
Abstract
Introduction:
In order to reduce transmission of COVID-19, in March 2020 the UK national and devolved governments imposed restrictions including spatial distancing, stay-at-home orders, and travel restrictions. The aim of this study is to compare the characteristics of cases referred to the Coronial system for autopsy in the months before and during the lockdown period.
Methods:
In all, 580 autopsy cases, performed in the London area between January and June 2020 were included in the study.
Results:
In the postlockdown period, there was an increase in the proportion of black individuals referred for autopsy, which just attained statistical significance (p = 0.047). The proportion of decomposed bodies submitted for examination was significantly increased (p = 0.011). The study did not show a significant increase in the proportion of out-of-hospital (community) deaths, traumatic deaths, or deaths due to alcohol or drug abuse or overdose.
Conclusion:
The study shows no evidence that COVID-19 preventative measures led to a change in the causes of death referred to the Coroner, except, of course, for COVID-related deaths. The proportion of black people among subjects for autopsy increased, probably because of a relatively higher incidence of COVID deaths among this group. Decomposed subjects were more common, probably due to social isolation.
Introduction
The novel coronavirus SARS-CoV-2 that causes COVID-19 reached the United Kingdom in late January 2020 (1). On March 23, 2020, the UK government imposed a stay-at-home order banning nonessential travel and contact with other people, restricting its citizens to one period of outdoor exercise per day, and shutting businesses deemed nonessential, public indoor (and some outdoor) spaces, schools, universities, and places of entertainment (2). Those with symptoms of COVID-19—persistent cough, fever, and breathlessness—were told to self-isolate, while those with serious health problems were told not to leave their homes. The police were given emergency powers to enforce these measures. There were concerns that the raft of restrictions, known as lockdown, would have an adverse effect on the population’s mental and physical health and lead to an increase in suicide (3). Rates of loneliness during the first months of lockdown were, not surprisingly, reported as high (4). On the other hand, failure to contain the virus might have overwhelmed the critical care facilities of the National Health Service, had not lockdown significantly reduced COVID transmission (5).
On March 5, 2020, COVID became a notifiable disease in England. By May 2020, the daily total of new cases of COVID-19 was falling, and in June a gradual easing of lockdown began. The cumulative total to July 3, 2020, of cases in which COVID was mentioned on the death certificate was 50,139 (6). By this time there had been 286,051 serologically confirmed cases (using polymerase chain reaction (PCR) tests, as lateral flow tests were not then available) and there had been 40,836 deaths within 28 days of a positive test (7). There were concerns that the excess deaths could overwhelm the Coronial autopsy service, as autopsies are likely to be arranged by the Coroner in many cases where the deceased’s hospital clinician or general practitioner is unable to complete a death certificate (8). From early April 2020, specialist groups called Pandemic Multiagency Response Teams (PMART), made up of police officers, firefighters, and health services staff, were formed to attend deaths in the community deemed likely to be due to COVID. They were authorized to pronounce life as extinct, confirm the deceased’s identity and establish there were no suspicious circumstances, after which the cause of death could be registered as COVID-19 infection without further examination (9).
During the first two months of lockdown, there were some 50,000 excess deaths in England and Wales, of which 38,000 were confirmed COVID. The remaining 12,000 may have been due to undetected COVID, at a time when PCR testing was not always readily available, or to unrelated conditions (10). There was speculation that health care avoidance during the pandemic could lead to deaths from conditions that would previously have been successfully treated by general practitioners or National Health Service hospitals (11). A preliminary study of 67 autopsy cases from England suggests that reduced access to health care may have contributed to a minority of excess deaths (12), though its author recommended a more extensive analysis of autopsy reports post-COVID to assess whether preventable deaths occurred due to a lower take-up of health care services.
The aim of this study is to compare the characteristics of autopsy cases in the London area in the first three months of lockdown with those of the period immediately before, particularly with regard to age, sex, ethnicity, cause of death, place of death, and degree of decompositional change.
Materials and Methods
The study sample comprises all Coronial autopsy cases examined by Convit House Pathology Ltd, an independent provider, between January 2, 2020, and July 3, 2020, in total 580 cases. All these cases were referred to Coroners in the London area North of the River Thames, who requested postmortem examinations to be carried out by our pathologist to determine the cause of death. The indications for referral of a case to the Coroner in England are that death was believed to be due to trauma, accident, suicide, poisoning, industrial disease, abortion, surgery, or medical intervention; or, that no doctor could complete a medical certificate of the cause of death, or that the offered cause of death had been disputed. The cases in this study do not include forensic examinations requested by the police in cases where death was suspected to be the result of malfeasance. Medical histories were obtained from the Coroner’s office in each case, supplemented in some cases by information from the deceased’s general practitioner. Hospital notes were consulted for those patients who died in hospital. All examinations were performed by the same consultant pathologist.
In the United Kingdom, standard Coronial autopsies are undertaken to determine the medical cause of death, and the examination is limited to that necessary to do so: typically opening the body cavities and head and dissecting the major organs (13). Histological and toxicological examination is performed if required to confirm the cause of death, or on the instructions of the Coroner. Histology/toxicology was performed in 10% and 26% of cases, respectively. In the postlockdown series, COVID-19 was offered as the medical cause of death based on findings of oedema and hyperaemia in the lungs at autopsy, in the setting of an appropriate history of symptoms including shortness of breath and pyrexia and in the absence of other significant pathology liable to have caused death. Serological testing was not generally available for postmortem cases in England during the period of this study.
Body mass index was calculated from measurements and weights obtained postmortem. Ethnicity was estimated by the pathologist based on external appearances and information supplied by the Coroner’s office. Where a cause of death could be offered, it was classified for statistical purposes according to the organ system containing the pathology considered to be the primary cause of death. The causes reported are taken from the medical cause of death offered by the pathologist, sometimes after discussion with the Coroner, and do not necessarily reflect the Coroner’s determination at inquest, however, in no case was the pathologist notified of any discrepancy.
Continuous Gaussian variables were reported as means with standard deviation (SD). Pearson’s chi-square test was used to compare variables between groups. Statistical significance was defined as a two-sided p value of <0.05.
Results
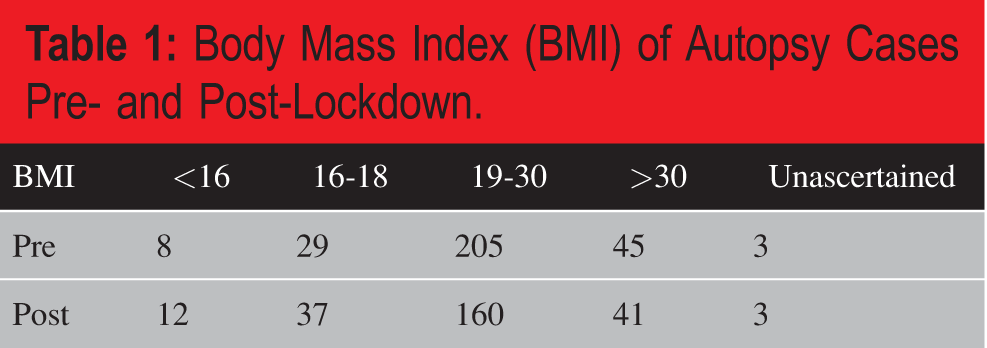
The pre- and post-lockdown series each comprised 290 sequential cases. The average age prelockdown was 62.3 years (SD 19.0 years), and the average age postlockdown was 63.2 (SD 18.7 years). The male:female ratio was 1.87:1 prelockdown and 2.11:1 postlockdown. There was no significant difference in body mass index (BMI) between the two groups ( Table 1 ).
Body Mass Index (BMI) of Autopsy Cases Pre- and Post-Lockdown.
There was an increase in the proportion of individuals referred for autopsy postlockdown who were black (23% vs 17%); this just attained statistical significance. There was a reduction in the proportion of Caucasians ( Table 2 ).
Ethnicity of Autopsy Cases Pre- and Post-Lockdown.

a Chi-square 0.049.
b Chi-square 0.047.
There was no significant difference in the place of death between the two groups: the proportion of hospital deaths was less postlockdown, but this was not statistically significant.
There was no significant difference in the causes of death classified according to major organ system ( Table 3 ). As expected, there was an increase in deaths due to respiratory tract infection, though this did not achieve statistical significance.
Causes of Death Pre- and Post-Lockdown According to Organ System.

There was no significant change in the proportion of unnatural deaths ( Table 4 ), the proportion of deaths to which alcohol (ethanol) was deemed to have contributed, or in the number of deaths from pulmonary emboli (4 in each group).
Types of Unnatural Death Pre- and Post-Lockdown.

Postlockdown, there were 23 deaths attributed to COVID-19 infection, of which, four subjects were obese (BMI > 30), 16 were male, 11 black, 10 Caucasian, and 2 Asian. The mean age was 62.2 years (SD 21.5); 48% of individuals who were considered to have died from COVID were black, compared with 23% overall (Chi-square 0.008).
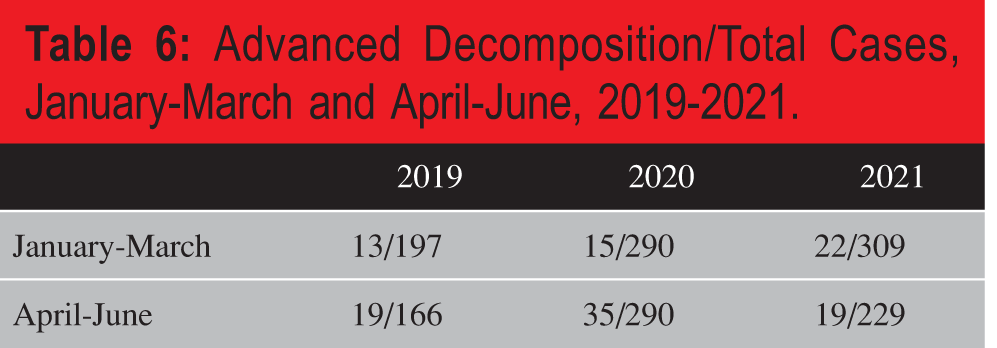
There was a statistically significant increase in the proportion of bodies showing advanced decompositional change postlockdown (5.1% pre- and 12% postlockdown, Table 5 ). In the preceding and following years, 2019 and 2021, there was also a higher proportion of bodies showing advanced decomposition in the months April to June compared with January to March, but this was not statistically significant ( Table 6 ).
Decomposed Cases Pre- and Post-Lockdown, 2020.
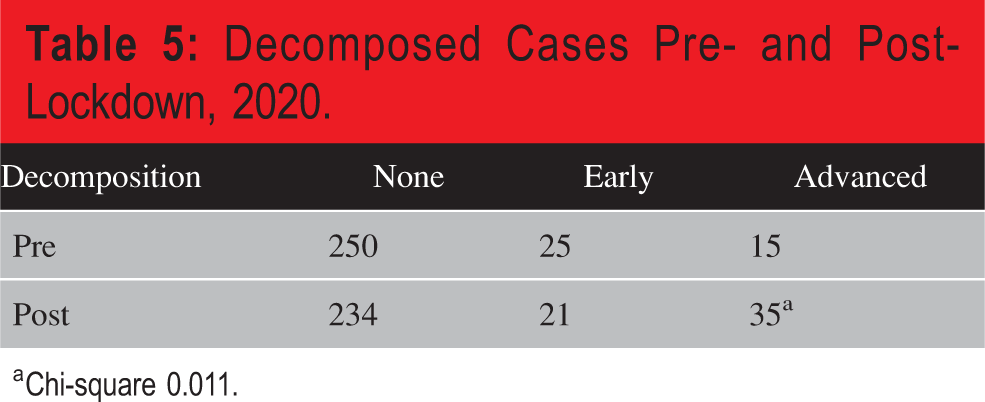
a Chi-square 0.011.
Advanced Decomposition/Total Cases, January-March and April-June, 2019-2021.
Discussion
The autopsy case mix postlockdown was similar to that pre-lockdown. There was no significant difference in age or sex, place of death or cause of death, with the obvious exception that COVID was offered as a cause of death only in the postlockdown group. The excess of males who undergo autopsy (approximately twice the number of females) is a longstanding characteristic of our Coronial practice. The possible explanations—including greater social isolation, self-neglect, and more suspicious circumstances surrounding the death of males—are, though interesting in themselves, outside the scope of the present study. There is no indication that referral practice on the part of the Coroners differed during lockdown, except that some deaths believed to be due to COVID were “signed up” by the PMART teams and so did not undergo autopsy.
The sole statistical difference in demographics of subjects for autopsy was ethnicity, where there was an increase in the proportion of individuals considered to be black postlockdown. This increase is attributable to deaths from COVID; the proportion of black people among the 23 deaths attributed to COVID was more than double that seen in deaths from all other causes, pre- and post-lockdown. Statistical data collected by the UK Government showed that, in the first wave of the pandemic, January 24, 2020, to September 11, 2020, the rate of death involving COVID-19 was highest for the Black African group (3.2 times greater than for the White British group) (14). A UK Government-commissioned report concluded that the disparity was due in part to social and economic disadvantages, though there was some evidence that genetic differences may also play a role (15). Excess deaths among black and Hispanic people during the pandemic have been reported in several Western countries (16).
That there was no significant increase in the proportion of deaths due to respiratory tract infection is explicable by the fact that COVID-19 deaths were often not referred for postmortem examination, as the Pandemic Multi-Agency Response Teams were able to certify death in cases where the history and circumstances were consistent with COVID-19 infection (17).
Thromboembolic episodes are reported to have increased due to complications of COVID infection and, rarely, vaccination (the AstraZeneca vaccine was implicated) (18). Up to 7% of hospitalized patients were reported to experience thromboembolic complications within 90 days of infection, though apparently no deaths in 61 cases were attributed primarily to thrombotic complications (19). Unusual types of thrombotic events associated with SARS-CoV-2 vaccines were widely publicised in the United Kingdom, despite being very rare events (less than one per million doses) (20). Clearly, the present study was too small to detect uncommon thrombotic events.
There was a statistically significant increase in the proportion of subjects showing advanced decompositional change, postlockdown. This was probably due in part to a seasonal increase in decomposition in the warmer months of April to June compared with January to March, however, the difference was not statistically significant in the years either side of lockdown, the greater difference in 2020 being most likely due to delays in discovering the deceased. This was probably responsible for the small, though not statistically significant, increase in the number of cases in which a cause of death could not be identified. This confirms a previous, smaller study of autopsies in the London area during the pandemic, in which the authors proposed advanced postmortem change as a surrogate marker for social isolation (21).
There was no detected increase in deaths due to trauma or drug overdose, and no increase of deaths in which alcohol was deemed to have played a significant part.
Conclusion
In the London area post-COVID, the proportion of black people among cases referred for autopsy increased, probably due to a higher incidence of COVID-related deaths among this group. Decomposed subjects were also more common, probably due to social isolation because of the restrictions on movement imposed by the government. There is no evidence from these data that the introduction of lockdown was followed by an increase in deaths from trauma, overdose, or alcohol-related causes. Overall, causes of death were not significantly different, as the proportion of COVID-related deaths among the workload was small.
Footnotes
Ethical Approval
NA.
Statement of Human and Animal Rights
NA.
Statement of Informed Consent
NA.
Disclosures & Declaration of Conflicts of Interest
The author, reviewers, editors, and publication staff do not report any relevant conflicts of interest.
Financial Disclosure
The author has indicated that he does not have financial relationships to disclose that are relevant to this manuscript.