
Abstract
Case Diagnosis
An 11-year-old male with medulloblastoma underwent gross total resection of a posterior fossa tumor, complicated by post-operative pediatric cerebellar mutism syndrome (ppCMS), exhibiting mutism, emotional dysregulation, impaired volitional movement initiation, and ataxia.
Case Description
While ppCMS's pathophysiology remains incompletely understood, prevailing hypotheses implicate cerebellothalamocortical dysregulation, functional diaschisis, and inhibitory-excitatory network imbalance. This case explores the use of lorazepam, a benzodiazepine that enhances GABA-A receptor activity, as a potential neuromodulator to facilitate recovery in ppCMS.
Setting
Tertiary care children's hospital.
Assessments/Results
Pharmacologic trials with bromocriptine, risperidone, and gabapentin yielded minimal benefit. However, administration of intranasal midazolam (5 mg) during radiation simulation resulted in transient resolution of mutism and improved initiation of movement. Based on this response, lorazepam (2 mg daily, 0.06 mg/kg) was initiated, leading to sustained improvements in speech, motor function, and therapy participation. Functional outcome assessments, including the WeeFIM, revealed a 40-unit gain within one week of lorazepam initiation compared to a 1-unit gain in the preceding week. Immediate regression was noted upon medication discontinuation and reintroduction resulted in subsequent recovery.
Discussion/Relevance
The differential response to benzodiazepines compared to other medications suggests potential for inhibitory-excitatory network imbalances. Future research should explore whether less sedating benzodiazepines, such as clobazam, or other GABAergic modulators could provide similar benefits without the cognitive side effects associated with lorazepam.
Conclusions
There is compelling evidence that benzodiazepine-mediated GABAergic modulation may facilitate CMS recovery by restoring cerebellothalamocortical network function. The observed improvements in motor initiation and speech fluency underscore the potential for pharmacologic neuromodulation as an adjunct to traditional rehabilitative therapies.
Abstract
An 11-year-old male with medulloblastoma underwent gross total resection of a posterior fossa tumor, complicated by ppCMS, exhibiting mutism, emotional dysregulation, impaired volitional movement initiation, and ataxia. Amid ongoing neurorehabilitation, a pharmacologic trial with lorazepam led to a reproducible improvement in speech and engagement. Though transient, the response suggested reversible disruption within functional circuits rather than fixed structural damage. This case report uncovers latent functional capacity in ppCMS, which can help distinguish ppCMS from other overlapping neurologic or psychiatric conditions throughout the course of rehabilitation.
Introduction
Post-operative pediatric cerebellar mutism syndrome (ppCMS) is a complication predominantly observed in children undergoing resection of posterior fossa tumors, particularly medulloblastomas. 1 Though first described by Rekate et al. in 1985 as cerebellar mutism following bilateral cerebellar injury, 2 subsequent studies have expanded the definition to encompass a broader and more heterogeneous clinical spectrum. 3 ppCMS is characterized by a triad of (1) mutism or impaired speech and language, (2) ataxia and hypotonia, and (3) emotional lability, irritability, and apathy. 4 The constellation of post-operative symptoms was defined as ppCMS. The term “posterior fossa syndrome” lacks anatomical and clinical specificity and has been formally retired by the international Posterior Fossa Society. In its place, ppCMS offers a more precise classification that acknowledges mutism as a severe manifestation of cerebellar cognitive affective syndrome (CCAS), reflecting disruption of speech planning circuits rather than merely motor or emotional sequelae. The reported incidence of ppCMS ranges widely from 7% to 50% in various study populations, 1 with considerable variability depending on tumor type, location, and surgical approach, although surgeries of tumors localized to the midline such as the vermis and fourth ventricle were more likely associated with ppCMS and poorer neuropsychological outcomes.5–7 Despite advances in neuroimaging and surgical techniques, there remains no established treatment and rehabilitation remains the mainstay of management. We present a successful therapeutic lorazepam trial for ppCMS highlighting key anatomical considerations, neuroimaging findings, and the implications for postoperative rehabilitation in ppCMS.
Early intervention included pharmacological management and structured rehabilitation, with lorazepam emerging as a key agent in facilitating speech and motor initiation. This case underscores the importance of early recognition and multidisciplinary intervention in mitigating the sequelae of ppCMS.
Case presentation
An 11-year-old male presented with vomiting, altered mental status, and difficulty ambulating. Neuroimaging demonstrated a posterior fossa mass with associated hydrocephalus. He underwent surgical resection of the mass with placement of an external ventricular drain followed by ventriculoperitoneal shunt placement. Pathology revealed medulloblastoma. A day after resection, he developed ppCMS, characterized by decreased arousal, delayed and reduced command following, irritability, mood lability, markedly decreased spontaneous initiation of movements (including eye opening and extremity movement), hemiparesis, urinary retention, dysphagia, and absent speech. After three days, he was admitted to a pediatric intensive inpatient rehabilitation program for these impairments.
Participation in therapy was initially limited by restlessness, irritability, combativeness, poor initiation of movement, and minimal verbal output. Pharmacologic interventions targeting these symptoms included gabapentin, risperidone, and bromocriptine, each trialed sequentially for symptom management. Gabapentin was initiated on February 5, 2024 and gradually titrated to 400 mg TID by February 20, 2024. Bromocriptine 2.5 mg daily was added on February 16, 2024. Midazolam was administered on February 22, 2024, risperidone was initiated on February 25, 2024, and lorazepam was initiated after the February 27, 2024 assessment. These medications were selected to address irritability, agitation, and impaired initiation, with clinical benefit anticipated over days to weeks; however, they produced limited observable functional or behavioral improvement. The patient was discharged from inpatient rehabilitation on March 8, 2024 on bromocriptine, gabapentin, lorazepam, and risperidone. During outpatient follow-up, bromocriptine was tapered beginning April 3, 2024 and discontinued on May 2, 2024 along with risperidone. Gabapentin was continued and subsequently weaned off by July 25, 2024. At most recent follow-up on February 13, 2025, the patient remained off all neuropsychiatric medications.
During radiation simulation, the patient received intranasal midazolam (5 mg) for procedural sedation. Following administration, he demonstrated transient but notable improvement in initiation of movement and verbal output. Given the short duration of effect and sedating properties of midazolam, a scheduled benzodiazepine trial was initiated to evaluate whether similar benefits could be achieved with sustained functional participation. He was started on lorazepam 2 mg daily (0.06 mg/kg). Following initiation, he demonstrated marked improvements in initiation and engagement, including improved tolerance of and participation in therapy sessions, reduced combativeness, increased ambulation distance with decreased assistance, and increased verbal output characterized by longer sentences and greater spontaneous speech.
The following paragraph summarizes the medication trials undertaken throughout the patient's treatment course. To assess whether these improvements reflected medication effect rather than natural neurologic recovery, lorazepam was held after five days of therapy. On the day it was not administered, he demonstrated clear functional regression, including decreased spontaneous movement, increased assistance required for ambulation, reduced oral intake, diminished verbal output, and delayed responses to commands. No concurrent medical changes, intercurrent illness, therapy interruptions, or other medication adjustments were identified to account for this decline. Lorazepam was restarted the following day, with subsequent re-emergence of functional and behavioral gains. Given the positive response to daily dosing, the frequency was not increased.
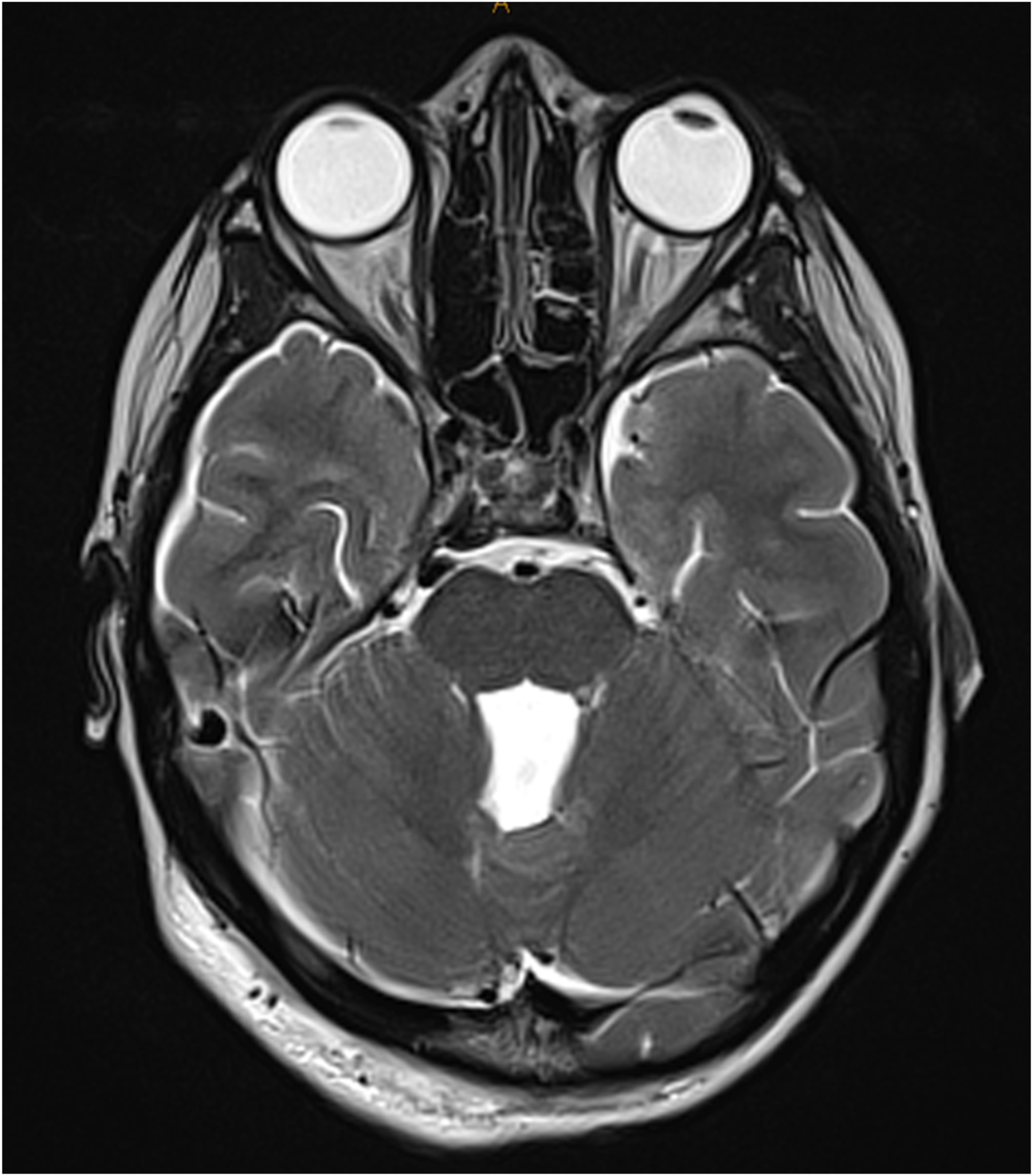
The following paragraph revisits an earlier phase of treatment to provide a detailed account of the lorazepam trial. The patient participated in 19 days of intensive inpatient rehabilitation, with functional progress assessed weekly using the WeeFIM instrument. During the first week of admission (2/20/24–2/27/24), prior to lorazepam initiation, he demonstrated minimal functional improvement, with a gain of only 1 WeeFIM unit (bathing). Lorazepam was initiated after the 2/27/24 assessment. After one week of lorazepam therapy, his WeeFIM score increased by 40 units, with improvements across mobility, self-care, communication, and cognition domains. WeeFIM scores by domain and timepoint are shown in Figure 1, demonstrating substantial functional gains temporally associated with lorazepam therapy. Changes in WeeFIM scores over time are graphed in Figure 2. A timeline of lorazepam administration and associated clinical changes are presented in Figure 3. Image 1 and Image 2 show a mass in the posterior fossa. Postoperative MRI findings are shown in Image 3 and Image 4.
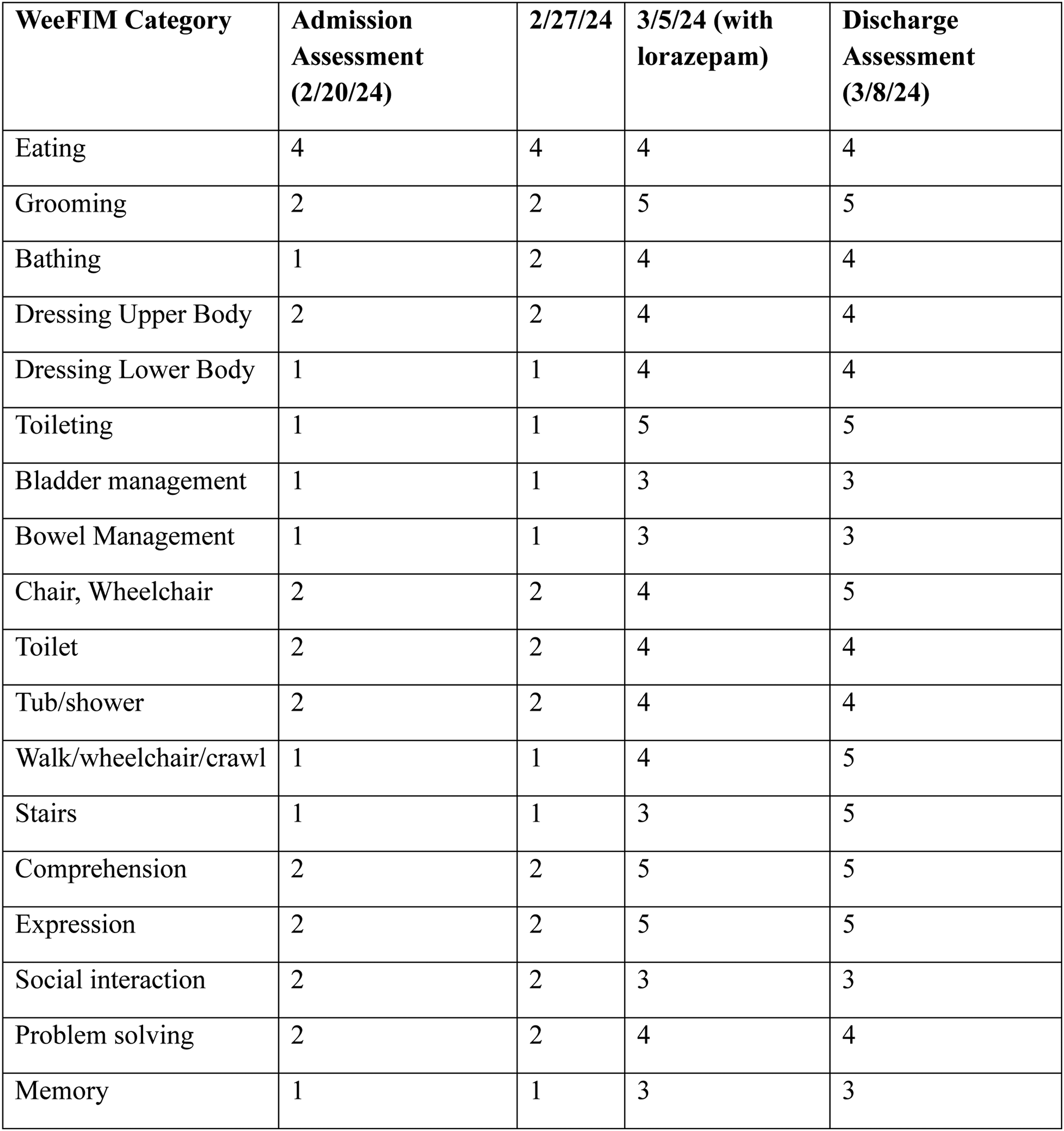
WeeFIM functional score changes before and after lorazepam initiation.
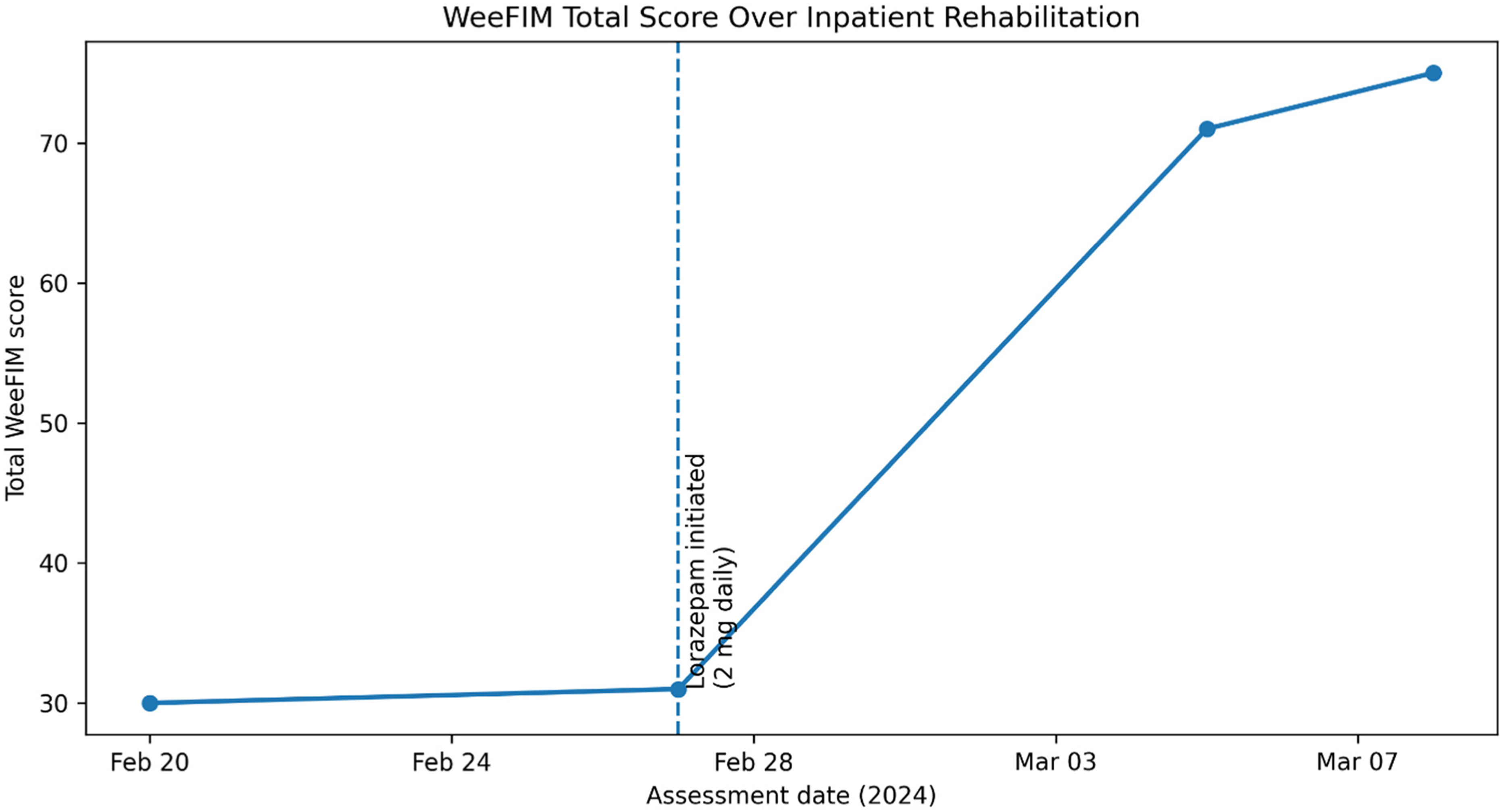
Weekly WeeFIM scores during inpatient rehabilitation demonstrating minimal functional change prior to lorazepam initiation and a marked increase in total WeeFIM score following initiation. Lorazepam was started after the 2/27/24 assessment, after which a 40-point gain was observed over one week, with improvements across self-care, mobility, communication, and cognitive domains.
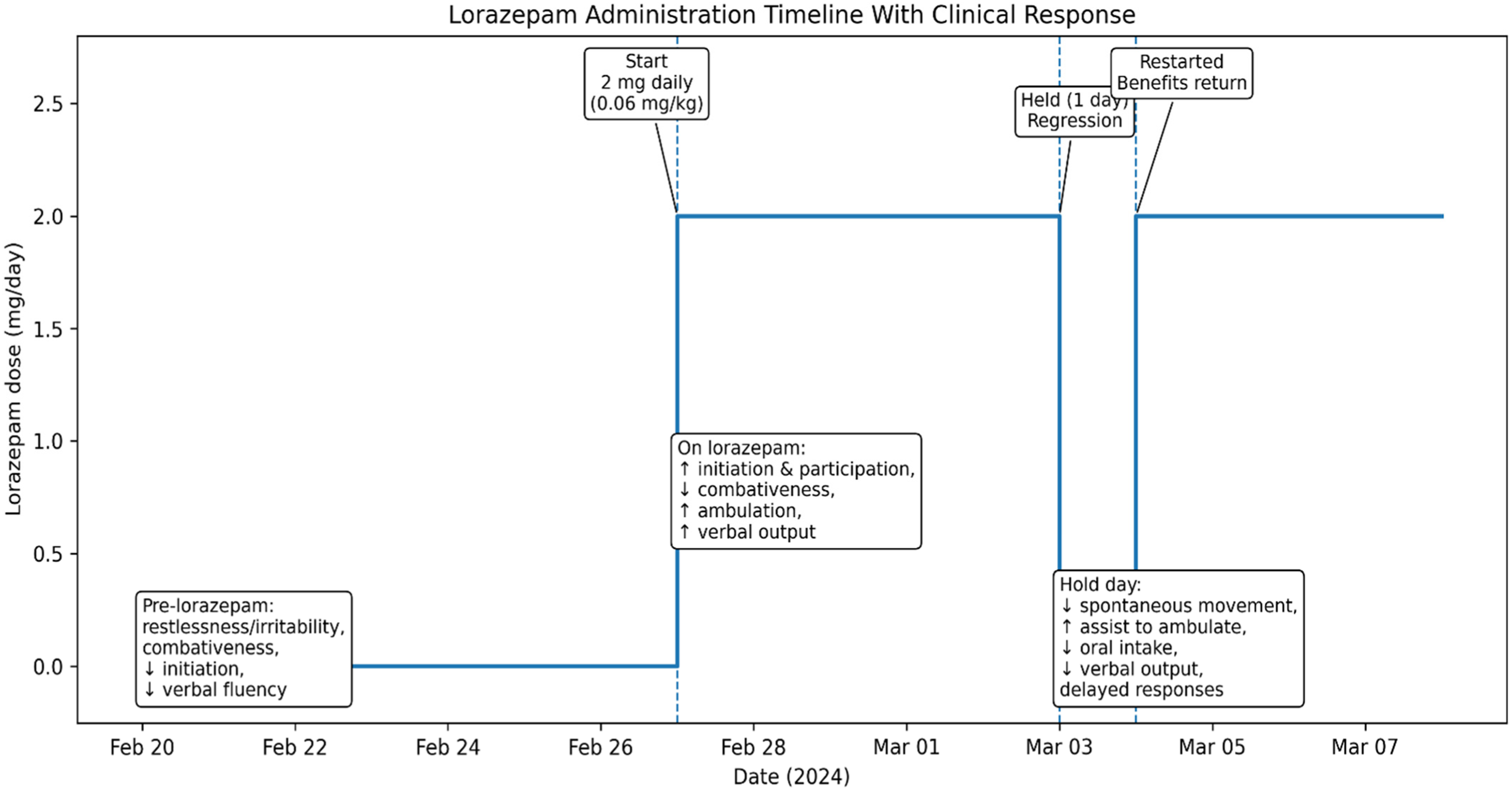
Timeline demonstrating initiation, temporary discontinuation, and resumption of lorazepam therapy with corresponding clinical response. Lorazepam was initiated at 2 mg daily (0.06 mg/kg) following limited response to other pharmacologic interventions. Functional and behavioral improvements were observed during therapy, with notable regression on the day lorazepam was held and re-emergence of benefit following resumption.
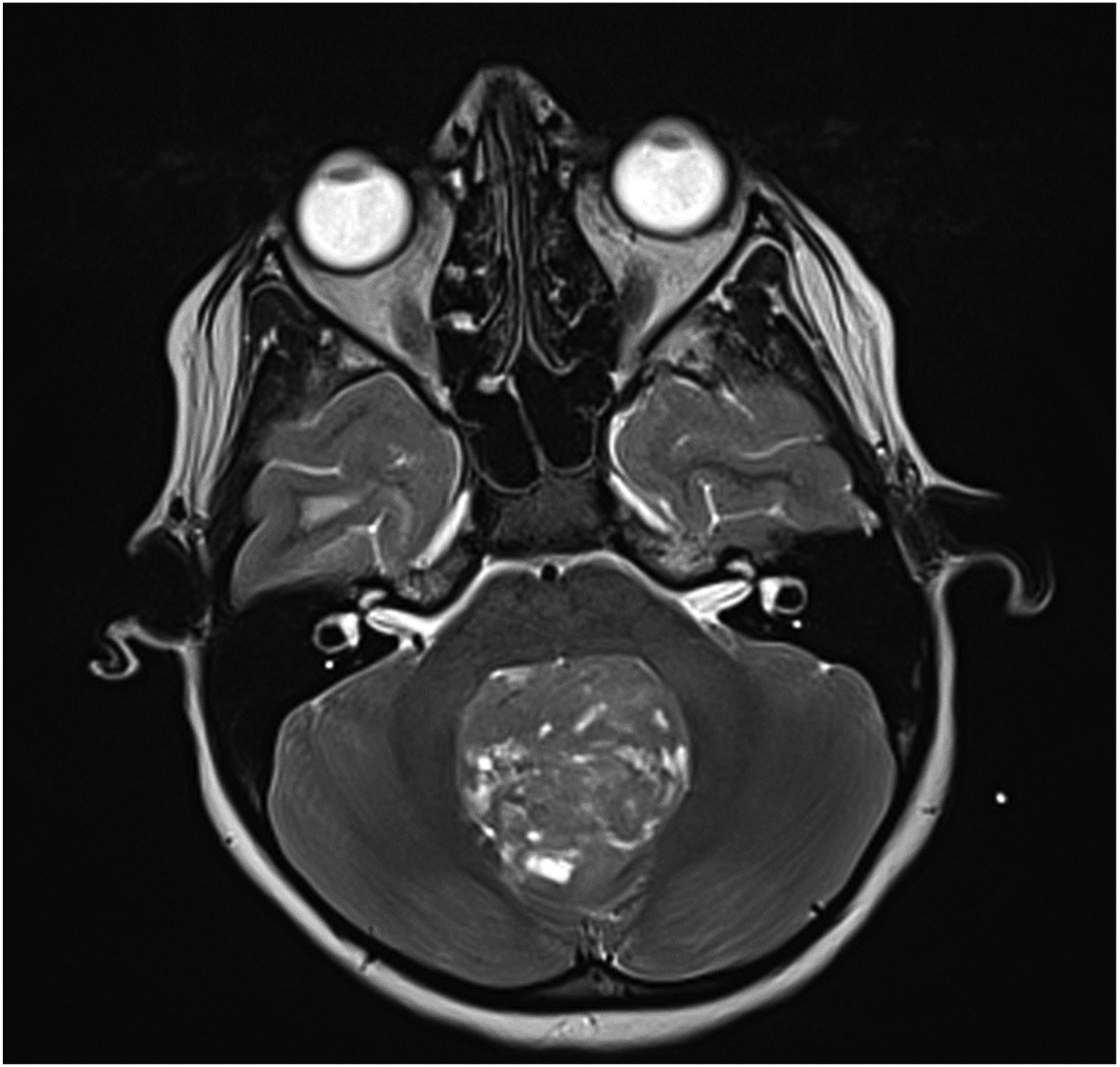
January 20, 2024 MRI T2 weighted Axial View.
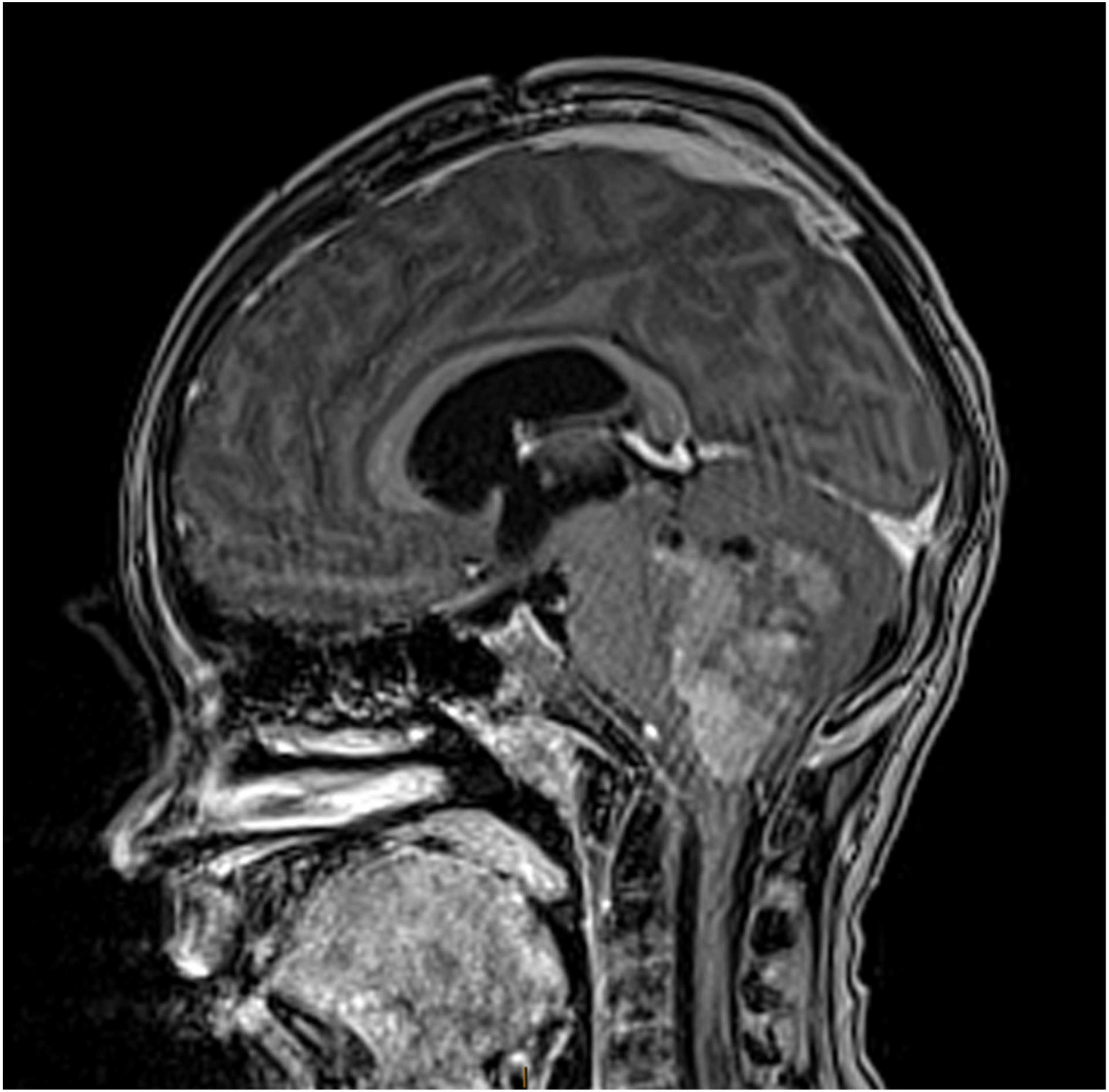
January 20, 2024 MRI T1-weighted Sagittal View.
January 23, 2024 Post Operative MRI T2-weighted Axial View.
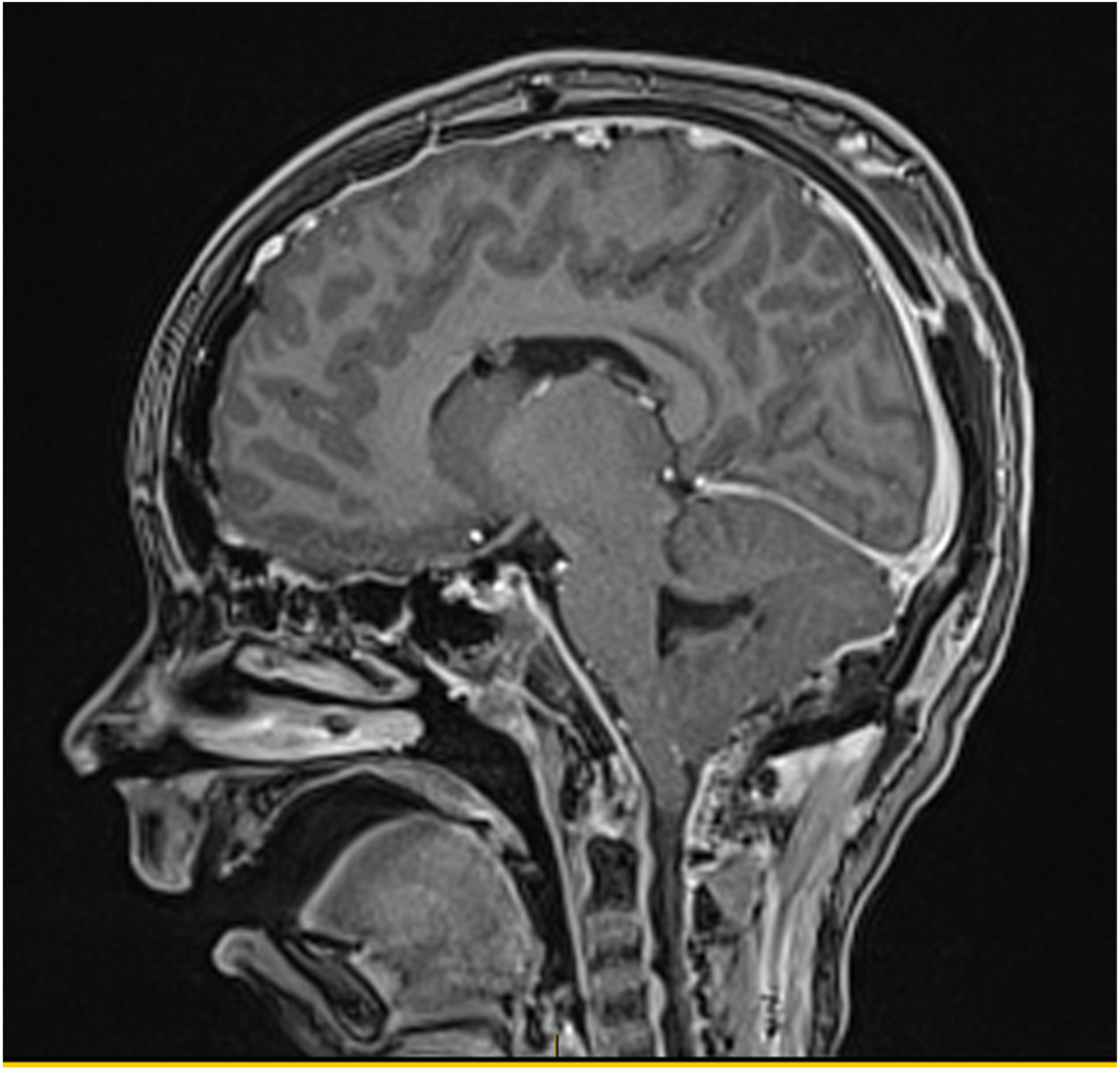
January 23, 2024 Post Operative MRI T1-weighted Sagittal View.
Following discharge from inpatient rehabilitation, the patient continued daily lorazepam therapy for approximately two months, after which the medication was gradually weaned. No functional regression was observed during or after discontinuation, and he has remained off lorazepam since that time without recurrence of symptoms. No clinically significant adverse effects attributable to lorazepam were observed during the treatment course.
Discussion
This report presents a case of ppCMS marked by mutism, ataxia, and emotional lability following resection of medulloblastoma with a positive response to lorazepam therapy. Symptom improvement began within one hour of administration, suggesting a potential therapeutic role for benzodiazepines in management of ppCMS.
Previous literature has documented variable outcomes with pharmacologic agents, but benzodiazepines are not widely cited as part of the therapeutic armamentarium.8,9 While lorazepam is not a standard treatment for ppCMS, there are cases documenting its success, particularly in management of mutism.10,11 Benzodiazepines, by potentiating GABA-A receptor-mediated inhibition, modulate basal ganglia-thalamocortical circuitry by attenuating indirect inhibitory pathways and enhancing striatal disinhibition of thalamic relay neurons, thereby enhancing cortical excitability, and rapidly reversing the functional suppression characteristic of cerebellar mutism. 12 This unexpected reactivation of cortical output, despite increased inhibition, may reflect a release from maladaptive suppression within the dentato-thalamo-cortical network, particularly in cases with catatonia-like features where disinhibition of thalamic relay nuclei restores behaviorally relevant function. 13 In the context of ppCMS, this mechanism may explain the paradoxical resolution of mutism following benzodiazepine administration, as the drug's modulation of inhibitory control pathways may transiently restore functional thalamocortical output disrupted by cerebellar diaschisis. However, its sedative potential and risk of dependency warrant judicious, short-term use under careful monitoring, and such usage must be individualized. Its therapeutic effect was also temporary, and symptom recurrence occurred once lorazepam's effect wore off. Future studies should move beyond asking whether lorazepam is effective in ppCMS and instead aim to define which patients respond, under what conditions, and why. The rapid and reproducible response to lorazepam in select cases suggests a treatable, reproducible improvement of the catatonic state in a subset of patients that calls for focused clinical investigations to guide treatment.
Conclusion
Pharmacologic intervention may reveal latent functional capacity in select ppCMS cases. The transient improvement following lorazepam suggests that some cases may involve reversible network-level inhibition rather than fixed injury. In this rehabilitation-centered context, the observed response offered clinical insight that informed ongoing therapeutic emphasis and supported continued engagement. As the understanding of ppCMS evolves, pharmacologic probing may complement neurorehabilitation by identifying reversible states within a broader spectrum of recovery, allowing clinicians to tailor strategies based not only on observed deficits, but on modifiable potential.
Footnotes
Acknowledgements
The authors thank the patient and their family for granting permission to share this case for educational and clinical advancement purposes.
Ethical approval and informed consent
Our institution does not require formal ethics committee approval for reporting individual cases. This case report was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent for the publication of this case and any associated images was obtained from the patient's legal guardian.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data relevant to this case report are included in the manuscript. No additional datasets were generated or analyzed.