
Abstract
Introduction
Schizophrenia is a severe form of mental illness, which affects about 24 million people worldwide. 1 Schizophrenia has a multi-factorial aetiology 2 and is among the most burdensome and costly illnesses globally. 3 It requires a disproportionate share of medical resources due to its early onset and chronic and severe nature. 2 There are three main aspects to the treatment of schizophrenia:
medications for the treatment and prevention of symptoms,
psychosocial interventions to help patients and families cope with the illness and
rehabilitation to help patients reintegrate into the community and possibly regain employment. 3
In the early 1970’s the atypical antipsychotic clozapine was discovered. It was found to be significantly more effective than other antipsychotic drugs without many of the extra-pyramidal side-effects (EPSEs) seen with the first-generation antipsychotics. 4 Significant problems were, however, associated with its use. Shortly after its introduction in Finland in the 1970’s, 17 cases of agranulocytosis were recorded amongst about 3000 patients treated. 5 The agranulocytosis led to eight fatalities which resulted in the voluntary withdrawal of clozapine from the market. It was re-introduced in the 1990’s but with compulsory haematological monitoring. 6 Clozapine is now licensed in Ireland for treatment-resistant schizophrenia in patients who have severe, untreatable neurological adverse reactions to other antipsychotic agents, including atypical antipsychotics. 7 One of the many challenges in medicine is non-adherence with therapy. Adherence has been defined as; “the extent to which a person’s behaviour – taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a healthcare provider”. 8 Non-adherence rates in psychiatric disorders have been shown to vary widely 9 however the average rate of non-adherence for schizophrenia is 50%. 10 Non-adherence can lead to the development of treatment-resistance schizophrenia. 11 Factors which have been found to be consistently associated with non-adherence include: poor insight; negative attitude or subjective response towards medication; previous non-adherence; substance abuse; shorter illness duration; inadequate discharge planning or aftercare environment; and poorer therapeutic alliance. 10 Medication-specific factors for non-adherence include adverse effects, ineffectiveness, regimen complexity and cost. 9 Studies have shown that patient education can improve medication non-adherence.12-14 Psychiatric patients who received written information with verbal reinforcement were also found to be significantly more adherent with their medication than control subjects. 15 Users of psychiatric services are more likely to have an impaired reading ability 16 and a recent review has shown patients want information that was tailored to their needs. 17 Individuals who suffer from both a mental illness and limited literacy are likely to be unable to effectively use mental health care services. 18 HL has been defined as; “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions”. 19 A strong link has been found between literacy and health 20 and also between health literacy and outcomes. 21 Despite this, a considerable proportion of written information currently available for psychiatric patients has been found to be at a reading age of 14 or above. 16 In the literature a readability level of grade 6 or lower is considered ideal for patient information as 75% of adult Americans can read at this level without difficulty and is a reasonable goal for most healthcare instructions. 22 One of the most common methods of estimating HL levels is to use the REALM. 23 This screening tool is a word recognition and pronunciation test that uses medical terms of varying levels of difficulty. 24 It is a validated screening instrument that can be used to identify patients with low health literacy levels and only takes 3-5 minutes to complete. A shortened version of the REALM was validated in 1993, this is more practical for busy primary care settings. 25 It allows reading levels to be determined quickly and easily and can be carried out by personnel with minimal training.
Patients should be provided with information that is simple and clear to help them understand their medical condition and its treatment. Combining easy-to-read written patient education materials with oral instructions has been shown to greatly enhance patient understanding. 26 Education materials are recommended to be short, clear and simple and should include pictures. The effectiveness of a low-literacy educational handout was demonstrated by increasing pneumococcal vaccine rates. 27 Foster and Rhoney assessed the readability of printed patient information for epileptic patients using the Flesch Reading Ease Score (FRES) and Flesch-Kincaid Grade Level (FKGL). 28 The FRES formula rates text on a 100-point scale based on the average number of syllables per word and words per sentence. 29 The higher the FRES, the easier it is to understand the document. The FKGL analyses, and rates, text on an American grade-school level based on the average number of syllables per word and words per sentence e.g. a score of 8.0 means that a person in eighth grade should understand the text. The majority of information tested by Foster and Rhoney was written at a level that exceeded the reading ability of many patients. The provision of such information is impractical. Education materials for patients should be written at the lowest grade possible as this has been shown to increase comprehension. 19
In the North Lee Mental Health Services patients who are started on clozapine are given information by the physician and a short digital video disk (DVD). 30 They also receive a PIL from the manufacturer of clozapine. 31 Thereafter patients receive a weekly/fortnightly/monthly supply of clozapine. Unless requested, patients do not receive any further formal education. Because treatment with clozapine is usually started when the patient is acutely symptomatic, it is possible that explanations provided at the time are poorly absorbed or retained. 32 No estimate of clozapine patient’s health literacy, relative to the information provided by the PIL, has previously been carried out. We are therefore unaware of how well the patients health literacy level corresponds to the educational materials provided. We hypothesise that the patient information leaflet provided to the clozapine patient was not aligned to the health literacy levels, of this population, as estimated by the REALM.
Methods
Ethical approval was obtained from the Clinical Research Ethics Committee of the Cork Teaching Hospitals and the Clinical Director of the North Lee Mental Health Services. All patients were pre-screened by the Clozapine Clinic Nurse Specialist, prior to the patients receiving any request from the pharmacist to be included in the study. The Clozapine Clinic Nurse Specialist works closely in conjunction with all of the psychiatrists (whose patients attend the clinic) and in consultation with these psychiatrists, patients who were acutely psychotic at the time of the study were excluded.
The Clinic Nurse gave a brief explanation about the study to all patients and they were then introduced to the research pharmacist. Inclusion criteria for the study were any patient who was receiving clozapine and registered with North Lee Mental Health Services. Exclusion criteria were those aged less than eighteen years of age. Verbal consent was obtained from all participants and the voluntary nature of the study was explained to them. This study was completed between March and July 2010. Demographics such as gender, age, employment, duration of treatment with clozapine and smoking status, were gathered from all participants. The total daily clozapine dose and information regarding the clozapine DVD was also noted. The REALM screening tool was then administered to each patient and scored out of 66. A score of 61 or greater indicates “adequate” HL, a score of 45-60 indicates “marginal” HL and a score of less than 45 indicates “low” HL. Using the National Adult Literacy Agency (NALA) approved guide to plain English, 33 a user-friendly PIL on clozapine was designed by the pharmacist. The FRES and the FKGL were used to assess readability, with the aim of producing a PIL with a higher FRES and a lower FKGL than the company produced PIL. The Flesch Kincaid Readability Formula is inbuilt within the Microsoft Word® application. 29
Statistical analysis
The statistical package for the Social sciences (SPSS) Version 15 (SPSS, Chicago, Ill.) was used for data analysis. Descriptive statistics include frequencies, percentages and mean values. Means are reported with standard deviation (SD) where appropriate. Bivariate analyses were conducted to determine any statistically significant relationships between varying parameters e.g. REALM score versus dose of clozapine. Pearson’s correlation coefficient is reported for parametric data and Spearman’s rho is used to describe correlations with non-parametric data. Correlations were significant at the 0.05 level unless otherwise specified.
Results
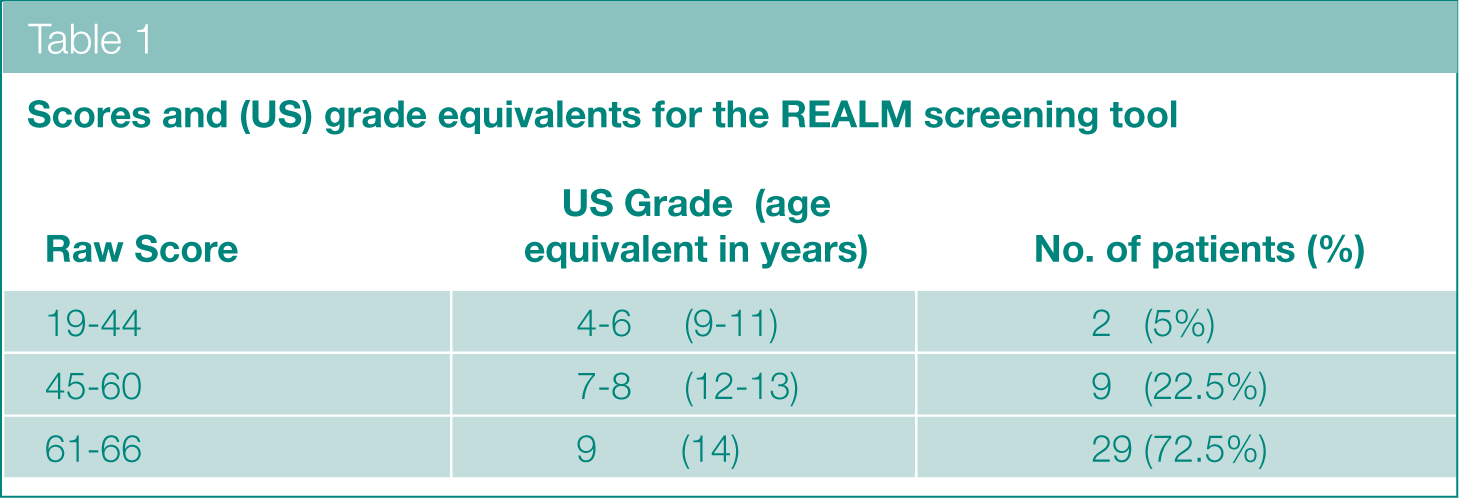
Forty patients (65% male, 95% unemployed and 70% smokers) of average age 38.0 years (±11.2) completed the REALM screening tool. Scores were marked out of 66. The average score was 60.6 (±8.7). Twenty-nine patients (72.5%) were found to have “adequate” health literacy. The remaining eleven patients were found to have either “marginal” or “low” health literacy (Table 1).
Scores and (US) grade equivalents for the REALM screening tool
Only 23% of those interviewed recalled watching the DVD on clozapine which is given to them at the initiation of clozapine therapy. The total daily clozapine dose ranged from 75-600mg, with an average of 373mg (±132.6). Average duration of treatment with clozapine was 39 months (±38.0). Correlation of REALM scores with age were not statistically significant (-0.065, p=0.69). Correlation of REALM and total daily dose (TDD) of clozapine was significant (-0.317, p<0.05).
Table 2 shows the higher readability scores found with the pharmacist-produced PIL. The company-produced PIL was found to have a FKGL of 10.3. This means a person would need to have attained the equivalent of the American tenth grade level (equivalent to age 15) to be able to read this document. The pharmacist-designed PIL was found to have a FKGL of 8.1. This means a person would need to have attained the equivalent of the American eighth grade level (equivalent to age 13) to be able to read this document.
Results of the Flesch-Kincaid readability score for PILs
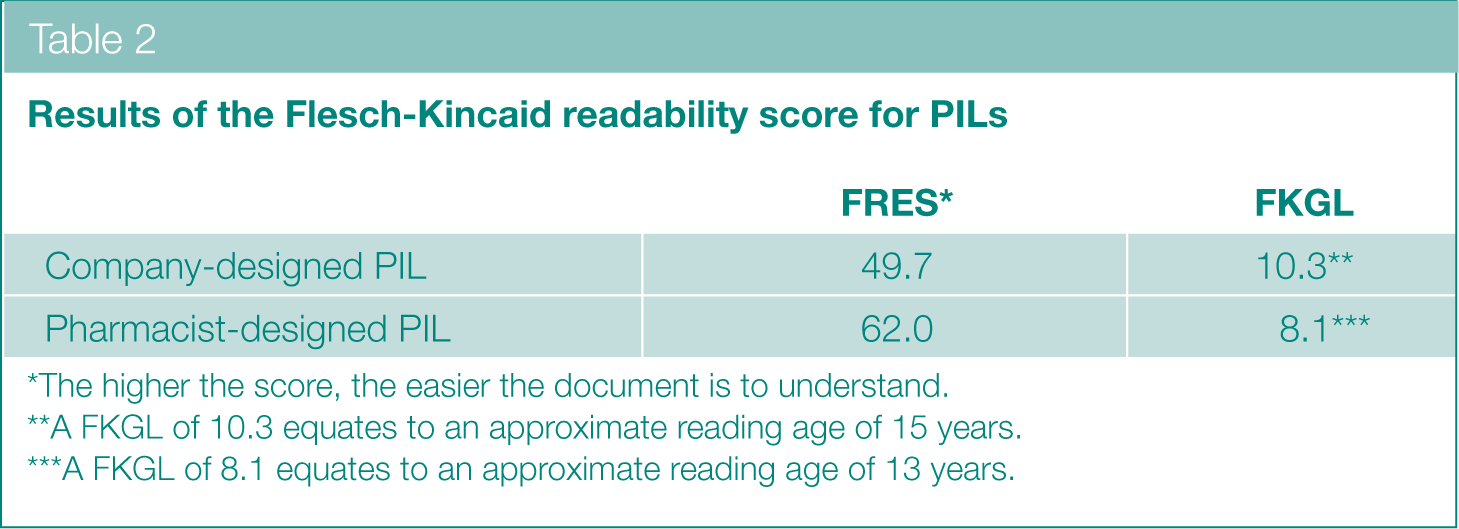
The higher the score, the easier the document is to understand.
A FKGL of 10.3 equates to an approximate reading age of 15 years.
A FKGL of 8.1 equates to an approximate reading age of 13 years.
Discussion
A total of 40 subjects completed the REALM screening tool with the average score of 60.6. This means the average patient from the study population would be expected to be able to read material at the American ninth grade level upwards (equivalent to age 14 upwards), 25 which is considered “adequate” health literacy. Of the overall study population, 22.5% were found to have marginal health literacy. This means that they would struggle with most patient education materials, whilst 5% with low health literacy would not be expected to be able to read prescription labels. The REALM results for this population are in contrast to another study which found 76% of the population to read at or below the US seventh- to eighth-grade level. 24 However it should be noted that REALM has never been specifically validated for use in psychiatrically unwell patients. The reading levels for the study population were compared to the readability of the company-produced PIL and the pharmacist-designed PIL. The results of the REALM indicate that 95% of the study population would be expected to be able to read the pharmacist-designed PIL, whereas only 72.5% of the study population would be expected to be able to read the company-produced PIL.Users of psychiatric services have been shown to be more likely to have an impaired reading ability. 16 Because of the strong correlation between health literacy and health outcomes, 34 it is important to take these facts into consideration. 35 When REALM scores for the population were compared with age, no significant correlation was found (p=0.690) which was unexpected 36 but may be due to the average age of the study population being 38. When REALM scores were compared with total daily dose of clozapine, a significant correlation was found (p<0.05). It was found that the higher the REALM score, the lower the total daily dose of clozapine. This suggests patients with high health literacy are not as ill as those with poor health literacy. This is consistent with other studies, which found inadequate health literacy to be associated with poorer health status. 37
Fewer than one in four of the study population recalled watching the DVD on clozapine which is given to them at the initiation of therapy. The importance of educating psychiatric patients has been well documented.15,32 It also serves as a reminder that giving written/visual information to a patient does not necessarily equate to the patient reading/watching it.
The effectiveness of low-literacy educational handouts has been established 27 however not all materials are adapted to the reading ability of the target audience and this should be recognised, specifically in vulnerable groups such as those with mental illness.
Conclusions
More than one in four patients receiving clozapine has either marginal or low health literacy as estimated by the REALM screening tool. As assessed by the FRES and FKGL, the pharmacist-designed PIL was an easier document to read and understand than the company-produced PIL. It is important to be aware of patient’s health literacy when providing them with information as health literacy is strongly correlated to health outcomes. Although the pharmacist-designed PIL may be a more easily read document, further research is required to design a PIL which meets the needs of low literacy patients.
Footnotes
Acknowledgements
We would like to acknowledge all the participants who took part in the study. We would especially like to thank the Clozapine Clinic Nurse Specialist; Erin Foley for her assistance. This study was undertaken in part fulfilment of the MSc in Clinical Pharmacy (SB), School of Pharmacy, University College Cork.
The authors wish to declare that there is no conflict of interest in this work.
Ethical approval to undertake this study was obtained from the Clinical Research Ethics Committee of the Cork Teaching Hospitals. In addition the Clinical Director of North Lee Mental Health Services was consulted and his permission obtained to undertake the study.
No funding was received for this study.