
Abstract
Case Description
A 16-year-old male with spastic quadriparesis secondary to cerebral palsy underwent baclofen pump placement in August 2024. During a routine refill in September 2025, a hard, non-mobile bump was noted over the pump's central port. Ultrasound revealed low acoustic density material with tubelike structures at the site. Pediatric neurosurgery suspected catheter dislodgement, and the refill was deferred. Surgery two days later revealed that the pump tubing had migrated ventrally and calcified near the refill port, though the pump remained well-secured. Scar tissue was excised, and the tubing was repositioned behind the pump.
Discussion
It is estimated that 80–92% of patients diagnosed with cerebral palsy are affected by spasticity. Baclofen pumps are used when conservative treatments (e.g., bracing, therapy, oral antispasmodics, botulinum toxin) fail and require strict monitoring to ensure proper function. This case demonstrates an atypical baclofen pump catheter migration, where suspected dislodgement prevented the refill process, requiring surgical intervention. It underscores the importance of meticulous physical examination, ultrasound evaluation, and clinical judgment to prevent accidental catheter puncture during refills.
Conclusions
Routine follow-up with established care teams is essential for early detection of baclofen pump catheter dislodgement and to ensure proper positioning and function.
Introduction / background
Cerebral palsy (CP) encompasses a broad group of conditions characterized by abnormalities in muscle tone, anatomy, and function. 1 There are multiple phenotypic subtypes of CP. The primary motor subtypes include spastic (diplegia, hemiplegia, quadriplegia), dyskinetic (dystonic, choreoathetotic), and ataxic. Current studies estimate that the vast majority of individuals with CP fall into the spastic motor subtype, with smaller proportions presenting with dyskinetic or ataxic subtypes. 2 Approximately 80–92% of patients with CP experience spasticity, with the most recent data suggesting 84% fall under the spastic subtype.3,4
There are many conservative options for the treatment of spasticity in CP (e.g., physical/occupational therapy, splinting/bracing, oral anti-spasmodic medications, botulinum toxin/phenol/alcohol injections). If patients fail to respond to treatments or if these options are contraindicated, surgical implantation of an intrathecal (IT) baclofen pump may be considered. 5 This modality requires a multidisciplinary approach. An IT baclofen trial may be performed by a physiatrist or in consultation with other specialists and involves administering a test bolus prior to pump implantation. If the patient responds, the pump is surgically implanted, followed by long-term programming and management, usually with a physiatrist or neurologist. 6
Before initiating spasticity treatment, clear functional goals must be established to justify intervention. Will spasticity management help the patient regain functional mobility? Will the chosen interventions improve the patient's ability to perform daily activities or reduce the physical burden on caregivers? Is treating spasticity beneficial for reducing the risk of complications?7,8
Careful patient selection and clearly defined functional goals are therefore essential when considering IT baclofen pump implantation. The patient and family must understand the treatment and be able to reliably attend routine follow-up appointments for pump refills and replacement at the end of the device's shelf life. 9 Families should also be thoroughly counseled on the risks and signs of baclofen withdrawal. Pump malfunction or component displacement requires urgent evaluation to prevent potentially life-threatening complications. 10
This case describes an atypical presentation of IT baclofen pump catheter dislodgement in a child with spastic quadriparesis secondary to CP. This complication required urgent surgical intervention to prevent the onset of baclofen withdrawal.
Informed consent
The patient is a minor and has cognitive deficits secondary to his disability that preclude his ability to provide informed consent. Therefore, parental informed consent was obtained in accordance with ethical guidelines for publication of this case report and any accompanying images. The process was conducted with the assistance of a certified Spanish interpreter, and the consent form was provided in Spanish to ensure full comprehension by the parents.
Case presentation
A 16-year-old male with a past medical history of spastic quadriparesis secondary to CP underwent IT baclofen pump implantation in August 2024. During a routine outpatient pump refill visit, a previously unrecognized mobile soft tissue mass was identified adherent to the pump and overlying the reservoir port.
Patient history
This patient's spasticity manifested as spastic quadriparesis without significant dystonia. The spasticity had been managed over several years with physical therapy, bracing and splinting, oral baclofen, and botulinum toxin injections. He began receiving botulinum toxin injections to the bilateral lower extremities in late 2013, resulting in improved spasticity and reduced caregiver burden. As spasticity progressed, oral baclofen therapy was initiated in 2016 and titrated gradually to 70 mg daily by early 2024. At this dose, the patient developed dose-limiting side effects, primarily drowsiness.
Given persistent spasticity and a limited response to conservative interventions, the patient was screened for IT baclofen pump placement. Goals of care were defined in the context of the patient's disability and functional status, and it was determined that the patient would benefit from IT baclofen to improve comfort, reduce spasticity-related pain, prevent the development of contractures, and ease caregiver burden.
The patient was referred to pediatric neurosurgery for consideration of an IT baclofen trial. A trial dose of 50 mcg IT Gablofen was administered in July 2024, yielding a positive clinical response. Consequently, an IT baclofen pump was implanted in August 2024. Intraoperatively, the catheter was anchored to the back fascia, then tunneled to the abdomen, where it was connected to the pump. Before closure, the catheter was positioned behind the pump and secured to the surrounding fascia with both nylon and Vicryl sutures. The patient's oral baclofen regimen was gradually tapered, then discontinued entirely in the days after pump implantation.
After implantation, the initial infusion rate was set at 96 mcg/day. The patient was followed routinely in the outpatient pediatric rehabilitation clinic for dose titration and pump refills. Visit frequency was determined by the degree of spasticity, as measured by the Modified Ashworth Scale (MAS), in relation to the current baclofen dose and the remaining medication volume in the reservoir; however, follow-up generally occurred at intervals ranging from two weeks to two months. At each visit, the pump's position and contours were examined to confirm that it was secure and that no anatomical abnormalities were developing. Over the subsequent year, the pump was refilled once, in April 2025, without complication.
The patient's dose was titrated up to 259.3 mcg/day by August 2025. At that visit, the pump was appropriately in place without evidence of anatomic abnormalities on or around the device. One year post-implantation, the patient's hip abductor and flexor spasticity improved from MAS 3 to MAS 2. This resulted in meaningful functional gains, particularly by facilitating easier clothing and diaper changes for caregivers.
Outpatient evaluation & subsequent hospitalization
In September 2025, the patient presented to the pediatric rehabilitation clinic for a scheduled IT baclofen pump interrogation and refill. At that time, the patient's mother noted stability in the patient's spasticity and denied any withdrawal symptoms. On examination, a firm, non-tender, mobile mass was palpated between the skin and the pump, obscuring access to the central refill port. (Figure 1) When this was brought to the mother's attention, she stated the finding was new and that she had not noticed it herself. Point-of-care ultrasonography, performed due to the presence of this palpable irregularity, demonstrated a low-density structure overlying the refill port. (Figure 2)

Central mobile lump observed on physical exam.
Point of care ultrasound of mobile lump.
Neurosurgery was contacted and presented bedside for consultation. Based on both teams’ evaluations, the multidisciplinary team suspected that the catheter had migrated anteriorly and possibly calcified over the reservoir refill port. Given the risk of catheter puncture, the decision was made to defer the refill procedure. At that time, approximately 0.2 mL of baclofen remained in the reservoir. The patient was scheduled for urgent surgical exploration, with intraoperative refill planned.
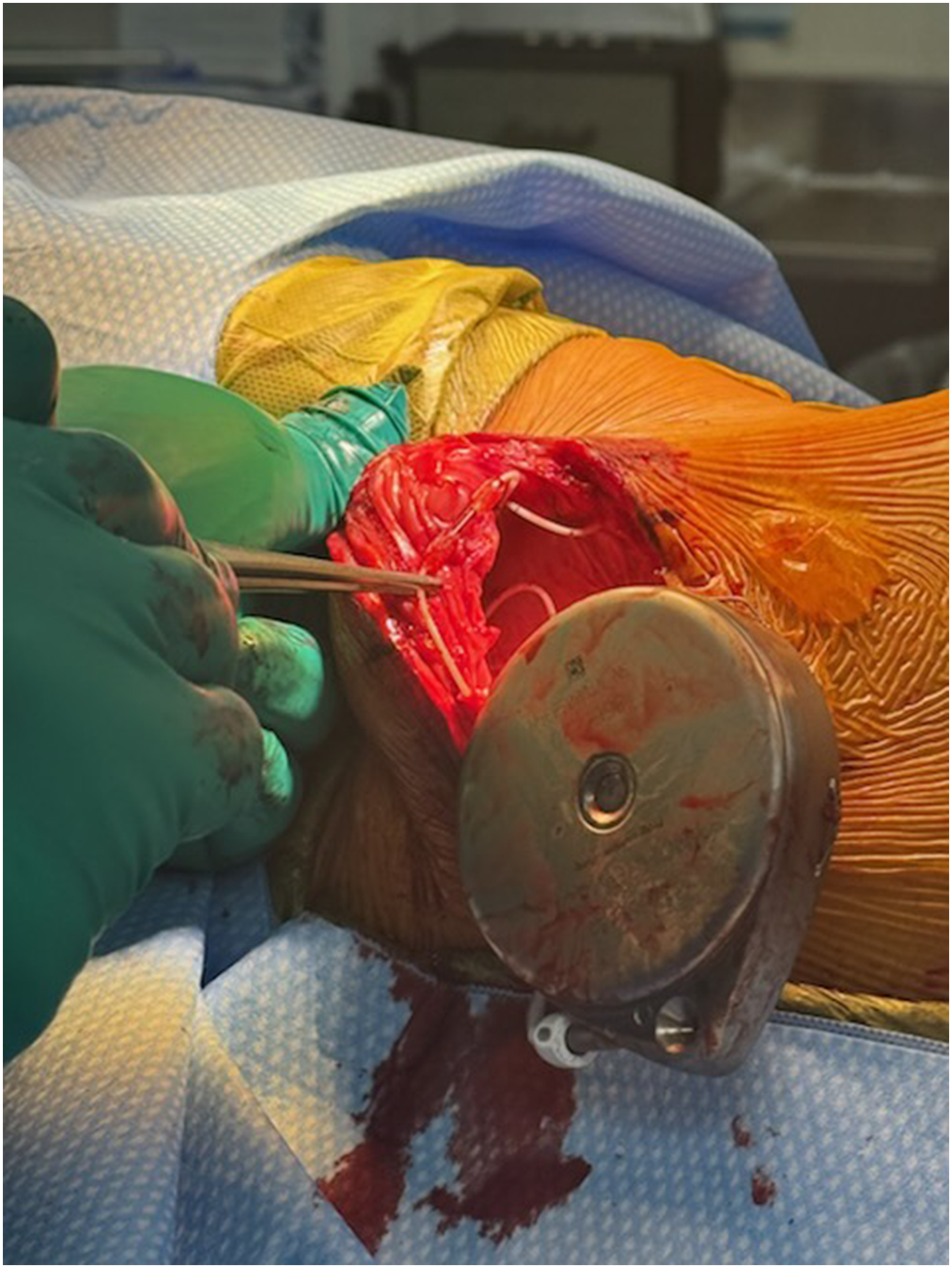
The patient was admitted under neurosurgery several days later. The previous abdominal incision was reopened to access the pump. The proximal end of the catheter was visualized ventral to the pump, and the tubing had calcified in front of the reservoir port. (Figure 3) The catheter was repositioned dorsally and secured behind the pump. (Figure 4) No tissue sample was taken from the calcified tubing for pathological analysis. Successful aspiration of cerebrospinal fluid confirmed catheter integrity. The residual baclofen was removed, and the pump was refilled with 20 mL of baclofen. The patient tolerated the procedure well, with no intraoperative complications.

Intra-operative picture of baclofen pump. Catheter tubing calcified at reservoir fill port.
Intra-operative picture of baclofen pump. Catheter repositioning.
Postoperatively, the pediatric rehabilitation team interrogated the pump in the hospital. The daily infusion rate was increased by 15% to 298.3 mcg/day. The patient's postoperative recovery was uneventful, and he was discharged with scheduled outpatient follow-up appointments with both neurosurgery and pediatric rehabilitation.
Post-hospitalization management
In early October 2025, the patient returned to the pediatric rehabilitation clinic for follow-up and baclofen pump interrogation. Physical examination demonstrated reduced spasticity in the bilateral lower extremities and improvement in ankle clonus following the recent dose increase. However, hamstring tightness persisted bilaterally with a MAS of 2 in both legs. The infusion rate was further increased by 5% to 313 mcg/day. A follow-up visit three weeks later, in late October 2025, demonstrated improvements in the patient's spasticity on the MAS, and the dose was maintained at 313 mcg/day.
Discussion
Appropriate monitoring of IT baclofen pumps requires routine follow-up with a spasticity specialist (often a pediatric rehabilitation physician) to ensure optimal medication delivery and patient safety. While interrogation, reprogramming, and refilling of the pump are well-established components of this process, thorough physical examination of the patient's spasticity and pump positioning is equally critical for assessing medication efficacy and minimizing the risk of complications. Even when physicians and patients adhere closely to treatment and safety protocols, issues with IT baclofen pumps can still arise, particularly catheter-associated complications.11–14
There are no clearly documented cases in the existing literature of a baclofen pump catheter migrating in front of the refill port and calcifying, thereby impeding a routine refill in a pediatric patient with CP. Several publications have described complications associated with baclofen pump catheters. Most reports indicate that the most common catheter-related issues involve catheter breakage, kinking, or occlusion.15–18 Extensive documentation also exists on catheter dislodgement, either at its proximal connection to the pump or at its distal end within the IT space.15–19 In rare cases, a displaced catheter may lead to the development of a granuloma at the distal catheter tip. 20 It is highly unusual for a catheter to migrate and adhere in front of the central port. Moreover, this complication developed rapidly, as the patient had an unchanged physical examination approximately one month earlier with no identifiable soft tissue abnormalities at pump site.
No clear cause for the catheter migration was identified in this case. At the September 2025 visit in which the anomaly was identified, the patient did not demonstrate any signs or symptoms of baclofen withdrawal (e.g., altered mentation from baseline, seizures, fevers, hypertonia/spasms, gastrointestinal symptoms) and the pump interrogation was unremarkable. The patient was not obese and had no notable change in body mass since the prior examination. He had no documented scoliosis and a negative scoliosis X-ray survey in April 2025, reducing the likelihood that anatomical changes in the abdominal cavity contributed to catheter migration. There was no history of physical trauma or any identifiable inciting event that could have caused the migration. Intraoperative assessment indicated that the pump itself was firmly in place, so the catheter migration was unlikely to be related to surgeon error. Thus, this patient's catheter migration was distinct both in the timeline and manner of presentation.
This case also highlights the importance of thorough physical examination and sound clinical judgment in safely refilling a baclofen pump. The care team identified a soft tissue abnormality that was partially adherent to the pump and recognized its potential to interfere with the refill process. Physical exam was key to identifying the problem, as the patient showed no signs of withdrawal in the history, suggesting continued IT delivery and making common catheter complications such as kinking, breakage, or occlusion less likely. Proceeding with the refill in an outpatient setting could have posed a considerable risk of catheter puncture, even with ultrasound guidance.
Conclusions
This case highlights the unique challenges associated with managing IT baclofen pumps in pediatric patients with CP. Although extensive literature exists describing catheter-related complications and outlining protocols for managing postoperative issues, atypical catheter complications can still occur in unpredictable and idiosyncratic ways.
Cases like this demonstrate that dynamic imaging may help better assess atypical catheter-related complications, such as dislodgement and migration. Despite awareness of baclofen withdrawal symptoms and signs of catheter displacement, history-taking and physical examination may not reliably detect migration or prevent complications during refills.
Future reports should continue to document uncommon presentations of catheter-associated complications in IT baclofen pumps, such as the one described here. Detailing management strategies for these atypical cases can help guide other providers in safely and effectively addressing similar challenges. As more of these cases are published, patterns may begin to emerge, recasting once rare complications into better understood aspects of IT baclofen pump management.
Footnotes
Ethical approval/informed consent
Our institution does not require ethical approval for reporting individual cases or case series, as long as patient information is de-identified. The following article was written using only de-identified patient information to protect the privacy of the patient.
Author contributions
Alex Landau MD (Corresponding Author): clinical care, writing, editing.
Kevin Batti, MD (Co-Author): writing, editing.
Tejas Shah, DO (Co-Author): writing, editing.
Andrew Kobets, MD (Attending): clinical care.
Yuxi Chen, MD (Attending): clinical care, article guidance, supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
This article is a case report and has no data to share.