
Abstract

In November 2019, the House of Commons Scottish Affairs Select Committee published its report into problem drug use in Scotland. This came in response to statistics published earlier in the year by National Records of Scotland (NRS), which revealed a sharp rise in drug-related deaths in this part of the UK. Deaths attributable to the use of drugs had risen by 27% in Scotland in 2018, reaching a total of 1187, or 0.16 per 1000 population (Fig. 1). This was the largest number ever recorded by the NRS, more than double the figure from a decade ago (NRS, 2019).
Trend in drug-related deaths 1996-2018.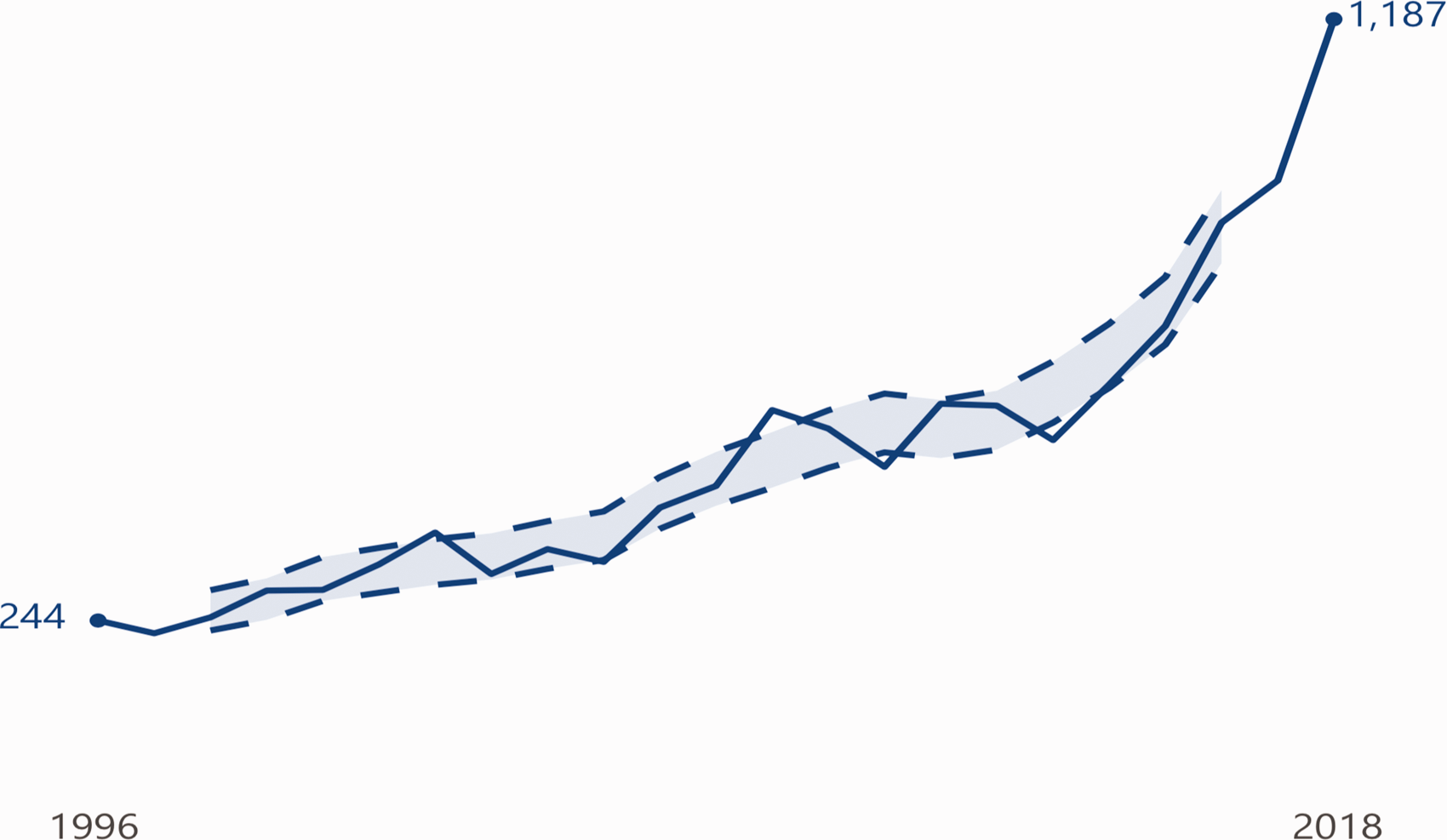
Although there was an increase UK-wide, the rate of drug-related deaths in Scotland was approximately three times higher than in England and Wales. Scotland’s figure is, in fact, the highest in the European Union, 50 times that of Portugal, and on a par with the United States (NRS, 2019). Faced with these statistics, the Select Committee report concluded that ‘Scotland is in the midst of a drug death crisis’, urging the UK Government to declare a public health emergency and to ‘take urgent and radical steps’ to address the problem (House of Commons, 2019: 8).
A wider understanding of the reasons for Scotland’s position as an outlier is crucial to formulating a response. According to the report, although the underlying drivers of problem drug use are not specific to Scotland, for various reasons they have been expressed more acutely here, both in terms of the size and vulnerability of the drug-using population. Although the scale of the problem in Scotland is therefore symptomatic of deeper social issues, the timing of the crisis may reflect recent trends in drug taking, such as the concurrent use and toxicity of street drugs. On top of this, it is worth examining the extent to which UK drug policy and the treatment of drug dependence over the past decade may have contributed to the problem.
In terms of underlying drivers of drug misuse, the report highlighted, in particular, the role of poverty and inequality. Deprivation correlates with a number of more specific social risk factors: exposure to drug use in childhood, adverse childhood events (ACEs), unstable home life, homelessness, unemployment and social marginalisation. Figures from Turning Point Scotland, for example, show that children experiencing four or more ACEs are 11 times more likely to go on to use crack cocaine or heroin (House of Commons, 2019: 10). The prevalence of adult mental illness, psychological trauma and exposure to drugs in prison are further drivers of the problem. Inequality also affects the likelihood of overcoming drug addiction. Unsurprisingly, those with limited personal resources and social support do worst (House of Commons, 2019: 9).
Although Scotland is home to some of the poorest areas in the UK (Lloyd et al., 2017), and sees higher levels of children being brought up in care (House of Commons, 2019: 13), overall, the level of poverty is broadly similar to that in England (Joseph Rowntree Foundation, 2018). Clearly there is more to the story in Scotland. A closer look at the data reveals just that: both historical and demographic factors contribute to the particular vulnerability of Scotland’s drug-using population.
For one thing, the NRS statistics show that the average age of drug-related deaths in Scotland is rising sharply. Most of the increase in deaths in 2018 was accounted for by the 35–44 and 45–56 age groups, occurring at approximately twice the rate of deaths in the 25–34 age group (NRS, 2019). In other words, these deaths were occurring in an ageing cohort – the so called Trainspotting generation – who started using drugs during the heroin epidemic of the 1980s. Now in their fourth decade of drug use, with an accumulation of complex health problems and high levels of social isolation, this is a prematurely frail and vulnerable population – and a disproportionately large one in Scotland.
The fact that Scotland has maintained significantly higher rates of drug use than the rest of the UK since the 1980s invites further analysis. Epidemiologists have pointed to the economic policies of the 1970s and 1980s – namely deindustrialisation – which appear to have had a greater social impact in Scotland. Twin losses of employment and cultural identity created a legacy of displacement and deprivation, which has been referred to as ‘The Glasgow Effect’ (House of Commons, 2019: 13).
Although these historical and demographic factors provide some context to the rise in drug-related deaths in Scotland, the timing of the recent spike is the result of more acute trends, on which the NRS data again sheds some light. Of the 1187 deaths in 2018, only 68 were in cases where only one drug was implicated. Opiates had a role in 86% of deaths, benzodiazepines in 67%, methadone in 47% and cocaine in 23% (NRS, 2019). This pattern of poly-drug use coincides with a recent increase in the strength, toxicity and variability of street drugs, creating what has been described as a ‘perfect storm’ of risk factors (Brooks, 2019). Although these trends are not specific to Scotland, they go a long way to explaining the picture when looked at alongside the size and age of the Scottish drug-using population.
What is not captured by the NRS report, however, is the extent to which changes in the delivery of opiate dependence treatment in the UK over the past decade have contributed to the current crisis. As Kalk et al. (2018) explain, treatment of opiate dependence in the UK since the 1980s has been characterised by both ‘triumph and failure’. As the centre of the human immunodeficiency virus (HIV) epidemic in the 1980s, Scotland was at the forefront of the shift in UK drug policy from a ‘punish and deter’ model towards harm reduction, through the introduction and expansion of interventions such as needle exchange services, methadone maintenance treatment, and take-home naloxone. Although this shift was a clear response to a public health crisis, it was at the same time firmly rooted in evidence, and led to dramatic results.
Cases of HIV caused by needle and syringe sharing fell from 55% in the early-1980s, to 20% in the early- 1990s, and the UK avoided the rapid rise in HIV and drug-related deaths seen in other European countries (Kalk et al., 2018). Methadone maintenance treatment led to better engagement and retention of patients, as well as significant and cost-effective reductions in harm to drug users compared with detoxification-orientated treatments (Kalk et al., 2018). Wider benefits were also observed: during treatment, the number of crimes committed fell by two thirds and criminal involvement of drug users halved (Kalk et al., 2018).
Over subsequent decades, despite this success, there remained unease at a societal and political level over a drug policy that was seen as overly soft on drug use, and insufficiently orientated towards recovery, as defined by abstinence. By 2008, with the HIV epidemic decades past, and the political climate shifting to the centre-right, there was a new commitment to drug-free services throughout the UK, marked in Scotland by the publication of the ‘Road to Recovery’ strategy (Scottish Government, 2008). This heralded changes in both funding and attitudes that came at the expense of harm-reduction interventions, which despite their evidence base are seen as antithetical to the notion of recovery. Opiate substitution services have instead become increasingly geared towards stricter, lower-dose, reducing regimes over the past decade, damaging both accessibility and user engagement (Kalk at al., 2018). It is telling that these changes have coincided with a rise in poly-drug use: the failure of treatment driving drug users towards riskier behaviour.
With this in mind, the recent spike in drug-related deaths in Scotland must be seen not only as a consequence of the size, habits and make-up of Scotland’s drug using population, but also as a result of flaws in UK drug policy in general, and in the delivery of opiate dependence treatment over the past decade in particular. With this conclusion becoming clearer, so the case for political change becomes stronger. Currently, the responsibility for UK drug policy resides with the Home Office, in Westminster. Moving it to the Department of Health and Social Care (which is devolved to the Scottish Government) would not only allow a more Scotland-focused approach, but would help to reframe the problem itself as a matter of public health rather than criminal justice.
The Select Committee’s recognition of the role of criminal justice interventions in driving problem drug use led it to advocate for precisely this change, as well as for the decriminalisation of small-volume drug possession (House of Commons, 2019: 55). In Portugal, a similar policy, coupled with an expansion of harm-reduction services, has led to a significant reduction in drug-related deaths (House of Commons, 2019: 40). Currently, however, the Home Office remains a barrier to local, evidence-based harm-reduction interventions, an example being the blocking of proposals from Glasgow’s Health and Social Care Partnership last year for safer injecting facilities.
Certainly, as long as the socio-historical forces at play continue to put Scotland at higher risk of drug-related deaths, a more robust and radical response is needed. Current policy perpetuates a disproportionate level of harm in Scottish society. Meanwhile, lessons from home and abroad point to the benefits of a public-health approach; the importance of prioritising harm-reduction; and the continuing need to be guided by evidence over attitudes.
GPs witness the effects of problem drug use daily, and are well placed to contribute to this debate, and to advocate for these principles. However, on a practical level, the delivery of drug dependence treatment is fraught with challenges for many GPs. For example, opioid substitute prescribing is complicated by the risk of overdoses and black market redistribution, making it a source of medicolegal anxiety. A lack of specific training or field experience is common, and fears about confrontational patients add to the hesitancy around an area of prescribing that can be seen as divisive or controversial. Tellingly, the majority of prescribed doses of methadone fall below the bottom of the recommended therapeutic range (Kalk et al., 2018).
Maintaining engagement and confidence in this field among GPs is vital. To this end, the UK Guidelines on the Clinical Management of Drug Misuse and Dependence are a key resource. Distinctive in its pragmatic and accessible tone, The Orange Book (as it is often called) combines formal summaries of evidence with practical information, for example, on the cleaning of injecting equipment (Department of Health and Social Care, 2017).
Beyond this, the RCGP provides training by way of the two-part Certificate in Management of Drug Misuse. Part 1 consists of two e-learning modules and a face-to-face session, and is designed for GPs or trainees seeking to provide or improve their understanding of drug dependence treatment. Part 2 looks at more advanced aspects of management and service provision, and is aimed at those wishing to become GPs with a special interest.
These resources support GPs in providing the sort of care that is needed by people who use drugs: care that is both long term and sporadic, coordinated and opportunistic, and holistic and individualized. GPs are ideally placed for this role, located in communities and integrated with the wider primary care team of pharmacists, nurses, health visitors and social workers. Moreover, as Robertson (2020) argues, such care is not only rewarding for doctors and patients, but is also an opportunity for general practice to show its strengths.