
Abstract
Gallstones are common, with an overall UK prevalence of approximately 20%. However, despite being so prevalent, only 20% of people with gallstones will experience biliary colic or complications such as cholecystitis, pancreatitis or cholangitis. The definitive treatment of gallstones is surgical removal of the gallbladder and laparoscopic cholecystectomy is now the most common abdominal surgical procedure performed in the UK, with around 60 000 operations annually. It is important for GPs to be aware of the ways in which gallstones and their complications can present in primary care and be able to distinguish between patients who need urgent surgical admission for intervention and those who may be referred more routinely via the outpatient setting.
The GP curriculum and gallstone disease
Be able to manage primary contact with patients who have a digestive problem Understand the epidemiology of digestive problems as they present in primary care and their often complex aetiology Know how to interpret common symptoms in general practice, including dyspepsia, abdominal pain, nausea, vomiting, anorexia, weight loss, haematemesis and melaena, rectal bleeding, jaundice, diarrhoea and constipation, and dysphagia Demonstrate a systematic approach to investigating common digestive symptoms, taking into account the prevalence of these symptoms in primary care and the likelihood of conditions such as peptic ulcer, oesophageal varices, hepatitis, gastrointestinal cancers and post-operative complications Understand that digestive symptoms are frequently linked to psychosocial factors and empathise with individuals who are psychologically distressed Explore gastrointestinal symptoms and psychological and social factors using an integrated approach Intervene urgently when patients present with an acute abdomen Be cautious with telephone advice when the abdomen has not been examined Understand dietary factors associated with various gastrointestinal conditions and offer appropriate dietary advice Identify patients’ attitudes and beliefs about digestive symptoms and disease, and how they might influence patterns of presentation Advise patients appropriately regarding lifestyle interventions that have an impact on gastrointestinal health, such as advice on diet and on stress reduction
The prevalence of gallstones in the UK population has historically been reported from autopsy studies to be approximately 12% in men, and 24% in women (Godfrey, Bates, Harrison, King, and Padley, 1984). However, prevalence significantly varies throughout the UK and estimated prevalence in more socio-economically deprived areas is as high as 50% (Gurusamy & Davidson, 2014). This would appear to be indirectly supported by the fact that there is a threefold variation in laparoscopic cholecystectomy rates across the UK Clinical Commissioning Group areas, ranging from 112 procedures per 100 000 population to 371 per 100 000 population (Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland, 2013).
Risk factors for the development of gallstones.
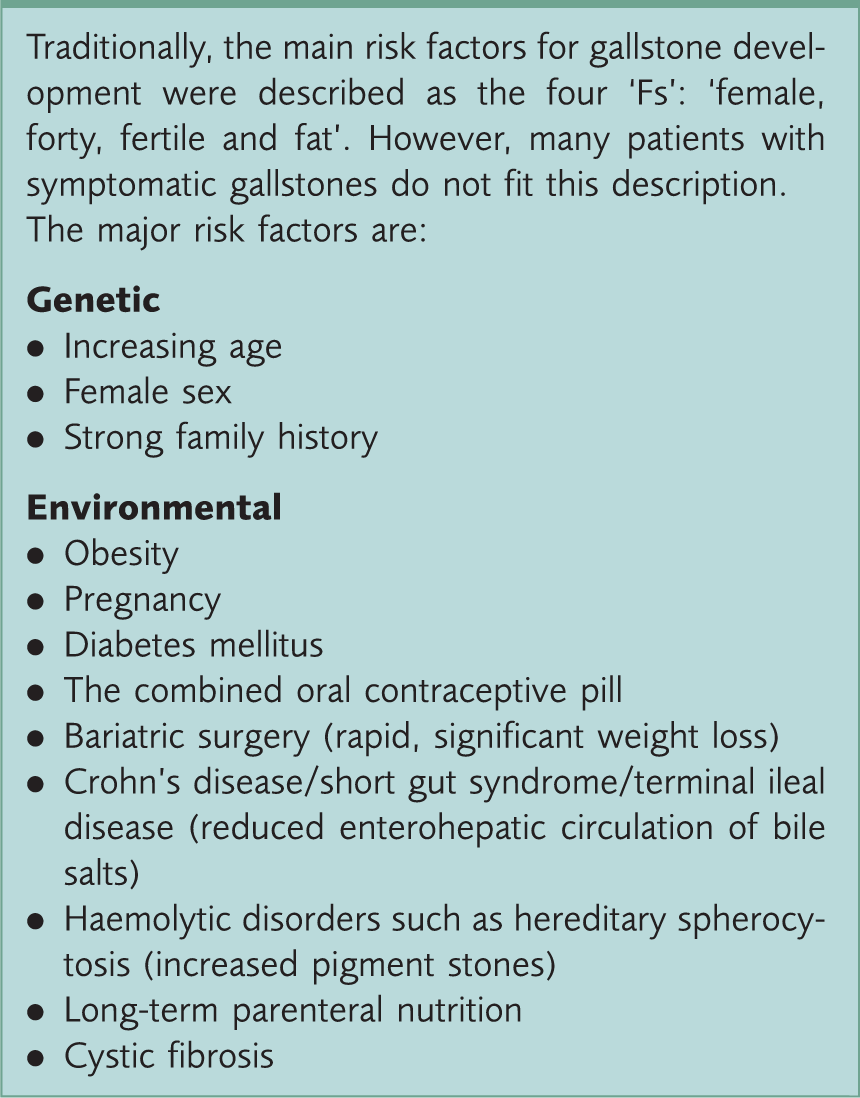
However, despite a high prevalence, gallstones remain an incidental finding in most people, with studies suggesting that approximately 20% of patients with gallstones are symptomatic, with only around 2% of patients with gallstones actually become symptomatic every year (Gurusamy & Davidson, 2014). With obesity levels continuing to rise rapidly, it is likely that GPs can expect to see and manage more gallstone-related complications in the coming years. Worryingly, there is also evidence that acute gallstone-related admissions are increasing in the paediatric population, perhaps also reflecting an increase in obesity in this population.
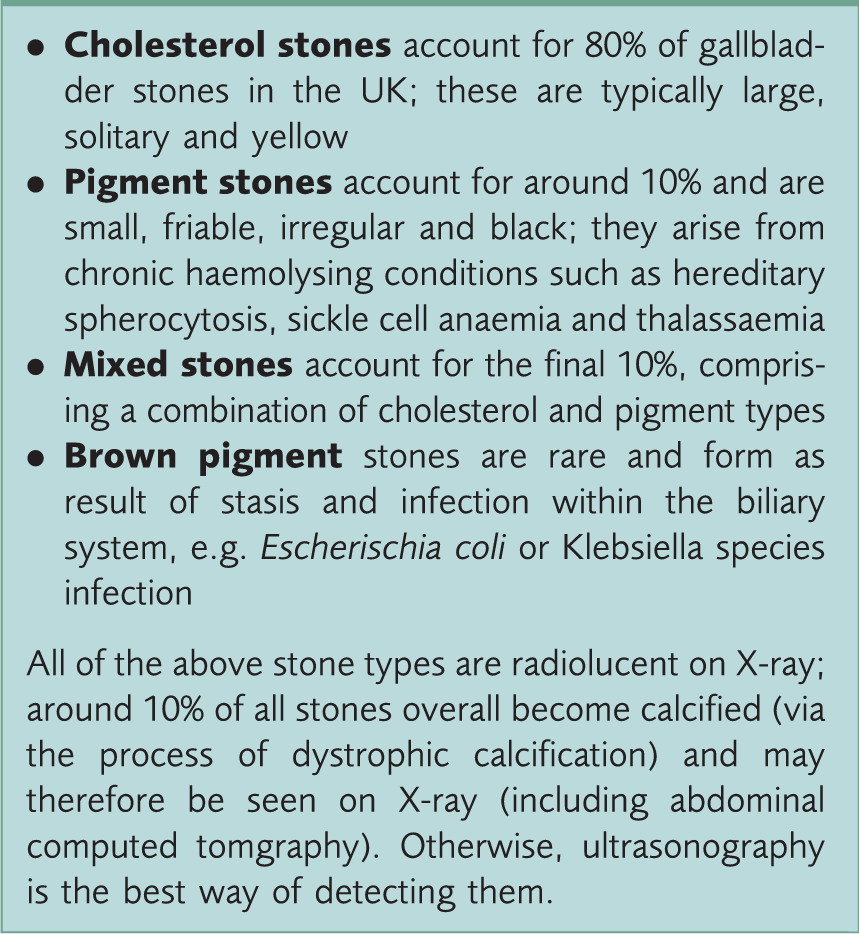
Types of stone
Gallstone composition.
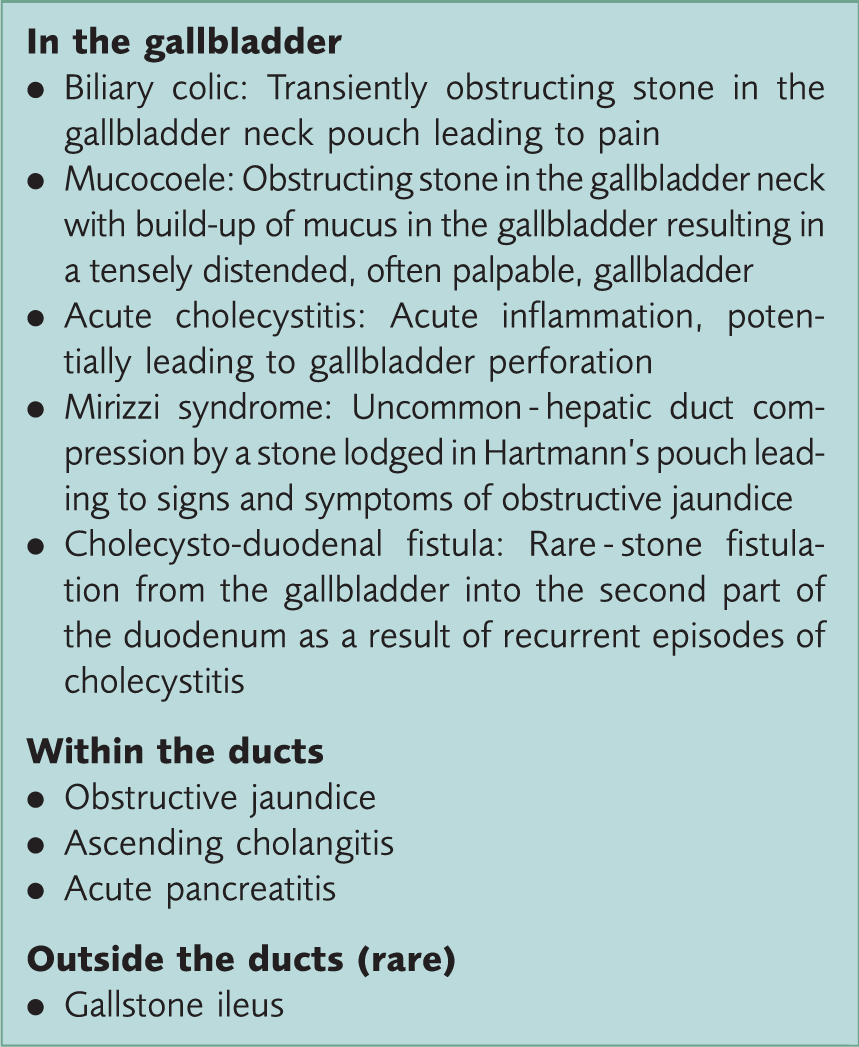
Complications of gallstones
A simple method of remembering the potential complications of gallstones is to consider the potential sequelae of gallstones according to anatomical location, i.e. in the gallbladder, in the ducts and (rarely) outside the ducts (see Fig. 1). These potential complications are described in Box 3.
The anatomy of the biliary tree. Gallstone-related complications according to anatomical site.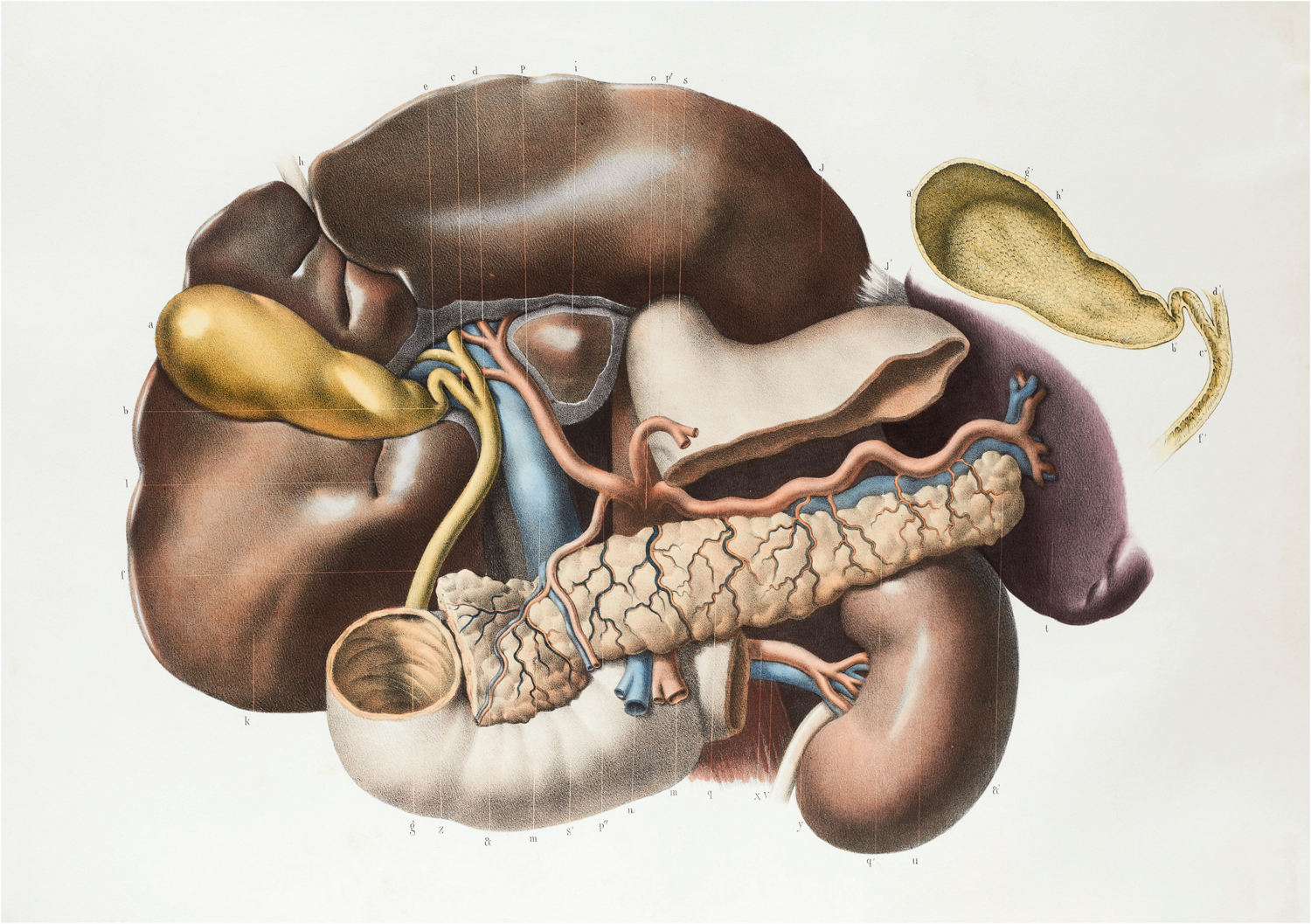
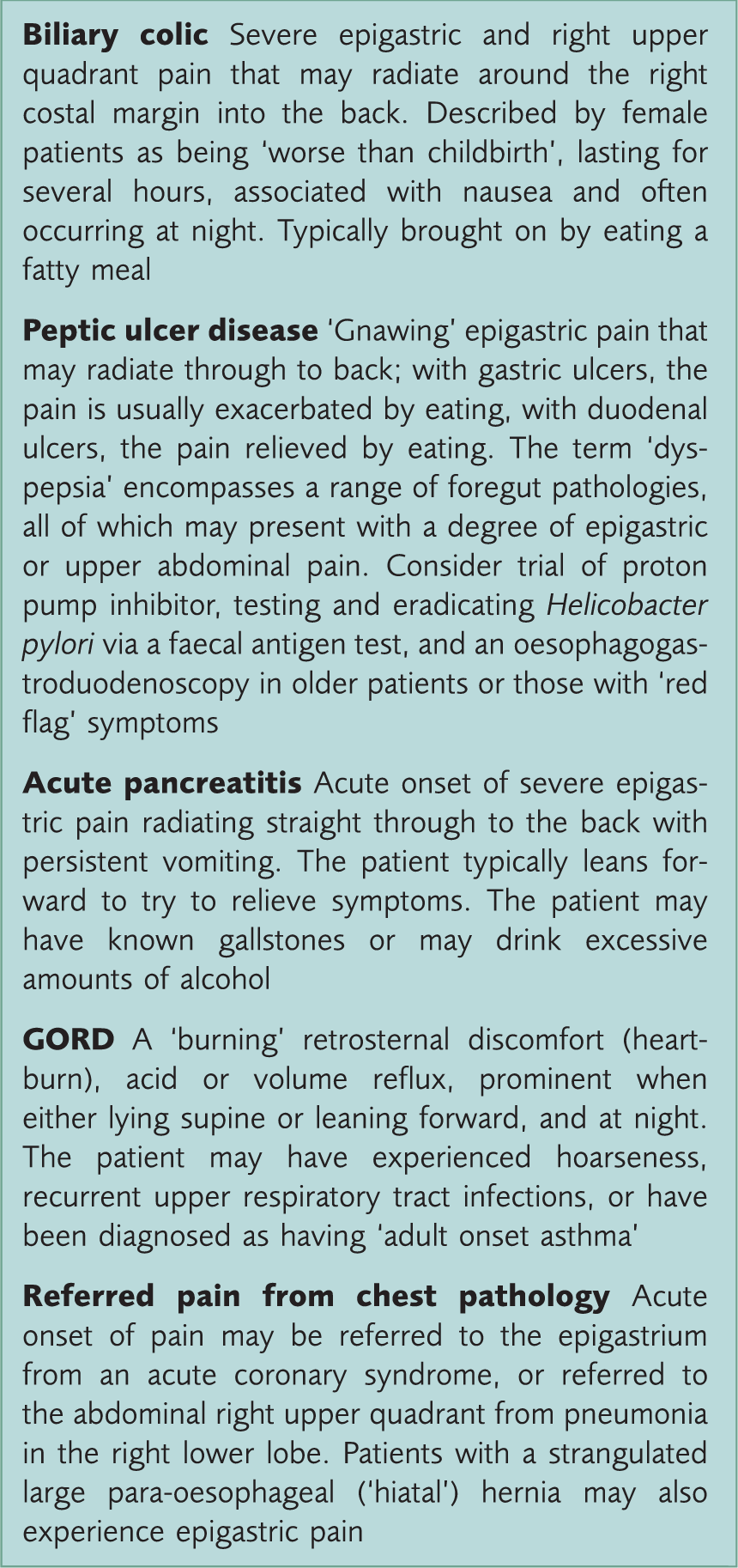
Biliary colic
Biliary colic is the most common presentation of gallstone disease, and describes a visceral pain caused by a gallstone transiently obstructing the neck (Hartmann's pouch) of the gallbladder. Despite the name, the pain tends to be constant rather than colicky, and is caused by contraction of the gallbladder against an obstructed outlet. Gallbladder contraction is stimulated by the hormone cholecystokinin, released by duodenal mucosal cells in response to food, particularly fatty foods. It follows that pain is triggered by a fatty meal, and resolves as either the stone dislodges back into the gallbladder, or is propelled through the cystic duct in to the common bile duct.
Patients typically describe epigastric and right upper quadrant pain, radiating around the right side to the back. The pain is usually severe (female patients compare its severity as being equivalent to that of childbirth), and associated with nausea and vomiting. It typically begins shortly after eating a fatty meal, often in the evening or at night, and lasts for several hours.
Biliary colic and its differential diagnosis.
In patients who present with convincing biliary colic but have no ultrasound evidence of stones, and in whom other differentials have been excluded, a repeat ultrasound can be considered. The overall sensitivity for the ultrasound detection of stones when present is around 90 – 95%, and depends on a number of factors, including the patient’s body habitus (gallstones are more difficult to visualise in obese patients), whether the patient has been adequately starved pre-scan (the gallbladder distends after fasting and is more easily visualised), and the individual skill and experience of the ultrasonographer. A second ultrasound may therefore disclose stones not seen on the first, confirming gallstones as the likely source of pain, and allowing referral for consideration of cholecystectomy.
If there is still doubt about the presence of stones and the patient has typical symptoms of biliary colic, consider referral to secondary care (usually the upper gastrointestinal surgical team), where the next investigation may be an endoscopic ultrasound. This may help to identify the presence of tiny stones (microlithiasis) not seen with transabdominal ultrasound.
Most patients with biliary colic can be managed adequately within the primary care setting. Further episodes can be avoided in around 30% of patients by sticking to a strict low-fat diet. Following the onset of an acute episode of biliary colic, established pain can be controlled with simple analgesia, and there is evidence that non-steroidal anti-inflammatory medications in particular may also reduce progression to cholecystitis (Colli, Conte, Valle, Sciola, and Fraquelli, 2012). Opiate analgesia is effective in some patients, although traditional teaching suggests that opioids can exacerbate biliary pain by causing spasm of the sphincter of Oddi. There is limited evidence to support this claim, so working in partnership with the patient to negotiate a mutually agreeable individualised management plan is essential (Bird, 1986).
Patients with recurrent or troublesome symptoms, with confirmed gallstones on ultrasound should be referred to an upper gastrointestinal surgeon for consideration of laparoscopic cholecystectomy. The decision to operate is made by the patient with guidance from the surgeon including assessment of the risk of recurrent symptoms, risk of the development of serious complications, and risk of complication rates of surgery in relation to individual patient’s co-morbidites, age and preference. Current guidelines recommend that asymptomatic gallstones within the gallbladder, picked up as incidental findings, need not be referred. However, asymptomatic gallstones in the common bile duct should always be referred because of the higher risk of complications (Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland, 2013).
Acute cholecystitis
The main difference between biliary colic and acute cholecystitis is the inflammatory component in the latter. If a stone obstructs the neck of the gallbladder for long enough, local oedema secures the stone in place and the gallbladder becomes oedematous and inflamed. The fluid within the gallbladder is initially sterile, but may become infected, triggering a systemic inflammatory response. Increasing age and co-morbidity increase the likelihood of infection.
Acute cholecystitis is a surgical emergency. Therefore, distinguishing it from biliary colic is imperative. The cardinal symptom is rapid (but not sudden) onset pain in the right upper quadrant or epigastrium, which may radiate around to the right scapula tip (Boas’ sign). Nausea, vomiting and fever often accompany the pain. There may be a pyrexia and tachycardia, with marked right upper quadrant abdominal tenderness or guarding (peritonism). A distended gallbladder may be palpable, but alternatively may be shielded by the right costal margin. In this case, deep inspiration to bring the gallbladder down to palpating fingertips will result in pain and sudden cessation of inspiration as the inflamed gallbladder impinges on the depressed abdominal wall. This is known as ‘Murphy’s sign’ and will only be positive if the manoeuvre does not cause pain when repeated on the left side. Blood tests are likely to demonstrate a raised white cell count and C-reactive protein, although importantly the liver function tests may be normal if there is no obstruction of the common hepatic or common bile ducts.
Traditionally, the management of acute cholecystitis was to admit the patient for a course of intravenous antibiotics and fluids. An interval laparoscopic cholecystectomy would then be booked on a routine surgical waiting list once the acute episode had settled. However, over recent years there has been a trend for such patients to be operated on during their acute admission. Indeed, commissioning guidelines published by the Royal College of Surgeons of England in 2013 now recommend that patients with acute cholecystitis undergo immediate (acute or ‘hot’) cholecystectomy, as opposed to waiting for the gallbladder to ‘cool down’ before carrying out the procedure electively in the future. These guidelines emphasise the real risk of gallbladder wall necrosis and perforation with conservative therapy alone and therefore recommend acute cholecystitis be treated similarly to acute appendicitis, with a definitive operation on the index admission.
In frail, elderly patients with acute cholecystitis who are systemically unwell, laparoscopic cholecystectomy may be regarded as being too risky. In such patients, percutaneous cholecystostomy may be appropriate. Usually performed by an interventional radiologist, it comprises a local anaesthetic procedure performed at the bedside, using ultrasound guidance to insert a drainage tube into the inflamed gallbladder. Once the gallbladder is drained, the sepsis usually resolves very quickly. The cholecystostomy tube can be removed after a period of several weeks, once a mature tract has formed. During this time, and once the patient has made a recovery from the acute setting, consideration can be given as to whether an elective laparoscopic cholecystectomy is warranted, based on the patient's fitness for surgery.
Chronic cholecystitis
Chronic cholecystitis is a histological diagnosis only, based on a chronic inflammatory cell infiltrate seen in the wall of the gallbladder. It is thought to arise from recurrent episodes of acute cholecystitis leading to a thickening and fibrosis of the wall of the gallbladder. Its presence does not correlate with any specific clinical symptoms.
Mirizzi syndrome
Mirizzi syndrome is an uncommon syndrome that occurs in around 1% of patients with biliary colic or acute cholecystitis. A stone in the neck of the gallbladder or cystic duct causes oedema, which results in compression of the common hepatic duct, with a resulting obstructive jaundice. This is one cause of ‘painful obstructive jaundice’, the other being an obstructing common bile duct stone.
Ascending cholangitis
Ascending cholangitis is acute inflammation of the biliary tree. Obstruction of biliary ducts allows bacterial proliferation in the bile and rapidly leads to septicaemia, shock and death. Therefore, prompt diagnosis and intervention is essential. Charcot's triad is present in approximately 70% of patients and the combination of biliary colic, fluctuating jaundice and swinging fever should prompt swift referral to the acute surgical team (Miura et al., 2013). Older patients may present with non-specific symptoms such as malaise and confusion, and given acute cholangitis is more common in this population, it is important to take care not to miss this as a possible source of sepsis in older patients.
Although gallstones are the most common cause of ascending cholangitis, bile duct malignancy (cholangiocarcinoma) must also be considered, particularly in the elderly or where no gallstones have previously been seen on imaging.
Although blood tests, blood cultures and abdominal ultrasound scan (USS) will be part of the initial work up in these patients, there is a role for magnetic resonance cholangiopancreatography (MRCP) in confirming a definitive diagnosis. However, computed tomography (CT) may be used as an additional tool in patients in whom MRCP is contraindicated (e.g. patients with pacemakers). The definitive management of common bile duct stones is endoscopic retrograde cholangiopancreatography (ERCP). This allows the cause and site of obstruction to be confirmed, and allows therapeutic intervention such as stone removal, sphincterotomy or stenting of any obstruction.
Acute pancreatitis
Gallstones are the most common cause of acute pancreatitis in the UK. Sudden onset, severe upper abdominal pain, radiating to the back with nausea and vomiting, are all suggestive of acute pancreatitis. Examination of the patients should assess for tachycardia, tachypnoea, hypotension, pyrexia, abdominal rigidity, body wall bruising around the umbilicus (Cullen's sign) or flanks (Grey Turner's sign). Biochemically, the diagnosis is made with a serum amylase greater than around 300 (if 100 is the upper limit of normal).
It is recommended that a stable patient with a good history for pancreatitis and known gallstones should be referred for urgent cholecystectomy (Williams et al., 2008). However, any evidence of cardiovascular compromise or sepsis warrants urgent surgical admission, intravenous fluid resuscitation, pain control and close monitoring for sepsis. Once the patient is stable, it is recommended that the patient undergoes common bile duct clearance (usually via ERCP) and cholecystectomy on the same admission (Williams et al., 2008). MRCP may be preferred prior to intervention to confirm the presence of common bile duct stones.
Common bile duct stones
Causes of obstructive jaundice.
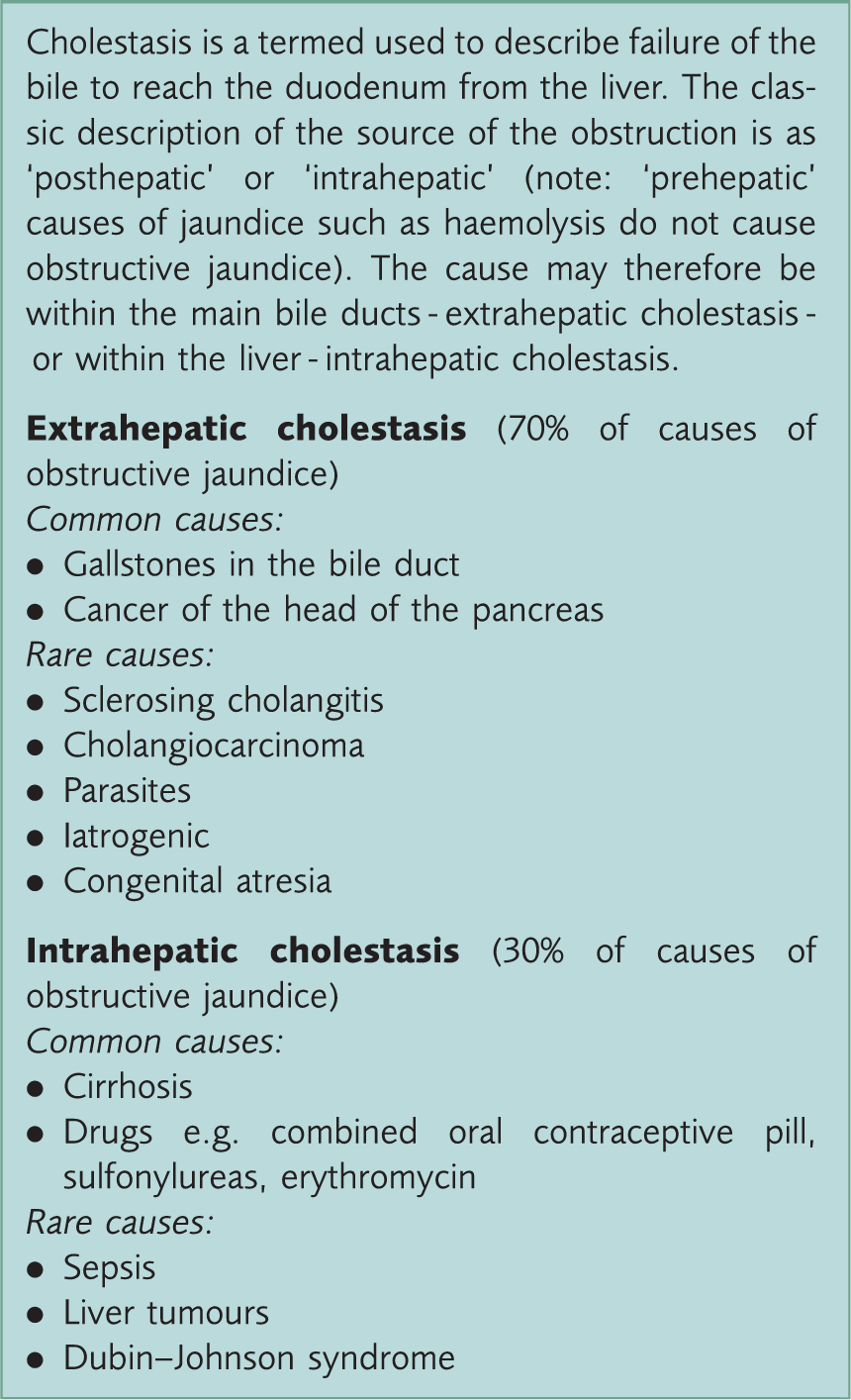
Patients in whom laboratory testing and USS have confirmed common bile duct stones will generally proceed to urgent laparoscopic cholecystectomy and intra-operative cholangiogram. For poor surgical candidates or patients with evidence of acute cholangitis, urgent ERCP may be the preferred option, with postponed cholecystectomy if deemed fit for surgery. In patients in whom the diagnosis is in doubt despite USS, MRCP may be performed to confirm the definitive diagnosis prior to undergoing invasive treatment.
Patients who have previously had a cholecystectomy can occasionally still form primary common bile duct stones, which may obstruct. Guidelines recommend that these patients undergo ERCP and endoscopic stone extraction, with considerations of a biliary stent if stones are irretrievable (which again may be definitive treatment if the patient is unfit for surgery) (Williams et al., 2008).
Gallstone ileus
Gallstone ileus is actually a misnomer. It is a rare mechanical small-bowel obstruction caused by an obstructing stone in the distal small bowel (the narrowest part of the small bowel). It is facilitated by a fistula between the gallbladder and duodenum (cholecystoduodenal fistula); the end result of many episodes of cholecystitis.
Gallstone ileus is diagnosed on plain abdominal X-ray by ‘Rigler’s triad’; the presence of small-bowel obstruction, calcified stone in the lower abdomen and gas in the biliary tree (pneumobilia). Note that this is different to Rigler’s sign, the presence of extra-luminal gas indicating a bowel perforation. Management is a laparotomy and small-bowel enterotomy to remove the stone. The fistula itself is very rarely resected due to the risk of damaging the common bile duct.
Gallstones in pregnancy
Gallstones are more common during pregnancy, largely due to the effect of hormones on the biliary system. Oestrogen increases cholesterol secretion whereas progesterone reduces bile aid secretion, resulting in the bile becoming supersaturated with insoluble cholesterol. Furthermore, progesterone reduces gallbladder motility, with relative stasis of bile-promoting stone formation.
The presentation of gallstone disease during pregnancy is not dissimilar to the non-gestational state. Fewer than 2% of woman with gallstones develop symptoms, and the most common symptomatic presentation is biliary colic. Acute cholecystitis, cholangitis and gallstone pancreatitis are relatively rare initial manifestations.
The criteria for diagnosis of gallstone disease in pregnant women are much the same as in non-pregnant women. Blood tests are typically normal during asymptomatic periods and during attacks of colic.
Significantly raised bilirubin, alkaline phosphatase and transaminases should raise the possibility of a common bile duct (CBD) stone, cholangitis or Mirrizi syndrome, although differentials such as ‘HELLP syndrome’ (haemolysis, elevated liver enzymes and low platelet count) should be considered in a pregnant lady. Furthermore, it should be remembered that the normal range for white cell count is higher in pregnancy, which reduces the diagnostic usefulness of this test for infection.
Ultrasonography is a safe, reliable and accurate method for the identification of gallbladder stones in pregnancy. CBD stones may be more difficult to identify via transabdominal USS and therefore complicated cases may necessitate MRCP (as CT and plain radiography are generally contraindicated in pregnancy).
For pregnant patients with a first episode of biliary colic, management is usually supportive and theoretically can be achieved in the community. Women should be advised to use simple analgesia and avoid eating during an acute attack (which exacerbates the pain with cholecystokinin-causing gallbladder contraction). This will lead to resolution of symptoms in most cases. However, in reality, most pregnant ladies with biliary colic will have brief inpatient admission to optimise pain control, exclude important differentials of right upper quadrant/epigastric pain in pregnancy (including acute fatty liver of pregnancy and HELLP), and ensure that complications do not develop.
Recurrence of biliary colic later in the pregnancy is very common, and women are usually offered elective cholecystectomy if pain is bothersome. With a laparoscopic approach, this is a safe procedure for mother and baby, and is performed in the second or third trimester. If troublesome colic occurs nearer to term, it is generally advisable to wait until 6 weeks post-partum.
Any evidence of more complicated biliary pathology, such as acute cholecystitis, warrants urgent hospital admission. Acute cholecystitis is an indication for urgent cholecystectomy, and given the high risk of serious complications and recurrence of infection without definitive surgery, pregnancy does not negate the need for emergency laparoscopic cholecystectomy. Providing adequate attention is paid to altered physiology and anatomy, this is a safe procedure for mother and baby, and pregnancy alone does not appear to increase post-operative morbidity.
Gallbladder cancer
Gallbladder cancer is an uncommon but aggressive malignancy. The presence of gallstones is the strongest risk factor for the development of gallbladder carcinoma. Patients with early disease are usually asymptomatic, with malignancy found during routine histopathology examination of the gallbladder after elective cholecystectomy (Carriage & Henson, 1995). Surgery is the only potentially curative treatment for gallbladder cancer. Patients with localised disease are offered cholecystectomy together with resection of the underlying liver, regional lymph nodes and extrahepatic biliary ducts.
Unfortunately, over 90% of patients have locally advanced disease with or without distant metastases, and present too late for surgery. Therefore, the focus of management in most patients’ treatment is palliative, aiming to relieve pain, jaundice, bowel obstruction, and maintain quality of life.
Gallstones following bariatric surgery
Obesity and rapid weight loss are both risk factors for gallstone formation, so it is no surprise that approximately one-third of patients may develop gallstones after bariatric surgery. Furthermore, up to 15% of all patients will require cholecystectomy for symptomatic gallstones (Sioka et al., 2014).
Some surgeons routinely perform a cholecystectomy at the time as weight loss surgery to prevent gallstone-related complications. However, other clinicians suggest that the operation may increase the overall operative time and length of hospital stay, and that cholecystectomy may be easier to perform after weight loss.
It is important to remember that some bariatric procedures such as gastric bypass, may preclude endoscopic intervention due to altered anatomy, therefore ERCP is impossible via the conventional route. In such patients, MRCP may be indicated to confirm ductal stones. If present, common bile duct stones may still be removed surgically via common bile duct exploration or through the use of techniques such as percutaneous ERCP.
Key points
Incidentally found gallstones (for example, on a scan performed for other reasons) in an otherwise normal gallbladder without symptoms of biliary colic require no further action Gallstones in a patient with typical biliary colic symptoms should prompt consideration of referral for elective laparoscopic chlolecystectomy Patients with suspected acute cholecystitis, ascending cholangitis or acute pancreatitis should be referred to hospital as an emergency Laparoscopic cholecystectomy is currently the gold standard method of gallstone management CBD stones should be treated with ERCP and sphincterotomy, with interval laparoscopic cholecystectomy if fit for surgery If gallstones are found in patients with acute pancreatitis