
Abstract
Primary care sees a large proportion of older adults experiencing or at risk of falls, providing an important opportunity for falls prevention. Falls can result in significant burden of fractures, hospitalisation and mortality and they have high associated healthcare costs. A third of falls could be prevented through use of evidence-based interventions. This article will present up-to-date evidence in falls prevention from the latest global guidance and experts in the field. It will provide an overview of how to assess the likelihood of an individual experiencing falls in the future, provide guidance on signposting and referral to appropriate services. In current primary care practice, with significant time pressure and conflicting priorities, this article aims to focus our attention and provide a practical approach to prevention of falls in the community.
Clinical case scenario 1
Mrs Khan, aged 80 years, is seen for her annual health review. She has hypertension and has had a kidney transplant. During the COVID-19 pandemic she stayed at home due to isolation rules and fear of catching COVID-19. She previously walked to the local shop to get a newspaper every day. Her mobility has declined in the last year. A month ago, she fell over in the house when she lost her balance. During an annual hypertension chronic disease review her blood pressure is checked and there is discussion about her blood tests. She does not feel it necessary to tell you about her recent fall as she wasn’t hurt. Two months after her review she subsequently has another fall, and she is hospitalised with a neck of femur fracture.
Suggested approach to falls prevention
Background and diagnosis
A fall is defined as ‘an event which results in a person coming to rest inadvertently on the ground or floor or other lower level’ (World Health Organization (WHO), 2021). Older adults at risk of, or experiencing, falls can present to GPs in different ways. Between 30 and 50% of falls result in minor injury, and around 10% of falls result in serious injuries, including hip fractures, other fractures, traumatic brain injury, or subdural haematoma (Nevitt et al., 1991). Individuals may seek review immediately after or some time following a fall. Alternatively, individuals may fall without seeking help and subsequently not inform their GP.
The components to acute management and assessment of an individual presenting with a fall are covered in a previous article (Sritharan, 2016). In summary acute assessment should include a falls history, clinical examination, investigations, and medication review.
This article focuses on an approach to falls prevention, which could be performed opportunistically or after acute assessment of a recent fall. A third of falls could be prevented through use of evidence-based interventions (Morris and O’Riordan, 2017).
Barriers to falls prevention in primary care are significant, with time constraints, multiple conflicting priorities, and variability in clinical training. This article aims to educate on evidence-based interventions and highlight opportunity for intervention and effective risk stratification (Mackenzie and Mcintyre, 2016).
Opportunity for falls prevention
Patients infrequently volunteer that they have had a fall. The National Institute for Health and Care Excellence (NICE) recommends that adults over 65 years in age should be asked routinely if they have fallen in the past year, the frequency, how they fell and the features of these incidents (NICE, 2013).
Primary care contact with patients can take many forms. Discussion about falls could take place opportunistically during annual health checks for Quality and Outcomes Framework (QOF) conditions, during consultation about other concerns or during contact with a healthcare practitioner for investigations. Review could also occur when reading documentation received or health records.
A single question ‘
However, individuals who have not experienced a recent fall, but who have other risk factors for falls can still be missed by only asking this question. For example, those with worsening balance. If time permits there are other tools that have been developed that could be used in primary care, such as the 3 Key Questions (3KQ) (Tinetti et al., 1998). The 3KQs include:
Have you fallen in the past year? Do you feel unsteady when standing or walking? Do you have worries about falling?
Clinical case scenario 2
Mr Taylor is seen for a same-day appointment aged 80 years. He has hypertension and has had a kidney transplant. He has experienced a fall today. He did not sustain any injuries. He tells you he slipped on a rug and had no preceding symptoms. He tells you he could not reach the phone until his daughter found him on return from work, which was luckily soon after. He tells you that she is busy, and he only sees her infrequently. You perform a focused falls assessment and cannot find any other concerning features. You are able to explore options with him, including referral to the social prescriber to discuss social activities to help with his loneliness and to the local first response service. You see him for a follow up review. He tells you about the local gardening group he has joined and shows you his new pendant alarm.
Assessment of falls risk
There may be individuals who may benefit from additional support around falls risk who may not traditionally meet criteria for a falls assessment in secondary care. For example, those who have risk factors for falls such as reduced mobility, balance and fear of falling.
The 2023 World guidelines for falls prevention and management for older adults can be used to guide clinicians in risk assessment (Montero-Odasso et al., 2022). The guideline produced by a group of worldwide experts and older adults, formed a formal group consensus using current research and expert knowledge. The algorithm for risk stratification can be applied in a primary care setting (shown in Fig. 1), categorising individuals who present due to falls and opportunistic assessment into low, intermediate and high risk of falls (Montero-Odasso et al., 2022). As one in three adults over 65 years fall, a low risk does not equate to no risk (Lewis and Griffin, 2023).
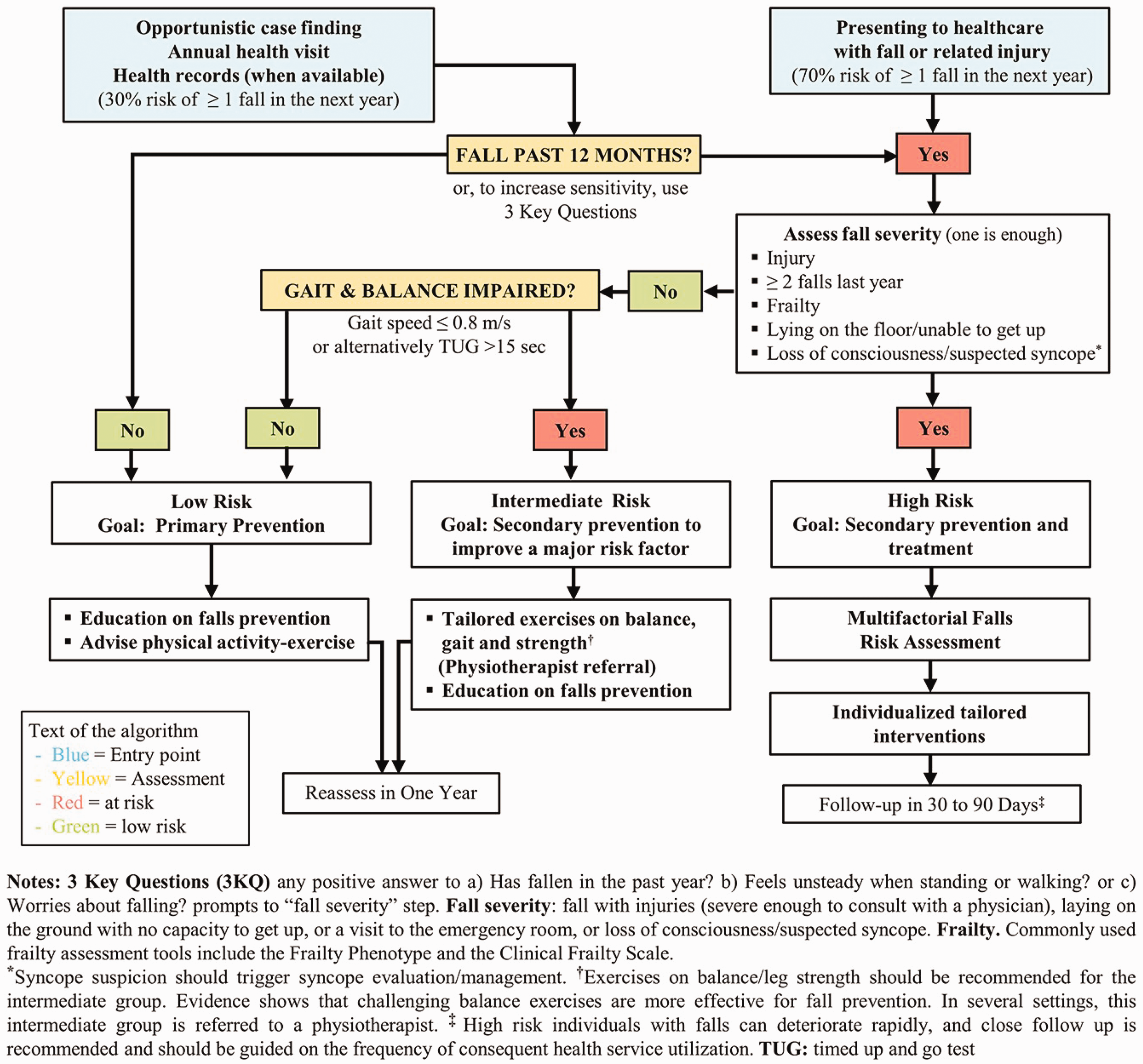
Algorithm for risk stratification in the World Guidelines for falls prevention.
Observing the speed patients walk into the consulting room and gait speed can be a useful objective measure of the risk of patients falling again. Walking four metres at less than 8 m/s indicates a higher risk of falling. This is used in the next step of the algorithm to risk stratify individuals who have fallen (Montero-Odasso et al., 2022). Observing patients’ walking from the waiting room into the consultation room allows for assessment of their gait speed.
What interventions for falls prevention are effective?
Educational and information giving
NICE advises that oral or written information be provided to individuals at risk of falling. This can include preventative measures to take, risk modification including physical and psychological changes, signposting to further information and how to manage a fall (NICE, 2013). Age UK have produced ‘
Clinician’s hold a privileged position and a key role in encouraging engagement and motivation in exercise, with evidence that this can reduce falls risk (Paganini-Hill et al., 2017).
The NHS Physical Activity Guidelines for Older Adults advise that all older adults (NHS, 2024):
Undertake daily activity of any form Strength and balance exercises twice a week 150 minutes of moderate-intensity exercise or 75 minutes of vigorous exercise Reducing long periods of immobility
Their thoughts and future goals around exercise could be discussed during healthcare encounters.
Strength and balance
There is a strong evidence base for strength and balance exercises reducing falls risk. These should particularly include balance challenging and functional exercises such as sitting to standing and stepping. These activities should take place at least three times a week, they should be tailored to the individual and progressively more challenging over at least 12 weeks (Sherrington et al., 2020). Activities including Tai Chi have been recommended.
Exercise programmes for falls prevention in the UK are commonly based on two evidence-based programmes called OTAGO (Campbell et al., 1997) and Falls Management Exercise (FaME) (Skelton et al., 2005), although provision of services varies greatly across the UK. Otago includes lower limb strength and balance whereas FaME builds on this to include upper limb and reactive stepping (Later Life Training, 2024).
Focus should be made to engage individuals with early Parkinson’s disease, early cognitive decline including those with dementia, those who are hospitalised and in long term care, who are at higher risk of falls. During GP appointments, referral to the local tailored exercise programmes or gym may need discussion. Stay Steady provides advice around staying active in a care home (Age UK, 2024).
Multifactorial risk assessment
NICE recommends individuals with multiple falls, those who seek medical attention because of a fall or individuals with abnormality of gait or balance should be offered a multifactorial falls assessment. They advise this should be performed by a suitably trained individual, and normally in a falls clinic. The 2023 World guidelines for falls prevention and management for older adults identify other individuals who would also benefit from being assessed.
The multifactorial risk assessment should include assessment of falls history, gait, balance and mobility, muscle weakness, osteoporosis risk, older person's perceived functional ability and fear relating to falling, visual impairment, cognitive impairment and neurological examination, urinary incontinence, home hazards, cardiovascular examination and medication review (shown in Fig. 2) (NICE, 2013).
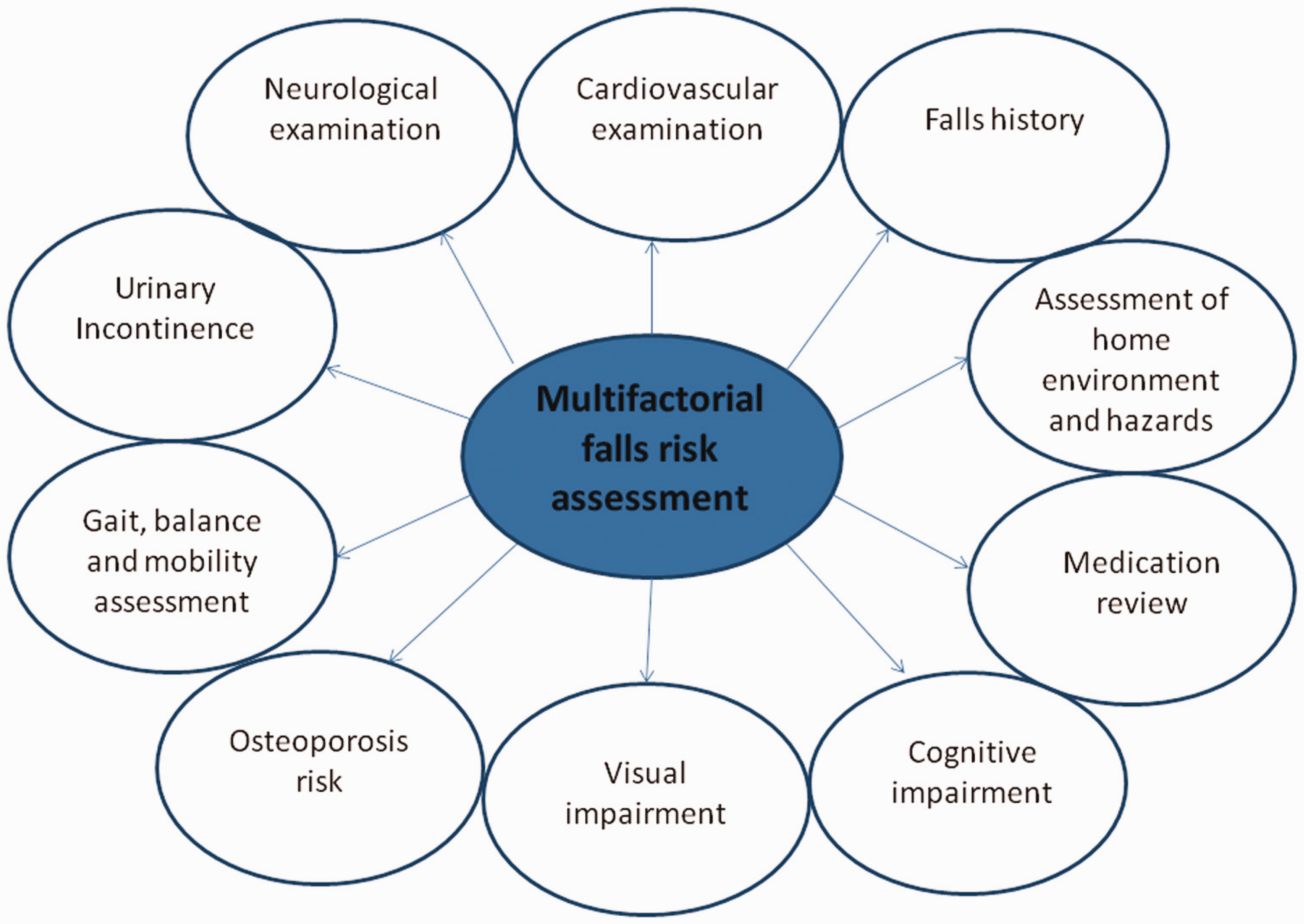
Multifactorial falls risk assessment.
Identification of a fall or falls risk will require appropriate time to assess and manage. Where provision of services varies across the UK with different tiered services, risk stratification could be used to best refer individuals to appropriate tiered services. Where falls assessment and support are being provided in primary care this this likely to require further assessment and follow ups. An example of this could be a patient who presents for an appointment with her GP following a fall. They are then booked to see a practice nurse for investigations such as lying and standing blood pressure, ECG and memory assessment. They have a further GP appointment to assess their osteoporosis risk, refer to other teams for example the falls team, memory clinic, continence clinic, social prescribing or make medication changes.
Multifactorial interventions
NICE advise those individuals at risk of falls should be considered for a multifactorial intervention which includes strength and balance training, intervention for home hazards, vision assessment and medical review (NICE, 2013). Interventions should also address confidence in performing activities of daily living, balance and concerns about falling.
Bone health
Vitamin D deficiency supplementation is beneficial in individuals at risk. NICE advise those aged 65 years and above should take a daily supplement of 400 international units equivalent to 10 micrograms of vitamin D throughout the year (NICE, 2022). Individuals living in residential care, who are more likely to deficient should be considered for supplementation, as this has been shown to reduce falls (Cameron et al., 2018). Other factors that make individuals at risk of vitamin D deficiency should be considered, including sun exposure, severe liver and kidney disease, obesity, malabsorption disorders and darker skin pigmentation (NICE, 2022). An assessment of calcium intake should also be made (NICE, 2022).
Women aged over 65 years, men aged over 75 years and those with a high risk of falls and fragility fracture require an osteoporosis assessment. A risk assessment will need to be performed using QFracture or FRAX, with further investigation e.g., DEXA, bone protection or referral determined based on this (NICE, 2022).
What is the future of falls protection?
Where the research affirms the use of strength and balance training, there is emerging promising research that simulating fall scenarios in a safe environment using obstacles and hazards and stepping exercises can reduce falls risk. For example, home-based electronic games using a step mat, changing movements on a treadmill and scenarios involving trips and slips on a wooden decking trip mat (Nørgaard et al., 2021 and Pelicioni et al., 2023). In an ever-digitising world, we may see the emergence of wearable devices, tailored digital health interventions and the use of AI to further personalise interventions.
Practice initiatives to reduce the falls risk in at risk patients could be undertaken as a quality improvement project (QIP). We have made some suggestions for a QIP in Box 1. QIP suggestions. To implement these guidelines and evidence, a QIP could be developed in your practice. QIP is a mandatory requirement of GP training. Suggestions for a QIP:
Develop a text message/paper document to either send or give to patients at risk/ who have fallen. This could include information about how to prevent falls including exercise advice and relevant local services
Develop a template for risk stratification of falls to determine referral into different local services and further investigations. This could include coding and documentation
Develop a pop up to prompt clinicians to assess bone health. Check compliance to guidelines before and after the intervention
Pilot a falls screening assessment at chronic disease appointments with nursing staff/ healthcare associates. Possible questions could include whether patients have fallen in the last year, NICE guided questions (the frequency, how they fell and the features of these) or the 3KQs. This could be further developed to create a pathway of referrals and assessment including requests for investigations
Develop a pop up to prompt assessment of postural hypotension in those aged 80 years and above. Monitor compliance to guidelines before and after the intervention
Key points
Falls in older adults can result in fractures, hospitalisation and increased mortality and have a high burden of associated healthcare costs Falls prevention is an important public health issue and general practice care provides opportunities for assessment of risk, treatment and signposting/referral to services Asking screening questions such as have you fallen in the last 12 months at QOF annual reviews or opportunistically improves identification of patients at high risk of falls Further stratification of risk of falls can be achieved using the World Falls Guidelines Current research has shown that exercise, multifactorial assessment and bone health assessment can improve risk of future falls