
Abstract
Persistent idiopathic facial pain (PIFP), formerly known as ‘atypical facial pain’, is a dull, constant, poorly localised ache in the face (most commonly the maxilla) that is not associated with any other clinical signs or pathology. It has no known cause and is therefore not a true diagnosis but rather a description. This article sets out to describe the ways in which PIFP may present in primary care, and discuss the key differential diagnoses to be excluded.
The GP curriculum and persistent idiopathic facial pain
Manage primary contact with patients who have a common/important ENT, oral or facial problem Demonstrate empathy and compassion towards patients with ENT symptoms that may prove difficult to manage, e.g. facial pain Be aware of the need to refer patients with oral disease to appropriate specialist services in oral medicine or oral and maxillofacial surgery Refer patients with dental or gingival problems to their general dental practitioner or local community dental services
Be able to demonstrate how you manage primary contact with patients who have a neurological problem Know the epidemiology of common and/or important neurological conditions such as epilepsy, headache and facial pain syndromes Coordinate care with other primary care health professionals to enable chronic disease management and rehabilitation Describe the indications for referral to a neurologist for chronic conditions requiring on-going specialist management
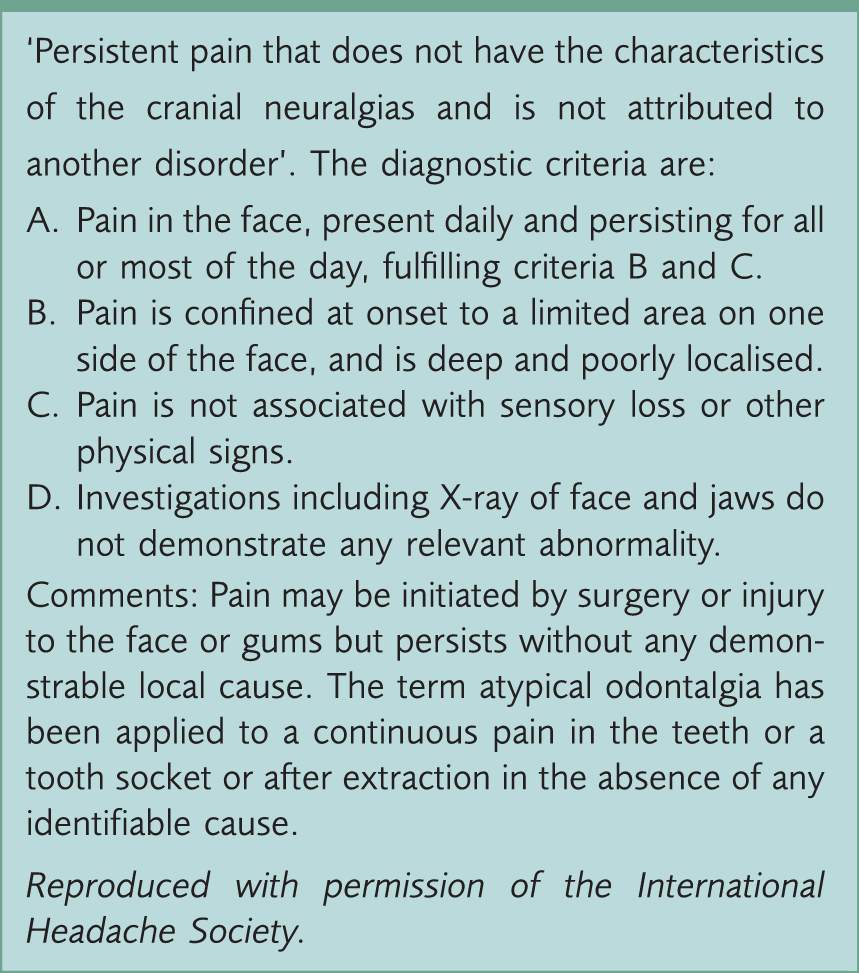
Diagnostic criteria
International Headache Society diagnostic criteria for PIFP.
Aetiology
PIFP has no known aetiology. It is, however, often preceded by a history of trauma or dental treatment such as tooth extractions or root canal therapy, which has led some authors to suspect that it may be a result of subclinical nerve damage. Studies have shown that on quantitive sensory testing and blink reflex examination a proportion of these patients do have mild sensory changes (Forssell, Tenovuo, Silvoniemi, & Jaaskelainen, 2007). It is likely that some patients presenting in this manner may actually have subclinical neuropathy.
Others argue that PIFP may have a psychogenic origin, pointing out that around one-third of affected patients also suffer from depression (Aghabeigi et al., 1993). However, a deficit in tyramine conjugation has been demonstrated in PIFP patients with or without depression (Aghabeigi et al., 1993). Moreover, there are changes in brain activity in patients with PIFP compared with healthy controls consistent with those seen in other chronic pain syndromes (Derbyshire et al., 1994). These would suggest a neurobiological basis to the condition.
Epidemiology
PIFP is rare. In a study of 6000 members of the general population in Germany the prevalence of PIFP was estimated at 0.03% (Mueller et al., 2011). Another study, this time using a GP-based database in the Netherlands, estimated an incidence of 4.4 per 100 000 per year (Koopman et al., 2009). However, when atypical odontalgia (thought to be a localised version of PIFP affecting only a small area around either a tooth or extraction socket) has been studied it has been shown to affect between 3 and 5% of all root-treated teeth (Polycarpou, Ng, Canavan, Moles, & Gulabivala, 2005). PIFP is twice as common in women than men.
Differential diagnosis
The classification of chronic orofacial pain is still a hotly debated topic. In the past the term ‘atypical facial pain’ has been used to describe jaw pain that was not typical of neuralgia-type pain. Historically, it has been used as an umbrella term to encompass groups of conditions that did not fit within the accepted knowledge base at that time. Consequently, different specialties with different viewpoints and expertise placed different conditions in this category, and the usage became confusing. With time, and advances in understanding of pain conditions, certain entities have become more widely recognised and as such the diagnostic sieve has been refined.
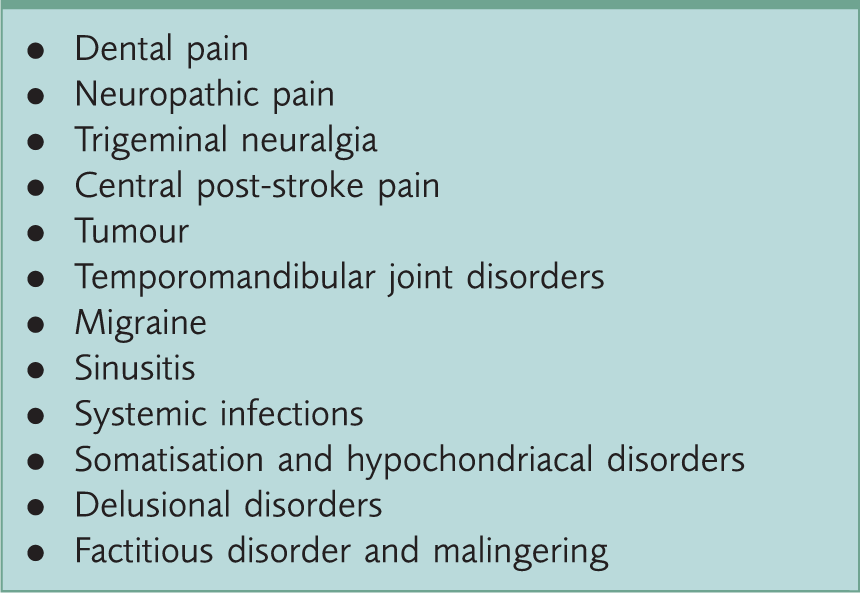
Differential diagnosis of PIFP.
Dental pain
The deep and poorly localised nature of PIFP is similar to early toothache. It is essential to exclude potential dental problems. However, pain of dental origin usually changes over time, progressing from an intermittent, poorly localised pain provoked by hot or cold stimuli to a constant severe throbbing pain that disturbs sleep, finally localising to a specific tooth that may be tender to percussion or finger pressure. A dentist can identify dental problems by checking for dental caries clinically and on dental radiographs, as well as performing vitality testing of teeth to assess response to thermal stimuli (usually ethyl chloride spray on a cotton roll, or electrical stimuli via a tooth pulp tester).
Neuropathic pain
There are close parallels between PIFP and neuropathic pain. History and presentation may be similar, but neuropathic pain also includes sensory symptoms. These can be positive symptoms such as hyperalgesia and dysaesthesia, or negative symptoms of reduced sensory response to touch, pinprick, temperature or vibration.
Post-herpetic neuralgia is probably the best understood neuropathic pain condition. It follows reactivation of herpes zoster infection in the nerve distribution of the affected site (shingles). However, neuropathic pain can also follow other types of nerve insult, especially after trauma or surgery. It should be managed in accordance with National Institute for Health and Care Excellence (NICE) guidelines on this condition (NICE, 2010).
Trigeminal neuralgia
This is usually a short, sharp stabbing pain felt in the region of either the second or third branches of the trigeminal nerve. However, it can atypically cause a constant background pain that is present between stabbing episodes. There may be an accompanying trigger point, the stroking of which can elicit a paroxysmal attack. See the accompanying article in this series for a more complete description of the diagnosis and management of trigeminal neuralgia (O‘Neill & Rajlawat, 2013)
Central post-stroke pain
If a stroke produces a lesion that affects the spinothalamic pathway, pain can result. As with other forms of neuropathic pain, this syndrome is accompanied by impairment of sensation to touch or temperature. Usually, however, other areas of the affected side are involved and weakness as well as sensory symptoms may be apparent. The pain starts suddenly and is usually associated with other neurological deficits characteristic of stroke.
Tumours
Tumours of the head and neck region may present with pain. Statistics from Cancer Research UK state that the incidence of oral cancer in the UK is 6539 persons per year (Cancer Research UK, 2013). Occult tumours in the maxillary sinus could generate pain in the mid-face similar to that of PIFP. Symptoms usually worsen progressively and can be accompanied by a loss of function or sensation. This combination of symptoms should raise suspicion and prompt referral for a specialist opinion and further investigations, including imaging. Facial pain around the ear or temple can also, rarely, occur as a consequence of invasion of the vagus nerve by lung carcinoma; any history suggestive of this diagnosis thus warrants appropriate investigations (e.g. chest X-ray and referral for specialist respiratory review).
Temporomandibular joint disorders
Pain can be referred from either the temporomandibular joint (TMJ) or from muscular trigger points in any of the muscles of mastication or, less commonly, the muscles of facial expression. Pain from the TMJ is usually worse on use and, if the joint is inflamed, there will be tenderness during palpation of the overlying area. Muscular trigger points can be felt as firm fibrous bands (or knots) in the muscle tissue. They can either be active or latent. A latent trigger point will be locally tender to palpation, whereas an active trigger point will be both locally tender but also refer pain to other areas. If a trigger point is located and its palpation aggravates the presenting pain then this may be the source.
When treating TMJ disorders consideration should be given to physiotherapy if any of the muscles of mastication or neck are painful on palpation, as this can help reduce referred pain that is of muscular origin. Physiotherapy may be accessible through some hospital-based services, and general dentists can provide a mouth guard to reduce forces during grinding of the teeth. If such services are unavailable, the patient should be advised to do simple stretching exercises and self-massage at home. He or she should also be advised to rest the area, and apply heat and topical non-steroidal anti-inflammatory drugs. The accompanying article in this series about TMJ disorders provides a more complete description of the diagnosis and management of this condition (Field, Steele, & Thayer, 2013).
Migraine and medication overuse headache
Migraine can present with persistent daily pain in and around the face. Usually migrainous episodes consist of intermittent pain lasting between 4 and 72 hours, with intervening pain-free periods. However, an increasing dependence on simple analgesia can cause the headache to transform, with pain-free periods becoming shorter and shorter until the pain occurs daily with very little time between attacks. It may present with or without aura, but migraine without aura is more common. There are usually accompanying symptoms, including: nausea, photophobia, phonophobia and osmophobia. Prodromal symptoms such as tingling, mood disturbance and cognitive dissonance may precede attacks. Migraine may become worse with exertion, whereas this not the case for PIFP.
Sinusitis
Sinusitis tends to present acutely alongside other symptoms of an upper respiratory tract infection. Typical symptoms include stuffiness of the nose and tenderness over the sinus cavity. Pain characteristically worsens on bending over, for example, when putting on shoes. Chronic sinusitis is often associated with a chronic nasal discharge. Both may cause symptoms of facial pain, but acute sinusitis usually abates after a short duration; it is chronic sinusitis (that may be present for several months and therefore in the same time frame as PIFP) that needs to be excluded.
Multisystem disorders
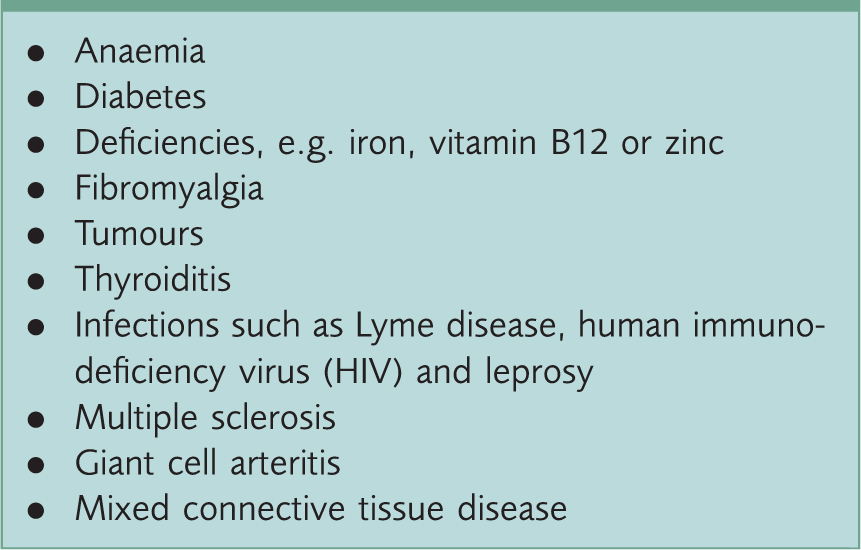
Systemic causes of facial pain.
Psychiatric disorders
Many patients with PIFP readily give accounts of anxiety, depression, behavioural problems, psychosocial issues, or illness behaviour, suggesting a psychiatric origin for - and/or psychiatric effects of - their pain. Adding to this picture, patients may also describe pain in terms suggestive of heightened perception, with the nature and degree of pain being unrelated to any recognised pathophysiology, and associated with unexplained complaints such as orofacial swellings, lesions, fluids and odours that are never found despite repeated clinical examinations. While anxiety and depression are common in chronic pain conditions and may often be caused by the daily struggle of living with PIFP, this needs to be distinguished from the less common but important psychiatric conditions described in the following sections.
Somatisation and hypochondriasis
The main features of somatisation are multiple, recurrent and frequently changing physical symptoms, and a long and complicated history of contact with medical services, negative investigations and unsuccessful treatment. When the search for pathology linked to a compliant in one area of the body has been exhausted the focus of the compliant may move to another area or system of the body. Often patients are unaware of their pattern of behaviour. Hypochondriasis, as with somatisation, may lead to many contacts with medical services. However, it differs from somatisation in that in hypochondriasis the focus is on the feared presence of an underlying serious disease.
Factitious disorder and malingering
In factitious disorder the patient intentionally and repeatedly feigns symptoms or disabilities for obscure reasons designed to elicit care. Malingering also involves the intentional production or feigning of symptoms, but differs in that it is motivated by external stresses or incentives (e.g. to obtain benefits). Full exclusion of pathology must be completed, even if factitious disorder or malingering is suspected, and in truth it may be impossible to prove if either of these conditions is present.
Delusions
True delusions of pain are extremely rare but may be the first sign of psychiatric disease. Bizarre, fixed, unshakeable beliefs expressed in terms of pain may be a feature of psychotic disorders such as schizophrenia with somatic delusions, and depressive disorders with hypochondriacal delusions.
Examination and investigations
In PIFP the clinical examination will be normal; however, a systematic examination is required to exclude potential differential diagnoses. This should begin with evaluation of the cranial nerves. Any abnormality in cranial nerve function may indicate the presence of an intracranial-space-occupying lesion, peripheral nerve pathology or a cerebrovascular accident, and should initiate a full neurological examination. It may also warrant referral for a specialist neurological opinion. Specific attention should be given to testing sensation in the distribution of the trigeminal nerve, which can be carried out by testing responses to cotton wool, pin-prick and temperature and also testing the corneal reflex.
Following a neurological examination, palpate the facial structures. Any tenderness over one or both cheeks, especially if associated with nasal stuffiness or discharge, may indicate the presence of sinusitis. Tenderness overlying the TMJs and pain on jaw movements may indicate TMJ pathology. Tenderness of the masseter or temporalis muscles, especially if associated with obvious wear of the teeth, may indicate pain from bruxism.
Intra-oral inspection may reveal obvious dental cavities, poor oral hygiene, or suspicious swellings or ulcers. Any of these may require referral to a maxillofacial surgery, oral surgery or oral medicine department, depending on the type of problem and local arrangements.
Blood tests may help to exclude rare causes of facial pain including: a full blood count for anaemia, fasting glucose/HbA1c for diabetes mellitus, vitamin B12 and zinc for deficiencies, thyroid function tests for thyroiditis, erythrocyte sedimentation rate for giant cell arteritis, and screening for Lyme disease, HIV and leprosy - if these infections are suspected. Imaging is of value, again to exclude other pathologies – most notably magnetic resonance imaging to exclude space-occupying lesions or tumours of the head and neck. If dental radiography has not been undertaken to rule out pain of dental origin then this should be carried out, either with the patient's general dental practitioner or through local referral to specialist services. If the process of examination and investigation reveals no evidence of clinical or psychological abnormality, and the pain has been present and similar in character for at least 3 months, then consider the diagnosis of PIFP.
Treatment
Successful management of PIFP often requires a multidisciplinary approach, mainly because the exclusion of the various differentials can be difficult, and psychiatric or psychological support may be necessary. Once the potential differential diagnoses are excluded and PIFP is suspected, then pharmacological or psychotherapy therapy can be instigated. The management options for PIFP are described in the following sections.
Pharmacotherapy
The drug treatment of choice for PIFP is a tricyclic antidepressant (TCA), although this is an unlicensed indication. Amitriptyline or nortriptyline (which may be better tolerated) are the best choices, starting with a dose of 10 mg at night, gradually increased if necessary to 75 mg daily; higher doses may be used under specialist supervision. Relief is usually of gradual onset and it is best to initially prescribe for a ‘trial’ period of around 12 weeks. Other options include serotonin and norepinephrine reuptake inhibitors (SNRIs) (e.g. duloxetine, venlafaxine and mirtazapine) and selective serotonin reuptake inhibitors (SSRIs) (e.g. fluoxetine), although the latter may be less effective.
Patients taking long-term TCAs need to be monitored both for progress and for side effects. Typical side effects include drowsiness, dry mouth, blurred vision and constipation, all of which are reversible if the TCA is stopped. TCAs can also have serious cardiac effects and hence are contraindicated in the immediate recovery period from myocardial infarction and in arrhythmias, particularly heart block. They should be used with caution in the elderly, who should be closely monitored for psychiatric and cardiac side effects, and in patients with heart disease. TCAs should be also used with care in patients with concomitant medical conditions that may be exacerbated, such as prostatic hypertrophy. When stopping a TCA, SSRI or SNRI the prescription should be tailed-off slowly to avoid withdrawal symptoms.
Psychological interventions
Any pharmacological treatment should be accompanied by psychological support, which may also require specialist referral. Psychological approaches are increasingly used in the management of patients who have chronic pain associated with disability and psychological distress. Cognitive behavioural approaches aim to improve the way patients manage and cope with their pain. The focus is on identifying and challenging negative thinking, anxiety, mood and patterns of behaviour, using techniques such as distraction and relaxation training. The outcome is variable, but many people find relief.
A systematic review of the relatively few studies of psychosocial interventions for the treatment of chronic orofacial pain showed that the risk of bias in many was high but, where pooling of data was achievable, beneficial effects for some outcome measures could be observed. The authors conclude ‘given the non-invasive nature of such interventions they should be used in preference to other invasive and irreversible treatments that also have limited or no efficacy’ (Aggarwal et al., 2011).
Self-help
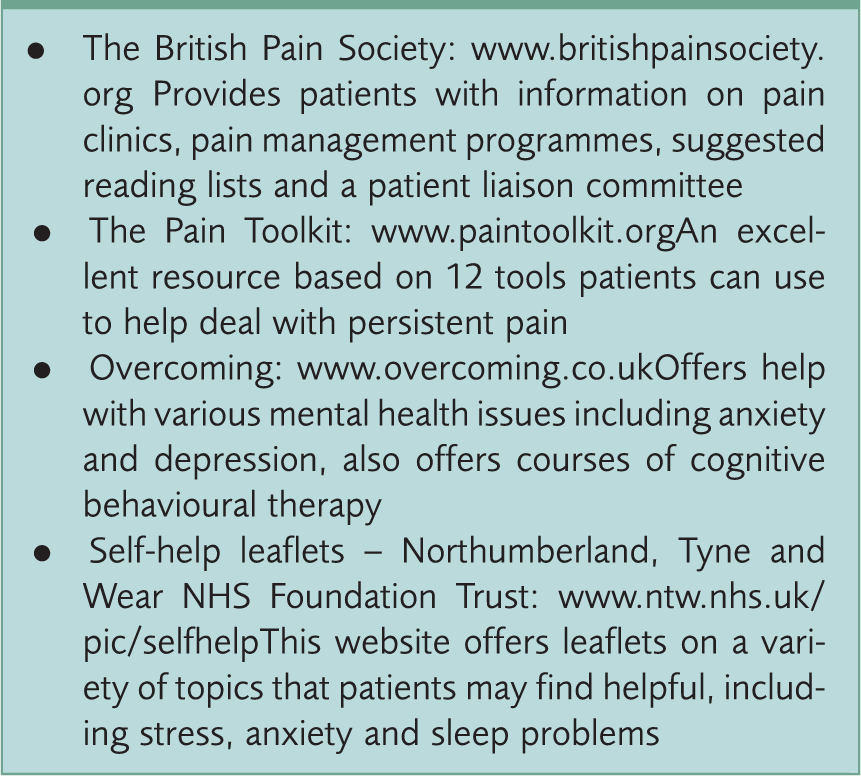
Self-help websites for patients.
Reasons for referral
There are a number of circumstances under which a referral should be considered. Foremost amongst these is if there is suspicion of serious underlying disease, in which case an urgent referral to the appropriate specialty will be required. Another important reason is if there is difficulty in excluding a differential diagnosis and/or further investigations are required. If the diagnosis in question is neuropathic pain, trigeminal neuralgia, central post-stroke pain, migraine or multiple sclerosis the patient should be referred to neurological services, whereas patients with potential head and neck tumours, sinusitis or TMJ problems should be referred to local maxillofacial surgery/ENT services.
Even after a diagnosis of PIFP has been made, referral may still be required. This includes situations in which there has been no improvement with therapy after 6 months or there are severe side effects of medication; refer such difficult cases to specialist pain management services. Similarly, further help should be sought if there is increasing distress or are psychiatric/psychological issues affecting management. Some pain management services have psychological therapy-based support programmes, otherwise a direct referral to local psychological services may be indicated.
Key points
PIFP is a diagnosis of exclusion and multiple tests may be required to exclude primary pathology Adequate investigation may require referral to more than one specialist for exclusion of differential diagnoses Treatment often requires a combination of pharmacological and psychological techniques