
Abstract
Spinal dural arteriovenous fistula (SDAVF) is an important cause of venous congestive myelopathy, as timely treatment offers the potential for neurological recovery. However, it is sometimes misdiagnosed when presenting with atypical intracranial or brainstem lesions. Although venous congestion in SDAVFs typically develops adjacent to the shunting site, altered venous outflow dynamics occasionally result in remote parenchymal involvement. We present a case of lower cervical SDAVF manifesting as a remote medullary lesion mimicking area postrema syndrome. Subsequent spinal imaging and digital subtraction angiography revealed a right C6 SDAVF with cranially directed venous drainage. Fusion imaging of three-dimensional rotational angiography and anatomical MRI delineated the venous outflow bottleneck with abrupt focal narrowing at the cerebellomedullary fissure, which likely served as a morphological bottleneck contributing to preferential medullary congestion. The fistula was successfully treated via endovascular embolization, achieving complete angiographic obliteration and clinical recovery. A literature review was also conducted to characterize the clinical features and identify the common diagnostic pitfalls associated with these rare manifestations; however, the precise anatomical mechanisms for remote lesions remain elusive. This case highlights a potential anatomical mechanism wherein focal narrowing in the venous drainage pathway may predispose to atypical lesion localization. Furthermore, therapeutic considerations are discussed, emphasizing a stepwise treatment strategy in which endovascular obliteration is prioritized when the anatomy is favorable and surgical disconnection is reserved for refractory cases.
Plain language summary
A spinal dural arteriovenous fistula (SDAVF) is an abnormal connection between an artery and a vein near the spinal cord. This connection increases pressure in the veins, which usually causes swelling in the spine. However, in rare cases, the blood flows upward and causes swelling in the brainstem instead. We treated a patient whose fistula was located in the neck (cervical spine), but the resulting swelling was found higher up, in the brainstem. To understand why the swelling happened so far away from the fistula, we used a specialized 3D imaging technique. We discovered a “bottleneck”—a physical narrowing of the veins at the point where the brain meets the spine. This narrowing acted like a dam, forcing the high-pressure blood into the brainstem tissue. The fistula was successfully closed using an endovascular procedure, where medical glue was injected via a microcatheter to block the abnormal connection without the need for open surgery. The patient made a full recovery. Our findings help explain the anatomical reason for this unusual blood flow, which can help other medical teams diagnose this condition more effectively.
Keywords
Introduction
Spinal dural arteriovenous fistula (SDAVF) is a critical cause of venous congestive myelopathy; timely treatment enables neurological recovery. However, it is occasionally misdiagnosed when presenting with brainstem involvement. Although parenchymal edema typically occurs adjacent to the shunt, altered venous outflow dynamics can cause remote lesions. We report a case of lower cervical SDAVF presenting as a remote medullary lesion, where radiological evaluation demonstrated a venous outflow bottleneck at the cerebellomedullary fissure. This case illustrates how anatomical constraints restrict venous compensation, increasing outflow resistance and precipitating regional edema. We also conduct a review of the relevant literature and discuss a stepwise therapeutic strategy, prioritizing endovascular treatment alongside surgical approaches.
Case report
A 63-year-old man presented to a community hospital with a 1-week history of vertigo, nausea, persistent hiccups, and gait disturbance. Brain MRI demonstrated a focal signal abnormality involving the left dorsal medulla (Figure 1(a) and (b)). The symptoms and the lesion topography mimicked area postrema syndrome, suggesting inflammatory or demyelinating disorders and prompting referral to our institution.

Preoperative imaging of the brainstem lesion and associated cervical spinal dural arteriovenous fistula. Axial (a) and sagittal (b) 3D-FLAIR images show a lesion predominantly involving the left dorsal medulla with caudal extension. Coronal contrast-enhanced MRI (c) and sagittal T2-weighted imaging (d) show a dilated, elongated posterior spinal vein.
Contrast-enhanced and T2-weighted spinal MRI revealed perimedullary serpiginous enhancements and flow voids, suggesting vascular pathology (Figure 1(c) and (d)). Spinal digital subtraction angiography (DSA) identified SDAVF supplied by the right C6 segmental branch of the ascending cervical artery, remote from the medullary lesion. To further characterize angioarchitecture, three-dimensional rotational angiography (3D-RA) delineated the venous outflow pathway. The shunted flow ascended the posterior spinal vein, entered the cerebellomedullary fissure via the medial posterior medullary vein, and drained through the vein of the inferior cerebellar peduncle into the superior petrosal sinus.
The dilated vein exhibited an abrupt focal narrowing at the cerebellomedullary fissure, adjacent to the medullary lesion (Figure 2(a)–(c)). No arterial connections from the feeding or adjacent segmental arteries to the spinal arteries were identified.
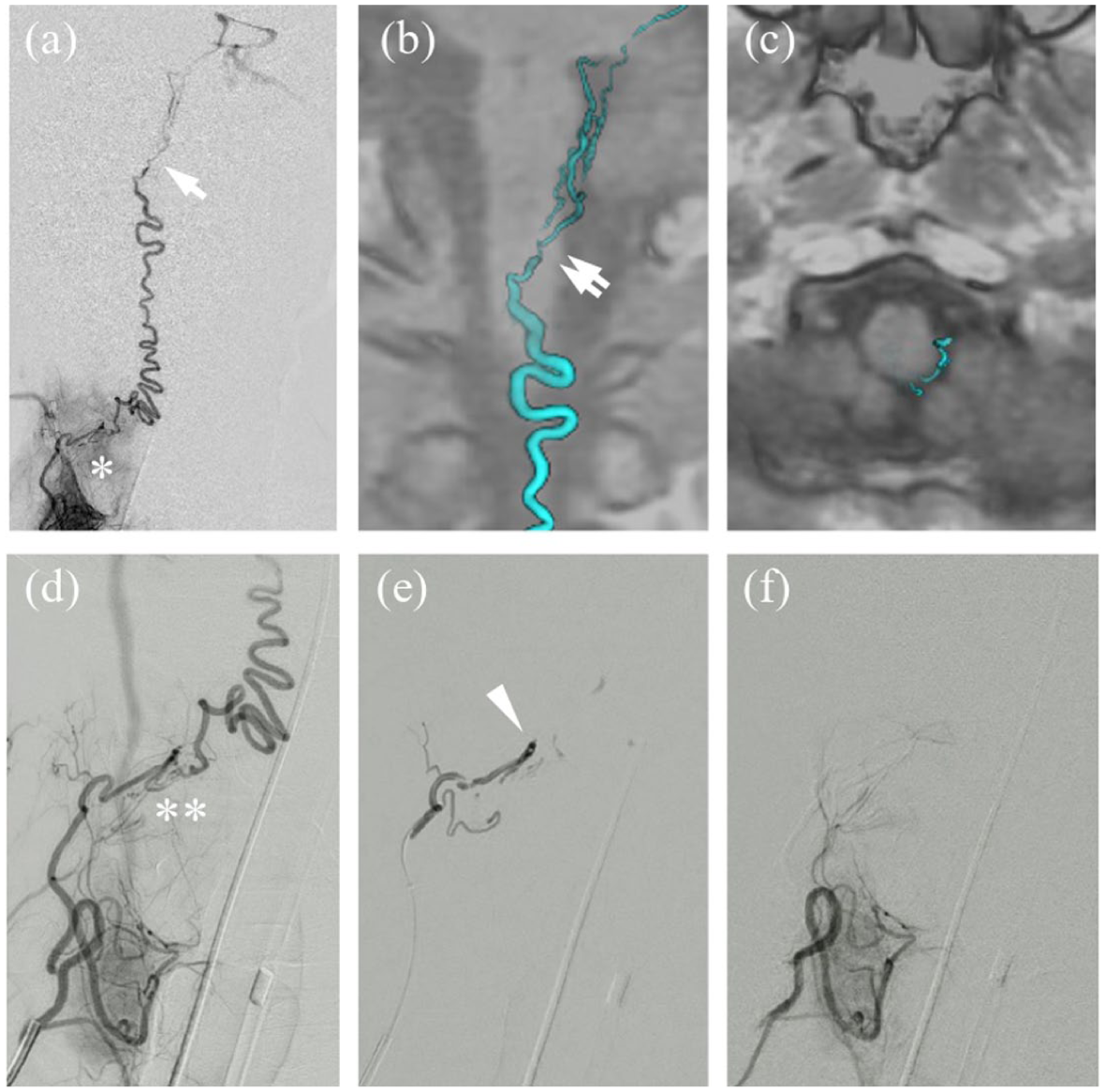
Angiographic evaluation and endovascular treatment of the cervical spinal dural arteriovenous fistula. (a)–(c) Angioarchitectural evaluation of the spinal dural arteriovenous fistula. (a) Digital subtraction angiography shows a fistula at the C6 level (asterisk) with cranially directed drainage and an abrupt focal narrowing of the draining vein (arrow). (b) 3D-RA confirms the venous narrowing (double arrows). (c) Fusion imaging of 3D-RA and anatomical MRI localizes the venous narrowing precisely at the cerebellomedullary fissure, identifying the anatomical “bottleneck.” (d)–(f) Endovascular treatment sequence. (d) Pre-embolization selective angiography shows the shunting site (double asterisk). (e) Embolic material is injected via the microcatheter positioned in close proximity to the shunt (arrowhead). (f) Post-embolization angiography confirms complete obliteration of the fistula.
Given the favorable anatomy, we adopted a stepwise treatment strategy, with endovascular obliteration as the initial approach and surgical disconnection reserved for incomplete obliteration or recurrence. Following microcatheter placement in close proximity to the shunt, a single injection of n-butyl cyanoacrylate successfully penetrated the shunting point, achieving complete obliteration of the fistula (Figure 2(d)–(f)). Neurological symptoms improved on postoperative day 1. Follow-up MRI on postoperative day 21 demonstrated regression of the brainstem lesion, and the abnormal perimedullary veins were no longer detectable (Figure 3). At 10 months, the patient remained asymptomatic.
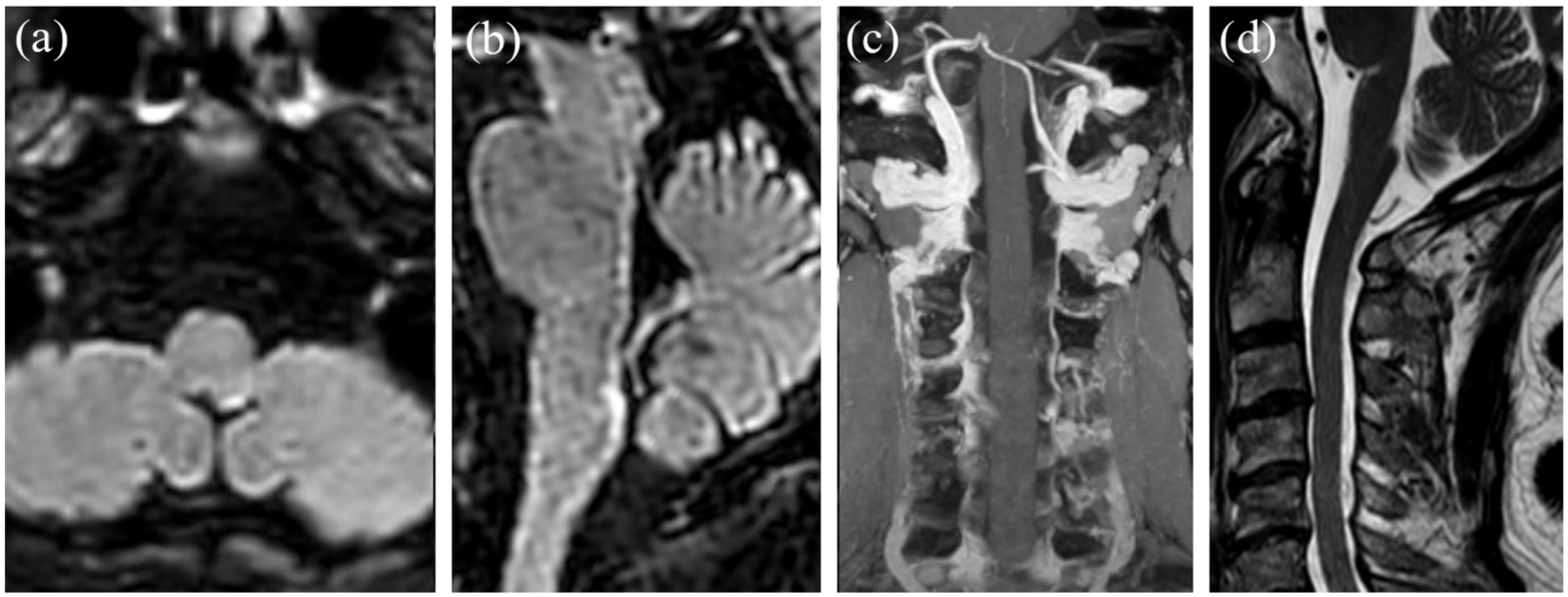
Postoperative follow-up imaging after endovascular treatment. Axial (a) and sagittal (b) 3D-FLAIR images show marked regression of the brainstem lesion. Coronal contrast-enhanced MRI (c) and sagittal T2-weighted imaging (d) demonstrating the resolution of previously found abnormal veins or associated flow voids.
Literature review
A literature review was conducted to identify previously reported cases of SDAVF presenting with remote brainstem lesions. PubMed, Google Scholar, and Web of Science were searched on December 16, 2025, using the search string: “spinal dural arteriovenous fistula” AND (“brainstem” OR “medulla”), without date restrictions. We focused on cases with isolated brainstem involvement to examine site-selective (“remote”) manifestations; cases with concomitant cervical spinal cord involvement, likely reflecting typical contiguous cranial propagation adjacent to the shunt, were excluded. Only studies providing sufficient clinical detail were included, while non-English publications were excluded due to limited accessibility for full-text evaluation. Four relevant cases were identified (Table 1).1–4
Clinical features of previously reported SDAVF with remote brainstem lesion.
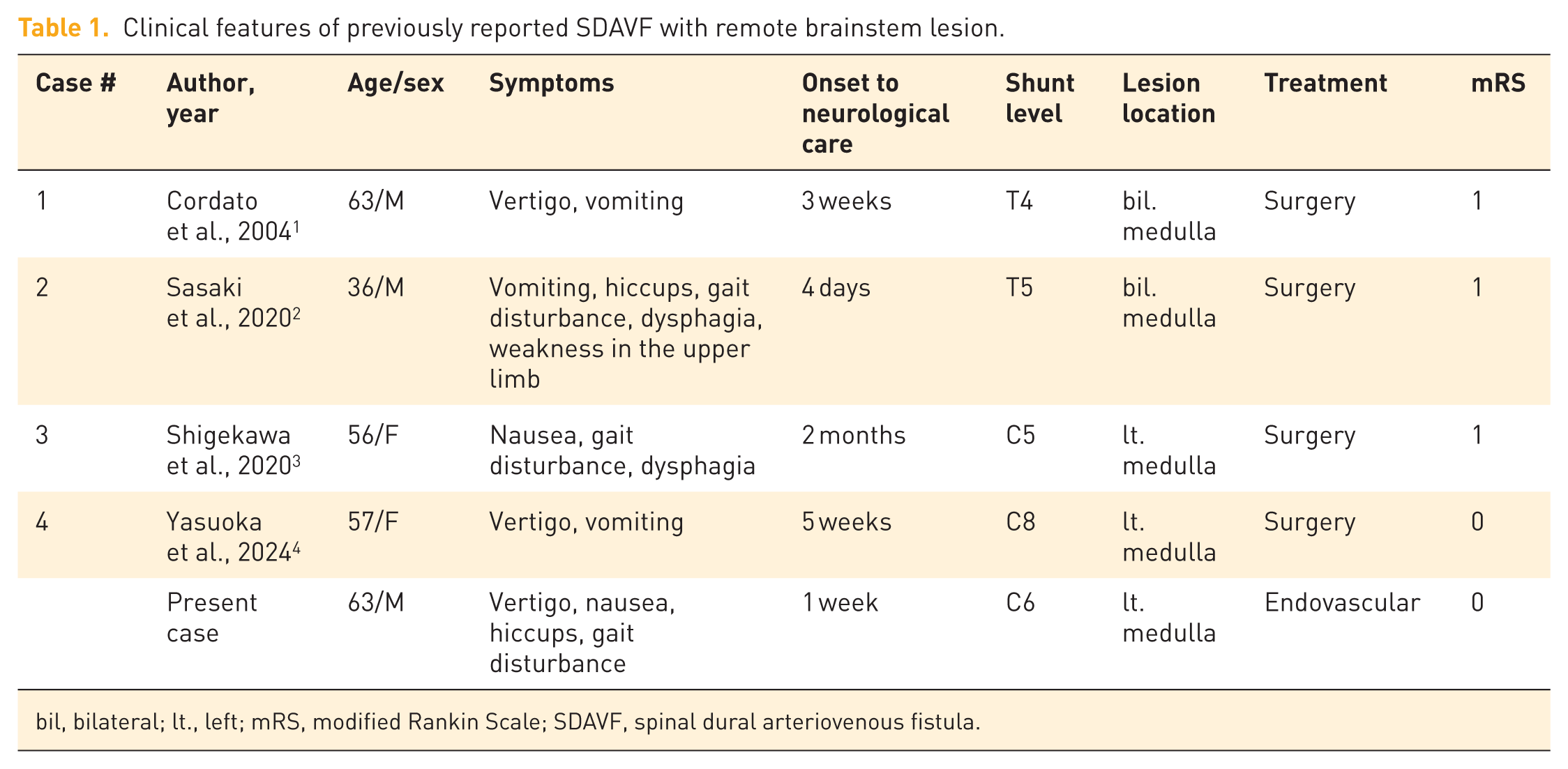
bil, bilateral; lt., left; mRS, modified Rankin Scale; SDAVF, spinal dural arteriovenous fistula.
Nausea and vomiting were the common symptoms, followed by vertigo and gait disturbances, suggesting vestibular or truncal ataxia. Across the identified cases, shunt levels ranged from T5 to C5, and lesion laterality varied between unilateral (left-sided) and bilateral presentations. While all previous cases underwent surgical disconnection, our case was managed via endovascular embolization. The outcomes were generally favorable, despite Case 2 presenting with pretreatment limb weakness.
Discussion
SDAVFs are a rare but clinically important vascular disorder, as prompt diagnosis and timely treatment can substantially mitigate progressive—and occasionally severe—venous congestive myelopathy. SDAVFs most commonly occur at the thoracic (65.3%–67.7%) and lumbar (22.9%–26.9%) levels, whereas cervical involvement is relatively rare (3.8%–5.2%).5,6 This distribution can cause diagnostic delay, especially when presenting with brainstem symptoms rather than classic longitudinal myelopathy. From our literature review, previous cases presented with nausea, vomiting, or gait disturbances; the non-specific nature of symptoms frequently led to diagnostic delays, typically weeks. Patients are sometimes referred for neurological care after misdirected gastroenterology or otolaryngology evaluations.
Classically, SDAVFs present on MRI as longitudinally extensive spinal cord lesions with contrast enhancement, making their differentiation from inflammatory, demyelinating, or neoplastic disorders a formidable diagnostic challenge. Indeed, in the present case, SDAVF was initially overlooked during the differential diagnosis. In some cases, a patchy pattern of nonenhancement within an otherwise enhanced cord lesion—referred to as the “missing-piece sign”—might provide a diagnostic clue. 7 Abnormal perimedullary veins, reflecting venous congestion, are often visualized as dilated and elongated vascular structures on contrast-enhanced imaging or as flow voids on T2-weighted sequences; however, these findings may occasionally be subtle or occult, and repeated DSA may be required for a definitive diagnosis, causing diagnostic delay. 8
Pathophysiology of the remote brainstem lesion
Venous congestion of the spinal cord associated with SDAVFs typically develops adjacent to the shunting site; however, remote parenchymal lesions occasionally occur when the venous outflow dynamics are altered. In the present case, the lesion was localized to the medulla (inferior extent at C1) with relative sparing of the intervening cervical spinal cord, suggesting a hemodynamically “remote” manifestation rather than simple contiguous cranial extension. A literature review indicates that even with shunts located as distally as the T5 level, the resulting parenchymal edema was consistently localized to the medulla with selective sparing of the intervening spinal cord. Several anatomical and hemodynamic factors likely contribute to this atypical remote localization.
First, the area postrema, located in the dorsal medulla, lacks a robust blood–brain barrier with endothelial tight junctions, which normally restrict permeability and protect the brain parenchyma from toxic blood-borne substances and elevated intravascular pressure. 9 Consequently, elevated venous pressure is more readily transmitted to the interstitial space, resulting in region-selective parenchymal vulnerability.
Second, susceptibility to venous congestion is influenced by regional drainage capacity, which may account for the relative sparing of the cervical spinal cord. The cervical spinal cord possesses a redundant, low-resistance venous network with the vertebral venous plexus, facilitating pressure dissipation. 10 By contrast, the brainstem venous system is organized predominantly in a cranio-caudal direction with progressively increasing vessel caliber. Retrograde venous flow engorges the small-caliber brainstem veins with limited capacity for pressure redistribution.
Finally, this intrinsic hemodynamic vulnerability is further compounded by the anatomical constraints of the craniocervical junction. Fusion imaging of 3D-RA and anatomical MRI delineated the shunted flow pathway traversing the narrow anatomical corridor of the cerebellomedullary fissure. At this juncture, the draining vein is subject to an abrupt focal narrowing. Our findings suggest that such focal anatomical constraints may function as a venous outflow bottleneck. While direct hemodynamic measurements were unfeasible, the close spatial correlation between the site of narrowing and the parenchymal edema provides a plausible morphological explanation for the remote lesion localization. This anatomical constraint likely restricts compensatory venous dilatation, resulting in elevated upstream venous pressure and the site-specific edema remote from the primary shunt.
Together, these findings support the concept that medullary involvement in lower cervical SDAVF may represent a site-selective, hemodynamically remote manifestation, potentially related to bottleneck-mediated vulnerability of the brainstem, rather than simple longitudinal venous congestion.
Treatment strategy for spinal dural arteriovenous fistulas
Direct microsurgical disconnection of arteriovenous shunts has traditionally been regarded as the standard treatment for SDAVFs. Surgical management is associated with high cure and low recurrence rates. A literature review reflects this traditional preference, as all identified cases were managed via surgical disconnection. However, this can sometimes be overly invasive in certain clinical contexts. With advances in neurointerventional technology, endovascular obliteration has emerged as a viable therapeutic alternative in selected cases. Favorable anatomical conditions include the ability to advance a microcatheter to the proximity of the shunt and the absence of spinal arteries arising from or communicating with the feeding artery. Meta-analyses of SDAVFs, predominantly involving thoracolumbar lesions, have demonstrated higher initial cure rates with surgical treatment than with endovascular therapy; however, the overall complication rates appear comparable between the two approaches, consistent with recent findings.5,6,11 In this context, treatment selection should balance efficacy with procedural risk and invasiveness, particularly in relation to patient comorbidities and angioarchitectural features. Accordingly, a stepwise treatment strategy—attempting endovascular treatment when the anatomy is favorable and reserving surgery for recurrence—represents a pragmatic and clinically feasible approach.
In endovascular treatment for cervical SDAVFs, particular caution is warranted. Compared with thoracolumbar lesions, inadvertent migration of liquid embolic material into the spinal arteries or vertebrobasilar system can result in catastrophic complications, including brainstem or spinal ischemia leading to tetraparesis. Therefore, precise interpretation of the angioarchitecture, together with meticulous reflux control, is essential for successful treatment.
In this patient, owing to the favorable vascular anatomy, an endovascular-first strategy guided by careful interpretation of the angioarchitecture successfully achieved complete fistula obliteration without recurrence, illustrating the feasibility of this approach in appropriately selected cases.
Conclusion
Although spinal venous congestion typically occurs adjacent to the shunting site, SDAVFs can occasionally manifest as remote lesions. In the present case, anatomical narrowing at the cerebellomedullary fissure may function as a venous outflow bottleneck, contributing to preferential medullary congestion. Although surgical disconnection remains highly curative, its invasiveness limits its feasibility in patients with comorbidities. Advances in endovascular techniques now offer less invasive therapeutic options when the vascular anatomy is favorable.
Supplemental Material
sj-pdf-1-tan-10.1177_17562864261456509 – Supplemental material for Remote brainstem lesion associated with lower cervical spinal dural arteriovenous fistula—venous outflow bottleneck: a case report and literature review
Supplemental material, sj-pdf-1-tan-10.1177_17562864261456509 for Remote brainstem lesion associated with lower cervical spinal dural arteriovenous fistula—venous outflow bottleneck: a case report and literature review by Yohei Takenobu, Kayoko Yukawa, Jumpei Sugiyama, Takeshi Kawauchi, Yukinori Terada, Manabu Inoue and Kenji Hashimoto in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.