
Abstract
Introduction
Neuromuscular scoliosis (NMS) in children poses significant challenges, including postural instability, pain, mobility limitations, and respiratory issues. Sensory dynamic orthosis (SDO) garments provide dynamic compression and proprioceptive feedback aimed at improving alignment and function. This pilot study explored the feasibility and preliminary effectiveness of SDO garments in the management of NMS.
Methods
A single-group pre–post, multicentre pilot study was conducted in 30 paediatric patients who used the SDO® Advanced orthosis for six months. Radiographic outcomes (Cobb angle, coronal balance, pelvic obliquity) and functional assessments (FLACC-R scale, Barthel Index) were recorded at baseline and after the intervention. Caregiver-reported satisfaction and perceived functional changes were gathered through a custom-designed questionnaire.
Results
Of the 30 participants, 25 completed the study (median age 13 [IQR 10–15]). Statistically significant within-subject reductions in Cobb angle were observed during SDO use at baseline (median difference −2.6°, p<0.001) and at final evaluation (median paired difference −4.0°, p<0.001). Similar within-subject improvements in coronal balance were observed at both time points (baseline median paired difference −2.1 cm, p<0.001; final −1.8 cm, p=0.005). Pelvic obliquity and Barthel Index scores showed no significant changes. Most caregivers reported slight to moderate improvements in functional domains and high satisfaction. No serious adverse events were observed, and adherence was high.
Conclusions
This pilot study suggests that SDO garments may contribute to short-term postural spinal alignment and balance during wear and perceived functional benefits in children with NMS. These preliminary findings support further research through controlled trials with longer follow-up to clarify clinical relevance and durability of effects.
Keywords
Level of evidence
Level IV – Pilot single-group pre–post study without a control group.
Introduction
Neuromuscular scoliosis (NMS) is a progressive spinal deformity affecting children with neurological or myopathic disorders, such as cerebral palsy (CP), myelomeningocele, Duchenne muscular dystrophy, spinal muscular atrophy, and Rett syndrome, among others.1,2 This condition results from poor motor control and muscle imbalance, especially in non-ambulatory patients, leading to abnormal spinal curvature and significant postural dysfunction.1,2 Scoliosis develops in approximately 75–90% of individuals with neuromuscular conditions,3,4 occurring in the setting of predominantly spastic or hypotonic axial trunk control. Its consequences include pain, cardiorespiratory compromise, mobility restrictions, and impaired performance of activities of daily living (ADL), such as sitting or feeding.1,2
Non-operative management typically includes orthotic interventions, such as casts, rigid braces, and textile orthoses, as well as wheelchair adaptations, aiming to improve postural alignment and function. However, these interventions rarely halt progression or avoid the need for surgery.1,2,5 Moreover, traditional rigid braces may cause discomfort, skin issues, and low adherence, particularly in NMS compared to those with idiopathic scoliosis. Surgical treatment, while often required in severe or progressive cases, carries considerable risk in children with underlying neurological conditions and comorbidities, highlighting the need for alternative or adjunctive strategies.1,2,5
The Sensory Dynamic Orthosis Advanced (SDO® Ad.) is a textile-based orthosis designed to provide dynamic compression and proprioceptive input. 6 Its elastomeric fabric delivers continuous sensory feedback, aiming to enhance trunk control, postural stability, and overall alignment.7–10 Unlike rigid thoracolumbosacral orthoses (TLSOs), which apply three-point corrective forces, the SDO promotes active postural alignment by stimulating trunk musculature, improving body awareness, and supporting proximal stability during functional activities. The garment is custom-patterned for each child, incorporating strategic panel reinforcement and variable tension zones to encourage midline alignment while preserving mobility of the ribcage and pelvis. This flexibility allows use during activities such as sitting, standing, transfers, communication, feeding, and assisted mobility—tasks that are often restricted by rigid bracing. Previous studies of dynamic elastomeric fabric orthoses (DEFOs) have reported potential benefits in scoliosis management, including improvements in Cobb angle and functional capacity11–13; however, evidence specific to NMS remains limited.
This pilot study represents an initial step in evaluating the clinical utility of the SDO Ad. in a well-defined paediatric NMS population. The primary objective was to explore the preliminary effects of the SDO Ad. on spinal alignment and balance, alongside caregiver-reported outcomes related to function, usability, and satisfaction. These early findings may serve to guide future controlled trials and support clinical decision-making in the management of complex paediatric neuromuscular conditions.
Methods
This pilot, single-group pre-post, multicentre, non-randomised, and non-blinded intervention study was conducted at two health centres: the Hospital Universitario de Cruces in Bizkaia and the Hospital Infantil Universitario Niño Jesús in Madrid. Thirty paediatric patients (under 18 years) with NMS were recruited, all of whom had previously used DEFOs and had received medical recommendations for the use of the SDO Ad. The intervention was integrated into their standard care pathway. Each participant served as their own control, with within-subject comparisons performed between measurements obtained with and without the orthosis. All participants were non-ambulatory or had only marginal ambulation. Ethical approval was obtained from institutional ethics committees at both centres (no. R-0044/23), and informed consent was provided by participants or their legal guardians before the study began.
Eligibility criteria
All patients were prescribed the SDO Ad. orthosis by their treating physician based on clinical indications, including axial hypotonia with poor trunk control, postural instability, difficulty maintaining midline alignment, and documented or anticipated limited tolerance of rigid TLSOs. Radiographic curve progression was considered as part of the overall clinical assessment but was not used as a primary decision criterion for SDO prescription. Families were informed about available standard orthotic options, including rigid and 3D corrective bracing, and the decision to initiate SDO use was made collaboratively, taking into account comfort, tolerance, and individualised functional goals.
Exclusion criteria included major surgery within three months prior to enrolment, or scheduled surgery during the study period, baclofen pump implantation within the previous three months, ongoing axial muscle treatments (e.g., botulinum toxin), the use of rigid orthotic braces, or other scoliosis-specific interventions, such as serial casting. Patients intending to use the Exopulse Suit neuromodulation device during the study, those with allergies to orthosis materials (polyamide, elastane, cotton), and other medical contraindications such as cardiovascular conditions, skin disorders, or oedema were also excluded. Patients who declined participation or withdrew consent were not included in the study cohort.
Intervention
The SDO was introduced gradually, starting with a wearing schedule of two hours on the first day and increasing by one hour daily until reaching a minimum of eight hours per day or the maximum tolerated duration. This progressive wear schedule was designed to maximise proprioceptive input while ensuring comfort and tolerance, in line with clinical recommendations for DEFOs and routine paediatric neurorehabilitation practice. The target wear duration was maintained for six months. Participants were instructed to wear the orthosis during daily activities, including sitting, standing, and limited mobility tasks. Compliance was meticulously recorded for each participant, calculated as the average daily wear time (hours/day) and percentage of days used per month, with monthly follow-up phone calls conducted to monitor adherence and address concerns. All participants continued to receive standard postural support (e.g., customised wheelchair seating), as part of usual NMS management.
All SDO garments were fully tailored to each patient. For children with gastrostomy tubes, a customised gastrostomy opening (“gastro hole”) was incorporated during fabrication to avoid pressure on the stoma and to allow safe access for feeding and routine care. Other medical devices (e.g., tracheostomies) were accommodated through individualised pattern modifications as required, ensuring comfort, safety, and uninterrupted use of the orthosis.
The study protocol did not include a formal weaning phase. After the final assessment, families were free to continue or discontinue SDO use according to clinical needs, and post-study use was not monitored.
Outcomes and assessments
The primary outcome focused on spinal curvature magnitude, measured using the Cobb angle from full-spine radiographs (taken in standing or sitting positions). Curve location and type, pelvic obliquity (measured at the iliac crests), and coronal plane balance (assessed using a plumb line method, in centimetres) were assessed. Radiographs were obtained at baseline and six months post-intervention, both with and without the orthosis, allowing paired within-subject comparisons under both conditions at each time point. To ensure consistent positioning, a custom-designed seating device was used during radiographic assessments for all participants. All spinal curves were partially flexible, as assessed indirectly through radiographic comparisons with and without the orthosis.
Secondary outcomes included pain/irritability, evaluated using the Face, Legs, Activity, Cry, Consolability – Revised (FLACC-R) scale, and ADL performance, assessed with the Barthel Index. The FLACC-R scale rates five categories (0–2 per item), yielding a total score (0–10) classified as relaxed/comfortable (0), mild discomfort (1–3), moderate pain (4–6), or severe pain (7–10). The Barthel Index measures performance in ADL on a scale of 0–100, with higher scores indicating greater independence. Both tools were administered at baseline and after six months.
Finally, caregiver feedback and satisfaction were evaluated through a custom-designed questionnaire based partly on the International Classification of Functioning, Disability and Health (ICF) framework. This tool aimed to assess changes in ADL following the use of the SDO Ad. and to measure caregiver satisfaction, as no existing instrument fully met these objectives. Parents or primary caregivers completed the questionnaire at the conclusion of the study. The questionnaire consisted of two sections: 1. Functional Assessment (Q1-Q10): Evaluating changes in posture, attention, feeding, communication, breathing, hand use, transfers, emotional state, family and social interactions, and school activities, rated on a five-point Likert scale (from “worse” to “significant improvement.”) 2. Satisfaction and Usability (Q11-Q15): Assessing ease of use, tolerance, and overall satisfaction, with scores rated on a five-point Likert scale (from “absolutely not” to “definitely yes.”)
Scores were weighted for the satisfaction section, with a maximum total score of 100 points, providing a comprehensive evaluation of functional and satisfaction-related outcomes (Supplemental Figure 1).
Additionally, adverse events related to orthosis use were recorded throughout the study period to ensure participant safety and assess any potential complications associated with wearing the SDO.
Statistical analysis
Analyses were conducted using IBM SPSS Statistics software (version 23, IBM Corp., Armonk, NY, USA). Quantitative variables were expressed as medians with interquartile ranges (IQRs), while qualitative data were reported as absolute values and percentages. Given the single-group pre–post design, all primary analyses were conducted using paired within-subject comparisons rather than between-group analyses. The Wilcoxon signed-rank test was used for paired data, and the Mann–Whitney U test was applied for independent samples. The primary endpoints were changes in the Cobb angle, pelvic obliquity, and coronal balance from baseline to the final follow-up, both with and without the orthosis. Secondary analyses included changes in pain levels and functionality in ADL, assessed using the FLACC-R and Barthel scales, respectively, as well as key responses from the questionnaire. Pearson’s correlation coefficient was used to examine relationships between average daily use (hours/day), percentage of days used, and variables such as age, Barthel Index scores, FLACC-R scores, and radiographic measures. Multivariate analyses were performed to identify group differences in numerical variables. ANOVA was employed to compare means among three or more groups, and the Mann–Whitney U test was used for non-normally distributed data. Binary logistic regression was conducted to identify factors influencing high satisfaction scores, specifically for perceived quality of life (QoL) (Q11), willingness to reuse the orthosis (Q14), and likelihood of recommending the orthosis (Q15). A p value < 0.05 was considered statistically significant for all analyses. Because of the exploratory nature of this pilot study and the use of predefined clinical outcomes, no formal correction for multiple comparisons was applied.
Results
A total of 30 patients with NMS were initially recruited for this pilot study. Of these, five were excluded due to non-compliance with the intervention protocol or inability to attend the required initial and final evaluations, resulting in a final sample of 25 participants who completed the study protocol and were included in the paired analyses. The median age of participants was 13 years (IQR: 10–15), with 48% of the cohort being female. The primary diagnoses included CP (13; 52%), chromosomopathy (3; 12%), Rett syndrome (2; 8%), epileptic encephalopathy (2; 8%), and other conditions such as myelitis, Pierre Robin syndrome, acquired brain injury, spinal muscular atrophy, and leukodystrophy (1; 4% each). Spinal curves were predominantly single (76%), while 24% exhibited double curves. Curve localisation was thoracolumbar in 10 participants (40%), thoracic in nine (36%), and combined thoracolumbar in six (24%). Some patients had structured surgical curves; however, surgery was ruled out due to their overall health condition. All participants presented with predominantly hypotonic trunk involvement.
Orthosis usage and adherence
The median daily wear time of the SDO was 8.5 hours/day (IQR: 5.8–9.5), with participants using the orthosis on 84.7% (IQR: 76.6–92.4) of days throughout the six-month intervention period (Figure 1). Six participants demonstrated full adherence, wearing the orthosis almost every day. In contrast, individuals with the lowest compliance wore the device on fewer than 50% of the study days, highlighting variability in adherence across the cohort. This variability was primarily attributed to external factors unrelated to the orthosis itself, such as caregiver health issues, hospitalisations, and patient health issues that temporarily hindered use. No rebound worsening in posture, discomfort, or function was observed during temporary interruptions of use. Clinical images of a patient with and without the SDO are displayed in Figure 2. Histograms depicting the distribution of average daily usage (hours [h]/day) and the percentage of days the sensory dynamic orthosis was used during the six-month intervention period. Clinical images of a patient with and without the sensory dynamic orthosis (SDO), demonstrating front, back, and side views. The images illustrate the changes in posture and alignment observed without using the orthosis (upper row) compared to with it (bottom row). Permission to use these photographs was obtained.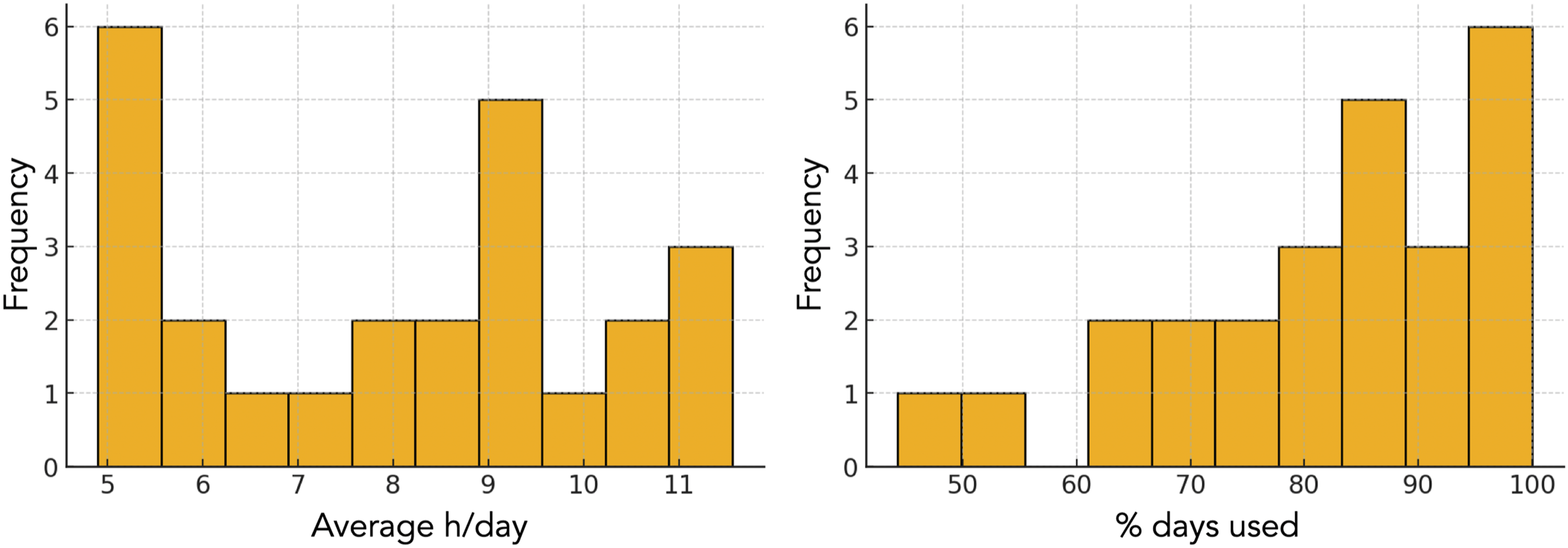

No serious device-related adverse events were reported. Participants generally tolerated the orthosis well, with no reports of significant discomfort or complications directly attributable to its use. Minor issues were reported in a small number of cases, including skin irritation, which was effectively managed by incorporating additional soft lining materials to reduce friction and improve comfort. Additionally, a few participants experienced mild reflux, which was resolved by integrating abdominal expansion zippers into the orthosis design, allowing for improved fit and pressure distribution.
Radiographic outcomes
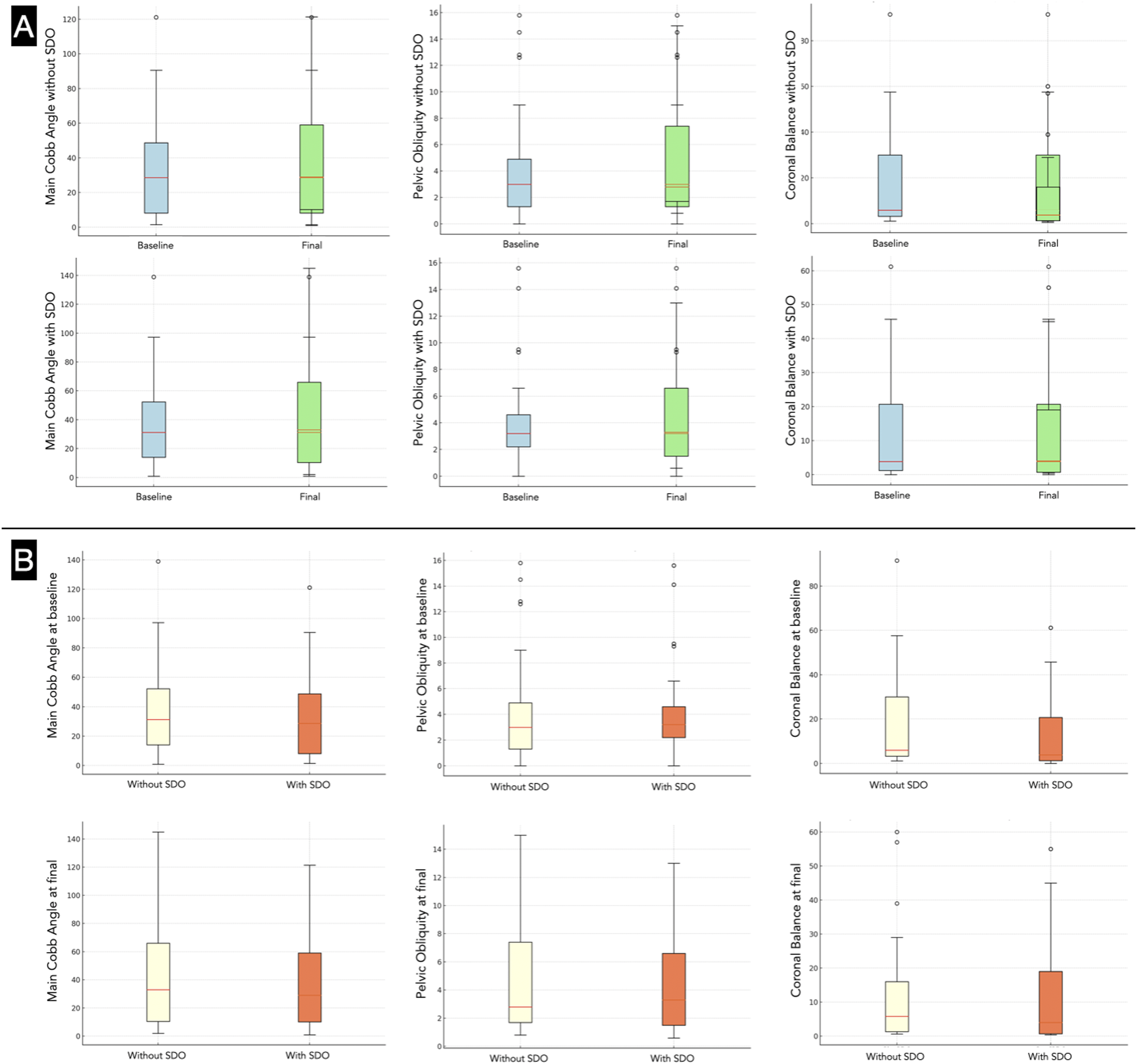
All radiographic comparisons are presented as within-subject paired comparisons (with vs. without SDO). Radiographic analyses demonstrated significant reductions in Cobb angle during SDO use at baseline (median difference −2.6°, p<0.001) and at final evaluation (median difference −4.0°, p<0.001). However, longitudinal changes in Cobb angle over time, either with or without the SDO, were not significant (p > 0.05). Pelvic obliquity also showed no significant changes between baseline and final evaluations, regardless of orthosis use (p > 0.05).
Coronal balance showed significant within-subject improvement during SDO use at baseline (median paired difference −2.1 cm, p<0.001) and at final evaluation (median paired difference −1.8 cm, p=0.005). Furthermore, coronal balance also improved modestly over time in measurements obtained without the orthosis (5.9 cm [IQR: 3.2–30.0] to 5.8 cm [IQR: 1.3–16.0]; p = 0.049) (Supplemental Tables 1 and 2; Figures 3 and 4). Baseline (left panels) and final (right panels) radiographic images from a study participant, illustrating measurements of the Cobb angle (Cobb), pelvic obliquity (PO), and coronal balance (CB) with and without the sensory dynamic orthosis (SDO). A. Comparative boxplots illustrating changes between baseline (blue) and final (green) measurements for the main Cobb angle, pelvic obliquity, and coronal balance, assessed both with and without the sensory dynamic orthosis (SDO). B. Comparative boxplots illustrating differences in the main Cobb angle, pelvic obliquity, and coronal balance between measurements without SDO (yellow) and with SDO (coral) at both baseline and final evaluations.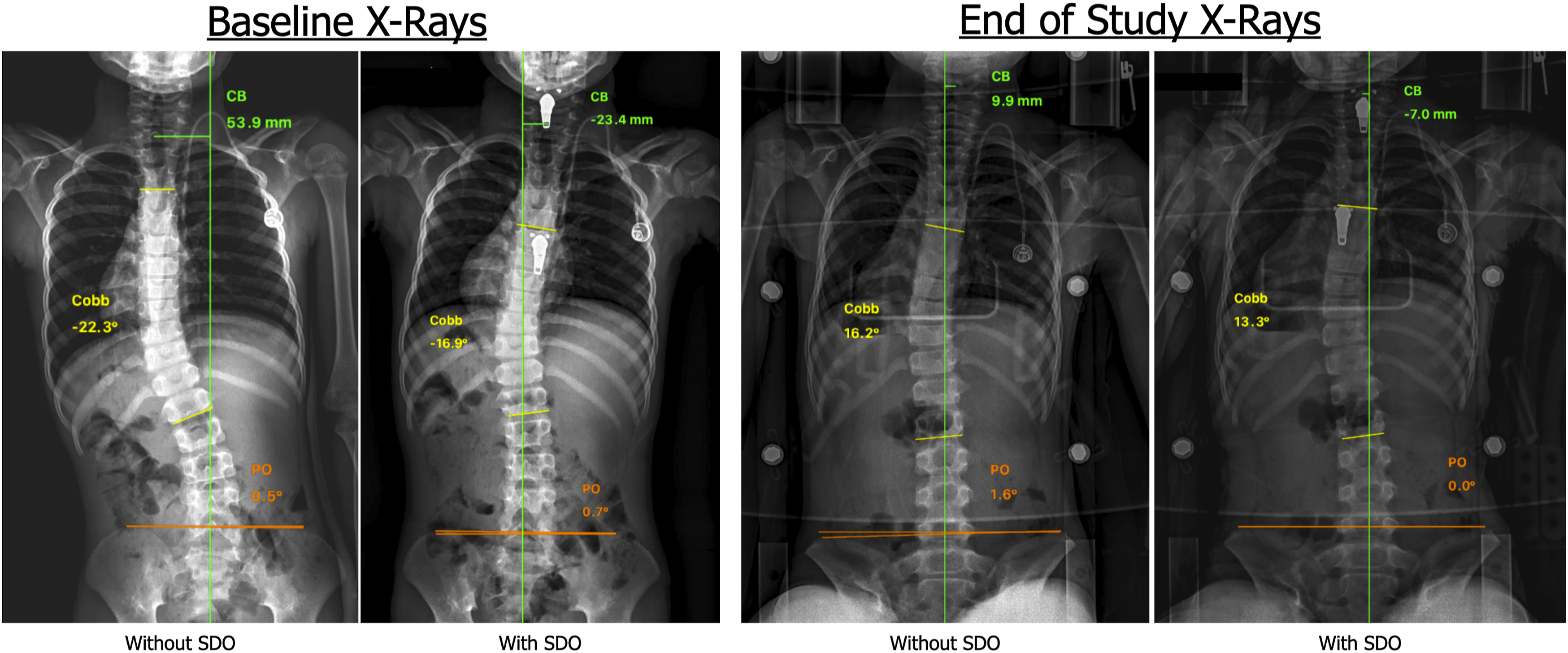
Functional outcomes
Pain levels, assessed using the FLACC-R scale, remained unchanged throughout the study, with all participants scoring zero at both the initial and final evaluations, indicating no discomfort or irritability. Similarly, functional independence measured by the Barthel Index showed no significant changes, with a median score of 20 (IQR: 0.0–35.0) at both time points, indicating no significant decline in functional status during the intervention period.
Caregiver-reported outcomes
Caregiver-reported outcomes (Supplemental Table 3; Figure 5) indicated notable improvements in specific functional domains and high levels of satisfaction with the orthosis. For functional assessments (questions 1–10), improvements were most frequently reported in posture, attention, hand use, transfers, and school-related activities. In contrast, feeding, communication, breathing, emotional state, and family interactions most commonly showed no change, although some caregivers reported slight to significant improvements in these domains. Satisfaction and usability (questions 11–15) received overwhelmingly positive feedback. The majority of caregivers selected “almost certainly” or “definitely yes” when asked about perceived QoL improvements, ease of use, tolerance, and willingness to reuse or recommend the orthosis. Horizontal stacked bar chart representing the distribution of parent-reported outcomes across 15 questions.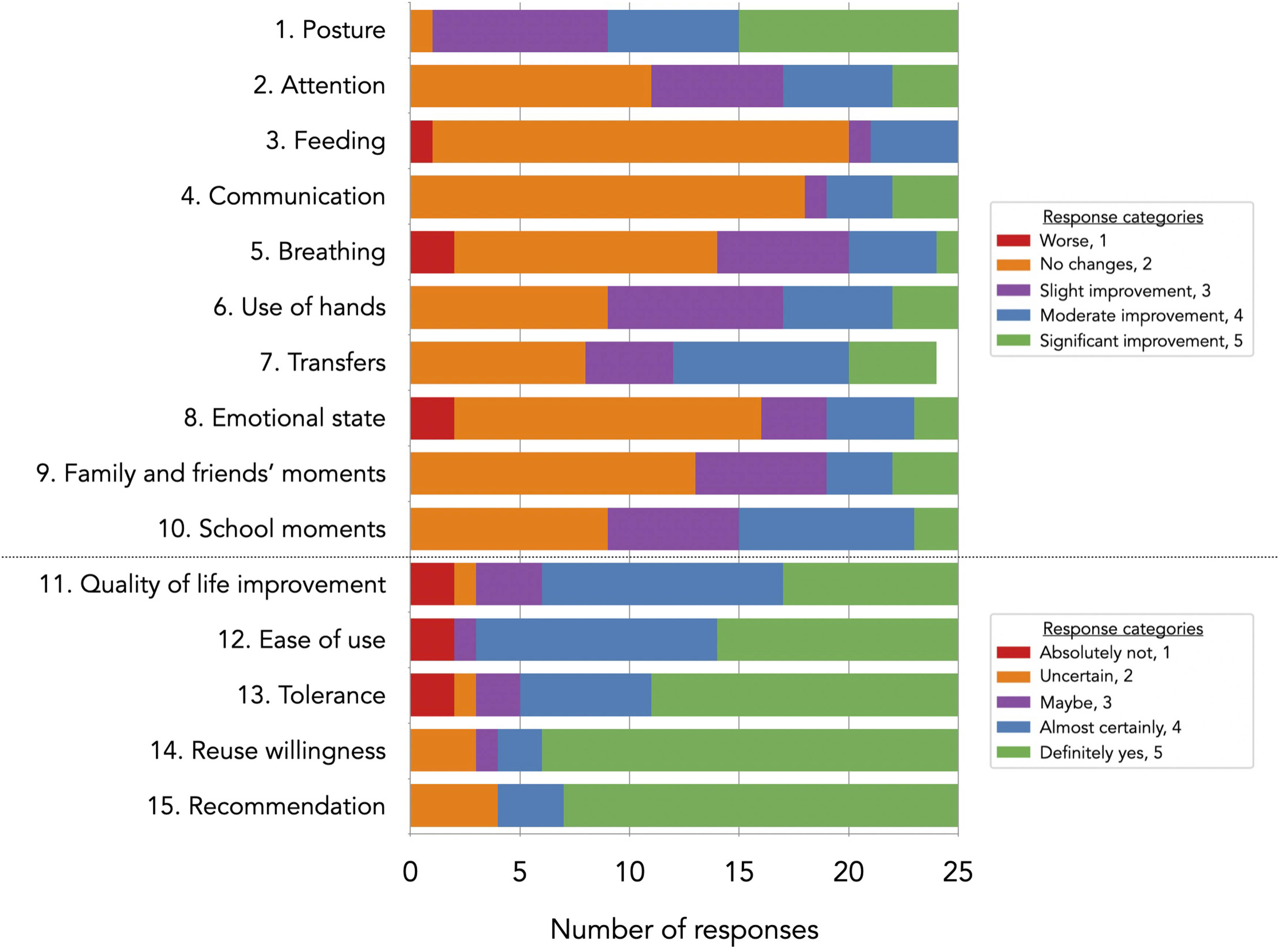
Correlation and logistic regression analysis
Correlation analyses between key variables of interest (age, Barthel scores, FLACC-R scores, Cobb angle, pelvic obliquity, and coronal balance) and orthosis usage (hours/day, percentage of days used) did not identify any significant associations (p > 0.05). Similarly, multivariate analyses examining relationships between usage metrics (hours/day and percentage of days used) and categorical variables such as sex, curve type, localisation, underlying pathology, head control, sitting, standing, and walking ability, as well as responses to the caregiver questionnaire, also failed to yield significant correlations (p > 0.05). Moreover, no significant correlations were found between baseline Cobb angle without the SDO or changes in Cobb angle and caregiver-reported outcomes (p > 0.05).
Binary logistic regression analysis was conducted to identify predictors of high satisfaction scores (questions 11, 14, and 15). However, no significant predictors were identified. Variables such as age, sex, compliance levels, and clinical outcomes did not significantly influence the likelihood of higher satisfaction scores. These findings suggest that caregiver satisfaction and functional outcomes may depend on unmeasured factors or that the study lacked sufficient statistical power to detect clear associations.
Discussion
To the authors’ knowledge, this is the first study to evaluate the efficacy of SDOs in managing NMS through radiographic assessments and functional outcomes in a paediatric cohort with predominantly hypotonic trunk involvement. These findings demonstrate modest but statistically significant within-subject reductions in Cobb angle and coronal balance during SDO use, with sustained reductions in coronal deviation over the six-month intervention period, underscoring the potential role of the SDO in promoting spinal balance. Functional measures, such as pain levels and ADL scores, remained stable throughout, suggesting that the SDO may contribute to the maintenance of functional capacity in this high-risk population. High caregiver satisfaction and perceived improvements in QoL further support the clinical relevance and psychosocial value of the intervention. The present results should be interpreted within the context of trunk hypotonia, in which external dynamic support and enhanced proprioceptive input may help compensate for deficient active trunk control.
The current findings should also be considered in the context of the existing literature on orthotic management of NMS. Traditional rigid TLSOs have been shown to improve seating and postural support but do not prevent curve progression and are primarily used for functional positioning.14–16 In contrast, flexible and fabric-based orthoses have demonstrated potential benefits, including in-brace correction and improved functional performance, although the available evidence remains limited and heterogeneous. 17 Most previous studies have focused on short-term or in-brace effects without consistent radiographic or functional follow-up. In this context, the current study adds to the literature by combining radiographic, functional, and caregiver-reported outcomes in a paediatric neuromuscular cohort, providing a more comprehensive evaluation of SDO use in clinical practice.
Radiographic findings
The radiographic findings, particularly the within-subject improvement in coronal balance, highlight the potential efficacy of the SDO in enhancing postural spinal balance in children with NMS. These observations are consistent with prior research on DEFOs, which emphasise proprioceptive input and muscle tone modulation in achieving spinal balance, rather than focusing solely on curve progression, as is typically aimed for with rigid braces.12,18 While statistically significant within-subject reductions in Cobb angle were observed during orthosis use, the magnitude of change was small, and no significant longitudinal changes were detected over time; therefore, the current findings must be interpreted strictly as postural effects during orthosis wear, rather than evidence of structural modification of the spinal curve. The maintenance of curve stability is itself a relevant outcome, given the progressive nature of NMS.1,2,5 However, the six-month follow-up period is insufficient to assess long-term structural effects. Unlike rigid braces, dynamic orthoses may reduce the risk of secondary complications, such as muscle atrophy, respiratory issues, and discomfort, thereby promoting better tolerance and long-term adherence. 19
Adherence
Adherence remains a critical factor in the success of conservative treatments for NMS, given the physical and logistical demands on patients and caregivers. In this study, the median daily usage of the SDO was 8.5 hours/day, with participants wearing the device on 84.7% of days over the six-month intervention period. The dynamic materials, customised fit, and gradual wear schedule likely contributed to the good tolerance of the SDO, addressing common barriers like discomfort and limited mobility. 12 This adherence rate may compare favourably with rigid braces, which can be associated with lower compliance due to discomfort, bulkiness, and restricted mobility in NMS.20,21 The present findings align with previous reports highlighting that flexible, lightweight orthoses, which accommodate the child’s daily routine and comfort, can significantly improve adherence and treatment feasibility.22,23 However, adherence variability across participants, influenced by external factors such as caregiver health and hospitalisations, underscores the importance of supporting families to integrate orthotic use into daily routines, particularly in patients requiring high caregiver support. These findings emphasise that meaningful adherence is achievable in real-world conditions with appropriate device design and family support.
No significant associations were identified between daily wear time or percentage of days used and radiographic or functional outcomes. The absence of a detectable dose–response relationship may reflect the small sample size, heterogeneity of neuromuscular conditions, and ceiling effects in pain and ADL measures. In addition, wear time appeared to be influenced more by overall health status and tolerance than by orthosis-related factors alone, with children who were more medically fragile often requiring shorter wear periods and more frequent rest. Larger, stratified studies are needed to better explore whether dose–response relationships exist across different neuromuscular and postural profiles. Importantly, no rebound worsening in posture, discomfort, or function was observed during temporary interruptions of use. Given the dynamic and proprioceptive mechanism of the SDO, which supports active postural engagement rather than immobilisation, muscle disuse and rebound effects are considered unlikely.
Functional outcomes
Pain levels and ADL scores remained stable throughout the study. No significant decline was observed in FLACC-R pain scores or Barthel Index values over the six-month period. These findings should be interpreted cautiously, as both instruments may have limited sensitivity to detect subtle functional changes in a medically complex, predominantly non-ambulatory NMS population with low baseline functional levels. Nevertheless, the absence of detectable deterioration suggests that the SDO may support postural comfort and maintenance of functional status during the intervention period, which is particularly relevant in fragile NMS populations. This aligns with the primary goal of many orthotic interventions in neuromuscular conditions, which is to prevent deterioration rather than induce functional gains.22,23 Maintaining functional stability is particularly valuable in patients with neuromuscular conditions, where even small declines can significantly impact QoL.10,24 Dynamic orthoses, by providing adequate support and improving posture, 8 may facilitate sustained participation in daily activities, reinforcing their role as a conservative management option for NMS.7,11,15,25 Previous studies on DEFOs have reported that even short-term use can yield improvements in postural stability, sitting balance and trunk control, gait and manual dexterity in children with CP.26,27 However, long-term effects in NMS remain underexplored, reinforcing the need for additional research.
Caregiver-reported outcomes
Caregiver-reported outcomes revealed consistent positive experiences with the SDO, with improvements noted in domains such as attention, hand use, transfers, and school-related activities. These findings align with prior research emphasising the role of DEFOs in addressing postural challenges and in enhancing participation in daily life for children with neuromuscular conditions.11,12 However, modest changes in domains like feeding, communication, and emotional well-being point to the complexity of achieving uniform improvements across diverse functional domains in NMS populations. High caregiver satisfaction and willingness to continue or recommend the orthosis further support its ease of use and perceived benefits in enhancing functional independence, reinforcing its practicality in daily life. This aligns with literature indicating that caregiver perceptions are crucial determinants of adherence and treatment success.10,28 By addressing both functional and emotional aspects of caregiving, the SDO not only improves patient outcomes but also reinforces caregiver engagement, thereby enhancing adherence and overall well-being. These findings strengthen the argument for family-centred, user-adapted orthotic solutions in paediatric neuromuscular care. 29
Limitations, strengths and future directions
Several limitations should be acknowledged. The non-randomised, single-group design and small sample size of the study limit generalisability of the findings. Additionally, although the custom-developed caregiver questionnaire provided valuable insights, its non-validated nature may introduce bias and restrict comparability with other studies. The six-month follow-up period was insufficient to evaluate long-term outcomes, particularly with respect to curve progression and durability of postural effects. Furthermore, post-study use of the orthosis was not monitored, and no formal post-discontinuation assessment was performed. Variability in adherence due to external factors also highlights the need for strategies to improve compliance in future interventions. Finally, no predictors of high satisfaction were identified, likely due to limited statistical power, response variability, unmeasured factors, and potential multicollinearity among predictors.
Despite these constraints, a key strength of this study is its focus on real-world usability and adherence in a complex clinical population. Detailed monitoring of daily wear time and caregiver-reported outcomes provides valuable insights into the practicality and acceptability of SDO use. The inclusion of both radiographic and functional assessments offers a comprehensive evaluation of the impact of the orthosis, setting a foundation for future research. Future studies should incorporate controlled, long-term designs to assess sustained effects on radiographic and functional outcomes in children with NMS.
Conclusions
This pilot study suggests that the SDO Ad. is a feasible and well-tolerated conservative treatment option for children with NMS and hypotonic trunk involvement, particularly in promoting short-term spinal balance during wear and supporting functional stability. The high level of caregiver acceptance and usability highlights its potential role as an adjunct to standard postural management. These preliminary findings warrant further evaluation through controlled studies with longer follow-up to determine clinical relevance, durability of effects, and potential impact on long-term outcomes.
Supplemental Material
Supplemental Material - Use of sensory dynamic orthosis in paediatric neuromuscular scoliosis: A pilot single-group pre–post study
Supplemental Material for Use of sensory dynamic orthosis in paediatric neuromuscular scoliosis: A pilot single-group pre–post study by Idoia Gandarias-Mendieta, María Galán-Olleros, Carmen Martínez-González, Rosa M. Egea-Gámez, Ignacio Martínez-Caballero in Journal of Pediatric Rehabilitation Medicine
Footnotes
Acknowledgements
The authors sincerely thank the families who participated in this study for their support and cooperation. We extend our gratitude to Dr. Miren Cobos Prada and the Paediatric Traumatology Department at the University Hospital of Cruces for their assistance in patient recruitment, and to Dr. Susana Cartas Carrión, rehabilitation physician, for her continued involvement in the care of many of these patients at Hospital Infantil Universitario Niño Jesús. We also acknowledge the Radiology Departments of the University Hospital of Cruces and the Hospital Infantil Universitario Niño Jesús for conducting the imaging studies. Finally, we appreciate Medigarments for providing the SDO® Advanced orthoses free of charge, which made this study possible.
Ethical considerations
Institutional Review Board approval was obtained for this study (
Consent to participate
Written informed consent was obtained from all participants or their legal guardians before participation.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declare no conflicts of interest relevant to the content of this article. Medigarments provided the SDO® Advanced orthoses free of charge for the purposes of this study; however, the company had no role in study design, data collection, analysis, interpretation, or manuscript preparation.
Quality assessment
All authors affirm their responsibility for the accuracy, reliability, and integrity of the data presented, as well as the unbiased interpretation of the findings.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.