
Abstract
Background
Clinical manifestations of the post-acute sequelae of SARS-CoV-2, or long COVID, have been well-described. However, few pediatric studies explore the impact on everyday function. The objective was to describe functional outcomes for children and youth with long COVID.
Methods
A retrospective cohort study of individuals < 21 years of age with COVID-19 infection seeking care at 21 children's hospitals across the United States was conducted. Using a systematic chart review, children with confirmed long COVID were identified by clinician adjudication between March 2020 and December 2022. Outcomes were compared to children with COVID-19 infection without confirmed long COVID. Functional impairments included difficulty participating in school and extracurricular activities, new referrals to rehabilitative therapies, newly modified education plans, and new or worsening mental health symptoms. Descriptive statistics and logistic regression were used to evaluate these outcomes among children with and without long COVID.
Results
Among 686 children with completed chart review, 651 (95%) had a COVID-19 diagnosis. Functional impairment was documented in 139 (21%) children, of which 59 had clinician-adjudicated long COVID. Compared to infected children without long COVID, children with long COVID had higher odds of school decline (OR 3.5, 95% CI 1.6–7.9, p = 0.002), school support (OR 2.4, 95% CI 1.2–5.0, p = 0.014), and new or worsening behavioral or mental health symptoms (OR 4.6, 95% CI 2.1–9.2, p < 0.001).
Conclusions
Significant functional impairments exist among children and youth following SARS-CoV-2 infection and serve as a reminder to clinicians evaluating children with long COVID to explore everyday function. Future prospective studies with longer follow-up are underway.
Keywords
Introduction
The short-term and long-term effects of COVID-19 continue to have a significant impact globally. The term post-acute sequelae of SARS-CoV-2 (PASC) refers to ongoing, relapsing, or new symptoms or other health effects occurring after the acute phase of SARS-CoV-2 infection, that are present for four or more weeks. 1 PASC is also referred to as long COVID. Although limited, the literature on functional outcomes following COVID-19 infection reports poor quality of life2,3; persistent symptoms affecting daily function 3 ; and impaired attention, executive functioning or occupational performance, 4 with up to 40% of patients reporting psychiatric symptoms. 5 The symptom trajectory is yet to be defined, with some studies signaling a lack of resolution or improvement.6,7
While data are accruing on long COVID manifestations in children, 8 there are few published studies exploring the impact persistent symptoms on everyday function and quality of life in children and adolescents. One retrospective cohort study focused on children with multisystem inflammatory syndrome in children (MIS-C) and found little organ-specific sequelae at a six-month follow-up, but persistent physical mobility and mental health support needs. 9 In another study regarding children with long COVID, nearly all participants (96.6%) reported persistent exertional dyspnea, cough, an impaired six-minute walk test, and exercise intolerance despite having normal pulmonary function testing, suggesting ongoing functional limitations. 10 Additionally, a retrospective study of children in a multidisciplinary clinic for long COVID found overall elevated cognitive disengagement syndrome, with anxiety emerging as the primary predictor of functional impairment after accounting for mood and anxiety symptoms. 11 Emerging evidence suggests that a subset of youth experience ongoing cognitive, emotional, and behavioral difficulties that may interfere with academic performance, emotional regulation, and daily functioning. 12
To fully explore the impact of long COVID, it is essential to assess functional outcomes with shorter-term domains of mental status, communication, motor and sensory functioning, feeding, and respiratory status. Longer-term domains of cognition, school performance, the ability to perform daily routines, relationships, and sleep or mood status are also important. 13 Therefore, the objectives of this study were to describe functional outcomes in children with long COVID in a large electronic health record (EHR)-based cohort, including the ability to participate in school and after-school activities, need for therapies, initiation or changes to existing education plans, or new or worsening behavioral or mental health diagnoses.
Methods
Data source
A retrospective cohort study was conducted using the pediatric EHR cohort of the National Institutes of Health (NIH) Researching COVID to Enhance Recovery (RECOVER) Initiative, which aims to understand, treat, and prevent long COVID. 1 The pediatric RECOVER EHR network spans 40 health systems across the United States, of which 21 were included in the study. The primary object of this analysis was to examine overall associations across a large, heterogenous pediatric cohort. The study was conducted in accordance with ethical standards and was approved by the Institutional Review Board. A waiver of consent and HIPAA authorization was granted due to the retrospective nature of the study.
Study population
To be included in the cohort, children and youth had to meet the following criteria: 1) SARS-CoV-2 infection confirmed via clinical diagnosis or polymerase chain reaction (PCR), antigen, or qualifying serology test between March 2020 and December 2022; 2) age less than 21 years at first COVID-19 infection; and 3) at least two encounters within the healthcare system (at least one in-person or telehealth) during the post-acute phase (28–179 days following infection). 14 Each patient's initial infection date was either the date of diagnosis or the date of the positive PCR or antigen test. For patients with a positive serology test or diagnosis indicating a history of or complication related to COVID-19, a proxy date 28 days prior to the test or diagnosis was used to represent the date of initial infection.
Next, a computable phenotype was applied as previously described to identify patients with evidence of long COVID using a set of rules that rely on long COVID diagnoses and symptom clusters determined to be more common in patients following COVID-19 infection. 15 Patients were identified as having conclusive evidence of long COVID if they had at least two long COVID diagnoses (ICD-10-CM code U09.9), MIS-C diagnoses (ICD-10-CM code M35.81), or post-viral sequelae diagnoses of specified infectious and parasitic diseases separated by at least 28 days. Patients were identified as having probable evidence of long COVID if they had a single long COVID or MIS-C diagnosis, at least two diagnoses in the same cluster condition separated by at least 28 days, or at least one post-viral sequelae diagnosis with a positive PCR test. Patients were classified as having possible long COVID if they had a single post-viral sequela diagnosis without a positive PCR test. Patients without such diagnoses were classified as having no evidence of long COVID. Those with conclusive, probable, or possible evidence were grouped as having long COVID by the phenotype, while all others were classified as having no evidence of long COVID.
Next, subsets of patients with and without evidence of long COVID as determined by the computable phenotype were sampled for systematic chart review. Twenty-two patients with evidence of long COVID were selected from each of the 21 sites and matched 1:1 with patients with no evidence of long COVID on site, age at COVID-19 infection, calendar quarter of infection, and hospitalization status. In total, 351 patients with evidence of long COVID and 351 patients with no evidence of long COVID were sampled. Research teams from each institution completed structured comprehensive reviews of patient charts using REDCap. 16 Performance of the rules-based computable phenotype was assessed, and mental health, behavioral conditions, and functional outcomes after the initial COVID-19 infection were evaluated. The details are provided in the Supplemental Material. The reviews included the domains of sociodemographic and clinical characteristics, symptoms related to long COVID, mental health and behavioral conditions, and functional impairments four weeks to six months after the initial COVID-19 infection.
Clinicians then completed a secondary review and provided their clinical adjudication as to whether the patient likely had long COVID. First, they were asked if the patient had long COVID based on the NIH definition: signs, symptoms, and conditions that continue or develop after initial SARS-CoV-2 infection and are present for 28 days or longer after the initial phase of infection. These signals may be multisystemic and may present with a relapsing, remitting pattern and progression or worsening over time, with the possibility of severe and life-threatening events even months or years after infection. 1 Next, they were asked whether the patient had long COVID based on the computable phenotype rules. The answers to these questions were used to determine whether a patient had clinician-adjudicated long COVID. The comparison group comprised children without clinician-adjudicated long COVID.
Evaluation of functional impairments
Functional impairments included information about school and extracurricular activities, referrals for services, specialized education plans, and behavioral and mental health outcomes included in clinician documentation. Reviewers were first asked if the child missed school or extracurriculars or reported difficulties in school following COVID-19 infection. If the reviewer indicated that the child had any of these, they were identified as having school difficulties. They were then asked if the child had a modified school program (i.e., individualized education plan [IEP] or 504 plan) or referral for services (i.e., occupational therapy, physical therapy, speech and language pathology, or neuropsychological testing). For those questions, the reviewer was asked whether the child had a modified program or referrals prior to or after COVID-19 infection and whether the level of support increased or decreased post-infection. Children with new or modified support post-COVID-19 infection were identified as needing school support. Reviewers also evaluated new psychiatric or behavioral conditions experienced prior to and after the patient's COVID-19 infection. They were asked if the child had any new or worsening diagnoses (e.g., anxiety, depression, attention deficit hyperactivity disorder). Broad functional impairment variables included in analyses were school difficulty, school support and referrals for services, referrals for psychological services, and mental or behavioral health concerns. Additional details regarding these outcomes are provided in the Supplemental Material. Additional variables abstracted from the chart review for cohort description included sociodemographic characteristics, presence of a chronic condition, microbiologic evidence of SARS-CoV-2 infection, and vaccination status.
Statistical methods
Descriptive statistics were used to compare demographic and clinical features of the sample of children included in the chart review and the subgroup of children with documented functional impairment. Continuous variables were reported as medians and interquartile ranges (IQRs) and categorical variables as frequencies and percentages. Using logistic regression, the demographic and clinical features of children with evidence of COVID-19 and documented functional impairments were compared to the subsample of children with evidence of COVID-19 but no documented functional impairments. The subsample of children with evidence of COVID-19 and functional impairments was then further divided into patients with and without clinician-adjudicated long COVID. Demographic and clinical features of children with and without clinician-adjudicated long COVID were compared using logistic regression. In all logistic regressions, each demographic variable of interest served as the independent variable while the presence of a functional impairment served as the dependent variable.
Next, functional impairments of children with and without clinician-adjudicated long COVID were compared using logistic regression. In each model, long COVID was the independent variable, each broad functional impairment domain (i.e., school difficulty, school support or referrals, referral for psychological services, behavioral or mental health impairments) was the dependent variable, and age and sex were covariates. Results of all regression models were reported as odds ratios (ORs) and 95% confidence intervals (CIs). All analyses were conducted using R version 4.4.0 (Boston, MA).
Finally, functional impairments identified from unstructured health records were compared with corresponding ICD-10 diagnostic codes assigned in the structured EHR.
Results
Among 686 children with completed chart abstractions, 651 (95%) had documented COVID-19 infection. Of these, 139 (21%) children had a functional impairment noted (Supplemental Figure 1). Characteristics of the cohort with functional impairments compared to the cohort without functional impairments are summarized in Supplemental Table 1. The median age of children in the cohort with a functional impairment was 13.3 years (IQR 7.9–16.1), and 56% were female. School-aged children over five years old (OR 2.9 [95% CI 1.6–5.4]) and adolescents under 21 years old (OR 3.6 [95% CI 2.1–6.2]) had higher odds of functional impairment compared to children under five years of age.
Most children with a functional impairment were White, non-Hispanic (56%). Forty-eight percent had private insurance, 49% had a non-complex underlying condition, 49% received at least one dose of the COVID-19 vaccine, and 10% had an MIS-C diagnosis. Children with a chronic health condition had higher odds of having functional impairment than children without a chronic health condition (OR 1.9 [95% CI 1.2–3.0]). There were no significant differences between the cohort with functional impairments compared to the cohort without functional impairments with regards to sex, race, insurance, and variant period.
Patients with functional impairment comprised the main study cohort. Characteristics of the children with clinician-adjudicated long COVID and children without clinician-adjudicated long COVID are presented in Table 1. Fifty-nine children (42%) in the cohort with functional impairments were determined to have clinician-adjudicated long COVID. There were no significant differences between children with and without clinician-adjudicated long COVID with regards to age, sex, race, ethnicity, insurance, variant period, or vaccination status. Children with clinician-adjudicated long COVID were more likely to have a history of medical complexity.
Sociodemographic and clinical characteristics of the cohorts with and without clinician adjudicated long COVID.
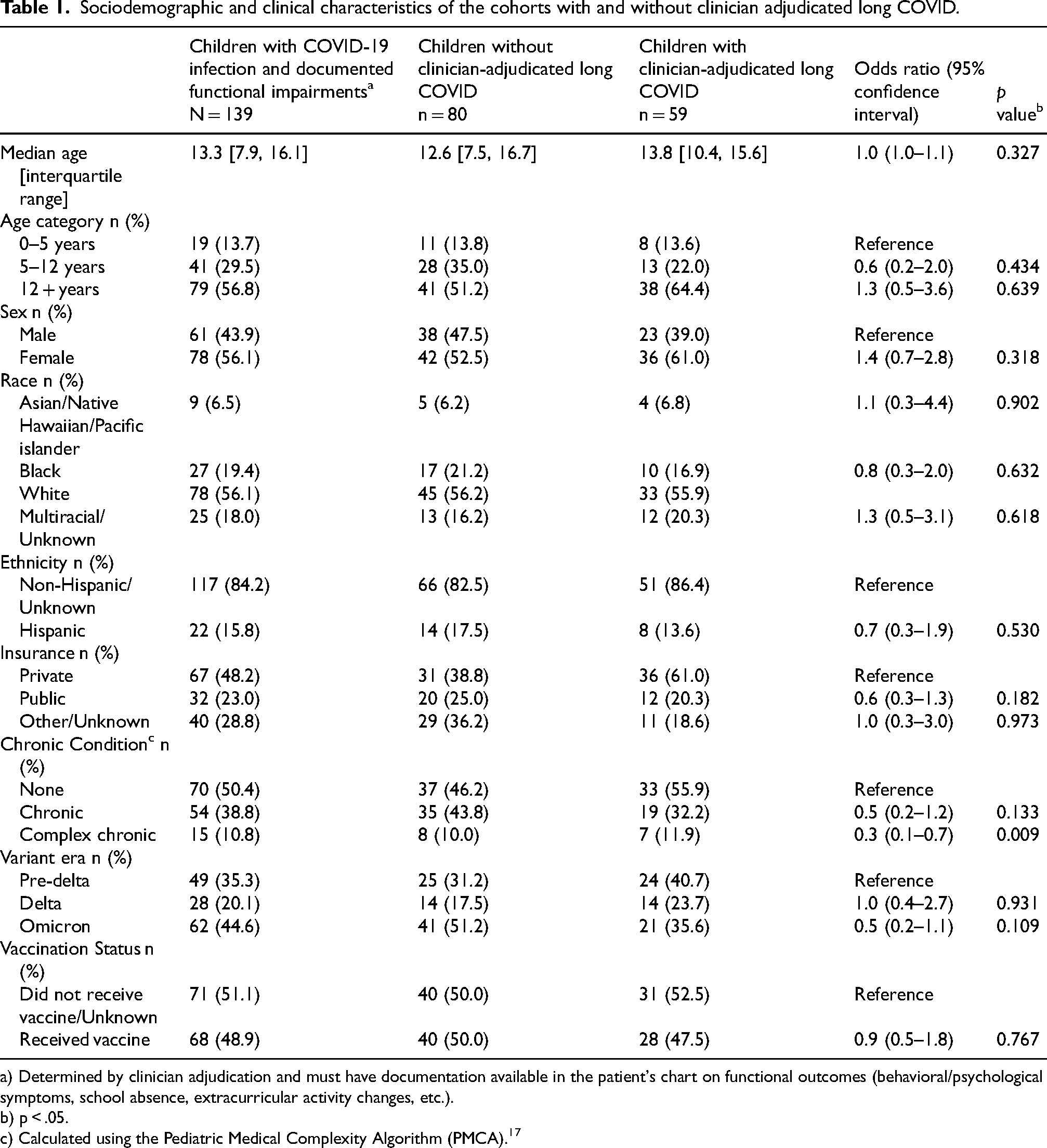
a) Determined by clinician adjudication and must have documentation available in the patient's chart on functional outcomes (behavioral/psychological symptoms, school absence, extracurricular activity changes, etc.).
b) p < .05.
c) Calculated using the Pediatric Medical Complexity Algorithm (PMCA). 17
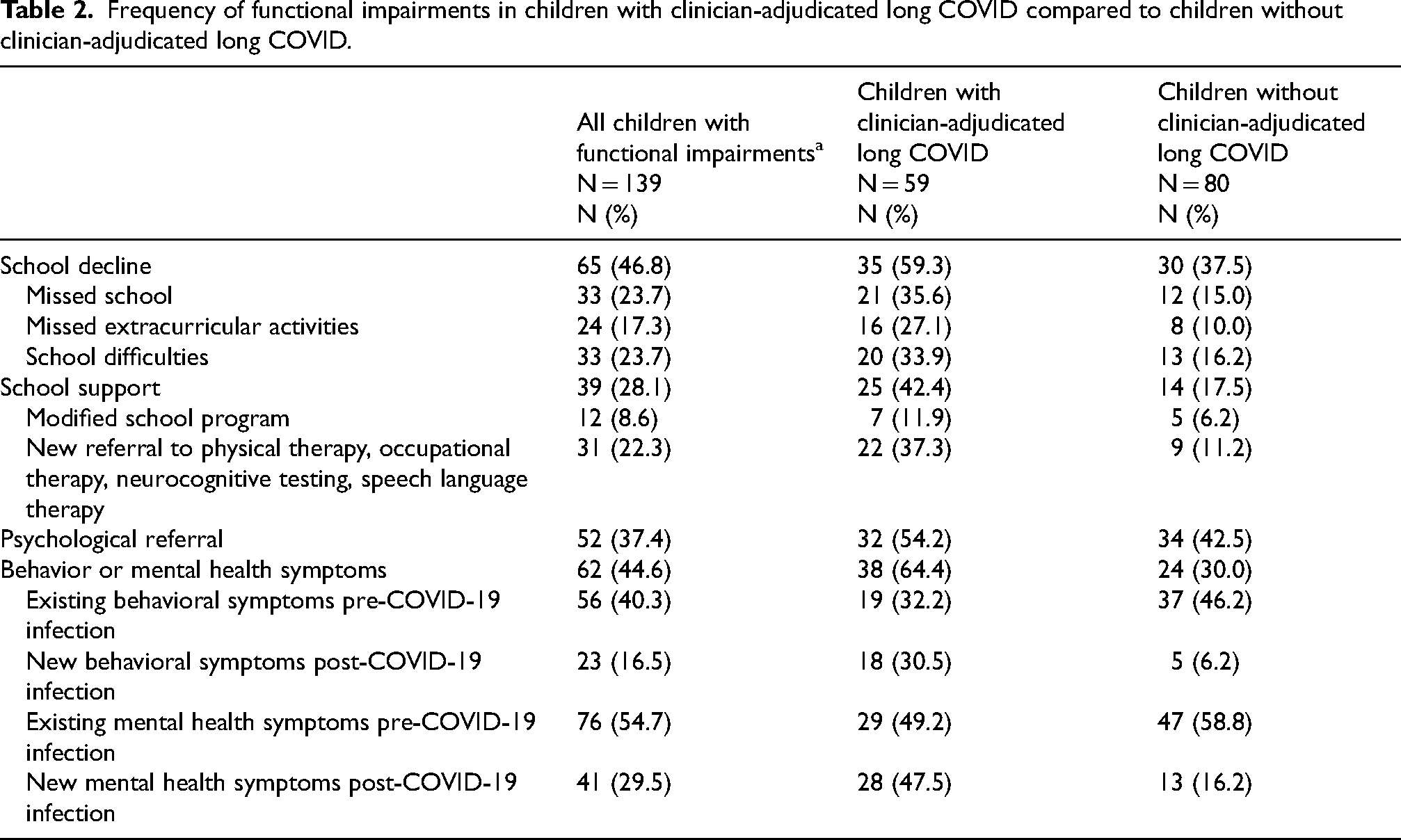
The frequency of functional impairments in each broad and specific domain is summarized in Table 2. Among children with functional impairments, those with clinician-adjudicated long COVID were more commonly reported to miss school (35.6% vs 15.0%) and extracurricular activities (27.1% vs 10.0%), exhibit school difficulties (33.9% vs 16.2%), and experience new behavioral symptoms and mental health diagnoses (30.5% vs 6.2%) compared with those without clinician-adjudicated long COVID. In logistic regression analyses, children with clinician-adjudicated long COVID were associated with increased odds of receiving school support (OR 2.4 [95% CI 1.2–5.0]), school decline (OR 3.5 [95% CI 1.6–7.9]), and behavior or mental health symptoms (OR 4.6 [95% CI 2.1–9.2]). Children with and without clinician-adjudicated long COVID had similar odds of receiving a referral for psychological or behavioral services (OR 1.2 [95% CI 0.6–2.4]). Excerpts from the EHR notes and clinician evaluation describing these functional limitations are provided in Supplemental Table 2.
Frequency of functional impairments in children with clinician-adjudicated long COVID compared to children without clinician-adjudicated long COVID.
Most patients in whom functional impairments were identified through chart review did not receive ICD-10 diagnostic codes for behavioral outcomes or school difficulties; only 6% of children with documented school difficulties or behavioral outcomes had an appropriate ICD-10 code assigned for the healthcare visit (Supplemental Table 3).
Discussion
In this retrospective cohort study of children with evidence of COVID-19 across 21 centers in the United States, functional impairments were examined in the broad domains of school decline, school support, psychological referrals, and behavioral and mental health symptoms using manual chart review (Figure 1). Of the full sample of children, approximately one fourth of patients had a documented functional impairment. Higher rates of school difficulties, school support or referrals to therapies, and new behavioral or mental health conditions were found in children with adjudicated long COVID, compared to those without clinician-adjudicated long COVID. This cohort is among the first to evaluate functional impairments in children with long COVID, highlighting the importance of collecting data to help evaluate the impact of illness, healthcare, and resource needs to support everyday functioning and recovery.
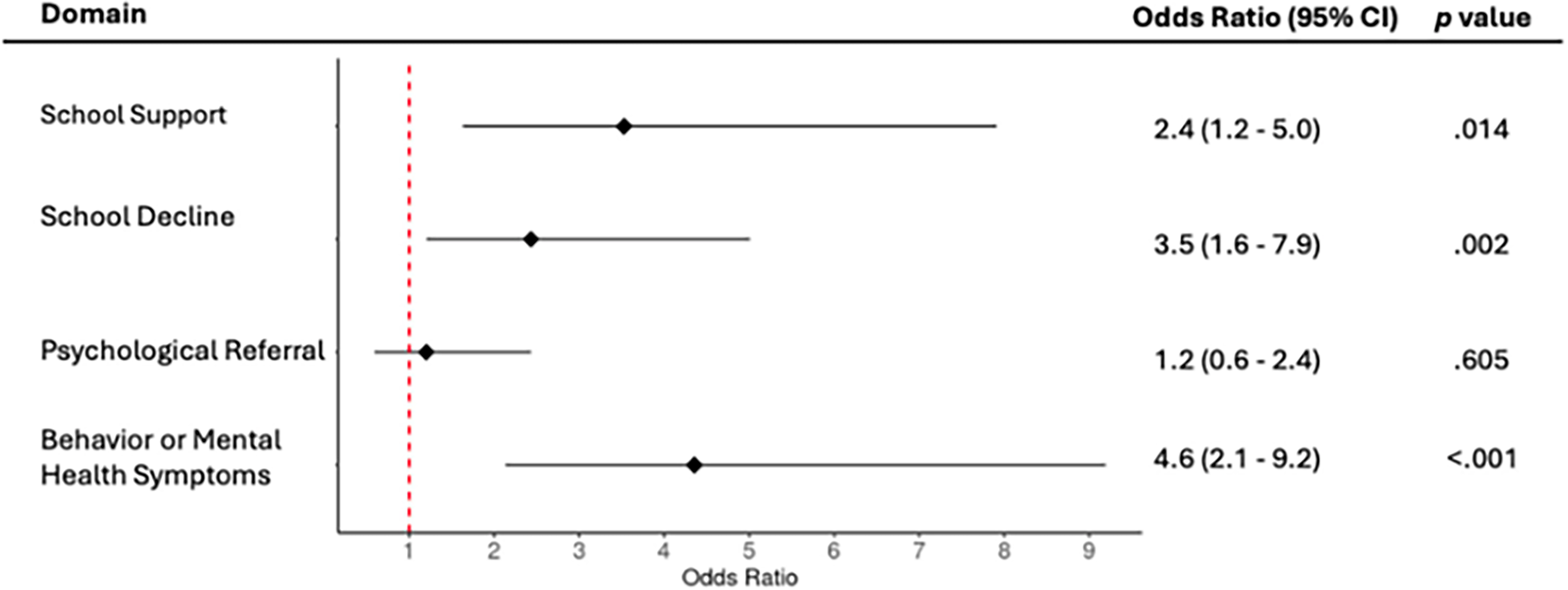
Forest plot of odds ratios and 95% confidence intervals (cis) comparing functional impairments in broad domains for children with and without clinician adjudicated long COVID.
A higher frequency of functional impairments was observed among adolescents compared to children under five years, during earlier versus later phases of the pandemic, and among children with underlying comorbidities compared to children without comorbidities. While differences were more pronounced among children with clear evidence of long COVID, there is likely a spectrum of illness manifestations which impacts children's everyday functioning following COVID-19 infection. Of note, the relatively small sample size did not allow for a definition of long-term impairments in patients with MIS-C, which may present distinct outcome patterns and remains included in the sample.
Importantly, children with clinician-adjudicated long COVID had higher odds of school decline, school support, and new or worsened behavior or mental health symptoms, including anxiety and depression. Considering the impact of social restrictions on youth mental health 18 and the often lengthy delay between onset of mental health or behavioral symptoms and formal identification by the school and healthcare systems, 19 higher rates of new and worsening mental health conditions and behavioral changes in youth with long COVID were observed within six months of infection. Higher rates of school-related impairments and referrals for psychological or behavioral services within IEPs were observed. The process from impact on school attendance and performance to evaluation to formal referral and finally engagement with psychological or behavioral services can take months to years, with less than half of children with mental health conditions receiving treatment.19–21 However, these ascertainment-related factors would be expected to bias the results toward a null finding rather than the positive findings observed. Additionally, those with clinician-adjudicated long COVID had higher rates of anxiety and depression, which may contribute or co-occur with functional impairment and school difficulty, warranting future studies to fully understand the impact.
Many of the reports identified by chart review (see Supplemental Table 2) indicate concentration and memory problems, which are in line with other studies that have found objective evidence of impairment in sustained attention, working memory, and inhibition following COVID-19 in adults. 5 Such cognitive impairments in youth would be expected to manifest as behavioral and school problems, particularly in younger children who have less developed meta cognition and ability to verbally report their thoughts. Therefore, there may have been an underreporting of functional impairments in children under five years, who may not yet be enrolled in school, who may not self-report symptoms comprehensively, and whose challenges at preschool and elsewhere may be under-recognized or may take time to be reported. Studying functional outcomes is challenging in children given the need to span developmental stages and the lack of a standardized tool specific to pediatric long COVID, such as those which exist for adults. 22 Clinicians must adapt their assessments to accommodate diverse developmental stages, cognitive abilities, and communication skills, which ideally require validated tools tailored to specific ages and abilities.
Strengths of this study include a wide geographic representation of centers across the US, as well as the use of a computable phenotype to initially identify children with PASC among those with COVID infection, given the unreliability and underutilization of long COVID diagnosis codes, followed by two-step chart reviews with clinician adjudication to confirm long COVID. The cohort was assembled from 21 different health systems, each of which may differ in clinical practice patterns, patient populations, and implementation processes. As health system-level variation was not modeled in this analysis, unmeasured inter-system differences may have contributed to residual heterogeneity. However, the study was designed as an exploratory, hypothesis-generating analysis given the relative novelty of the research question. Future studies with larger sample sizes and more granular data should evaluate health system-specific effects to better clarify how local practice environments influence outcomes. Next, extensive chart reviews were conducted to identify evidence of functional outcomes from medical notes, given that relevant outcomes are rarely available in structured data. In fact, only 6% of children with school difficulties or behavioral outcomes had the appropriate ICD-10 code designated for the healthcare visit in this cohort, since it is not a standard coding practice. The International Classification of Functioning, Disability and Health (ICF) is the system recommended for functional outcomes coding in the EHR, rather than ICD coding. 23
There are several limitations of this study which warrant discussion. The approach for cohort identification may have led to missed cases, especially later in the pandemic when home testing was widespread, earlier in the pandemic when access to molecular testing was limited, and in areas with decreased access to PCR testing for children. Additionally, the study focused on the post-acute period, specifically from 28 days to six months following infection. Extending the evaluation period beyond six months could be beneficial, as some patients in the sample may have experienced functional impairments that emerged after this timeframe. Additionally, attribution of long COVID is challenging given its overlap with other disease states. An ideal comparison group would be children without a SARS-CoV-2 infection with information regarding functional status; however, such a sample was not available. Instead, outcomes were compared with a group of children without evidence of long COVID with functional outcomes data, which further narrowed the sample size, and precluded more extensive covariate adjustment.
Next, while the health systems contributing to the cohort were geographically diverse, most children in the cohort sought care from large tertiary hospitals, which may bias the sample to more medically complex children. These children had more acute presentations of COVID and may overestimate the proportion of children with functional impairments. However, this approach enabled more patients with long COVID seeking subspecialty care, or care at long COVID clinics, to be captured. Utilizing EHR data may prevent adequate capture of vulnerable populations with challenges in accessing or receiving treatment. 24 Given the lack of focus on functional outcome evaluation during many clinical visits, the depth of data available was limited despite comprehensive chart review. Finally, because the univariate logistic regression analyses did not adjust for potential confounding variables, the observed associations should be interpreted cautiously. These findings reflect crude, descriptive relationships and may not represent independent effects once other variables are considered.
The findings also suggest that clinicians may benefit from focusing on school functioning, supporting appropriate accommodation requests, and considering early referral and collaboration with multidisciplinary teams to better support children with long COVID. Subsequent work from the RECOVER prospective cohort includes the evaluation of functional outcomes in pediatrics including mental and behavioral health outcomes using standardized patient-reported outcomes to standardize and improve reliability of the outcomes data across centers and raters. Sufficient follow up periods will also clarify long-term impacts of PASC on patients and their families.
Conclusion
The findings demonstrate evidence of functional impairments among children and youth following SARS-CoV-2 infection and serve as an important reminder to clinicians evaluating children with long COVID to explore its impact on everyday functioning.
Supplemental Material
sj-docx-1-prm-10.1177_18758894261460624 - Supplemental material for Functional outcomes of children after SARS-CoV-2 infection: An EHR-based cohort study
Supplemental material, sj-docx-1-prm-10.1177_18758894261460624 for Functional outcomes of children after SARS-CoV-2 infection: An EHR-based cohort study by Abigail Case, Morgan Botdorf, Nicole Marchesani, John E Leikauf, Rebecca Letts, Christine Maughan, Megan L Fitzgerald, Miranda Higginbotham, Aparna C Swaminathan, David Liebovitz, Deepika Thacker, Dima Dandachi, Jennifer A Muszynski, Kari Wellnitz, Nathan M Pajor, Ravi Jhaveri, Sandy L Gonzalez and Suchitra Rao in Journal of Pediatric Rehabilitation Medicine
Footnotes
Acknowledgments
This study is part of the NIH RECOVER Initiative, which seeks to understand, treat, and prevent PASC. For more information on RECOVER, visit ![]() . We would like to thank the National Community Engagement Group (NCEG), all patient, caregiver and community representatives, and all the participants enrolled in the RECOVER Initiative as well as the chart abstractors from the participating PEDSnet and PCORnet sites. Additionally, we would like to thank Elizabeth Chrischilles, PhD (The University of Iowa; Principal Investigator), Abu Mosa PhD, MS, FAMIA (University of Missouri School of Medicine; Principal Investigator), and Ami Patel (Ann & Robert H. Lurie Children's Hospital of Chicago; Chart Reviewer) for their contributions in helping obtain the data for this work.
. We would like to thank the National Community Engagement Group (NCEG), all patient, caregiver and community representatives, and all the participants enrolled in the RECOVER Initiative as well as the chart abstractors from the participating PEDSnet and PCORnet sites. Additionally, we would like to thank Elizabeth Chrischilles, PhD (The University of Iowa; Principal Investigator), Abu Mosa PhD, MS, FAMIA (University of Missouri School of Medicine; Principal Investigator), and Ami Patel (Ann & Robert H. Lurie Children's Hospital of Chicago; Chart Reviewer) for their contributions in helping obtain the data for this work.
Ethics approval and consent to participate
The Institutional Review Board obtained approval under Biomedical Research Alliance of New York (BRANY) protocol #21–08–508, with waiver of consent and HIPAA authorization.
Authorship has been determined according to ICMJE recommendations.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the NIH Agreement OTA OT2HL161847-01 as part of the RECOVER program of research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Role of funder/sponsor
The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Disclaimer
This content is solely the responsibility of the authors and does not necessarily represent the official views of the RECOVER Initiative, the NIH, or other funders.
Article summary
This retrospective cohort study describes functional impairment in children and youth following SARS-CoV-2 infection, affecting ability to participate in everyday activities.
What's known on this subject
Evidence suggests long COVID impacts children's long-term health, but no studies have investigated functional status in these children and youth.
What this study adds
This study demonstrates limitations in everyday functioning of children and youth with long COVID, including school difficulties, need for new school support and referrals for rehabilitation and psychological services, as well as mental or behavioral health concerns.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.