explanations can be tested in a single study design (e.g., a study can simultaneously examine beliefs about adaptive and about maladaptive ER strategies), and knowing that some explanations are not mutually exclusive. Beyond these five directions, we hope future research will lead to further follow-up questions, including testing additional explanations, possible interactions between explanatory mechanisms, and evaluating how each explanatory mechanism for ER strategy use relates to the causal chain of depression.
Direction 1: Focus on Context-Specific Deployment of Adaptive and Maladaptive ER Strategies
In parallel with examining “why,” we need to better understand “when.” That is, a full description of depressed persons’ ER strategy use requires more contextual information about exactly when depressed persons (and nondepressed persons) use maladaptive and/or adaptive strategies. The dominant reasoning in the literature presumes that depressed persons’ increased endorsement of maladaptive ER strategies indicates problematic usage of ER strategies. This assumption, too, may need to be reevaluated in light of future knowledge (Aldao, 2013; Bonanno & Burton, 2013). Emotion regulation is a process that involves a person, a situation, and a strategy. Increasingly, researchers are becoming aware that the benefits and costs of exerting an ER strategy may depend on the person (i.e., who is using what strategy), the situation (i.e., what strategy is used in which situation), and the interactions between the person and the situation (i.e., who is using what strategy in which situation; see Doré, Silvers, & Ochsner, 2016). Drawing on this contextual information, Bonanno and Burton (2013) highlighted “the fallacy of uniform efficacy.” Attention to context, for example, might help explain situations in which use of maladaptive ER strategy could actually have beneficial consequences. For example, research on bereavement indicates that those who repress their emotions, a putatively maladaptive ER strategy, ironically exhibited healthy outcomes after their loss in both short-term and long-term physical health problems and emotional distress (see Bonanno, 2004). For this reason, it is essential that we have research that sheds light on the specific situations (e.g., intense emotional events) in which depressed persons use maladaptive ER strategies and that assesses the possibility that the consequences of ER strategy use may not be uniform.
Experimental designs can be useful in helping us to gain traction on the context of ER strategy choice in depression. A model in this regard is Sheppes et al.’s (2011) paradigm where participants were instructed on different ER strategies, exposed to multiple emotional stimuli with varying intensity levels (i.e., emotional pictures), and then asked to choose an ER strategy to cope with emotions induced by each stimulus. This paradigm with high- and low-intensity emotional stimuli will allow tests of context (i.e., high vs. low) on depressed persons’ choice of ER strategies. If individuals with depression endorsed maladaptive ER strategies only when they are regulating highly intense emotions (resembling what nondepressed people do), depressed persons’ endorsement pattern might be seen as more normative rather than a pattern that reflects pathology.
Direction 2: Directly Examine Depressed Persons’ Knowledge About Adaptive ER Tactics and Their Ability to Access This Knowledge When Needed
Given the dearth of direct evidence, future work is needed to test whether depressed persons lack knowledge or ability to access knowledge regarding how to use adaptive ER strategies in real-life situations. To empirically test the hypothesis, future work might draw from research on coping repertoire (Cheng, 2001). Cheng (2001) examined coping repertoire using a daily assessment study design in which participants recalled the stress event of the day and reported all the strategies they used to cope with the stress, once a day for 6 days in a 3-week period. Based on Cheng’s (2001) study, future work can ask participants to recall the most emotional event for which they had to regulate their emotions, with additional questions about knowledge regarding ER. Participants can be asked what strategies they actually applied and what (else) they might have done to regulate their emotions provoked by the event. In this way, investigators can capture the number and range of ER tactics a person knows (allowing for group comparisons). In post hoc analyses, multiple assessors could categorize each tactic into putatively adaptive or maladaptive responses, again affording group comparisons.
Direction 3: Directly Assess Depressed Persons’ Negative Beliefs About Adaptive ER and Positive Beliefs About Maladaptive ER Strategies
People with depression might hold specific beliefs about both adaptive and maladaptive ER strategies, which will influence their use of those strategies and, accordingly, their depressive mood. Papageorgiou and Wells (2001a) investigated depressed individuals’ positive beliefs about rumination by interviewing participants with depression and identifying common theme(s) in their thoughts. Based on the initial data, they created the Positive Beliefs about Depressive Rumination Scale (PBRS; Papageorgiou & Wells, 2001b). Future work can expand Papageorgiou and Wells’s (2001a, 2001b) to capture beliefs about multiple maladaptive ER strategies and also to investigate negative beliefs about adaptive ER strategies, including perceived advantages and disadvantages of both using and not using various adaptive and maladaptive strategies. Using a similar validated self-report instrument that cover a broader array of strategies than the PBRS, future work can examine whether beliefs about ER strategies differ between depressed and nondepressed people. Further, models should be tested longitudinally to probe whether beliefs about ER strategies predict their endorsement, and whether this, in turn, predicts severity of depression symptoms. These studies will serve as a key next step in establishing whether the beliefs that depressed people hold about particular ER strategies drive their use.
Direction 4: Investigate the Trajectory of Benefits (and Costs) of Using Adaptive Versus Maladaptive Strategies
One important idea is that people with depression use more maladaptive ER strategies because they provide short-term emotional benefit, even if such usage results in longer term costs. There are challenges to testing this idea. Despite abundant research on outcomes of emotion regulation strategies (e.g., Gross, 2002; Haga, Kraft, & Corby, 2009), there is mixed evidence on whether maladaptive ER strategies produce short-term emotional benefits, more so than adaptive ER strategies (Egloff, Schmukle, Burns, & Schwerdtfeger, 2006; Levitt, Brown, Orsillo, & Barlow, 2004). Further, most previous studies focused on immediate impact of ER strategies within a single domain (Dan-Glauser & Gross, 2011; Egloff et al., 2006; Levitt et al., 2004), and no study has yet examined relatively long-term benefits of multiple ER strategies within various domains. Thus, more research is needed to establish the temporal benefits of each ER strategy for multiple outcomes—such as affective, cognitive, and task-related outcomes—and covering several domains.
To further illustrate how costs and benefits might be assessed in carefully controlled designs, we recommend adopting previously used methods (Egloff et al., 2006; Levitt et al., 2004) to randomly assign depressed and nondepressed persons to multiple ER-strategy groups prior to a stress task (e.g., a speech task). Participants are trained to use each ER strategy before the task, complete the task, have a recovery period, and then unexpectedly perform the task again 30 minutes later. A battery of outcome measures assessing affective (e.g., self-reported emotions, and physiological measures such as skin conductance), cognitive (e.g., a memory task about the speech content), and task-related outcomes (e.g., task performance evaluated by a third assessor) could be administered at baseline, right after the task (immediate effect), and 30 minutes later (longer term effect). Although it would not capture the long-term effects, this work would allow first steps to examine the different temporal benefits and costs of ER across domains, and also can examine whether this differs between depressed and nondepressed groups.
Direction 5: Clarify Whether Preference for Sad Stimuli in Depression Impacts ER Strategy Choice
Depressed persons’ usage of maladaptive strategies might stem from their conscious or unconscious desire to maintain sad states. If this is the case, it would be reasonable for interventions to focus on altering emotional preferences. Previous studies examined preference for sad states by examining preference for sad stimuli that produce the states (e.g., sad images or music; Millgram et al., 2015; Yoon et al., 2019). However, as we discussed before, this design overlooks the possibility that exposure to sad stimuli might not produce only sad states, but also positive emotional states such as calmness (see Yoon et al., 2019). To overcome this limitation and clarify what emotional states depressed persons prefer, a future study needs to examine affective outcomes of their preferred stimuli (whether depressed persons feel better or sadder after engaging with their chosen stimulus). If a depressed person feels less depressed after engaging with a sad stimulus, it is logical to infer that the person does not want to feel sad even though he/she chose a normatively sad stimulus.
Use of ecological momentary assessment (EMA) designs may be beneficial to allow repeated testing of emotional preferences in more naturalistic contexts. For example, depressed participants could be asked to choose from a menu of songs that are normatively happy or sad, and the effects of these choices could be assessed at multiple assessment points. EMA designs also permit examination of what music is listened to during periods of low mood, as well as the beliefs about the effects of music on mood. Such work can help us confirm, or refute, the idea that depressed persons try to upregulate sadness because they prefer sad states.
Reflections Upon the Future
The empirical record of clinical science shows the value of revisiting untested assumptions. For example, mental health professionals had long presumed that bereaved persons should work through memories and feelings about the deceased, until researchers later found that such “grief work” may not be effective or may even interfere with ordinary bereavement (Bonanno, 2004). Likewise, our review reveals the value of testing assumptions about emotion regulation usage in the context of depression. Given that research on depression and ER is expanding rapidly, what is most needed at this juncture is to correct misconceptions regarding ER strategy employment in depression, to take stock of what we know, and to sketch key future research directions designed to help improve our clinical description of depression and ER.
Although our focus has been on depression, we believe that our analysis can provide a helpful framework for thinking about a range of psychological disorders that evidence problematic ER strategy use. We hope other scholars follow suit. For example, it is possible that many of the proposed 10 explanations can be applied to anxiety disorders. Carthy et al. (2010) showed that children with anxiety disorders were able to successfully implement cognitive reappraisal to reduce their negative emotional reactivity to negative images when instructed in the lab (Explanation 1: the ability to implement adaptive strategies). However, children with anxiety disorders in the same study (Carthy et al., 2010) demonstrated poor knowledge concerning cognitive reappraisal tactics, which was shown by a reduced production of positive or neutral statements regarding negative images when instructed to use cognitive reappraisal, compared to nonanxious children (Explanation 2: knowledge of ER tactics).
Further, we also believe that applying our analysis to multiple psychological problems will enhance our knowledge on both what is transdiagnostic (what applies across disorders) about why people with psychopathology endorse higher levels of maladaptive ER strategies, and pathway(s) that are disorder-specific. For instance, some disorders might have relatively little involvement with maladaptive ER strategy usage. A meta-analytic article showed that substance-use problems may be less related to faulty ER strategy choice than other conditions (i.e., smaller effect sizes than depression and anxiety; Aldao et al., 2010). Finally, still other disorders might evidence a mix of pathways to maladaptive ER that contain both transdiagnostic and disorder-specific paths.
Finally, this work has clinical implications. Changing ER strategy usage has long been a focus for both traditional treatments such as CBT (i.e., a therapy that enhances cognitive reappraisal by helping clients correct their negative automatic thoughts), and newer treatments that explicitly focus on ER, such as emotion regulation therapy (Mennin, 2004) or dialectical behavior therapy (Linehan et al., 1999) that provide skills training and/or general education about ER. Future research, guided by our work, may reach stronger conclusions on how and why both traditional and newer treatments change ER strategy choice, and how these treatments might be enhanced to more efficiently alter ER strategy use in the future. In turn, researchers should utilize the insights gained in clinical studies to better understand how maladaptive ER use operates, and the pathways by which it operates.