
Abstract
There is great potential within general practice for doctors to neglect their own physical, emotional and spiritual needs as a result of the ever-increasing demands of their role. Such neglect is neither in the interests of doctors, their families or their patients. Ultimately, a healthy, balanced and emotionally stable doctor is a doctor who is likely to make better decisions. Looking after patients with palliative care needs can place particular burdens on GPs, especially if there has been a long-term relationship with the patient; the patient evokes memories of close personal experiences from the past; or the physical and emotional burdens that the patient faces are unusually difficult. This article will look at the issues surrounding compassion fatigue, burnout and resilience, and discuss the ways in which a GP can devise strategies to manage the former while trying to build the latter.
The GP curriculum and palliative self-care
Awareness of your own capabilities and values Delivering care with compassion and kindness Being able to identify the ethical aspects of your clinical practice (prevention, diagnostics, therapy, factors that influence lifestyles) Awareness of self: Understanding that your own attitudes and feelings are important determinants of how you practice Being aware of the interaction of your work and your private life, and striving for a good balance between them
Recognise, monitor and manage personal emotions arising from the consultation Recognise how personal emotions, lifestyle and ill-health can affect your consultation performance and the doctor–patient relationship Have an awareness of your own capabilities, values and ethics Identify your own strengths and limitations, the impact of your behaviour on others and the effect of stress on your own behaviour Identify your own emotions and understanding how these can affect your judgement and behaviour
Compassion fatigue
Symptoms of compassion fatigue include different dimensions of wellbeing.
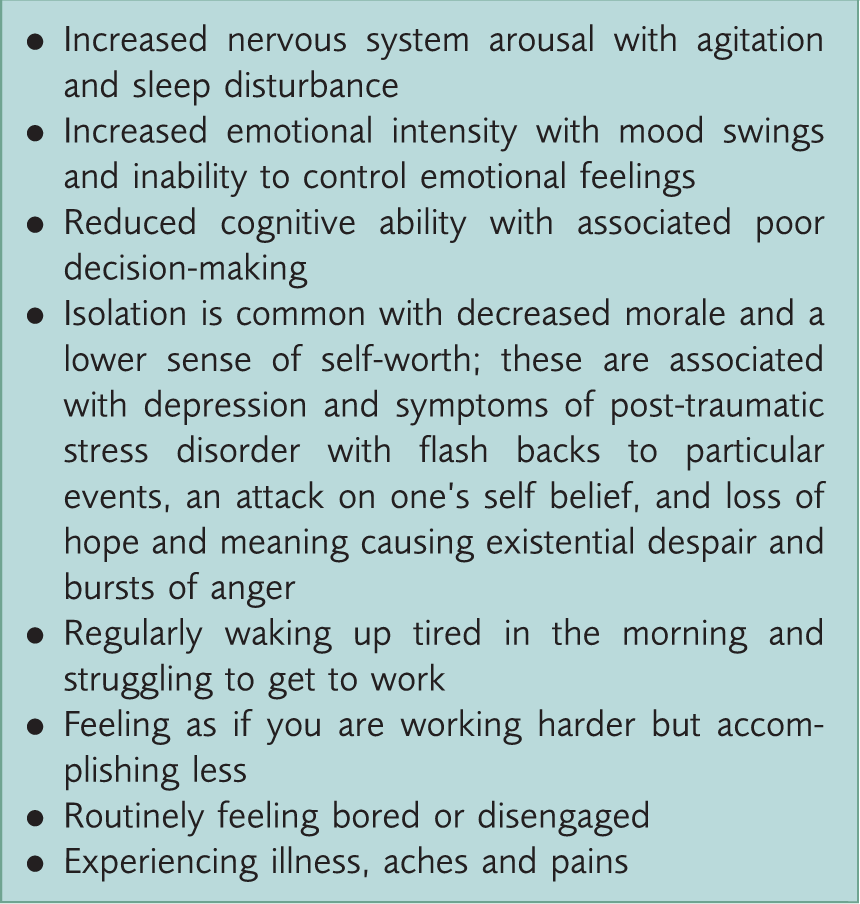
Although compassion fatigue and burnout can co-exist, they are distinct entities and should not be confused. Compassion fatigue can develop in response to one particularly challenging situation (‘the straw that broke the camel’s back’) but is more likely to develop gradually as a result of the accumulation of events.
Burnout
Burnout is much more common than compassion fatigue. It is a term that describes low job satisfaction, feeling powerless, exhausted, depleted and frustrated by the work environment (Maslach, Schaufeli, & Leiter, 2001). Many people in ‘non-helping’ jobs may experience burnout, despite not working in a particularly traumatic environment. However, increased central demands and bureaucracy, constant threat of litigation, an ever-rising workload and patient expectations all make the working environment of the NHS a very difficult one. These factors, combined with the inherent stress of dealing with sick patients and their families day in and day out, may increase the risk of burnout.
Psychological resilience
Psychological resilience can be defined as an individual's ability to adapt to stress and adversity. Resilience is not a rare ability; it is found in the average individual, as many of our patients demonstrate. It can be learned and developed by virtually anyone. Resiliency is demonstrated within individuals who can effectively navigate their way around crises and utilise effective methods of coping.
Managing compassion fatigue
One response to managing compassion fatigue is to use the ‘A, B, C’ mnemonic, as described by Saakvitne and Pearlman (1996):
A represents B represents C represents
Awareness
The key to managing compassion fatigue is self-awareness. This requires that we have a realistic appreciation of our general capacity to work for prolonged periods beyond our emotional comfort zones. It also requires that we are aware of those patient situations that are most likely to increase our vulnerability to compassion fatigue.
Awareness also involves ongoing self-monitoring throughout our working day, taking stock of the numerous situations where transference and countertransference are taking place and looking out for particularly strong or unusual reactions from within, especially when we perceive:
A change in our ability to function as a result of a particular incident A situation or incident does not seem ‘typical or ordinary’ or is rather more ‘traumatic’
Awareness by itself is only of marginal help in managing compassion fatigue. By the time such fatigue is well established, there is a sense of defeat and being trapped, which pervades doing anything with this information other than becoming yet more aware that you are ‘sinking’. Thus, before events occur it is important to put in place preventative measures that can reduce the risks of developing compassion fatigue and specific plans of what to do in the event of recognising the tell-tale symptoms (Wright, 2004).
Mother Teresa made it mandatory for her nuns working in Calcutta to take a year off every 4 to 5 years to ‘heal’ after the compassion demands of working in the Calcutta slums. This was for all nuns, including Mother Teresa herself.
An appropriate appreciation of our need for healing and restoration after prolonged periods of care-giving is essential for those working in the caring professions because:
Without adequate self-care we will become unbalanced and this will become a burden to patients, colleagues, families and ultimately to ourselves Without good self-care strategies we will be at risk of taking inappropriate help from our patients or from colleagues A lack of self-care strategic thinking leaves us prone to seeking other forms of support such as from drugs, alcohol or addictive behaviour, that can ultimately threaten the things that we most value
Balance
Maintaining balance in lives that are so intense with patient, professional and family demands is never easy, and although other doctors may appear to be well balanced, it is likely that even the most balanced paragon is struggling. Then, in addition to this general high level of stress, there are the particular pressures and emotional burdens of looking after families with a patient who is approaching the end of life. It is not surprising that balance can be hard to maintain.
That said, we can be sure that change and stress are going to be part and parcel of GP life and so we need to plan for that certainty in the same way as we plan our financial budgets each year. How you maintain that budget will be different for each GP, but consider the areas in life where stress is most likely to occur. Appreciate that the incident that makes you see red with a patient may well owe its origins to an accumulation of issues from other parts of your life that have been building in the background, such as:
Work Partner/family Friends/social life Financial affairs Health and wellness/body image Spiritual aspects Community/service
Balance strategies.

One anecdotal example of putting such strategies into practice is that of a hard-working hospice consultant. Every Friday afternoon at 4 pm she went to get her hair done; that was her ritual of self-care. We need to care for patients, but we also need to care for ourselves.
Connections
There is a myth that as doctors, we are those who sort out other people’s problems and so have limited need to be helped ourselves. This can lead to real isolation for GPs who can believe that if they admit to feeling any thoughts of difficulty in coping, their colleagues may look down on them or even institute some medico-legal process that could threaten their career. It is because of this that the British Medical Association has set up a helpline for doctors in difficulty, to provide an anonymous outlet for doctors to at least connect with another human being.
Connection is a very important part of being human. How and with whom we make that connection will differ greatly and there is no normative process that meets the need we have as human beings to be listened to and affirmed by others. However, is it not sensible to anticipate that if we are working with dying patients and their families, on top of working in a busy general practice, we will be affected emotionally by our work? If that is the case then do we not need to build into our monthly work plans some regular opportunities to deal with this emotional response?
Connection strategies are innumerable; the key is for each GP to develop individual strategies that work for them. Examples include speaking to a counselor a few times each year; going for a walk in the hills; playing sport; going on long weekends away; spending time with friends and family; walking your dog, etc. Whatever we do to maintain connection with others and with life, the hope is that it will give us the opportunity to process our difficult experiences in a positive manner.
Case study 1.
Dr Charles Morgan is a 40-year-old partner in the Holland House Surgery, working in a practice population of 7000 for the last 8 years. He is highly regarded by his colleagues, the practice staff and by the community nursing team, who value his thoughtful responses and willingness to go out of his way for the sake of patients. Privately they contrast him very favourably with the senior partner, whom they regard as brusque, egotistical, and lacking in empathy or consideration.
Increasingly Dr Morgan has been devoting more of his time to the palliative care work of the practice, in part because of his own natural disposition, but also because the nursing team and patients value the extra effort, time, and willingness to listen that are a feature of Dr Morgan’s practice. Currently Dr Morgan is looking after four families with patients who are approaching the end of life. Each of these families has his personal phone number to call in case of emergency.
Although Dr Morgan greatly enjoys the satisfaction that comes from looking after palliative care patients he is becoming increasingly fatigued and has begun to question some of his clinical decision-making. Things came to a head at the weekend when Dr Morgan found himself swearing at his very supportive and long-suffering wife for suggesting that he needed to take a holiday.
How do you think Dr Morgan could help himself in this situation?
How could others help him? What should they do?
Key points
The active practice of self-care is essential to ensure that GPs under ever-increasing pressure endeavour to protect themselves from compassion fatigue and burnout and develop resilience. This is particularly the case for those working with patients requiring end of life care and their families Compassion fatigue results in an inability to react sympathetically to a crisis or suffering, because of overexposure to previous crises, or suffering It is important to develop strategies to recognise and manage compassion fatigue