
Abstract
Haematuria in children, defined as five or more red blood cells (RBCs) per high-power field in a mid-stream urine sample, is a relatively common finding in general practice that frequently causes parental concern. It can be broadly classified as macroscopic (visible blood, ‘cola’, or ‘smoky’ urine) or microscopic (occult blood detected only on microscopy or dipstick). Although the prevalence of microscopic haematuria is estimated to be low, the underlying causes span a wide spectrum from benign, transient conditions, such as urinary tract infection (UTI) or viral illness, to serious organ-threatening diseases, including glomerulonephritis, malignancy (e.g. Wilms’ tumour) and chronic renal disease. The GP registrar's critical role is to perform an efficient, safe initial work-up to reliably distinguish between benign and serious aetiologies, and to initiate timely, risk-stratified referral when ‘red flags’ are present. This article provides a systematic, evidence-based triage pathway for the primary care assessment of paediatric haematuria.
Clinical case scenario 1 – macroscopic haematuria in a child with recent sore throat
Noah is a 7-year-old boy brought to your GP clinic by his mother. He has had macroscopic haematuria for the past 2 days, which his mother describes as ‘smoky and dark brown, like cola’. Noah is generally well, but his mother recalls that he had a mild sore throat and fever approximately 2 weeks ago that resolved spontaneously. On examination, Noah is apyrexial, and his blood pressure is measured at 128/84 mmHg. You note slight periorbital oedema. Abdominal examination is unremarkable with no palpable masses.
Management and rationale
This case presents classic red flags for acute nephritic syndrome, specifically post-infectious glomerulonephritis (PIGN), given the: (1) macroscopic, cola-coloured haematuria (suggesting glomerular bleeding); (2) latency period (sore throat 2 weeks ago); and (3) hypertension and oedema (signs of fluid overload and renal involvement) (Niaudet and Somers, 2025).
Importantly, blood pressure interpretation in children must consider age, sex, and height. A systolic or diastolic blood pressure equal at or above the 95th centile for age and height constitutes hypertension. In this case, Noah’s blood pressure is significantly above the 95th centile, confirming true hypertension rather than an isolated elevated reading.
The presence of hypertension and oedema means this is an immediate medical emergency. Arrange immediate, same-day referral/admission to the paediatric team or paediatric nephrology. Initial investigations should not delay urgent referral because blood tests and imaging will typically be performed by secondary care according to local pathways. This demonstrates the GP registrar's responsibility to identify the critical red flags that mandate rapid, life-saving intervention and/or urgent referral to secondary care.
Assessment and triage of paediatric haematuria
Differential diagnosis: glomerular vs. non-glomerular
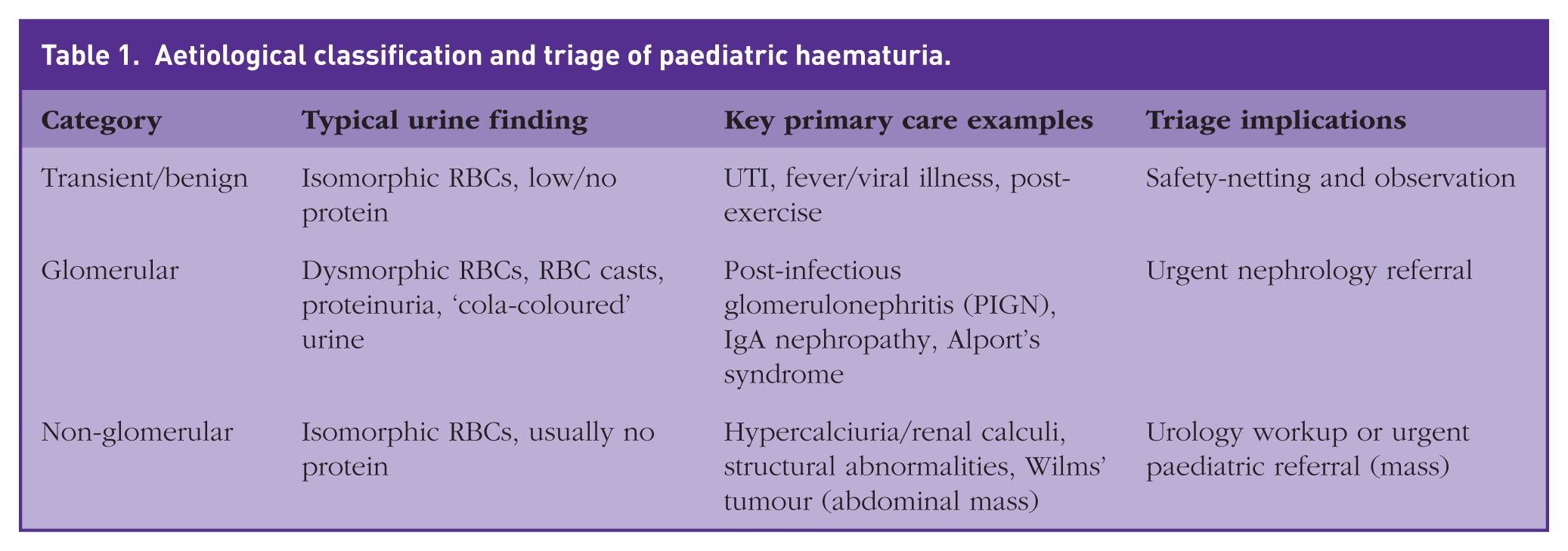
The fundamental step in assessing haematuria is determining its source: glomerular (from the kidney parenchyma/glomerulus) or non-glomerular (from the collecting system or lower urinary tract). Glomerular causes involve damage to the glomerular basement membrane. These are associated with systemic symptoms such as hypertension, oedema, and proteinuria. Examples include post-infectious glomerulonephritis (PIGN), which typically follows a streptococcal infection by 1–3 weeks, and immunogloblin A (IgA) nephropathy, which often presents with recurrent haematuria concurrent with a viral illness. Non-glomerular causes involve bleeding distal to the glomeruli. Hypercalciuria is a common cause of isolated, often recurrent, haematuria in children and is a key diagnosis to screen for in primary care (Srivastava and Schwaderer, 2009). Wilms’ tumour (nephroblastoma), the most common renal malignancy, presents primarily as an asymptomatic abdominal mass, though haematuria may occur in up to 25% of cases (Green, 1985). The initial assessment in general practice is essential for safe triage. Table 1 outlines aetiological classifications and key findings in haematuria.
Aetiological classification and triage of paediatric haematuria.
Clinical assessment: identifying red flags
History
A focused history is crucial to guide investigation, starting with the colour of the urine: smoky, brown, or cola-coloured urine is highly suggestive of glomerular bleeding due to oxidised red blood cells and is therefore a high-suspicion finding for nephritis, whereas bright red urine or the presence of clots points more towards lower urinary tract (urological) bleeding. Recent illness is also important, as an upper respiratory or skin infection in the preceding 1–3 weeks is highly relevant for post-infectious glomerulonephritis due to its delayed onset, while haematuria occurring simultaneously with a viral illness is more suggestive of IgA nephropathy. Associated symptoms should be explored, including dysuria or loin pain, which may indicate urinary tract infection or renal stones, as well as oedema (periorbital or dependent) or foamy urine, which suggests significant proteinuria or a nephrotic component. Finally, a family history of deafness and renal disease should raise suspicion for Alport’s syndrome.
Physical examination
The physical examination must focus on vital signs and evidence of systemic illness, with particular attention to blood pressure, which must be measured accurately using an appropriately sized cuff and interpreted against age- and height-adjusted paediatric centile charts; readings at or above the 95th centile indicate hypertension and represent a major red flag requiring urgent referral, with the National Institutes of Health’s paediatric blood pressure charts serving as useful reference tools (National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents, 2004). The examination should also assess for oedema, particularly periorbital or dependent oedema, which indicates fluid retention and possible renal compromise. Abdominal palpation is essential to assess for a renal or abdominal mass; however, if a mass is detected, palpation should not be forceful due to the risk of capsular rupture, and this finding mandates immediate urgent referral to paediatric services or paediatric nephrology care.
Investigations
Urine dipstick and microscopy
A positive urine dipstick for blood indicates the presence of haemoglobin or myoglobin and must be confirmed with formal urine microscopy to exclude pseudo-haematuria, such as urine discolouration from food, medications, or myoglobinuria secondary to rhabdomyolysis. Urine microscopy is the most valuable step in the primary care assessment because it helps distinguish glomerular from non-glomerular haematuria. The presence of dysmorphic red blood cells – particularly acanthocytes – reflects red cells that have traversed a damaged glomerular basement membrane and is highly specific for glomerular haematuria, warranting urgent referral to paediatric nephrology (Kohler et al, 1991). Red blood cell casts represent aggregates of erythrocytes within a protein matrix and are pathognomonic of acute glomerulonephritis, requiring immediate specialist referral. In contrast, isomorphic (uniformly shaped) red blood cells suggest a non-glomerular source of bleeding from the lower urinary tract and should prompt further urological evaluation, including screening for hypercalciuria. The presence of co-existing significant proteinuria, defined as a protein-to-creatinine ratio greater than 20 mg/mmol, alongside haematuria is a concerning feature and strengthens the indication for specialist referral (Gauci et al., 2023).
Initial blood and urine tests
If red flags (e.g. hypertension, oedema, dysmorphic RBCs, oliguria) are present, urgent referral should take priority, and investigations should not delay transfer to secondary care. Where clinically appropriate and where this does not delay referral, the investigations oulined below may be considered in primary care or requested by paediatrics on admission.
Baseline renal function should be assessed with urea, creatinine and electrolytes (U&Es) to evaluate for acute kidney injury. Where glomerulonephritis is suspected, a targeted immunological screen should be performed, including an antistreptolysin O (ASO) titre or streptozyme test to identify recent streptococcal infection consistent with post-infectious glomerulonephritis, along with complement levels (C3 and C4), because transiently low C3 levels are characteristic of this condition (Horvath et al., 2022). In cases where a non-glomerular source is suspected, screening for hypercalciuria is recommended, with a random urinary calcium-to-creatinine ratio greater than 0.6 suggesting hypercalciuria.
Clinical case scenario 2 – recurrent UTIs and haematuria
Andrea is a 1-year-old girl referred to your practice following her third episode of UTI in 6 months, despite previous antibiotic treatment. The latest urine culture was negative, but the dipstick was positive for blood. Her mother reports that Andrea is otherwise well, but she occasionally gets very upset when passing urine, and sometimes the urine looks slightly pink, even when she doesn't have a proven infection. On examination, Andrea is thriving and appears well. Her temperature is normal. Her blood pressure is within the normal range for her age. Abdominal examination is soft with no masses. Urine microscopy (from last sample) shows isomorphic (uniform) RBCs with no casts and no significant proteinuria. She has no family history of deafness or renal failure.
Management and rationale
Case scenario 2 presents a picture of recurrent UTI and non-glomerular haematuria, where the primary concern is underlying urological pathology or metabolic cause, rather than acute nephritis. Recurrent UTIs in a young child (under 2 years), particularly a girl, are a concern for underlying structural or functional abnormalities (e.g. vesicoureteral reflux or obstructive uropathy). The haematuria is intermittent and the red cells are isomorphic, suggesting a non-glomerular (urological) source. The absence of systemic red flags (normal blood pressure, no oedema, no proteinuria) makes acute nephritis unlikely.
Because acute red flags are absent, urgent referral is not required, but the history of recurrent UTIs warrants a systematic investigation for non-glomerular causes and underlying structural issues.
Screen for hypercalciuria: request a random urinary Ca/Cr ratio to rule out hypercalciuria, a common cause of recurrent non-glomerular haematuria and potential stone formation.
Referral: given the recurrent UTIs, routine referral to a paediatrician or paediatric urologist is required for further investigation (e.g. renal ultrasound to check for structural anomalies, which is often the standard workup for recurrent UTIs in this age group).
Case 2 demonstrates the need to investigate underlying structural or metabolic causes in children with recurrent symptoms and non-glomerular haematuria.
Monitoring children with transient or benign haematuria (no red flags)
A large proportion of children seen in primary care fall into this low-risk category. Clear guidance on follow-up and safety-netting is therefore essential. For children with isolated microscopic haematuria, isomorphic RBCs, normal blood pressure, no proteinuria and no systemic symptoms:
Repeat urinalysis and blood pressure measurement at 4–6 weeks
If haematuria resolves: no further action required
If haematuria persists beyond 3 months:
Repeat urine microscopy and protein: creatinine ratio
Screen for hypercalciuria (urinary Ca/Cr ratio)
Consider routine referral to paediatrics or paediatric nephrology
Parents should be advised to seek urgent medical review if the child develops:
Dark or cola-coloured urine
Facial or peripheral oedema
Headaches or vomiting (suggesting hypertension)
Reduced urine output
Key points
Hypertension is the single most important ‘red flag’ in paediatric haematuria, mandating immediate referral due to the risk of acute kidney injury (AKI) or hypertensive emergency
The key distinction between glomerular and non-glomerular haematuria is made by urine microscopy: dysmorphic RBCs or RBC casts are pathognomonic of glomerular disease (nephritis), while isomorphic RBCs suggest a urological cause (e.g. stones, hypercalciuria, UTIs)
Oedema, oliguria or an abdominal mass alongside haematuria are urgent referral criteria for potential glomerulonephritis or malignancy (Wilms’ tumour)
For persistent, isolated haematuria with isomorphic RBCs and no red flags, screen for hypercalciuria using a random urinary Ca/Cr ratio (greater than 0.6)
For transient, isolated haematuria with a normal examination and labs, provide clear safety-netting advice regarding monitoring for oedema, dark urine and headaches, with repeat urinalysis and blood pressure checks until resolution
Haematuria 2–3 weeks after infection suggests post-infectious glomerulonephritis (PIGN, often with low C3), while haematuria synchronous with infection suggests IgA nephropathy
Supplemental Material
sj-docx-1-ino-10.1177_17557380261456249 – Supplemental material for From practice to pedagogy: How the Salaried Portfolio Innovation Scheme is shaping GP educators
Supplemental material, sj-docx-1-ino-10.1177_17557380261456249 for From practice to pedagogy: How the Salaried Portfolio Innovation Scheme is shaping GP educators by Glory Lai, Clara Mead Robson, Mariya Rashid, Yasmin Bashir, Ajitha Arunthavaraja, Sanjiv Yogarajah, Istiakh Chowdhury, Urva Patel, Karan Bhatt and Anna Schmid in InnovAiT
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.