
Abstract
Metabolic health is an increasingly complex issue in UK primary care, yet attempting a comprehensive assessment within a typical 10-minute appointment can lead to superficial, directive and ineffective consultations. This article provides a highly pragmatic, curriculum-aligned framework for GP registrars preparing for the Simulated Consultation Assessment (SCA). Registrars can rapidly assess a patient’s readiness for behavioural change by shifting away from rigid diagnostic checklists and actively employing motivational interviewing (OARS (i.e. open questions, affirmations, reflections and summaries)) techniques. The framework anchors initial interventions to core lifestyle pillars and provides clear guidance on integrating medical escalation. This article equips registrars to deliver safe, patient-centred metabolic care that moves beyond generic advice by explicitly addressing the realities of regional specialist pathways and the current supply challenges surrounding glucagon-like peptide 1 (GLP-1) receptor agonists.
Clinical case scenario
Mark, a 38-year-old man, attends with fatigue and progressive weight gain. He works alternating day–night shifts and usually eats his largest meal late in the evening. Mark is frustrated by repeated unsuccessful attempts at dieting and asks whether he could start ‘one of those injections everyone is on now’. His body mass index (BMI) is 34 kg/m2. Initial blood tests reveal a glycated haemoglobin (HbA1c) in the prediabetic range and mildly elevated alanine transaminase (ALT).
Introduction
Metabolic health is an increasingly common and complex issue within UK primary care, contributing significantly to preventable morbidity. With approximately 64% of UK adults currently overweight or obese (NHS Digital, 2022), and the prevalence continuing to rise, the pressure on general practice is immense. Furthermore, nearly 4.9 million people live with type 2 diabetes (Diabetes UK, 2024), patterns which place considerable pressure on GP services.
GP registrars often find these consultations challenging; they must navigate complex behavioural change, significant emotional components and rising public interest in new pharmacotherapies, all within severe time constraints. However, attempting to encompass the entirety of metabolic medicine within a single, rigid template is unrealistic for a standard 10-minute appointment. As Miller (2026) highlights in a comprehensive review of integrating lifestyle medicine into primary care, clinical approaches must be focused and pragmatic.
Therefore, rather than providing a broad diagnostic overview, this article focuses on a single, practice-changing learning problem: how to effectively initiate metabolic change within a brief consultation. This article provides a practical framework for registrars preparing for the Simulated Consultation Assessment (SCA) by anchoring the approach to the core pillars of lifestyle medicine and explicitly utilising motivational interviewing (MI) techniques. Crucially, this framework does not exist in a vacuum; it provides a structured way to navigate the rising public demand for pharmacotherapy (e.g. glucagon-like peptide 1 (GLP-1) receptor agonists) and the complex, often fragmented, specialist referral pathways found across the UK. Registrars can move beyond ‘giving advice’ to delivering a robust, evidence-based management plan by integrating behavioural science with clinical escalation.
A behavioural approach: the 10-minute metabolic consultation
In practice, a comprehensive metabolic assessment – encompassing physical examination, psychological exploration and complex pharmacotherapy discussions – cannot be delivered in a single 10-minute appointment. Attempting to do so often leads to a superficial, directive consultation that fails to engage the patient.
Instead, the initial consultation should focus heavily on understanding the patient’s context and assessing readiness for behavioural change. To achieve this efficiently, registrars should move away from rigid, checklist-driven histories and consciously apply the principles of MI.
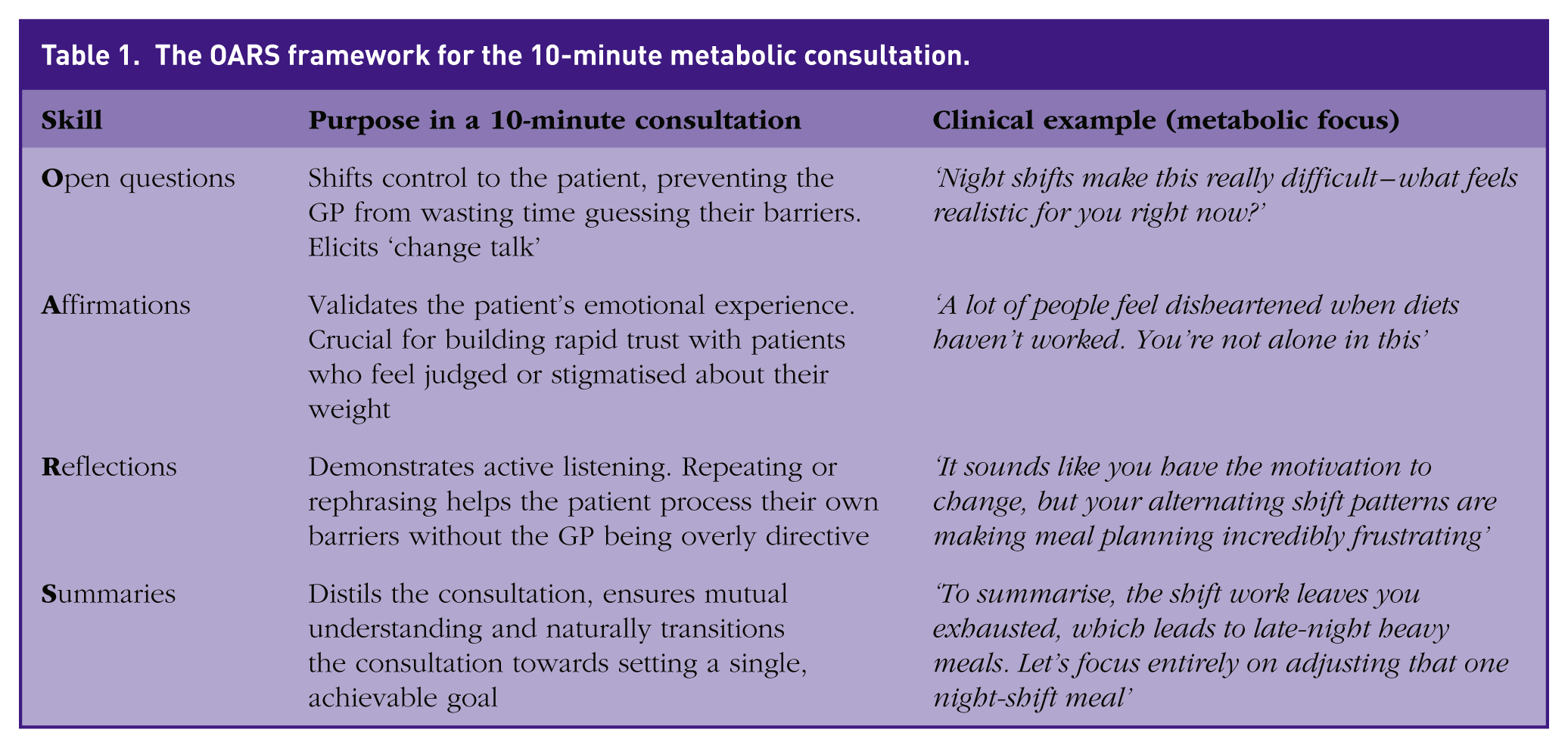
The foundational communication skills of motivational interviewing can be summarised by the acronym OARS (i.e. open questions, affirmations, reflections and summaries). Rather than relying on a rigid, checklist-driven history, registrars should use these techniques to rapidly assess readiness for behavioural change and build vital rapport within the time constraints of a standard appointment. Table 1 outlines how to practically apply these skills to a metabolic consultation.
The OARS framework for the 10-minute metabolic consultation.
Anchoring to lifestyle pillars
Rather than exploring every facet of the patient’s life, registrars should use the OARS approach to quickly assess the patient’s priorities within the core pillars defined by the British Society of Lifestyle Medicine (BSLM, 2024): nutrition, physical activity, sleep quality and stress or mood.
For example, asking about sleep hygiene and meal timing is particularly high yield for patients who eat late or work irregular patterns. Small, tailored adjustments – such as bringing dinner forward or identifying a 15-minute window for a brisk walk – are far more sustainable than generic advice to ‘eat less and move more’. By establishing a single, achievable behavioural goal and combining it with baseline objective data – such as waist circumference, blood pressure and an HbA1c – the clinician creates a safe, collaborative foundation for ongoing management.
Integrating medical escalation: pathways and pharmacotherapy
Although a collaborative lifestyle goal is the cornerstone of metabolic care, it is rarely the end of the conversation. Registrars frequently face patients who are demoralised by previous behavioural failures, actively seeking a pharmacological ‘quick fix’, or whose objective metabolic risk mandates immediate clinical escalation. In these scenarios, the consultation must sharply pivot. The clinician must seamlessly integrate medical management into the behavioural framework, ensuring that pharmacotherapy is positioned firmly as an adjunct to, rather than a replacement for, lifestyle change.
Merely stating BMI thresholds for specialist referral is inadequate; registrars must understand what these services provide to effectively manage a patient demanding a pharmacological ‘quick fix’. Furthermore, while the ‘Tier’ nomenclature is widely used conceptually, service structures and terminology vary drastically across the UK’s devolved nations. For example, while England utilises a formal Tier 1–4 system, Northern Ireland relies on regional Specialist Weight Management Services, and Scotland has its own distinct referral criteria. Registrars must familiarise themselves with their specific local Health Board or Trust pathways. Conceptually, escalating weight management services provide the following:
Community weight management: this is typically a community-based lifestyle programme providing structured dietary advice, behavioural modification techniques, and physical activity support. It is the appropriate first-line referral for a patient needing more intensive, sustained coaching than a brief GP consultation can provide.
Specialist multidisciplinary team: a specialist clinic involving physicians, specialist dietitians, and clinical psychologists. Crucially, this is not just ‘more diet advice’ – it is the highly regulated gateway for accessing complex pharmacotherapy (including GLP-1s under NHS pathways) and the mandatory preparatory step for bariatric surgery (National Institute for Health and Care Excellence (NICE), 2023).
NHS access varies significantly across regions, and long delays for specialist multidisciplinary services are common in many areas. Registrars must be prepared to discuss these timelines honestly from day 1 to prevent a breakdown in the doctor–patient relationship when the patient faces a multi-year waiting list.
The reality of pharmacotherapy: the ‘magic injection’
Once a patient understands the specialist pathway, or if they explicitly ask about bypassing the NHS for private options, registrars must confidently discuss the evidence base and limitations of the drugs themselves. GLP-1 receptor agonists (e.g. semaglutide) have fundamentally shifted metabolic care and can achieve 10–15% weight loss when combined with lifestyle modification (Wilding et al., 2021). However, registrars must be prepared to address the reality of global supply chain shortages; managing patient frustration regarding National Patient Safety Alerts and restricted prescribing is now a core component of this consultation. Registrars must clearly communicate the following to manage expectations:
The ‘scaffold’ analogy: explain that these medications act as a scaffold; they can help, but they work best alongside changes in eating patterns and activity. They are an adjunct to, not a replacement for, robust lifestyle changes.
Rebound weight gain: patients must be explicitly advised about the likelihood of significant partial weight regain when treatment stops if the prescribing window is not used to embed permanent behavioural changes.
Severe risks and MHRA warnings: GLP-1 receptor agonists are strictly contraindicated in patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2 (MEN 2). Patients must also be counselled on Medicines and Healthcare products Regulatory Agency (MHRA, 2023) safety warnings regarding acute pancreatitis and severe gastrointestinal adverse events.
NICE criteria: in the UK, prescribing is tightly regulated. NICE recommends GLP‑1 receptor agonists for adults with obesity as an adjunct to diet and exercise in those with a BMI ⩾35 kg/m2 and at least one weight-related comorbidity, or with a BMI in the range 30–34.9 kg/m2 who meet criteria for specialist weight-management referral (NICE, 2023).
Clinical case application: navigating Mark’s consultation
Mark’s presentation of progressive weight gain, fatigue and a direct request for pharmacotherapy is a common scenario that maps directly onto core RCGP capabilities. Attempting to address his prediabetes, shift work and medication request simultaneously will lead to an overwhelmed patient and a failed consultation; instead, the trainee must apply a streamlined, integrated behavioural framework.
Because Mark is frustrated by previous dietary failures, the registrar should lead with validation to prevent a breakdown in rapport, using OARS techniques to acknowledge that alternating shifts make meal planning incredibly difficult
Rather than a generic diet history, use open questions to target the lifestyle pillars most disrupted by his context, specifically sleep hygiene and meal timing, while framing his fatigue as a physiological consequence of his environment rather than a personal failure
Reframe the mildly elevated ALT and prediabetic HbA1c as objective, modifiable evidence of metabolic strain – likely early metabolic dysfunction-associated steatotic liver disease (MASLD) (Rinella et al., 2023) – and use the DIRECT trial evidence (Lean et al., 2018) to explain that intensive weight management can drive early metabolic disease into remission
Identify a collaborative goal focused on meal timing, such as planning a lighter, protein-dense meal for night shifts to reduce nocturnal insulin spikes, which is often more sustainable than generic advice to ‘eat less’
Address the request for ‘the injection’ using the scaffold analogy, explaining that, although GLP-1 receptor agonists are effective adjuncts (Wilding et al., 2021), he does not currently meet routine NHS criteria (NICE, 2023) for prescription without specialist referral
Provide clear safety-netting by counselling Mark on the ‘4 Ts’ of diabetes – thirst, toileting, tiredness and thinner – while advising review for symptoms of liver dysfunction or persistent right upper quadrant pain
Ensure psychological safety by screening for low mood and delegate an early progress check at 4–6 weeks to the wider primary care multidisciplinary team (MDT), such as a practice nurse or health coach, to troubleshoot barriers
Schedule a formal clinical review at 12 weeks to repeat the HbA1c and liver profile, providing objective feedback on the impact of his changes and planning long-term cardiovascular risk monitoring
Conclusions
Managing metabolic health within the severe time constraints of general practice is undeniably challenging, but it is not impossible. By abandoning rigid diagnostic checklists in favour of a targeted, behavioural approach, GP registrars can use their 10 minutes to lay a credible foundation for sustainable change. While a single consultation cannot reverse years of metabolic decline, applying the OARS framework, anchoring to core lifestyle pillars and maintaining a firm grip on the realities of medical escalation ensures that every appointment moves the patient forward safely and collaboratively.
Key points
Comprehensive metabolic care cannot be delivered in 10 minutes; shift from a rigid diagnostic checklist to a behavioural approach using MI (OARS) to build rapport and assess readiness to change
Focus brief lifestyle interventions on core areas like sleep hygiene, stress and meal timing – especially for complex patients like shift workers
Familiarise yourself with local criteria and waiting times for community lifestyle programmes and specialist MDT weight management services to manage patient expectations effectively
GLP-1 receptor agonists are highly effective but are adjuncts, not cures; registrars must proactively counsel patients on the requirement for concurrent lifestyle changes, gastrointestinal side effects and the risk of rebound weight gain upon cessation
Tailored follow-up (such as repeating prediabetic HbA1c at 12 weeks) and clear safety-netting for red flags are essential for safe, long-term metabolic care