
Abstract
The World Health Organization (WHO) estimate that by 2050 approximately 2 billion people worldwide will have a degree of hearing impairment, and more than 700,000,000 will require hearing rehabilitation. The presentation and aetiology of patients with hearing loss changes with age, and this can be a useful starting point for an assessment. Another important discriminator in the approach to patients with hearing loss is the timing of onset, which will differentiate those needing urgent management from the more routine. Hearing loss may be ‘conductive’, due to blockage of sound passage to the inner ear, which is often reversible, or ‘sensorineural’, due to damage to the inner ear or auditory nerve such as seen in age-associated hearing loss (also known as presbycusis), which is usually permanent. This article aims to provide a systematic framework for assessing these patients in primary care and a guide to indicate when referrals to secondary care are necessary.
Clinical case scenario 1.
A 20-month-old girl is brought to see you by her mother who is worried her daughter is not babbling much compared with her older brothers. She seems to be delayed in her social milestones. She is otherwise well, born after a healthy pregnancy. There were no birth complications and she passed her newborn hearing screen. She is eating and drinking well and on track with her motor milestones, keeping up with her two older siblings. Both parents are smokers. Her mother mentions that she frequently has a blocked nose and nasal discharge. General examination is unremarkable and examining the ears is quite difficult because she is not cooperative and there is some wax in the ear canals. She is mouth-breathing throughout the consultation but otherwise examining the front of the nose is unremarkable.
Paediatric hearing loss
The presentation of hearing loss in children will vary with the age of the child and the developmental stage a child is at. Infants and toddlers with hearing loss will present with speech and/or developmental delay – this may be reduced babbling, few/no words at age 2 or delayed social milestones. It is important to ask directly for any such signs of delay. In a slightly older child, the parents may have observed them not responding to their own name or in the child using electronic devices, the volume being turned up high. In a school age child, they may be struggling with school work and with socialising with their peers. A minority of children with hearing loss will present with increased sensitivity to normal levels of sound. Important questions in the history should cover all the above points, as well as a comprehensive medical history. Antenatal history with a focus on infections, and any admissions to the neonatal intensive care unit are significant, as these are associated with higher incidence of hearing loss (Gov.uk, 2019). It is important to establish if the patient passed their newborn hearing screen or not, noting that those born outside the UK may not have undergone screening. Any other anomalies or medical conditions, for example, hypothyroidism, should be noted as they may point to syndromes associated with hearing loss e.g. Pendred’s syndrome or Trisomy 21.
Physical examination should be tailored to the patient's age. Observing a child in a consultation room can give clues about their hearing and their speech development. In the very young, or for example, children with trisomy 21, very narrow external auditory canals can make examination challenging. However, it is important to try to examine the ears, as wax occlusion or foreign bodies are easily treatable causes of hearing loss. Being able to accurately perform tuning fork testing in children below the age of 4 or 5 is unlikely to be possible and the examination needs to be tailored to the age, with great emphasis on observing behaviours e.g. does a child speak during the consultation? Is the speech clear? Is the volume of the speech appropriate?
Otitis media with effusion (OME), also known as ‘glue ear’ is the condition not to miss, as it is very common and quite treatable. Up to 80% of children will experience one or more episodes of glue ear and peak presentation is aged 2–5, which is critical for speech development and the beginning of their academic career. Middle ear effusions may be associated with adenoidal hypertrophy, as likely in the case above, so asking about nasal symptoms and observing signs of nasal obstruction is very helpful.
Management of paediatric hearing loss
Where hearing loss is suspected in a child, early referral to a paediatric audiology unit should be considered, as delayed diagnosis of hearing loss can affect development, and delaying treatment can have lasting consequences. The most common diagnosis in children for non-acute hearing loss is glue ear. Up to 80% of children will experience one or more episodes of glue ear and peak presentation is aged 2–5, which is critical for speech development and the beginning of school life. The National Institute for Health and Care Excellence (NICE) guidelines on OME highlight useful information to be shared with parents during the GP consultation, such as explaining the fluctuant nature of the condition and how children with hearing loss can be supported, particularly in the educational setting by informing their teacher, seating them close to the teacher, minimising background noise, and using visual aids (NICE, 2023).
If the hearing loss due to OME persists beyond 3 months then it is appropriate to consider intervention which may be hearing aids or ventilation tube (grommet) insertion after an appropriate consultation of the risks and benefits of each in secondary care. If wax is seen, then cerumolytics such as olive oil drops can be prescribed. Other causes of hearing loss may benefit from air or bone conduction hearing aids, bone conducting or middle ear implants or cochlear implants for the profoundly deaf (NICE, 2018a).
Clinical case scenario 2
A 45-year-old female presents with sudden drop in her hearing on the left side which occurred 24 hours earlier. She has experienced some mild dizziness, but is otherwise completely well. Her only other past medical history is of mild asthma, for which she has only ever required a salbutamol inhaler. Examination of her ears is unremarkable. When performing tuning fork testing, Rinne’s test reveals that on the right air conduction is louder than bone conduction and on the left bone conduction is louder than air conduction. On Weber’s test she hears the sound loudest in the right ear.
Adult hearing loss
Assessment of the adult with hearing loss will commence with a history. Salient points include onset and duration of symptoms, laterality, associated symptoms (particularly pain), ear discharge and vertigo. Other important medical history factors include noise exposure (often occupational) new medications with a particular focus on ototoxic medications such as aminoglycoside antibiotics and platinum-based chemotherapy agents. (See Fig. 1). Sudden unilateral hearing loss needs urgent management, whereas gradual bilateral hearing loss does not.
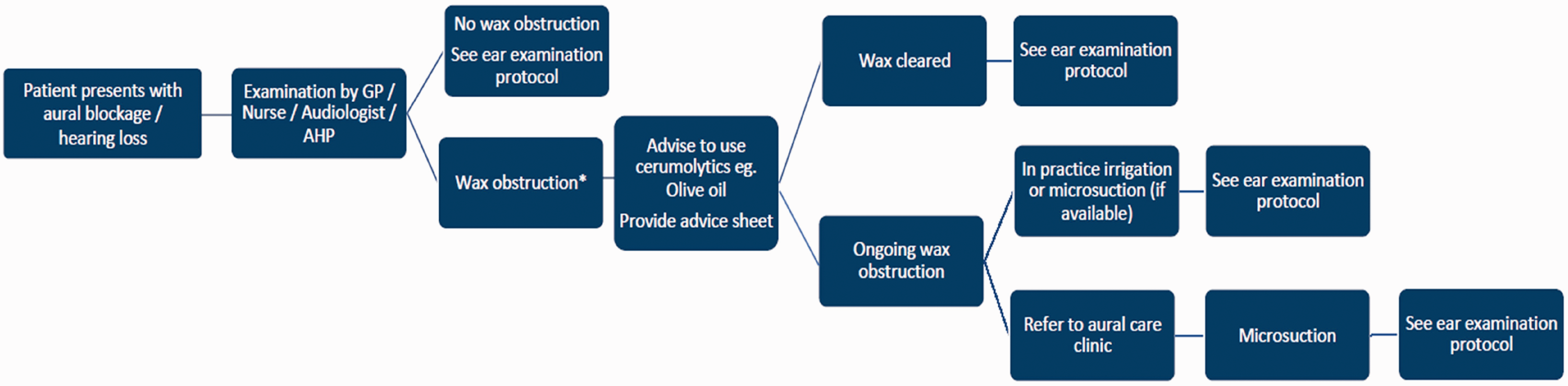
British Society of Otology (BSO) hearing loss pathway.
Patients with acute hearing loss are not suitable for a remote consultation because an examination of the ear and performing tuning fork testing is critical to differentiating unilateral sudden onset sensorineural hearing loss (SSNHL), which needs to be treated urgently by an ear, nose and throat (ENT) specialist, from other less time-critical diagnoses. In this context, sudden refers to hearing loss with onset over less than 3 days/72 hours (see Fig. 2). Even if wax is seen, it is important to perform tuning fork testing to avoid missing the presentation of SSNHL and delaying its treatment while the patient is using cerumolytics to clear the wax. A guide to performing and interpreting tuning fork tests is seen in Fig. 3. An app and website are available to guide performing and interpreting tuning fork tests and guiding referral at https://entintegrate.co.uk/starfish-for-clinicians. If unable to examine the patient using tuning forks, directing a patient to hum and asking which ear the sound is loudest in is a reasonable approximation to the Weber’s test, and can be performed remotely. If SSNHL is the suspected diagnosis, a referral to ENT for formal audiological testing should be done within 72 hours. In the past it was recommended that GPs start a course of oral steroids to treat SSNHL promptly, however, recent analyses suggest a short delay in steroid treatment does not affect hearing outcomes. There is an ongoing UK-wide clinical trial called STARFISH, which is trying to establish the best mode of steroid delivery and at the time of writing, the recommendation is to not start treatment in primary care, but rather refer patients to secondary care where they can be invited to participate in this trial.
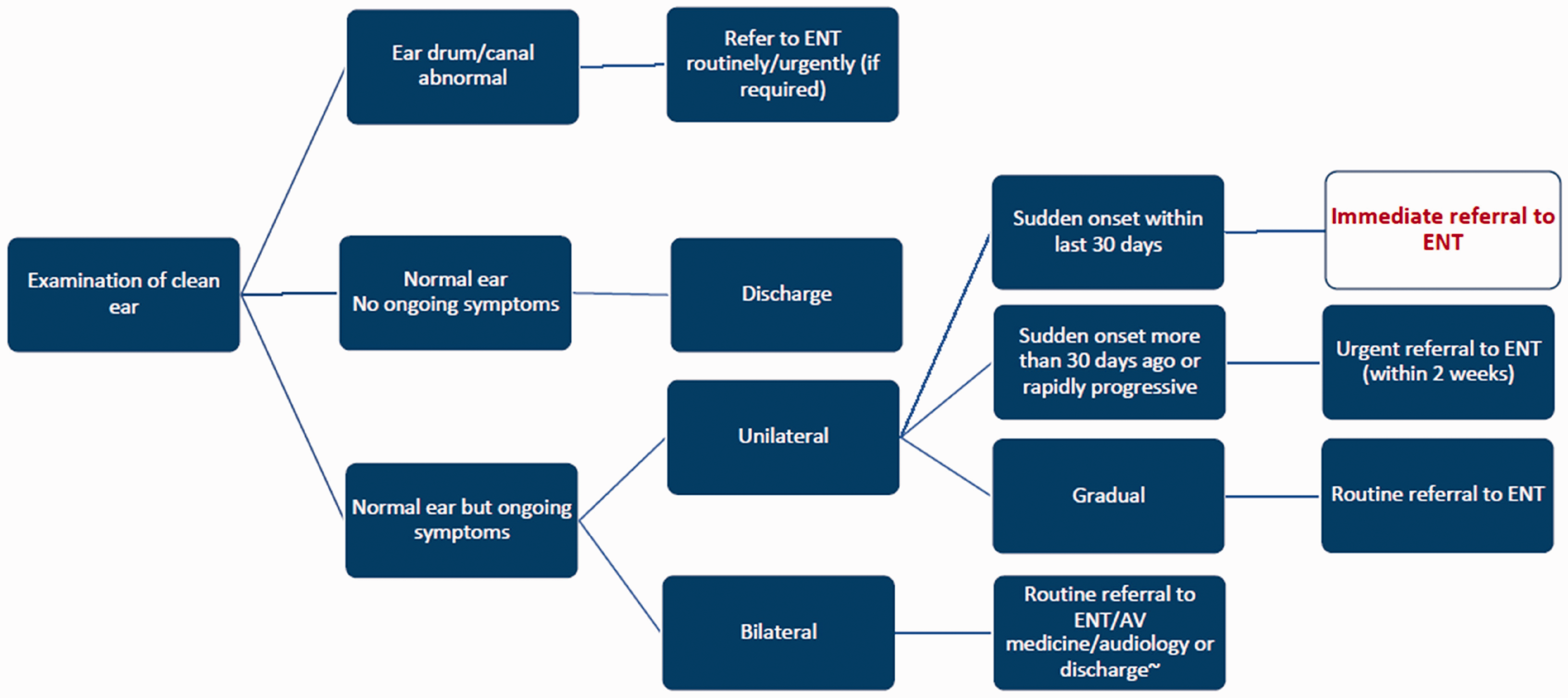
BSO ear examination pathway.
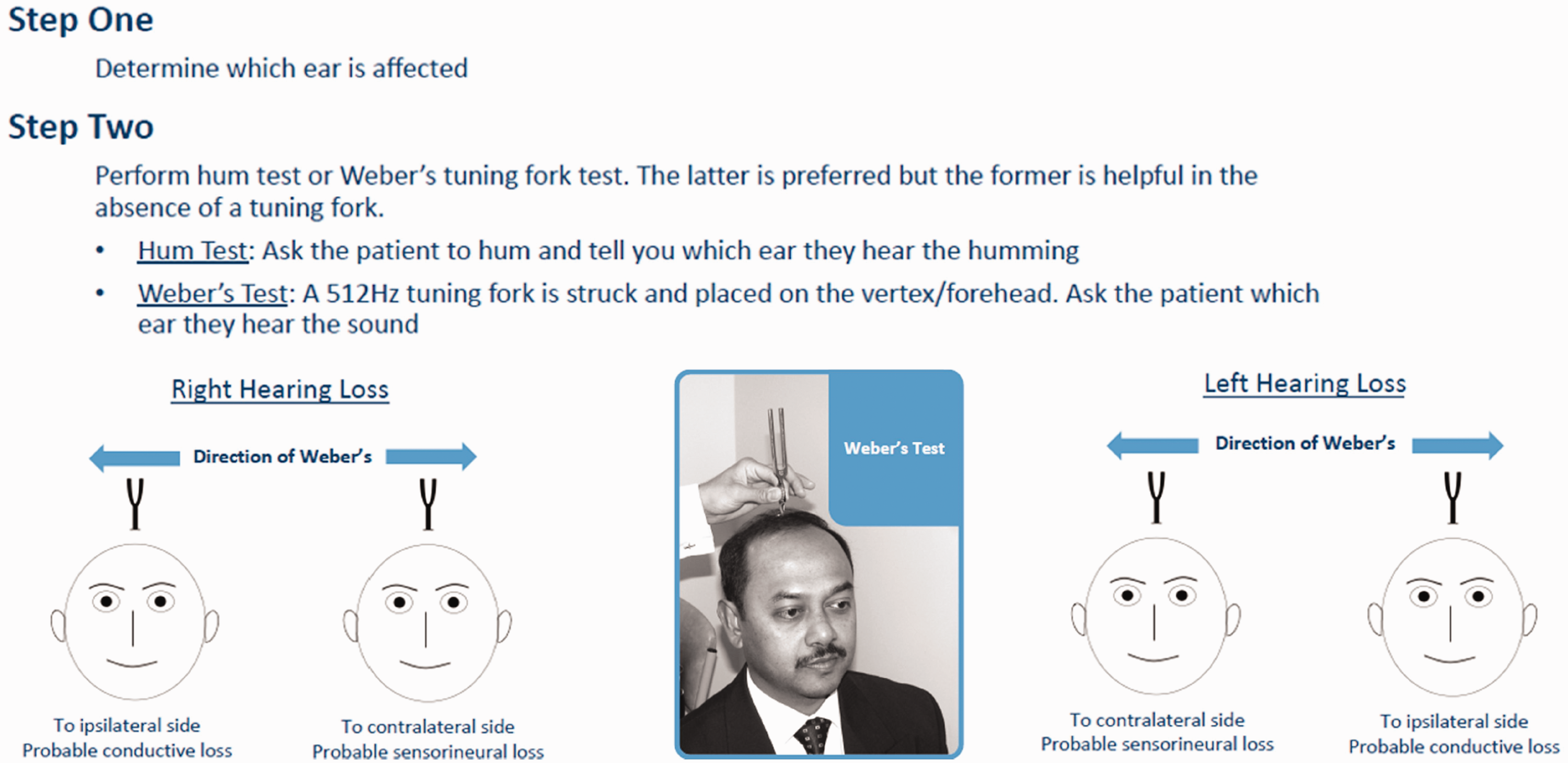
BSO guide to tuning fork testing.
In an adult, if purulent ear discharge is seen in the ear canal, this is likely to represent an otitis externa and topical antibiotics can be started according to local guidance. ENT departments often recommend ciprofloxacin as a safe first-line prescription, particularly because it gives Pseudomonas aeruginosa cover, which is a commonly encountered pathogen. An important differential diagnosis for the patient with ear discharge and hearing loss is cholesteatoma (a mass of keratinised squamous epithelium) but in the absence of other signs such as facial weakness or meningism, is not an ENT emergency. GPs should look for this as a pocket on the tympanic membrane filled with keratinous debris which may be white, but may also be obscured by infected material or pink, fleshy, inflammatory polyp.
Other findings on examination which might be linked with hearing loss include a perforation, a clean/dry retraction, a middle ear effusion which may be purulent, inflammatory or if after trauma blood. All of these are typically be associated with conductive hearing loss, which can then be diagnosed with tuning fork testing. Most of these can be managed conservatively in the first instance, with an interval follow up with repeat examination to check if the hearing loss and/or abnormality have resolved spontaneously. The purulent middle ear effusion in the context of acute otitis media may need treating, as per the NICE guidelines on acute otitis media (NICE, 2018a). Unilateral middle ear effusions in adults that do not resolve after 6 weeks should be referred urgently to ENT to exclude a nasopharyngeal tumour, particularly if the patient has any other red flags such as weight loss. Nasopharyngeal carcinoma is an uncommon presentation in the Caucasian population, but GPs should consider this in patients from the Far East where the incidence is higher.
In most cases of SSNHL, other than the tuning fork test abnormalities, the ear examination will be entirely normal. Out of the non-acute presentations, the most common diagnosis of SSNHL is age-associated hearing loss which will typically be a symmetrical ‘down-sloping’ (which relates to the progressively lowering hearing thresholds at higher frequencies on an audiogram) hearing loss. Other causes of SSNHL include noise-induced hearing loss, and less commonly, Meniere’s disease, autoimmune inner ear disease and progressive genetic causes of hearing loss.
Associated symptoms
In most presentations of hearing loss, pain is not a typical feature except in acute infections such as acute otitis externa (which is accompanied by ear discharge) and acute otitis media (which is typically associated with fever and a recent upper respiratory tract infection). However there are two frequently associated symptoms with hearing loss: tinnitus and dizziness. Tinnitus, (patient hearing a sound which is not originating in the external environment), is the most common symptom associated with hearing loss. In some individuals this may be the presenting symptom of an underlying loss, and therefore, any GP consultation on tinnitus needs to include many of the same questions as those in a hearing loss consultation. It is worth differentiating between pulsatile and non-pulsatile tinnitus, the latter being more common and linked to hearing loss. The other important distinction to ask for in the consultation is whether tinnitus is unilateral or bilateral. Unilateral tinnitus warrants non-urgent referral to ENT in case they are associated with a vascular anomaly (in pulsatile tinnitus) or vestibular schwannoma (in non-pulsatile tinnitus) (NICE, 2020). Examination in patients presenting with tinnitus is almost the same as in those with hearing loss only, except in the cases of pulsatile tinnitus, auscultation for bruits in the neck, post-auricular and temporal region should also be performed. For those with hearing loss and non-pulsatile tinnitus, providing hearing aids is often a very effective treatment for the tinnitus. An important consideration to enable treating patients holistically is to ask about anxiety symptoms as tinnitus is strongly linked to anxiety and this is very troublesome for patients. If very intrusive, tinnitus retraining therapy (usually incorporating cognitive behavioural therapy and education) can be beneficial.
Another important symptom to ask about in patients with hearing loss is dizziness. Discussing the full diagnostic pathway and differential diagnosis of vertigo is beyond the scope of this article; however, there are a few key points to note. Firstly, in the SSNHL presentation, vertigo is a poor prognostic indicator. Secondly, if a patient presents with an acute vertigo attack, the association with hearing loss differentiates acute labyrinthitis from vestibular neuronitis (the latter is a presentation with no deterioration in hearing). In both cases, a vestibular sedative such as Prochlorperazine can be prescribed to provide symptomatic relief, but it should not be used in the long term as it can have adverse effects in particular in relation to balance. Meniere’s disease is the triad of rotatory vertigo, low-mid frequency SSSHL and tinnitus. To diagnose Meniere’s disease, a patient should have at least two audiograms showing a fluctuating low-mid frequency SSNHL. It is a diagnosis that would be very difficult to make in the community. If this symptom triad is seen in primary care, a routine referral to the nearest secondary care balance clinic should be made.
Management of adult hearing loss
If SSNHL is suspected, a referral to ENT for formal audiological testing should be done within 72 hours as early treatment may improve outcome. This condition is treated with steroids, either high-dose oral prednisolone or intratympanic steroid injections. There is an ongoing UK-wide randomised controlled trial called STARFISH, funded by the National Institute for healthcare research open at over 50 UK sites. It is trying to establish the best mode of steroid delivery. As per NICE guidance, the recommendation is to not start treatment in primary care, but rather refer patients to secondary care where they can be assessed for sensorineural hearing loss, and currently trial eligibility. In the past it was recommended that GPs start a course of oral steroids to treat SSNHL promptly, however, the evidence as to whether this is the best delivery method for steroids is lacking.
Progressive age and noise-induced hearing loss can usually be referred directly to audiology via an AQP (any qualified provider) route, although local guidelines may vary and sometimes have an age cut-off. If there is an asymmetrical hearing loss, (defined by NICE as 15 dB or more difference at any two adjacent test frequencies, using test frequencies of 0.5, 1, 2, 4 and 8 kHz on the pure tone audiogram (NICE, 2018b), the patient will require investigation with a magnetic resonance image of the internal acoustic meatus to rule out a space-occupying lesion such as a vestibular schwannoma. Referral does not need to be done on a cancer pathway as even if present, vestibular schwannomas are benign and frequently either non-growing or slow growing at first diagnosis.
Most adult hearing loss is sensorineural and managed effectively with ‘behind the ear’ type hearing aids. Some adults with bilateral profound hearing loss are eligible for a cochlear implant in the NHS. In some adult and paediatric patients with hearing loss a surgical solution can improve hearing, by repairing a perforated or retracted tympanic membrane, rebuilding the ossicular chain with a prothesis (ossiculoplasty) or performing stapedectomy for otosclerosis.
The impact of hearing loss
Hearing loss affects all parts of patients’ lives as it is intrinsically linked to communication, it affects speech development, cognition, education, mental health and interpersonal relationships (WHO, 2024). It is extremely common to hear patients reporting that their hearing loss makes them feel isolated and/or makes them avoid social situations. Frequently patients struggle with hearing in noisy environments and find the effort of listening tiring. Specific populations who may struggle even more are ones with existing mental health issues, those who have music as a profession or hobby and those with dementia. This can even be true for those with a unilateral hearing loss and so referring patients for hearing rehabilitation is the key to delivering holistic care and improving quality of life (Brodie et al., 2018). Hearing loss and in particular the use of hearing aids have been shown to be a very important modifiable risk factor to prevent or delay the onset of dementia (Livingston et al., 2020). It is fitting for primary care clinicians to enquire about the impact of hearing loss and signpost those struggling to relevant community services and charities for social and psychological support where appropriate.
Key points
Hearing loss is very common worldwide and may be conductive or sensorineural Suspect hearing loss in children with delayed speech presentation The commonest cause of hearing loss in children is otitis media with effusion (‘glue ear’) SSNHL should be seen by ENT within 72 hours Steroids should not be started in primary care for acute hearing loss Gradual, bilateral hearing loss in adults is most commonly age-associated presbycusis