
Abstract
There are 31 500 children in the UK with diabetes, the second-most-common chronic disease in childhood, after asthma. Most have type 1 diabetes, those remaining have type 2 diabetes, maturity onset diabetes of the young, or cystic-fibrosis-related diabetes. About 25% of newly diagnosed children present with diabetic ketoacidosis. The NHS spends about £1 000 000 per hour on diabetes and GPs have a central role in early diagnosis, prevention of complications, prompt referral and coordination of care. Engagement with good advice and support is essential for young people with diabetes and their families. This article gives an overview of the management of childhood diabetes.
The GP curriculum and diabetes in children
Develop a flexible approach to health promotion which reflects that certain groups with obesity and diabetes mellitus require different approaches, e.g. children, adolescents and young adults Intervene urgently when patients present with a metabolic emergency, e.g. hypoglycaemia and hyperglycaemic conditions Demonstrate a logical, incremental approach to investigation and diagnosis of metabolic problems
Have an awareness of disease prevention, well-being and safety in children and adolescents, including in the following areas:
^ Healthy diet and exercise for children and young people Adopt a family-centred approach in dealing with patients, their families and their problems. This requires:
^ Effective communication and engagement (listening to and involving children and young people, and working with parents, carers and families) ^ Enable carers and young people to receive information on medicines in a clear way that is appropriate to their understanding as children, young people and parents ^ Demonstrate an understanding of the importance of multiagency working (working across professional and agency boundaries) and the principles of information-sharing.
Introduction
Diabetes is a chronic condition that has a significant impact on a young person and their family. The management of diabetes in childhood should include appropriate drug therapies, education of the patient and those involved in their care, along with access to support and psychological services.
Broadly speaking, the management of type 1 and type 2 diabetes is similar, and will take up most of this article. Genetic conditions such as maturity onset diabetes of the young (MODY) and cystic-fibrosis-related diabetes (CFRD) need more specialised care, but will be touched upon briefly.
All healthcare professionals should endeavour to act in the best interests of patients, with patient safety being paramount. When a young person is unable to consent to treatment, their family or carer should be given information and support to make an informed choice. Conversely, where the young person has the capacity to manage their treatment independently, they should be appropriately supported (National Institute for Health and Care Excellence (NICE), 2016).
Type 1 diabetes
Type 1 diabetes is the result of an auto-immune process, where the insulin-producing β cells of the pancreas are destroyed. Eighty-five percent of children with type 1 diabetes will have no family history of diabetes; however, individuals with a first-degree relative with type 1 diabetes have a 15-fold risk of developing it compared with the background population (Diabetes UK, 2016).
Presentation
A young person who presents with new onset type 1 diabetes may have:
Hyperglycaemia (random plasma glucose level that is greater than 11 mmol/L) Polyuria Polydipsia Weight loss Fatigue
A young person presenting with any of these symptoms on a background of vomiting, abdominal pain, dehydration or altered consciousness, may have diabetic ketoacidosis (NICE, 2016) and needs prompt referral for emergency assessment and treatment. Testing the urine for the presence of ketones and glucose is a simple, but, objective assessment in such circumstances.
In children not acutely unwell, with vague symptoms and with no discernible cause, routine urinalysis is recommended. If urinalysis is positive for glucose, a random blood glucose test is recommended. Similarly, if a well child has a urine dip that is positive for glucose (for example, if testing urine for a suspected urinary tract infection) then check the result using a random blood glucose test and contact the on-call paediatric team for advice.
WHO diagnostic criteria for diabetes.
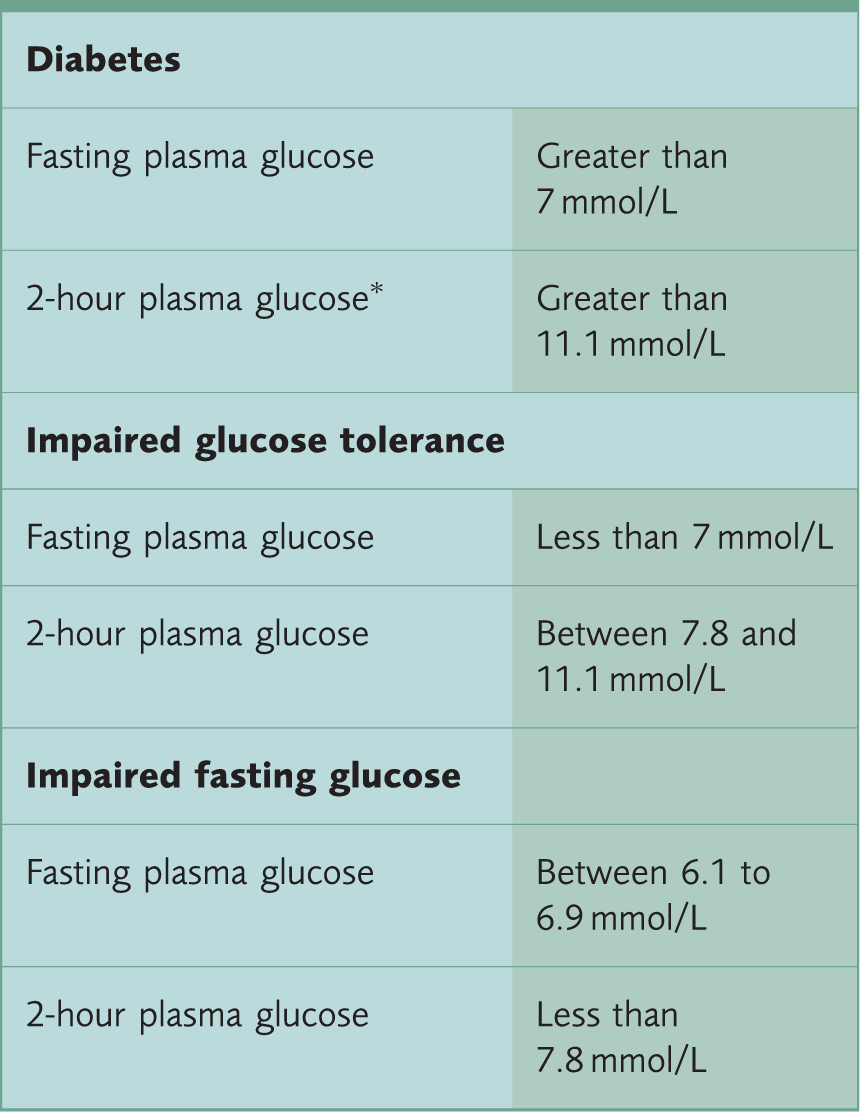
Venous plasmas glucose 2 hours post-ingestion of 75 g oral glucose load
Adapted from WHO (2006).
Types of insulin
Patients with type 1 diabetes are treated with insulin delivered subcutaneously through either a pen device or an insulin pump. The insulin regimes and mode of delivery are individualised to each patient. In children, a basal-bolus regimen, with twice daily doses of long-acting insulin and doses of short-acting insulin with meals is usual. Children with an insulin pump will be given a continuous or regular amount of short-acting insulin, administered subcutaneously via a needle or cannula. Additional boluses are given via the pump with meals, or by a pen device (NICE, 2016).
The type of insulin regimen and device should be tailored to the child and their family. A child with confident, competent parents should do well with a basal-bolus regime. A child with a chaotic family lifestyle may be more suited to a pump device. The target HbA1C level should be 48 mmol/mol (6.5%) or lower. If the child has a high HbA1C, or has consistently high blood glucose levels, then the child and the family’s needs should be reassessed.
Common forms of insulin.
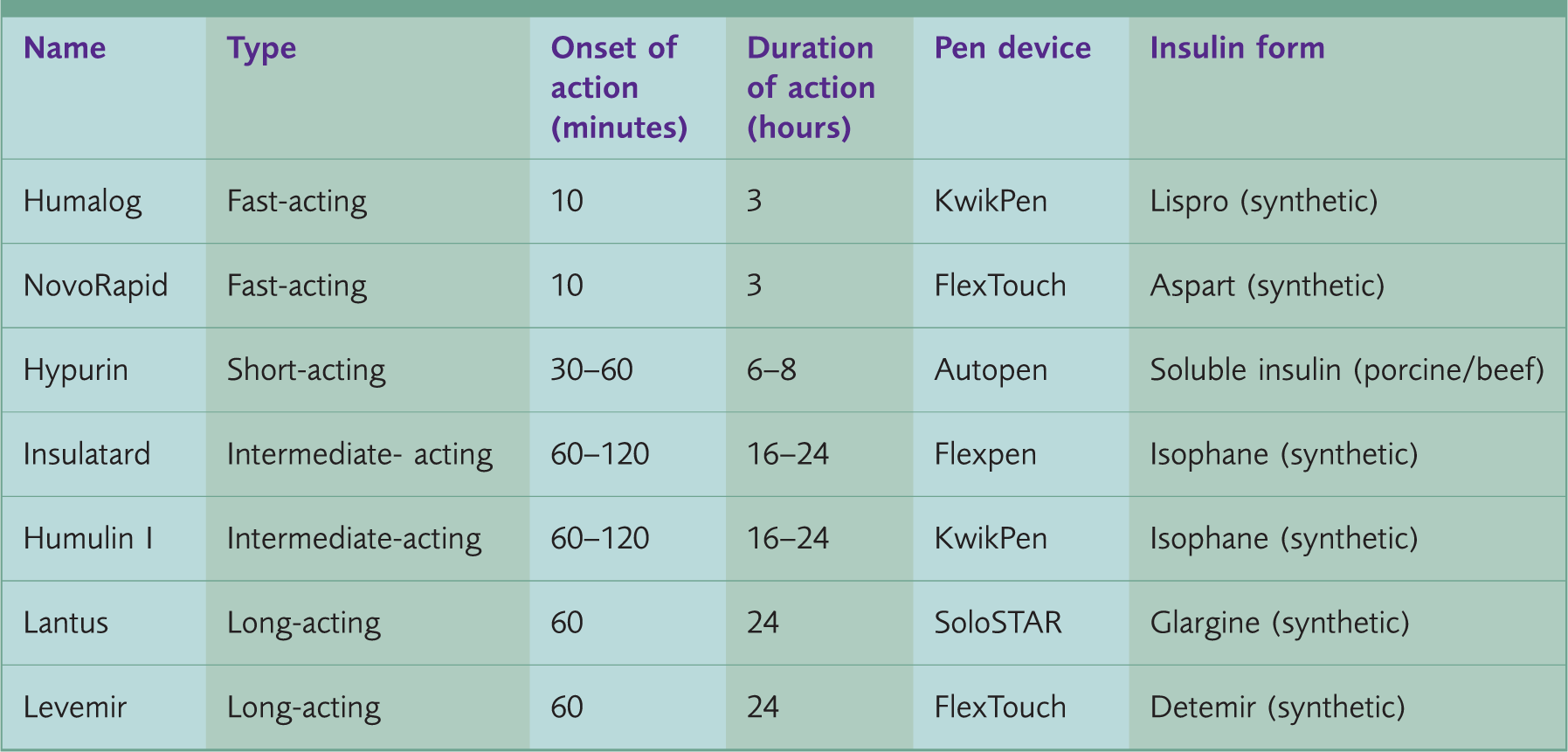
Adapted from Diabetes.co.uk (2017a) and Goad (2017).
Carbohydrate counting
Carbohydrate counting forms part of the management of type 1 diabetes. Education on this is disseminated by the diabetes specialist team to the child and their parents or carers. However, GPs have a role in supporting a healthy lifestyle and awareness of carbohydrate counting.
Carbohydrate counting (or ‘carb counting’, as it is commonly known) is a method for patients with diabetes to calculate how many carbohydrates they are consuming, and thus, their appropriate insulin or medication requirements. ‘Carb counting’ is of use in all forms of diabetes. In type 1 diabetes, it helps patients to match their insulin requirements with food intake; in type 2 diabetes it can help patients regulate their carbohydrate intake as a form of weight management.
Carbohydrates are counted using grams; one serving usually equates to 15 g of carbohydrates, and the effect on blood glucose remains the same, regardless of which type of food is consumed. Patients use food labels, reference books or apps to help them carb count accurately. There are also advanced level 3 carbohydrate counting courses such as DAFNE, X-PERT, and BERTIE that educate patients, families and healthcare professionals on how to count carbohydrates and adjust the dose of insulin safely based on the insulin-to-carbohydrate ratio.
Patients who inject short-acting insulin use an insulin-to-carb ratio to calculate how many units of short-acting insulin they need for the carbohydrates they have consumed. This ratio is calculated based on the individual’s dietary requirements, diabetic control and insulin regime. For example, the ratio may be 1:10, which is 1 unit of short-acting insulin for every 10 g of carbohydrate consumed (Diabetes.co.uk, 2017b).
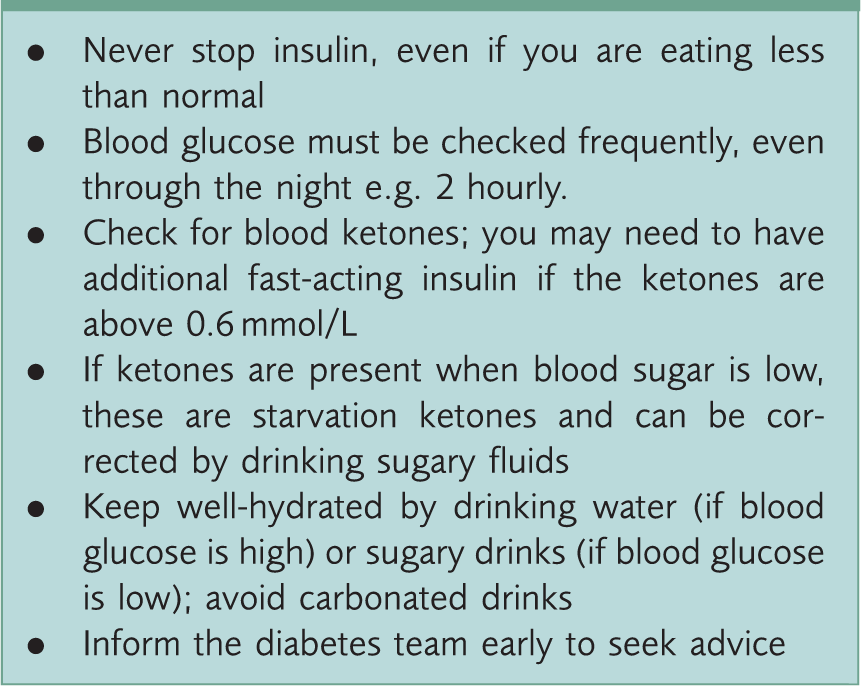
Sick day rules
Sick day rules for insulin pen devices and pumps.
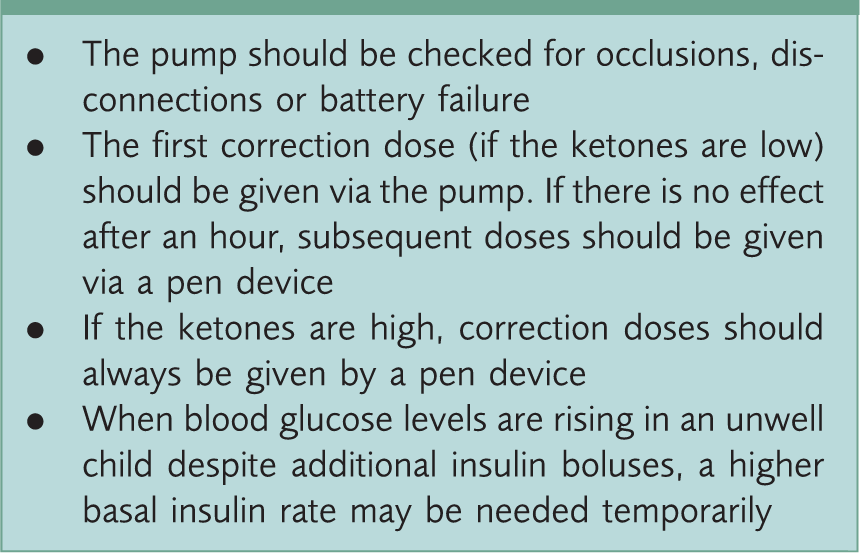
Additional sick day rules for insulin pumps.
Diabetic ketoacidosis
Patients and their carers must also be trained to recognise diabetic ketoacidosis (DKA). A child with type 1 diabetes can develop DKA while displaying normal blood glucose levels. A diabetic child with DKA can present with any of the following symptoms:
Nausea Vomiting Abdominal pain Hyperventilation Dehydration Reduced level of consciousness
It is important to measure blood glucose and blood or urinary ketone levels in diabetic children who are feeling unwell and are attending the GP surgery. If the glucose and/or the ketone levels are elevated, and the child looks dehydrated with fluctuating consciousness, urgent referral to the local A&E or paediatric unit is essential. Even when a child with raised blood glucose or blood/urine ketone levels looks relatively well, same-day assessment by acute paediatric services is indicated; children who are brewing DKA can deteriorate rapidly. DKA is diagnosed if there is:
Acidosis (blood pH less than 7.3 or bicarbonate less than 18 mmol/L) and Ketonaemia (blood ketones above 3 mmol/L) or ketonuria (++ and above on dipstick testing)
It is not appropriate to manage DKA within a primary care setting, however, awareness of DKA and important aspects of the management of DKA is important, not least to communicate the seriousness of this condition to patients and carers. In the hospital, further blood tests will help determine the level of hydration and blood pH. If severely dehydrated and acidotic, intravenous fluid (IV) therapy will be initiated. If vomiting, a nasogastric tube may be passed to prevent aspiration. If there is concomitant sepsis, IV antibiotics will be administered. Complications of DKA include cerebral oedema, hypokalaemia and venous thromboembolism. Management is usually on the high dependency unit, but may be on the general paediatric ward in less serious cases.
Following treatment, the child and their carers should be counselled on how to avoid future episodes of DKA. If they are not coping with the current insulin regimen, this should be adapted to ensure full compliance with treatment. The sick day rules should also be revised with them (NICE, 2016).
Hypoglycaemia
Hypoglycaemia is a low level of blood glucose; usually less than 4 mmol/L with or without any other symptoms. Young children will not report symptoms readily, so parents and healthcare professionals should consider hypoglycaemia if the child is:
Sweating Lethargic Dizzy Irritable Looks pale Finding it difficult to concentrate
To rectify hypoglycaemia, if conscious, give 7–15 g of carbohydrate in the form of a sugary drink (non-diet), usually about 100 ml, three glucose tablets, glucose gel or five sweets. It may take between 15 and 20 minutes to correct the hypoglycaemia. If after 15 minutes the blood glucose level is still less than 4 mmol/L, give another portion of a rapid-acting carbohydrate (Diabetes UK, 2017a).
Parents are advised to keep glucose tablets, full sugar drinks and food in the house and easily to hand when out and about. When older and going to school or visiting friends, provide a stock of glucose tablets and inform a responsible adult on use and whereabouts. In the event of a child becoming unconscious from hypoglycaemia, the parents need to put the child in the recovery position and call an ambulance. If trained to do so, the parents should administer intramuscular glucagon; this is a hormone that stimulates conversion of stored glycogen into glucose (Diabetes UK, 2017a). The administered dose should be 1 mg if the child weighs 25 kg or above, and 0.5 mg if the child weighs less than 25 kg.
Monitoring for complications and associated conditions
Children with type 1 diabetes are at risk of developing diabetic complications. They need to be monitored at regular intervals, as outlined below:
Thyroid function tests: At diagnosis and annually thereafter Total immunoglobulin A (IgA) and IgA tissue transglutaminase for coeliac disease: At diagnosis Diabetic retinopathy: Annually from the age of 12 years Albumin-to-creatinine ratio: Annually from the age of 12 years Hypertension: Annually from the age of 12 years Diabetic foot assessment: Annually from the age of 12 years
There are a few rare associated conditions that clinicians need to be aware of when a diabetic child attends for annual review:
Juvenile cataracts Necrobiosis lipoidica Addison’s disease
The child and their family should be made aware of the importance of screening for these conditions and attending appointments. Early diagnosis and treatment lead to better outcomes and fewer long-term complications (NICE, 2016).
Multidisciplinary team
Healthcare professionals involved in a diabetes MDT.
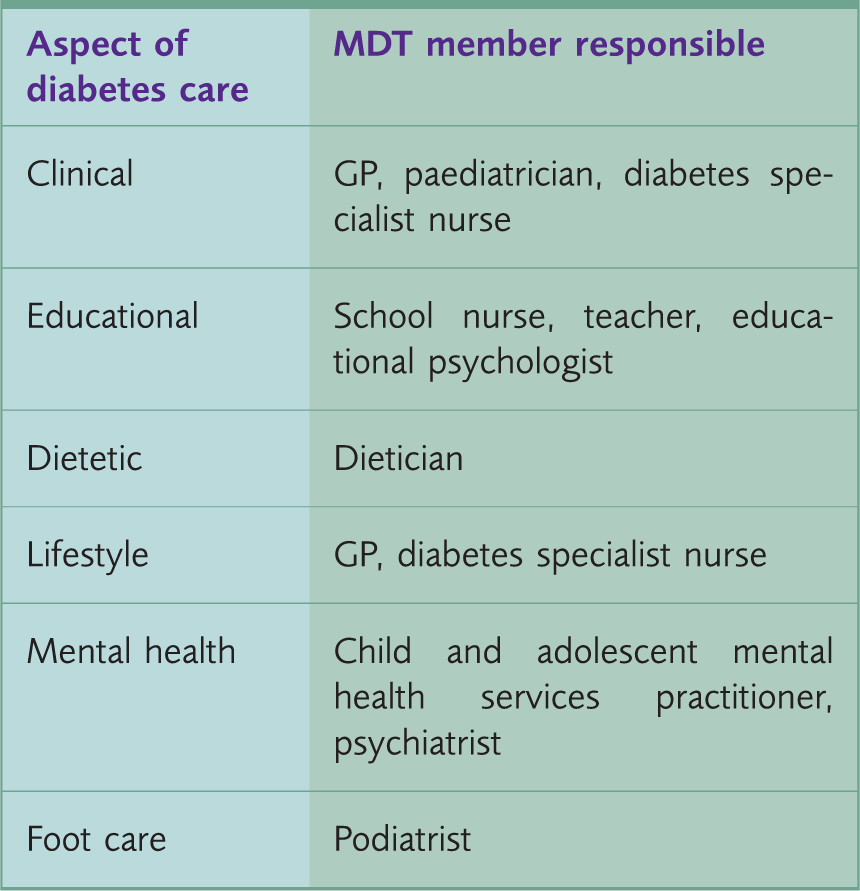
Adapted from NICE (2016) with original content from author.
Diabetic children and their carers need 24-hour access to the local specialist diabetes team. Normally, an individual from the paediatric diabetes team is available during working hours to answer any queries via telephone; out of hours, advice may be sought from the on-call paediatric registrar (NICE, 2016).
Lifestyle advice
Children with type 1 diabetes are encouraged to visit their specialist clinic four times a year; regular contact is associated with optimal glucose control. They should also have regular dental checks and an eye examination once every 2 years. Children over the age of 6 months should also be offered an annual influenza vaccine if they have diabetes. If there are concerns about the child’s nutritional status, referral to a dietician is warranted. Once the child is older, it is advisable for them to wear a medical bracelet or charm that can easily identify them as diabetic should they become unwell in an unfamiliar environment.
Teenagers with type 1 diabetes are often difficult to manage. Difficulties include non-compliance with treatment and smoking or substance misuse. Such patients and their parents need to be counselled on the dangers of non-compliance. Dangers include erratic levels of blood sugar, hypoglycaemic episodes and diabetic ketoacidosis. There are increased vascular risks from smoking, and additional risks associated with substance misuse. Consultations with teenagers (and indeed, a young person of any age) need to take account of individual maturity, personal beliefs, life goals, emotional well-being, social circumstances and cultural norms. Referral to Child and Adolescent Mental Health Services (CAMHS) may be appropriate if there are concerns about the child’s mental health (NICE, 2016).
It has been noted that children with psychological problems, such as depression, tend to have poor glycaemic control. Parents and patients should be actively encouraged to attend regular, scheduled sessions with a healthcare professional with whom they have a good rapport. Early engagement with healthcare professionals has been shown to reduce psychological issues in children with diabetes, which in turn, has a positive effect on their glycaemic control (Northam, Todd, & Cameron, 2006).
Type 2 diabetes
Type 2 diabetes is caused by a complex interaction between genetic and environmental factors. It is characterised by a sustained hyperglycaemic state, due to insulin resistance or inadequate insulin secretion. There is a strong familial trait: individuals with diabetics in the family are two to six times more likely to develop type 2 diabetes than those with no diabetes in the family. Those of South Asian and Black ethnicity are more likely to develop type 2 diabetes than their Caucasian counterparts (Diabetes UK, 2016).
Assessment
Type 2 diabetes should be considered in any child who is overweight, has a family history of diabetes, is of South Asian or Black ethnicity, and who may complain of:
Weight loss Thirst Fatigue Dysuria Itchy skin Blurred vision Slow-healing wounds Numbness or tingling of the hands and feet
If a child is suspected of having type 2 diabetes, test urine for glucose and a random blood glucose level. If the urine dipstick is positive, or the blood glucose level is greater than 11 mmol/L, contact the on-call paediatric registrar for advice. Depending on how unwell the child is, they may advise same-day assessment by the acute paediatric services, or suggest further tests to confirm diagnosis (Zeitler et al., 2014).
Management
A child newly diagnosed with type 2 diabetes should have an HbA1C level test performed every 3 months. The target level for HbA1C should be 48 mmol/mol. Management of the diabetes should be tailored to the child, their general health, and family circumstances (NICE, 2016).
In a child who has poor nutrition or who is overweight, the child and family should be educated on the importance of a good diet and regular exercise. Input from a dietician is beneficial in these circumstances. Body Mass Index centiles can be used in children to diagnose obesity. A weight loss of between 0.5 and 1 kg per month is an acceptable and achievable goal. Children should be discouraged from eating energy-rich foods, such as ‘fast foods’, and sedentary activities, such as watching television. Encourage children to pursue moderate exercise, such as brisk walking, for 60 minutes daily (Scottish Intercollegiate Guidelines Network, 2010).
Metformin should be offered to all children with type 2 diabetes. Metformin may be started in children aged between 10 and 16 years at a dose of 500 mg once a day and titrated up as necessary by 500 mg every week to a maximum daily dose of 2000 mg. Lactic acidosis can occur in patients with renal or hepatic impairment or cardiac/respiratory insufficiency. Renal monitoring using paediatric parameters is recommended. Adverse effects such as diarrhoea, nausea/vomiting abdominal pain and headaches may occur, and patients and their families should be counselled appropriately.
Other drugs used in adults with type 2 diabetes, such as thiazolidinedones, sulphonylureas, and GLP1-agonists, have either not been studied in children or have only been studied in small trials. Therefore, the mainstay of treatment for type 2 diabetes in children is exercise, nutritional advice and metformin (St Onge, Miller, Motycka & DeBerry, 2015).
Lifestyle advice
Children with type 2 diabetes have an increased risk of psychological conditions, and those involving complex social factors may adversely affect glycaemic control. Children with suboptimal glucose control should be screened for anxiety and depression. Monitoring for hypertension, dyslipidaemia and albuminuria should start at diagnosis; screening for diabetic retinopathy should start at 12 years of age, but referral to local eye-screening services is recommended at diagnosis. Diabetic foot problems should be assessed at the annual diabetes check for children over the age of 12 years; for younger children, parents or carers should be given basic foot care advice (NICE, 2016).
As has already been discussed above, a good diet and plenty of exercise contribute to optimal glycaemic control. Families of children with type 2 diabetes should be supported in making healthy lifestyle choices: a child has an increased risk of becoming obese if one or both parents are classed as obese. Signpost the families to local healthy lifestyle initiatives, such as Change4Life, as well as support groups, to empower them to make better choices and receive the help they need (Reilly et al., 2005)
MODY
MODY comprises 1–2% of all diabetes diagnoses. It is a rare form of familial diabetes, caused by genetic mutations that affect β-cell function. It is important to distinguish MODY from type 1 and type 2 diabetes, as the treatment options are different. Eighty percent of patients with MODY are misdiagnosed as having type 1 or type 2 diabetes, as the clinical features of the different forms of diabetes are similar.
Assessment
Patients suffering from MODY have a 50% chance of passing it on to their children. Subsequently, in any patient with a strong family history of diabetes (regardless of the type), a diagnosis of MODY should be considered, especially if there is:
A history of obesity, hypertension and dyslipidaemia (suggestive of a metabolic disorder) A history of pancreatic disease A history of early onset deafness (associated with mitochondrial diabetes) or cystic renal disease (associated with a HNF1B mutations, which are associated with MODY) Signs of insulin resistance, such as acanthosis nigricans, lipodystrophy, central obesity and dyslipidaemia Signs of endocrine disorders, such as Cushing’s disease or acromegaly Presence of autoantibodies to β cells Level of C-Peptide in the blood (C-Peptide levels are proportionally linked to endogenous insulin production)
Genetic testing for MODY is widely available, and the patient should be appropriately counselled prior to diagnostic testing. It is recommended that GPs refer patients suspected of having MODY to local diabetes teams or the clinical genetics department for further advice on MODY (Thanabalasingham & Owen, 2011).
Management
Key features of the types of MODY.
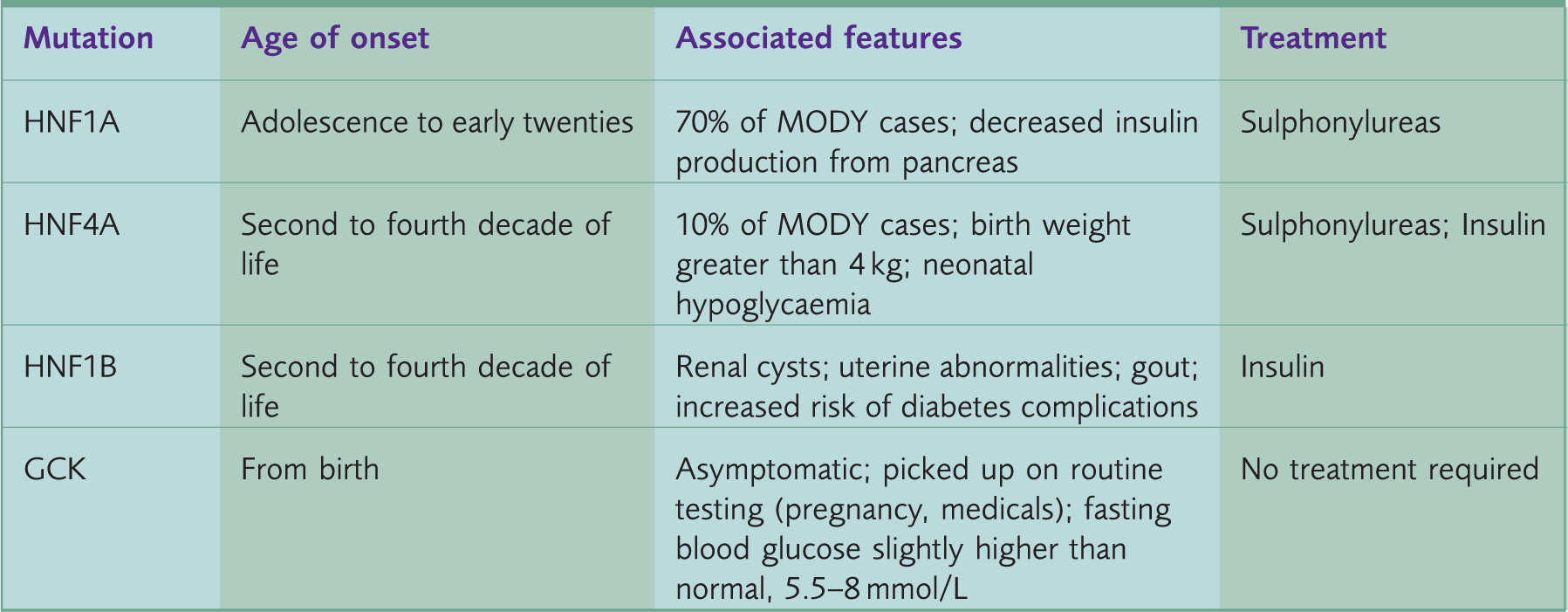
Adapted from Diabetes UK (2017b) and Owen, Thanabalasingham, & Juszczak (2014).
Cystic-fibrosis-related diabetes
CFRD is a form of diabetes affecting children with cystic fibrosis (CF); the longer they live, the more likely they are to develop CFRD. The onset is gradual and the glycaemic status of the patient varies with their general clinical condition. A delay in diagnosis can directly affect pulmonary status; thus, children with CF must be screened annually with oral glucose tolerance tests (OGTT) after the age of 12 years.
Progressive fibrosis and fatty infiltration of the pancreas lead to disruption of islet cell function, directly affecting the production of insulin, glucagon, and pancreatic polypeptide. Patients with CFRD have a worse prognosis than non-diabetic CF patients; there is a difference of 10 years in median survival age between the two groups.
Testing for CFRD is difficult in the initial stages of the disease. Traditional tests for diabetes, such as HbA1C, random and fasting blood glucose levels, have reduced sensitivity and specificity in CFRD. OGTT and serial glucose monitoring are far more accurate tests for CFRD.
Management of CFRD depends on the life expectancy of the individual. If the patient with CF has a poor prognosis, symptomatic treatment alone is acceptable. For patients who have longer life expectancies or who wish to get pregnant, treatment is indicated to avoid the long-term complications of diabetes. Depending on the individual’s CFRD classification (reactive hypoglycaemia, impaired glucose tolerance, CFRD with or without hyperglycaemia), treatment is usually dietary, as prescribed by a specialist dietician, or with insulin (Cystic Fibrosis Trust, 2016).
Key points
Always consider diabetes in an unwell child with vague symptoms Urinalysis for glucose and random blood glucose are simple, objective tests to inform diagnosis Early diagnosis and treatment lead to better outcomes and fewer long-term complications GPs and other healthcare professionals can promote good glycaemic control by providing holistic support to the child and their family MODY is a rare form of diabetes that should be considered in patients with a strong familial history of diabetes and features suggestive of metabolic disorders CFRD is linked to poor prognosis in patients with CF and assiduous screening for CFRD is required