
Abstract
Introduction:
Death investigators (DIs) such as coroners, medical examiners, and forensic pathologists play important and evolving roles in deceased organ donation. DIs communicate with organ donation organizations (ODOs) to gather case-specific information and release or restrict organs depending on the medicolegal requirements. This scoping review aims to identify the breadth of roles and decision-making processes that may facilitate or hinder deceased donation in DI cases.
Methods:
This study was conducted using a scoping literature review and subsequent thematic analysis.
Results:
Thirty-one eligible papers described 8 common themes with region-specific nuances. These include: 1) shared (ODO and DI) protocols for early communication around each case; 2) shared standards and education for death investigation practices related to organ donation; 3) DI support staff or teams to facilitate organ donation; 4) DI authority to order additional testing and imaging before organ recovery; 5) donation-specific legislation to enhance DI and/or ODO operations; 6) legally trained DI authority to veto medical decisions to proceed with organ donation; 7) DI attendance at organ recovery; and 8) surgeons recording specific DI evidence during organ recovery.
Conclusion:
These findings have cultural and resource-allocation implications and expose gaps in the international literature describing practices at the intersection of deceased organ donation and death investigation. A better understanding of the rationale and execution of various systems for DI and ODO cooperation may serve to advance both organ donation and death investigation.
Keywords
Introduction
Death investigators (DIs) such as coroners, medical examiners, and forensic pathologists play important and evolving roles in deceased organ donation. In almost all regions, DIs have jurisdiction over the deceased during sudden, unexpected, or non-natural deaths, with over 70% of potential organ donors falling under DI jurisdiction in the United States (1). The role of the DI is to determine the cause and manner of death. This involves understanding the circumstances of the death and may require postmortem examination of the body and organs. Death investigators often communicate with organ donation organizations (ODOs) to gather case-specific information as they weigh enabling donation against their medicolegal priorities.
The roles of DIs and ODOs increasingly intersect for two key reasons. First, medical advances have enabled the transplantation of organs that previously would have been nonviable (2). Second, technological advances often allow DIs to obtain the necessary information to fulfill their roles without a full autopsy; for example, postmortem computerized tomography (CT), postmortem tissue sampling, and rapid toxicological testing permit targeted dissections (2 -4). Additionally, improvements in donation practices universally (e.g., greater public awareness) have increased the number of organ donors. However, demand exceeds supply and barriers to donation remain, including restrictions imposed by DIs to ensure thorough inquiry.
Internationally, the coronial and medical examiner systems are diverse with various interhospital relationships, training, and medicolegal support staff. To improve organ donation rates in the context of a death investigation, we sought to understand how processes vary internationally, with a view to inform best strategies. This scoping review aims to identify the breadth of roles and decision-making processes that may facilitate or hinder deceased donation in DI cases, with an intent to inform Canadian provincial and national policy development.
Methods
To elucidate the manners of intersection of DI and organ donation across regions, the primary investigator conducted a scoping literature review based on Arksey and O’Malley methodology (5). This included five databases with no date or language restrictions: PubMed, OVID, Web of Science, TRIP, and CINAHL. Keywords included death investigator/coroner/forensic pathologist/pathologist/procurator fiscal/medical examiner AND organ donation/tissue donation/transplant/procurement. A second search using the PubMed MeSH terms “Coroners and Medical Examiners” and “Organ and Tissue Procurement” retrieved additional papers.
Eligible studies addressed the relationship between DI and organ recovery systems within any country or state. We excluded informal studies (editorials, letters) and focused on the most recent descriptive studies of practices in any given geographic region. Those that solely reported donation rates in forensic cases or effects of donation on court proceedings were also excluded. We then assessed the references of included articles for additional sources. Two investigators generated a checklist of preliminary themes to assess within each included article. As new themes emerged, we returned to the earlier articles and reassessed for these new themes.
Results
The literature search identified 76 articles, of which 31 articles originating from eight countries (Australia, France, New Zealand, Spain, Sweden, Turkey, United Kingdom, and United States) were eligible for review ( Figure 1 ). Of the American papers, nine were national and eight were state-specific (Arkansas, California, Colorado, New York, Nevada, and Texas). The regions reported on were those that had available literature, as most countries, including Canada, have not published on this topic. Investigators identified three additional themes in the first paper, which we subsequently assessed in all articles (Themes C, D, and E, Table 1 ). Additionally, we added two themes from a subsequent article and returned to assess all articles for these themes (Themes G and H, Table 1 ) (6). Ultimately, we identified 12 themes that appeared in articles from more than one country or state. We have consolidated these topics to report eight final themes ( Table 2 ).
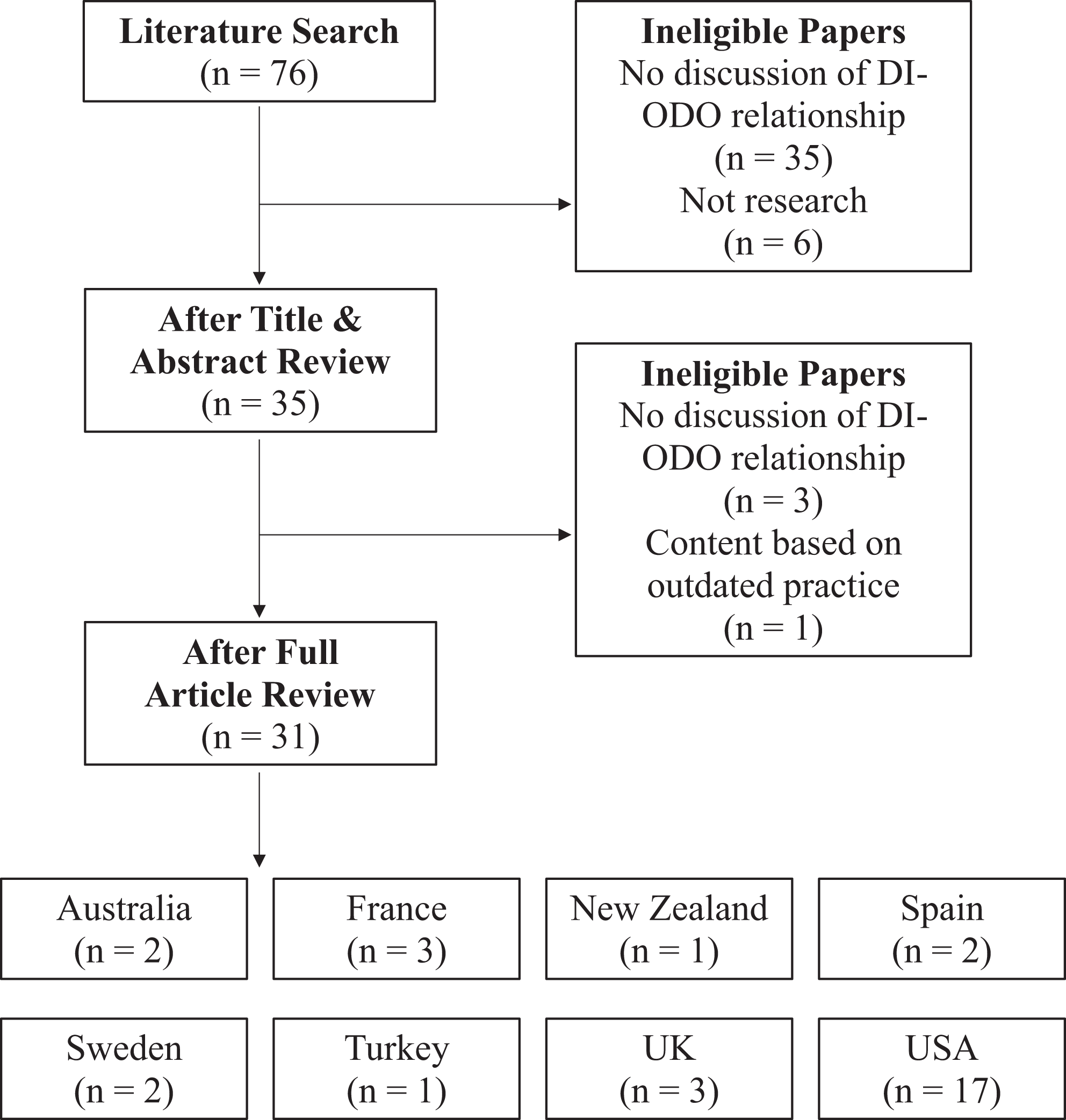
Article selection.
Thematic Distillation to Eight Final Themes.
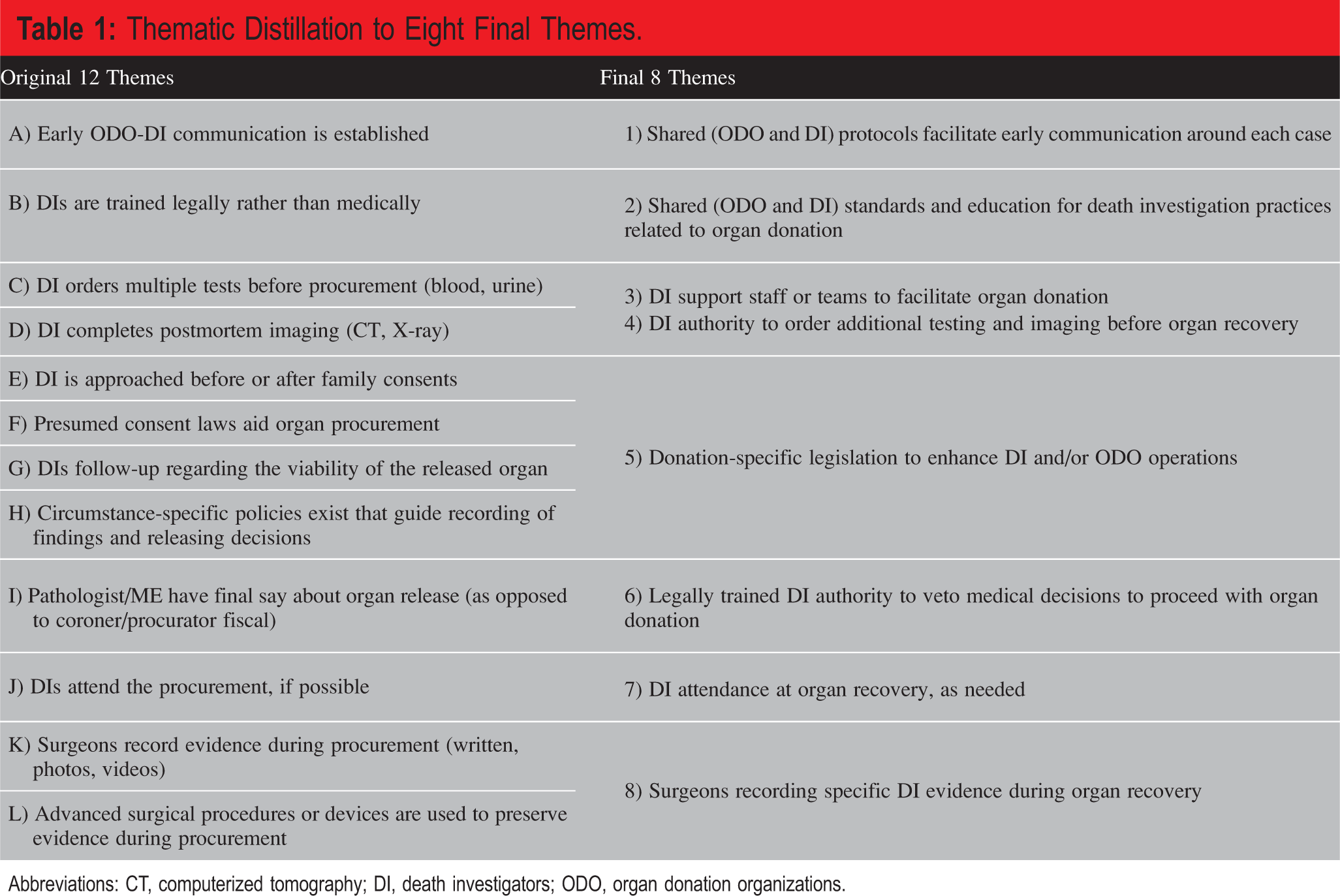
Abbreviations: CT, computerized tomography; DI, death investigators; ODO, organ donation organizations.
Death Investigation and Organ Donation System Themes Identified in the Scoping Review.
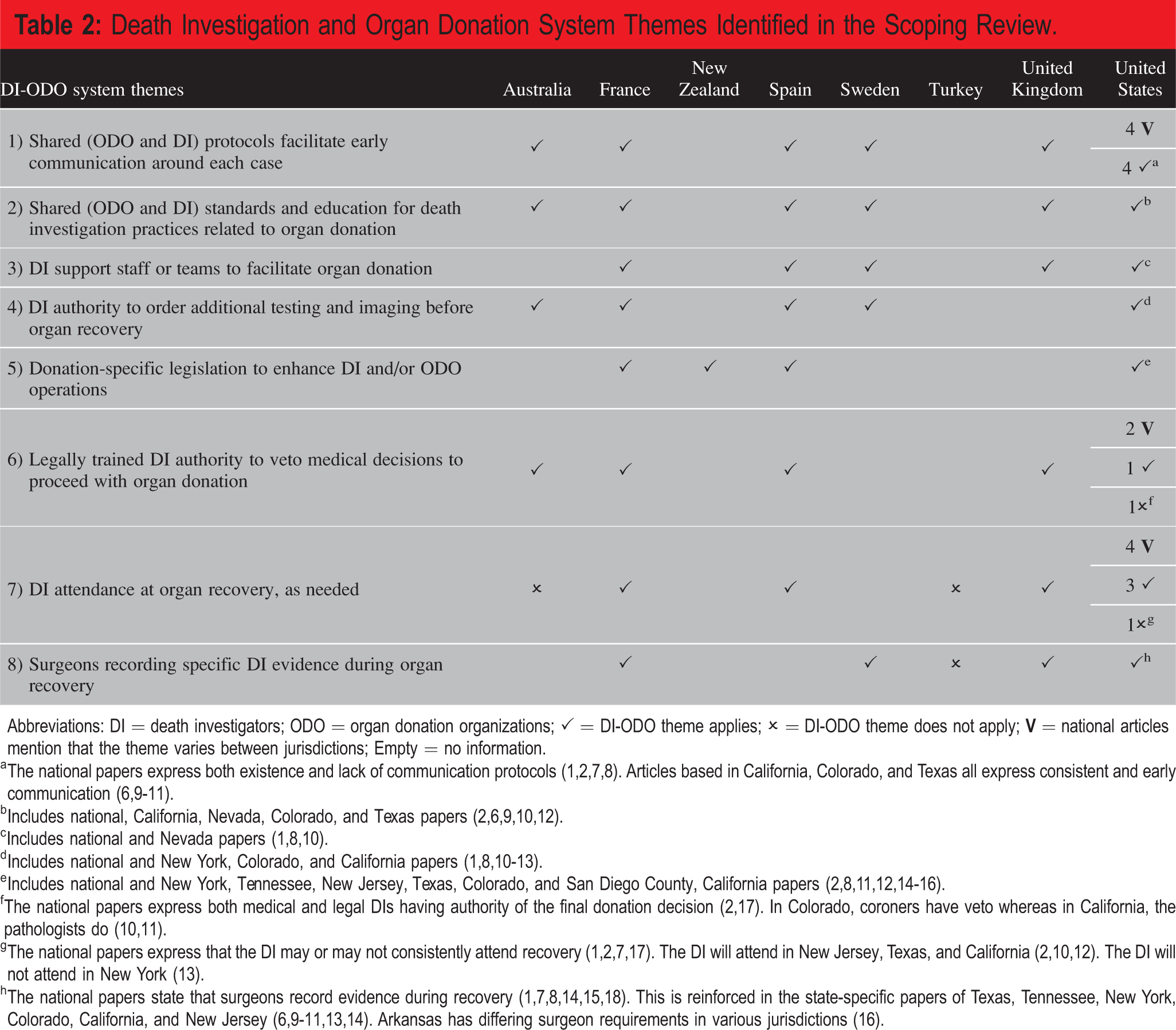
Abbreviations: DI = death investigators; ODO = organ donation organizations; ✓ = DI-ODO theme applies; ✗ = DI-ODO theme does not apply;
a The national papers express both existence and lack of communication protocols (1,2,7,8). Articles based in California, Colorado, and Texas all express consistent and early communication (6,9 -11).
e Includes national and New York, Tennessee, New Jersey, Texas, Colorado, and San Diego County, California papers (2,8,11,12,14 -16).
f The national papers express both medical and legal DIs having authority of the final donation decision (2,17). In Colorado, coroners have veto whereas in California, the pathologists do (10,11).
Themes
1) Shared (ODO and DI) protocols facilitate early communication around each case
Early and continuous communication was the most common theme, integrating DIs, ODO personnel, intensive care unit (ICU) physicians, nurses, and support staff. In France, magistrates, rather than physicians, initiated communication with the DI and ODO and may determine that a case did not require autopsy (13). In the United Kingdom, Specialist Nurses in Organ Donation contacted the coroner to facilitate organ release, while coroners protected forensic evidence and liaised with regional transplant centers (19). The Swedish National Council for Organs, Tissues, Cells and Blood also had agreements with distinct forensic units to facilitate early and consistent communication (20). In Spain, annual meetings held between judges, magistrates, DIs, and ODO coordinators facilitated discussion to identify communication weaknesses and to prompt quality improvement (6,21).
In the United States, communication channels varied among states. A study conducted in Virginia found that, nationally, PICU directors (who regularly liaise with DIs) were more interested in improving communication, education, and documentation with the DI than implementing systemic changes in workflow, and that many ODO or clinical staff did not understand the forensic intricacies (22). To improve both areas, Colorado hosted a joint task force of ODO staff, coroners, and district attorneys to develop the Colorado Organ Recovery Systems (23). As a result, stakeholders appreciated the urgency for donor hospitals to identify coroner cases and encouraged early communication (23). As well, Nevada established a death notification portal; an efficient and secure software to report referrals, view case information, and facilitate early and continuous hospital-DI communication (10). In addition to donation and medicolegal professionals, California police were involved early in the investigation and donation procedures to communicate key forensic findings (9). 2) Shared (ODO and DI) standards and education for death investigation practices related to organ donation
For various regions, authors reported the importance of delegating specific DI, ODO, and ICU physician responsibilities while ensuring each party understands the other roles (6,10,19
-25). Many stakeholders have advocated for standardized protocols to reduce subjectivity and personal bias during organ release, however, a survey by Kurachek et al. found that DIs (across 32 states) using objective protocols were less likely to release organs (25). Therefore, DIs had specific protocol guidance that allowed for some degree of subjectivity. Protocols typically aimed to specify who to contact, which questions to ask, and what evidence to observe or preserve before organ recovery (2,7,9,20,23). For example, Sturner’s decision-making guidelines were widespread in the United States and outlined six variants of pediatric deaths and how they qualified for organ release (2,16). Additionally, Harris County Medical Examiner in Texas had distinct protocols for organ requests and decedent transport (6). Protocols functioned to unite medical and forensic parties in California, where shared guidelines involved ODO, DI, and related intensivists (7). In Colorado, the Colorado Organ Recovery Systems protocol encompassed blood and urine tests, hospital procedures, and medical records to enforce ODO accountability, further involving surgeons and medical technicians (23). Aside from teaching these protocols in practice, some systems have mandated formal organ donation training. Sweden provides national practical courses for forensic staff (20). Similarly, Spain’s Ministry of Justice offers continuous training for forensic physicians (21). 3) Death investigator support staff or teams to facilitate organ donation
Many jurisdictions have introduced clinical or administrative roles specifically to support the integration of organ donation and forensic investigation. Throughout the United States, contracted pathologists, forensic nurses, and coroner liaisons assisted with DI donation cases alongside the UNOS Medical Examiner-Coroner Taskforce (1,10,12). Some ODOs have contracted distinct pathologists that can examine and release organs for donation even if they relate to the cause of death (1). Additionally, forensic nurses worked in hospitals throughout the United States to collect evidence from patient admission to death, specifically to facilitate time-sensitive organ donation procedures that follow death (12). Specific to Nevada, coroner liaisons and the Forensic Investigative Response Support Team (FIRST) act as clinical intermediaries between the ODO and DI (10). Liaisons examined decedents, collected specimens, and previewed images before involving the DI to grant permission (10). Coroner liaisons also prepared reports to communicate how investigative staff influence donation and to educate ODOs about forensic workflow (10). Otherwise, many European countries have initiated medicolegal positions to support donation. Sweden operated under a national donor coordinator, with explicit donor physicians and assistants at each regional unit (20). Distinctly, French magistrates, rather than forensic or surgical personnel, completed evidence collection before contacting forensic pathologists (13). 4) Death investigator authority to order additional testing and imaging before organ recovery
In articles that reported on this issue, DIs uniformly had the authority to request additional tests specific to death investigations before permitting donation. Thus, the DIs were knowledgeable about routine medical and donation-related specimen sampling and radiographic imaging (which varied across regions) and could request more. To facilitate the time-sensitive nature of DI input on organ donation, various regions established different protocols. Spanish coroners promptly visited the hospital to explore, photograph, evaluate, biopsy, and take tissues as needed, prior to organ donation (21). As a time-saving measure, an Australian system had the resources to acquire postmortem CT scans for 77% of potential organ donation coroner’s cases from 2009 to 2013, and this has since become standard practice (11). United States hospitals relied on the work of specialized forensic nurses for DI-specific sample collection, and timely communication of diagnostic test results, and photographs, whether polaroid, CT, magnetic resonance imaging (MRI), or X-ray, to the DI (12). In contrast, New York ODOs obtained CT, MRI, EEG, and lab results not only for donation purposes but to support subsequent death investigations, such that the DI could subpoena if needed (22). With similar intent, French coroners could impose preprocurement photos to aid in the death investigation (13). 5) Donation-specific legislation to enhance DI and/or ODO operations
Various donation-specific legislation concerning presumed consent of the decedent and autopsy protocols existed. Presumed consent is a framework in which potential organ donors are presumed to accept that they would be donors unless they formally registered their decision to opt-out, in advance. This allows ODOs and DIs to make donation decisions irrespective of each other or the family. However, it is common ethical practice to obtain consent from the next of kin. By Tennessee law, surgeons could retrieve organs without notifying the DI if the family consents (8). However, the DI and ODO established a relationship such that the DI was consistently contacted and informed of the organ condition and relation to death (8). In contrast, in New Zealand, if the decedent had consented to organ donation, there was no requirement for the DI to obtain additional family consent or notify the family of donation (14).
When the cause of death was explicit, the law may have limited the need for autopsies and death investigation to accelerate donation. In Spain, DIs would not complete an autopsy if the deceased was an organ donor, and the cause of death was clear (21). Following donation, the DI investigation was aided by following up on the viability of donated organs and the organs were automatically returned to French and American DIs if transplant could not proceed (13,15,24,27). Legislation may have also dictated whether the ODO first contacted the DI or the family of the deceased. In California, ODOs asked the family initially whereas, in Colorado, they first approached the coroner (7,15). In the United Kingdom, there was no national agreement on who to approach first (19). However, coroners were more likely to fully release organs in practice if they had known families had consented (89%) rather than if families had not yet been involved (77%) (19). 6) Legally trained DI authority to veto medical decisions to proceed with organ donation
Internationally, there were two classes of DIs: legally trained (judge, magistrate, procurator fiscal) and medically trained (medical examiner, forensic pathologist), with coroners having varied training (e.g., physician or not) depending on the region. In most jurisdictions, the legal DI authorized organ donation while the medical DI played a consulting role. This was the case in Australia, France, the United Kingdom, and some states in the United States (11,13,15,23,28,29,30). Depending on the system, legal bodies may have relied completely on the medical opinion or they may have decided in opposition. For instance, in Spain, judges rarely released organs without consulting a medical DI (6). Additionally, systems may have required DIs to provide reasons for total restriction or to negotiate with ODOs over partial restrictions (6). The notion of a legal DI veto was not a universal finding as medically trained DIs have the final say in California, New York, New Jersey, Texas, and Tennessee (9,12,17). 7) DI attendance at organ recovery, as needed
Examining the decedent preorgan recovery or attending the organ recovery could facilitate both organ donation and death investigations when there were resources to support this approach. In France, the same DI examined the decedent in the ICU, during the organ recovery surgery, and at autopsy (13,29,30). Protocols from states such as New Jersey, Texas, and Tennessee indicated that DIs could not deny organ donation without attending organ recovery (2,12,17). Additionally, Nevada implemented the FIRST to acquire photographic evidence and be present at the recovery and autopsy in place of the DI (10).
In other states and Australia, DIs attended organ recovery only when deemed necessary (2,12,17). In fact, Nunnink et al. reported that the DI attended only 1% of donation surgeries in Australia (11). On-call DIs in New York stopped attending each organ recovery due to insufficient overtime funding (31). In Turkey, if there was no perceived relationship between an organ and cause of death, a team of four physicians (cardiologist, neurologist, neurosurgeon, anesthesiologist) could determine the cause of death and proceed without involving a DI (32). 8) Surgeons recording specific DI evidence during organ recovery
In some cases, transplant surgeons were responsible for documenting organ abnormalities and evidence of trauma (27). Idiosyncrasies existed in the documentation, observation standards, and the legal role of the surgeon involved. In many jurisdictions, a copy of the operative note or postoperative report was sufficient for the investigation (1,12,27,29 -33). For example, in Sweden, DIs requested surgical reports if the donated organ was related to the cause of death (20). In the United Kingdom, the British Transplantation Society required surgeons to communicate findings in all coroner cases (28). Surgeons from Colorado and California may even be required to testify (9,15,23). However, without specific protocols for the documentation of such evidence, surgical reports were unlikely to inform death investigations. For example, DIs in New York argued that operative reports tended to focus on procedure rather than organ or body condition, therefore surgeons were not required to testify (31).
In addition to written observations by surgeons, the United States also employed photography and video documentation alongside altered surgical approaches or instruments to preserve evidence (1,9,23,24,26). For example, surgeons used alternative approaches to access pediatric chest organs and employ fiber optic instrumentation (24,26). Following recovery, any surgical interventions or means of vascular access were left for autopsy (9). Similarly, French DIs had all records of resuscitation, surgical procedures, and other interventions via postoperative reports (29,30). Altogether, surgeons played a critical investigative role in the absence of a DI during recovery.
Discussion
This scoping review of the literature assessing the intersections of death investigation and organ donation has revealed international commonalities as well as region-specific nuances. The work also highlights research and reporting gaps in this field. Nevertheless, the findings allow us to draw inferences for Canadian systems in the context of international reports.
The eight themes that emerged from this research reflect specific steps in the DI and donation processes that more than one report identified as helpful. For each of these steps, the specific implementation protocols varied substantially (e.g., differing communication methods between multidisciplinary parties, DIs accessing various hospital tests and imaging). The findings suggest a collaborative effort between DI and ODOs to maximize donation while maintaining high-quality death investigation. Conversely, other themes present opposing practices such as established versus no specific collaborative roles (e.g., forensic nurses); medical versus legal DI having final authority; DI attends versus does not attend the recovery; and surgeons do versus do not record evidence and/or testify. The origin and rationale for these distinct practices were unclear. Differing resource availability is apparent in the literature, such as when DIs in New York do not attend recoveries due to the lack of overtime funding (11,20,31).
These findings have many implications and highlight opportunities for potential practice improvement. As deceased organ donation awareness, registration access, and technological advances increase within both the public and the medical community, organ availability increases. Consequently, as more organs cross borders and as research in the field of organ donation extends internationally, there is an increased need for clarity and standardization between DI and ODO systems both within and between nations. Identifying unique practices such as the death notification portal and FIRST group in Nevada, the united hierarchy and training programs in Sweden, and the continuity of care for forensic donors in France prompts further innovation and potentially broader adoption (10,13,20,29,30). For countries not represented in this scoping review, interviews, surveys, and legislation review may identify additional opportunities to advance death investigation procedures in a manner that promotes deceased organ donation. These findings complement and are consistent with Nunnink et al., who identify similar themes but also review donation rates, restriction impact and types, and donation ethics (34). In contrast, this article provides an in-depth analysis of international ODO-DI systemic differences, with an intent to inform future Canadian provincial and national policy development.
Notably, there are no published Canadian reports on this topic and no national consensus on how best to implicate DIs when death investigations and potential organ donation intersect. This leads to variability in practice with aspects of all the above systems applied to individual cases, frequently decided on an ad hoc basis. There is currently no national database capable of reporting the number of cases that were refused due to DI refusal of organ recovery, but communication with provincial donation leads indicate that these situations are an infrequent but recurrent cause of nonprogression from potential to actual donor (personal communication Dr. Weiss, 25 August 2021). It is likely that national and provincial consensus using jurisdiction appropriate DI policies could result in at least some of these cases resulting in both successful organ donation and appropriate forensic investigations. Going forward, we will examine provincial rates of organ donation restriction in death investigations to elucidate any opportunities to increase donation while maintaining investigative integrity.
This study has some notable limitations. A single investigator conducted the scoping review with research supervision. It is plausible that the involvement of a broader investigative team throughout this scoping review might have generated additional themes. A major limitation was the paucity of available literature, such that for some countries, the most recent publications are pre-2000. Of the 31 articles identified, only eight countries were represented, and the majority (17 articles) originated in the United States. Moreover, there was insufficient information about some themes reflected in the original literature. Lastly, qualitative evidence concerning the degree of satisfaction with the varied DI-ODO themes was absent.
Conclusion
Effective collaboration between ODOs and DIs has the potential to enhance organ donation activity across jurisdictions. While the suitability of different approaches may vary across jurisdictions, this review stands to aid those reviewing individual practices by documenting the international experience, which has not been previously described. The vast differences in practice generate further questions concerning resource allocation, public attitudes, and government or health infrastructure in the context of organ donation. This work also highlights the need for innovation and international collaboration, prompting further research regarding the intersection of organ donation and forensic medicine.
Footnotes
Ethical Approval
N/A
Statement of Human and Animal Rights
N/A
Statement of Informed Consent
N/A
Acknowledgments
The authors would like to thank the following for their patience, insights, and guidance during the review process: Dr. Rob Ainsworth (Consultant Forensic Pathologist and Head of Specialty, NHS Lothian); Dr. Matthew Bowes (Medical Examiner, Nova Scotia); Dr. Frantisek Duska (Associate Professor and Head, Dept. of Anesthesia and Intensive Care, Charles University and FNKV University Hospital, Prague, Czech Republic); Susan Hannah (Regional Manager, Scotland Organ Donation Services Team, NHS Blood and Transplant); Jim Mohr (Associate Director, Deceased Donation, Canadian Blood Services); Marco Raggi (Manager, Surgical Recovery Services at Trillium Gift of Life Network); Dr. Karen Schiff (Regional Supervising Coroner, Ontario); Dr. Amar Singh (Coroner, Ontario); Phil Walton (Project Lead for Organ Donation Legislation Implementation, NHS Blood and Transplant); and Dr. Andrew Williams (Forensic Pathologist, Ontario Forensic Pathology Service). The authors would also like to thank the Canadian Donation and Transplantation Research Program for their support.
Author Contributions
Mackenzie Cullip contributed to the conceptualization, methodology, analysis, and original draft of the article. Aimee Sarti, Matthew Weiss, and Heather Whittingham contributed revisions to the methodology and edited the manuscript. Maureen Meade contributed to the methodology, analysis, and editing, and supervised Mackenzie Cullip. All authors approve the submitted version.
Disclosures & Declaration of Conflicts of Interest
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.
Financial Disclosure
The authors have indicated that he do not have financial relationships to disclose that are relevant to this manuscript.