
Abstract
Aims
Suicide by hanging remains a common modality of death across the globe. Despite this, the reported incidence of laryngohyoid fractures in suicidal suspensions remains widely varied across the current literature. This audit was conducted to benefit from a single institution's standard method of practice, coupled with a sufficiently large enough data set, to draw better conclusions on the incidence of laryngohyoid fractures in such cases and any predicting variables.
Method
Autopsy records for a total of 12 years from January 2011 to May 2023 were examined to identify cases of suicidal hanging and determine the laryngohyoid fracture incidence. A range of subsequent data relating to the deceased, the ligature, the suspension and post-mortem findings were recorded and statistically analysed to identify significant variables associated with the presence of such fractures.
Results
A total of 383 autopsy reports were included. Overall incidence of any laryngohyoid fracture was 59.3%. Thyroid and hyoid fractures were found in 51.4% and 29.2% of these cases, respectively. The most common fracture pattern was fractures of the bilateral superior thyroid horns. Significant associations between fracture incidence and the following variables were identified: ligature type, ligature mark, petechiae, age and height.
Conclusion
This audit highlights the ligature as a potential important predictor in the presence of laryngohyoid fracture. There is a relative paucity of information relating to the ligature used and the incidence of fracture. Future efforts should be focused on prospective and standardised collection of data, with particular focus on the ligature type.
Keywords
Introduction
Suicide remains a common manner of death, accounting for 10.7–13.9 deaths per 100,000 deaths across the UK.1–3 Although global suicide rates appear to be falling, 4 rates in the UK have remained largely static for the past two decades. 1 The most common method of suicide in England and Wales remains hanging, strangulation or suffocation; these accounted for 59.7% of all suicides in 2022. As a proportion of all suicide deaths across the UK, these methods have increased over the past decade.1–3 While firearms remain the most common modality of suicide in the USA, suffocation including hanging accounts for a significant proportion (24.37%) of suicides. 5
Hanging is defined as the act of wholly or partially suspending one's person from a ligature with the intention of causing death via compression of the structures of the neck.6–8 Although classified as a mechanical form of asphyxiation, the exact mechanism of death by hanging is debated. Possible causes of death include: compression of cervical arterial flow resulting in cerebral hypoxic injury; venous congestion in the head resulting from compression of the jugular veins; airway obstruction from pharyngeal occlusion by elevation of the tongue and larynx or neurogenic reflex vagal cardiac arrest following stimulation of the carotid baroreceptors.7,8 In the cases of long-drop hangings, classically seen in judicial executions, the mechanism of death may be fractures of upper cervical spine and subsequent damage to the spinal cord; these types of hanging are rare, but not unheard of, in cases of suicide.
Classically reported post-mortem findings upon external examination of suicidal hangings include: venous congestion and oedema in the head and neck; the presence of petechiae (often on tarsal plates, conjunctiva or oral mucosae) above the level of compression; abnormal fluidity of blood with right-sided cardiac congestion and cyanosis. 7 It is worth noting, however, cyanosis and right-sided cardiac congestion are not considered reliably recognisable features in modern pathology practice, despite their frequent listing in textbooks. Signs can develop within seconds following the application of fatal pressure to the neck or can be completely absent.7,8 However, such findings are not specific to suspension.7,9
Internal examination at autopsy in such cases can reveal haemorrhage to the strap muscles of the neck and often fractures of the laryngohyoid structures as well. Recent meta-analysis suggests the rate of fracture to be around 37.5% (including cervical fractures) 9 ; however, the reported incidence of fractures varies greatly from 7.6 to 72.5%.10–17 In comparison, the cricoid cartilage remains almost invariably uninjured in suicidal hangings.11,12 Heterogeneity in the reported incidence has been suggested to be down to methodology, especially with regard to the accuracy of retrospective studies in comparison to prospective9,18; however, Wilson et al 9 found this did not impact upon fracture incidence.
Another source of variation in reported incidence may well be linked to the lack of standardised approach to autopsy in these cases, as well as a lack of appreciation of the need for invasive examination.10,19 Variation in practitioners is commonplace. Further, with the emergence of post-mortem computed tomography (PMCT) as a non-invasive alternative to traditional autopsy, it is increasingly common for histopathologists to forgo detailed internal examination of the deceased, let alone detailed analysis of the neck with reflection of the infrahyoid musculature following appropriate drainage of blood. Differing local standard practice may be related to: time and monetary constraints; the availability of personnel and the availability of post-mortem imaging. Regardless, the varying standard of autopsy examinations likely influences the accuracy of fracture incidence. Given the standard technique employed in the department, our aim was to audit our own practice to ascertain the rate of laryngohyoid complex fractures.
Method
The Forensic Pathology Unit, given its nature as a forensic training institution, has an advantage for studying deaths by hanging through post-mortem examinations. As a standardised approach, all autopsies performed in the department's two mortuaries (whether suspicious or non-suspicious) receive detailed, forensic external and internal examination. Internal examination compromises Y incision with an in situ, layered neck dissection, with exposure of the hyoid bone and larynx. An audit of the unit's previous autopsy investigations from a period of over 12 years in the Liverpool region was carried out. The standardised examination, over a period of many years, will help to produce an accurate fracture incidence and also allow for the detection of significant patterns or associations between certain variables and the presence of laryngohyoid fractures. These patterns could provide more robust evidence in cases of death involving suspension in any medicolegal system of death investigation.
The Forensic Pathology Unit's autopsy register was manually searched from the period beginning January 1, 2011 to the May 31, 2023. This included both routine Coronial and forensic autopsies performed on behalf of police forces. Any post-mortem report where suicidal hanging was recorded as the cause of death in either parts Ia, Ib or Ic was included, as per the International Classification of Diseases. Those where hanging was included in part II were excluded. A list of both completed and provisional post-mortem reports were collated and subsequently located in the post-mortem database and read in their entirety by either EJW or EM. The nature of death was confirmed as suicide during this process; those reports which provided insufficient information on the discovery of the body or examination of the scene were excluded. On the occasion of a post-mortem report being inaccessible (for whatever reason, eg, sealed by the Home Office), the report would be excluded from the study.
All cases had undergone full layered neck dissection at autopsy, following vascular decompression and drainage in order to avoid artefactual cervical haemorrhages.
The minimum dataset from the post-mortem reports were gathered into a spreadsheet, including the following factors:
Post-mortem interval (PMI) in days Body condition (fresh/embalmed/decomposing*) Age (years) Gender (male/female) Height (centimetres) Weight (kilograms) Body mass index (BMI) Degree of suspension (full/partial/unspecified) Suspension/knot location on the neck (anterior/right anterolateral/left anterolateral/right lateral/left lateral/right posterolateral/left posterolateral/posterior/unspecified) Provision of ligature along with deceased (present/absent/unspecified) Ligature type** Type of knot used (fixed knot/slipknot/unspecified) Ligature mark formation (circumferential/with gap/unspecified)*** Nature of the ligature mark (rising/horizontal/unspecified) Anterior width of the ligature mark (centimetres) Relation of the mark to the laryngeal prominence (superior to/inferior to/overlying/unspecified) Presence of facial petechiae (sparse/multiple/none/unspecified) Presence of conjunctival petechiae (sparse/multiple/none/unspecified) Presence of oral petechiae (sparse/multiple/none/unspecified) Presence of other neck marks eg scratches (present/absent/unspecified) Presence of haemorrhage within the cervical strap muscles (present/absent/unspecified) Presence and location of hyoid bone fractures (right side/left side/bilateral/none) Presence and location of thyroid cartilage fractures:
Superior horn fracture (right/left/bilateral/none) Laminal fracture (right/left/bilateral/none) No fracture Presence and location of cricoid cartilage fractures (present/absent) Presence of bleeding around the laryngohyoid fractures (hyoid only/thyroid only/hyoid and thyroid/minimal bleeding/fracture but no bleeding/no fracture and no bleeding/unspecified)
*Cases were classified as ‘decomposing’ if the body condition had deteriorated to the point where examination of the soft tissues was impeded or impossible. Cases in the early stages of putrefaction, such as marbling, bloating and discolouration, were classified as ‘fresh’, if the soft tissues could still be examined and the post-mortem report reflected this.
**Ligature type was grouped into various categories: bedsheet, belt, cable, clothing/fabric, cord, dog lead, dressing-gown cord, necktie, rope, scarf, shoelace, strap and miscellaneous. The minimum number of ligatures for a single category was 5. If there were fewer than five cases where a specific ligature type was used, these cases were included in the category ‘miscellaneous’. The miscellaneous ligatures included: bandage, bike lock, blanket, ribbon, hosiery, wire, curtain, hosepipe, shower curtain, cable ties or chain. In three instances two types of ligature were used, these were also classified as miscellaneous.
***A gap in the ligature mark was demonstrative of a looser ligature, causing an ‘inverted V’ mark on the neck, in contrast to the continuous circumferential mark encircling the entire neck which would be caused by a tighter ligature.
For the purposes of analysis, for some of the categories above, data was recorded as ‘unspecified’. This was due to a variety of reasons, including the data was absent in the post-mortem report; there was a lack of clarity in the post-mortem report or decomposition of the body had obscured the autopsy findings. For any unclear data, both EJW and EM had to be in agreement on the final entry onto the dataset.
Statistical analysis was performed using Chi-squared, Kruskall–Wallis, Unpaired t-test, Mann–Whitney U and one-factor ANOVA tests using StatsDirect statistical software package by VS, significance level was set as P < 0.05.
Results
A total of 383 post-mortem reports were included according to the above criteria. Of these, 299 were male (78.1%) and 84 were female (21.9%). The ages of the deceased ranged from 12 to 86 years, with a mean age 41 years (median age 41 years). The PMI ranged from 0 to 32 days, with a mean interval of 4.7 days. The mean BMI for these cases was 24.1, ranging between 13.8 and 42.0.
No laryngohyoid fracture was found in the autopsies of 156 (40.7%) cases. 109 (69.9%) of these cases were male, and 47 (30.1%) were female. The age of these deceased ranged from 12 to 70 years, with a mean age of 35 years (median age of 32 years). PMI ranged from 0 to 30 days, with a mean interval of 4.7 days. The mean BMI for these cases was 23.9, ranging from 15.1 to 42.0.
About 227 (59.3%) cases were identified as having at least one fracture; either the hyoid bone, the thyroid cartilage or the cricoid cartilage alone, or any combination of these fractures. About 190 of these cases were male (83.7%), and 37 (16.3%) were female. The ages of these deceased ranged from 14 to 86 years, with 45 years being both median and mean age. PMI ranged from 0 to 32 days, with a mean post-mortem interval of 4.7 days. The mean BMI for these cases was 24.2, with a range of 13.8 and 38.9.
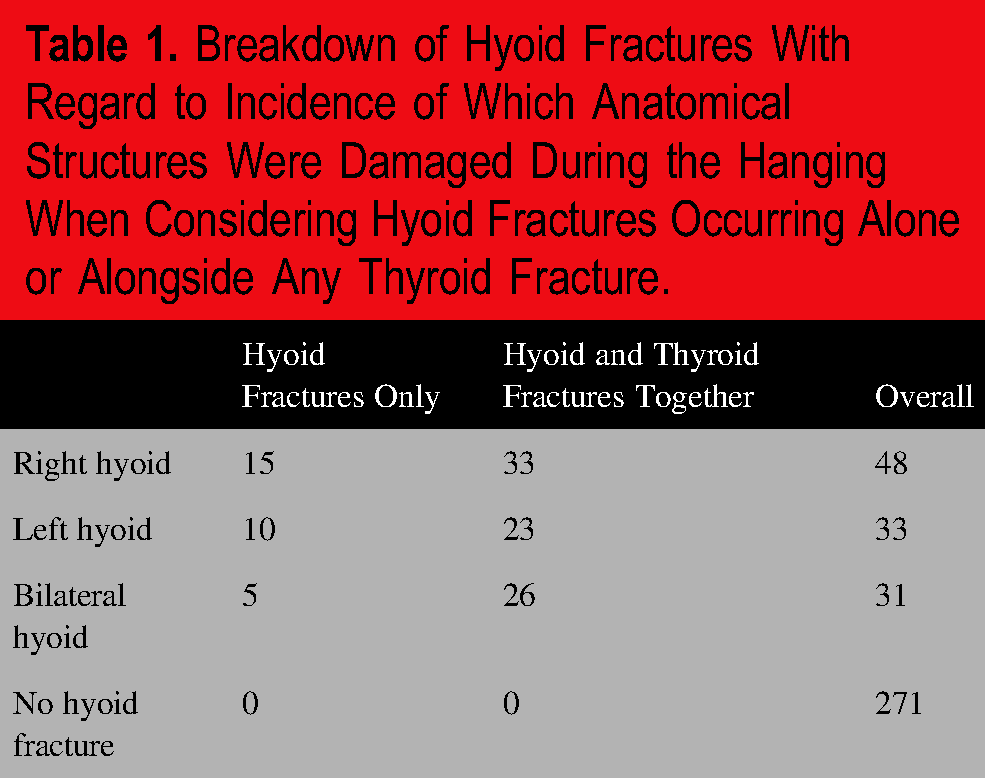
Of the 227 cases where a fracture was identified, 30 (13.2%) of these fractures were located in the hyoid bone only, 114 (50.2%) in the thyroid cartilage only and 82 (36.1%) cases sustained both hyoid and thyroid fractures. Only a single cricoid fracture was reported, which occurred alongside thyroid cartilage fractures. No individual demonstrated all three fractures. Tables 1 and 2 show the breakdown of fractures sustained, and Figures 1 and 2 demonstrate these visually.

Breakdown of Proportions of Which Anatomical Regions of the Hyoid Bone Were Fractured When Looking at Each of the Total 383 Cases in This Study.
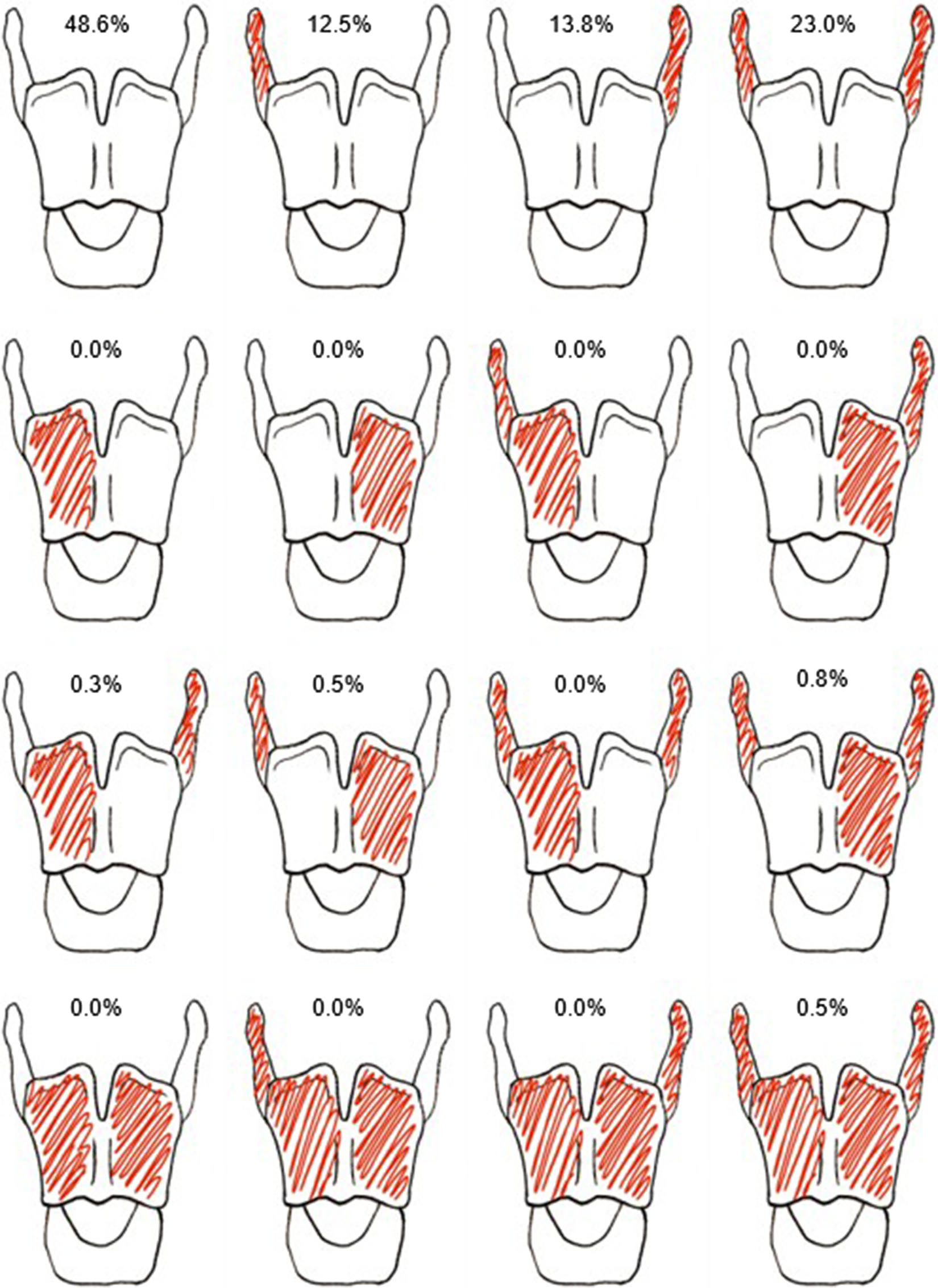
Breakdown of Proportions of Which Anatomical Regions of the Thyroid Cartilage Were Fractured When Looking at Each of the Total 383 Cases in This Study.
Breakdown of Hyoid Fractures With Regard to Incidence of Which Anatomical Structures Were Damaged During the Hanging When Considering Hyoid Fractures Occurring Alone or Alongside Any Thyroid Fracture.
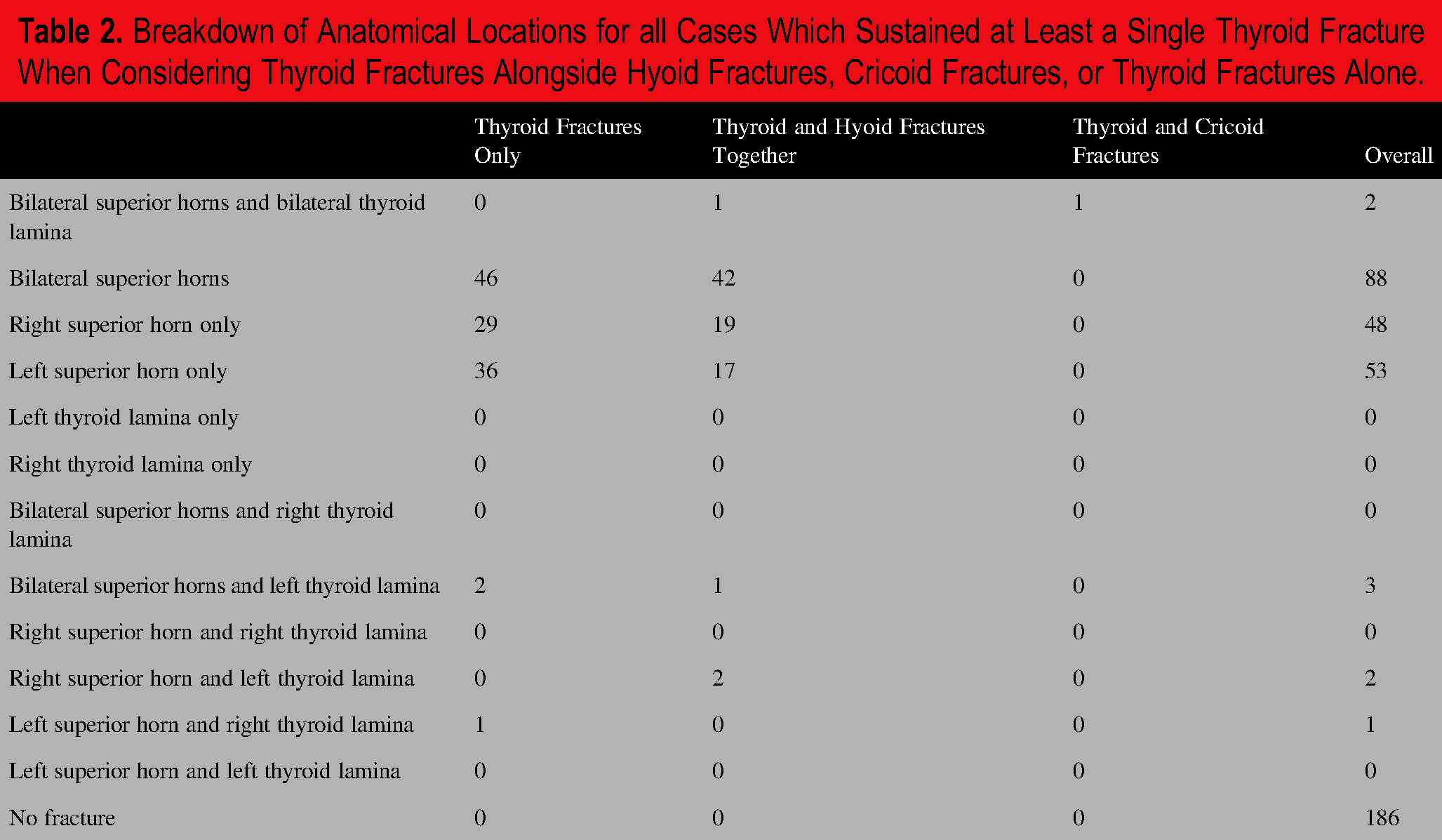
Breakdown of Anatomical Locations for all Cases Which Sustained at Least a Single Thyroid Fracture When Considering Thyroid Fractures Alongside Hyoid Fractures, Cricoid Fractures, or Thyroid Fractures Alone.
Statistical comparison was made between those who sustained any laryngohyoid fracture against those who did not sustain any fracture. This was performed alongside comparisons between different combinations of fractures (Hyoid only, Thyroid only, Thyroid and Hyoid combined and Thyroid and Cricoid combined) and the absence of fracture. The results are demonstrated in Table 3 , examining factors relating to the individual deceased, and Table 4 , examining factors relating to the ligature and suspension.
Comparison of Variables Relating to the Individual Deceased's Body.
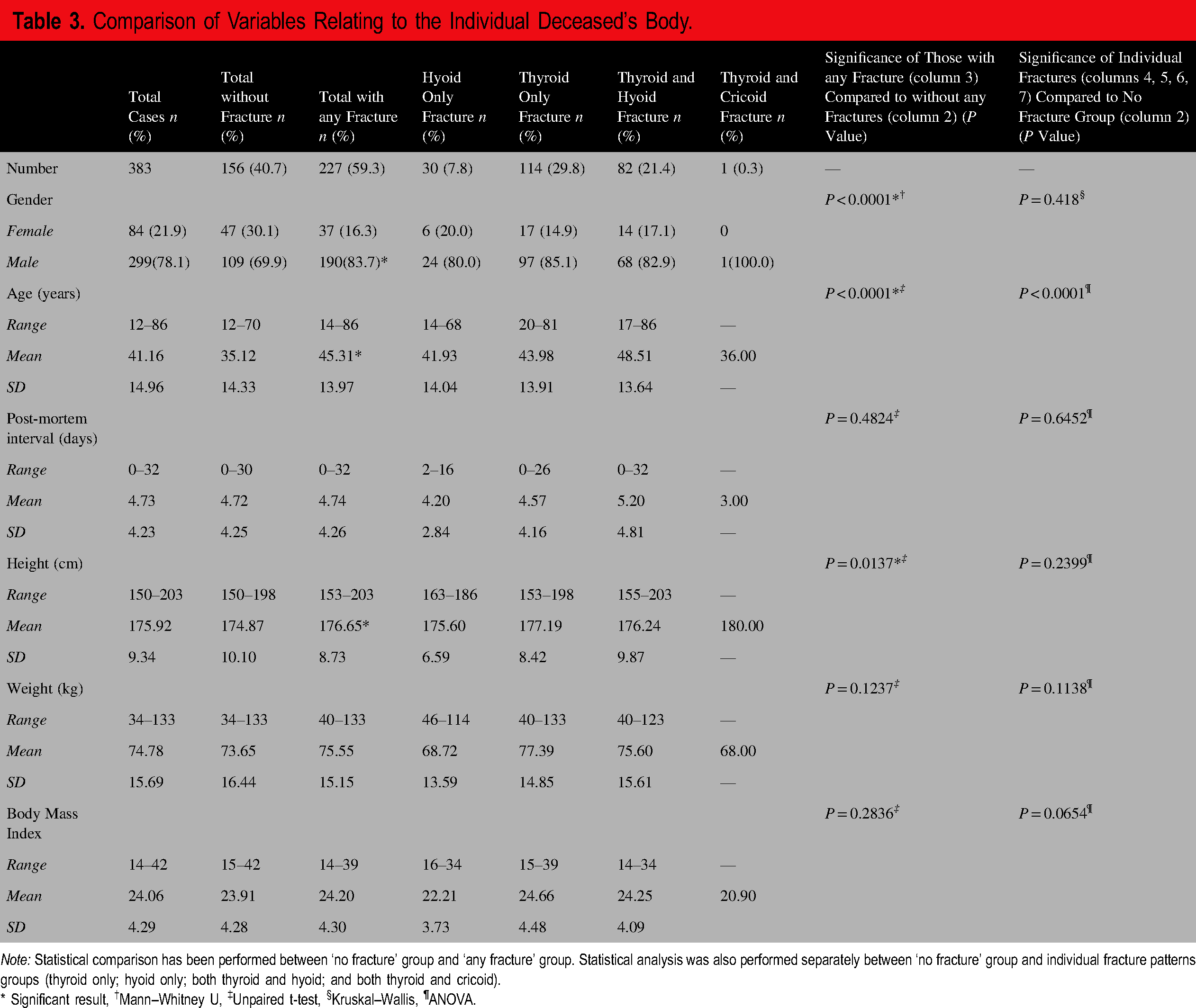
Note: Statistical comparison has been performed between ‘no fracture’ group and ‘any fracture’ group. Statistical analysis was also performed separately between ‘no fracture’ group and individual fracture patterns groups (thyroid only; hyoid only; both thyroid and hyoid; and both thyroid and cricoid).
* Significant result, †Mann–Whitney U, ‡Unpaired t-test, §Kruskal–Wallis, ¶ANOVA.
Comparison of Variables Relating to the Ligature and Circumstances of Death.
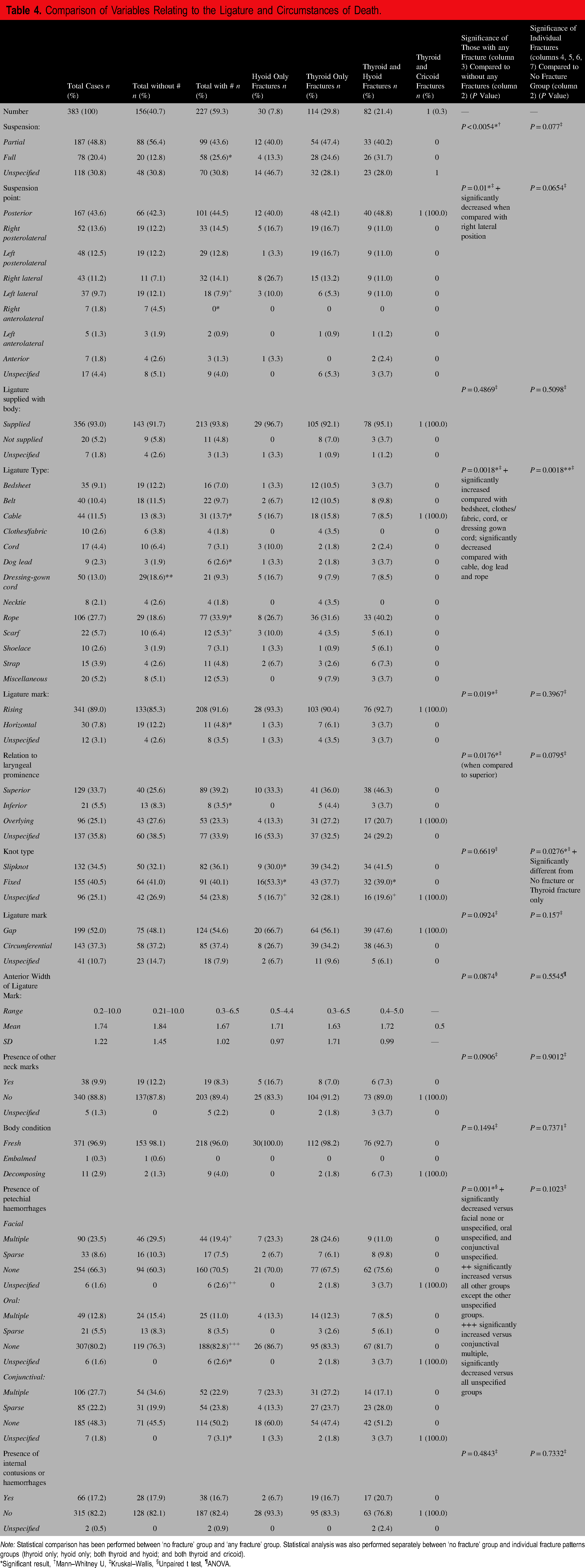
Note: Statistical comparison has been performed between ‘no fracture’ group and ‘any fracture’ group. Statistical analysis was also performed separately between ‘no fracture’ group and individual fracture patterns groups (thyroid only; hyoid only; both thyroid and hyoid; and both thyroid and cricoid).
*Significant result, †Mann–Whitney U, ‡Kruskal–Wallis, §Unpaired t test, ¶ANOVA.
When comparing the presence of any fracture against no fracture, statistically significant results are as follows: mean age and height were statistically higher in those sustaining any fracture. With regard to the type of hanging, cases of full suspension were found to have a higher laryngohyoid fracture rate than cases of known partial suspension or those where suspension type was not clear within the report. With regard to the suspension point, if it was located on the right side anterolaterally, then laryngohyoid fractures did not occur. Furthermore, if the suspension point was located on the left side laterally, there was a reduced rate of fractures when compared to all other suspension points excluding right anterolateral. When considering the type of ligature, it was found that there was an increased rate of laryngohyoid fracture when either a cable, dog lead or rope were used. The use of a scarf as a ligature was associated with an intermediately increased rate of fracture: the rate of fracture was lower than when the aforementioned three ligature types were used, but higher than the remaining ligature types. With regard to the ligature mark, a flat mark around the neck was associated with a decreased rate of laryngohyoid fracture, as was a ligature mark lying inferiorly to the thyroid prominence.
When comparing individual fracture patterns against those sustaining no laryngohyoid fracture, dressing gown cords were significantly less likely to be associated with fracture. Interestingly, when rope is used as the ligature, the hyoid is less likely to be fractured alone. It is more likely that either no fracture occurs, or the thyroid is fractured in isolation or in combination with the hyoid.
In this study, petechial haemorrhages displayed a complex pattern which was difficult to ascertain any meaningful results. As a result, we conducted a separate analysis comparing the presence of any location and any degree of petechiae against the type of suspension. We also compared presence of any petechiae against the presence of any fracture. For this analysis any case too decomposed (seven in total) were included under no petechiae present. We found the presence of any petechiae were more likely to be seen with partial suspension than in full suspension (Chi-squared = 25.7698, P < 0.00001). Petechiae were less likely to be seen when no fracture was present but this was a small effect (Chi-squared = 4.2855, P < 0.05). The data for this can be found in the Supplemental Materials (Tables 5 and 6, respectively).
Discussion
The demographics of the deceased show a majority male population with the average age in the fifth decade, which is broadly equitable with other studies.10–15,20–25
Incidence of Varying Laryngohyoid Fractures
With regard to the laryngohyoid fractures that were reported, we found that there was no statistical significance between the locations of fractures and their combinations within the laryngeal skeleton. As noted by Wilson et al, 9 the large variation in fracture patterns renders this little help in predicting death by hanging.
Similar to several other studies, we found that fractures of the thyroid cartilage, specifically the superior horns, were the most common in the laryngeal skeleton of suicidal hangings.10,13–17,19,20,22,26 Although there is no agreement in the current literature, there are several other studies finding equal incidence of both hyoid and thyroid fractures, or indeed a higher incidence of hyoid fractures.12,18,23,24 The most common singular fracture among all that were detected was the left superior horn of the thyroid cartilage, which was fractured in 147 (38.4%) of our 383 total cases, and present in 64.7% of the 227 cases where any fracture or combination of fractures were identified. The second most common singular fracture among all that were detected was the right superior horn of the thyroid cartilage, which was fractured in 143 (37.3%) of our 383 total cases, and present in 63.0% of the 227 cases where any fracture or combination of fractures were identified. The third and fourth most common singular fractures were the right side of the hyoid bone and the left side of the hyoid bone, respectively. The right side of the hyoid bone was fractured in 79 (20.6%) of our 383 total cases, and present in 34.8% of the 227 cases where any fracture or combination of fractures were identified. The left side of the hyoid bone was fractured in 64 (16.7%) of our 383 total cases, and present in 28.2% of the 227 cases where any fracture or combination of fractures were identified.
Hyoid fractures were present in 112 (29.2%) of our 383 cases; of all of the hyoid fractures, 82 (73.2%) were found alongside thyroid fractures. The hyoid bone was most commonly fractured on the right side (12.5%), followed by the left side (8.6%), and lastly bilaterally.
Thyroid fractures were present in 197 (51.4%) of our 383 cases; of all of the thyroid fractures, 82 (41.6%) were found alongside hyoid fractures and one (0.5%) was found alongside a cricoid fracture only. The most common thyroid fracture combination was bilateral superior horns (23.0%), followed by left superior horn only (13.8%), and then right superior horn only (12.5%). Other combinations of fractures either made up <1.0% of all of the thyroid fractures detected or were not reported at all. Laminal fractures (on either side of the thyroid cartilage, and with or without other thyroid fractures) were present in only seven (3.6%) of all of the combinations of thyroid fractures.
We found that a cricoid fracture was a rare finding in suicidal hangings, with many studies also finding them extremely rare, if not entirely absent.10,11,14–17,19,22,26 A single cricoid fracture was noted out of 383 cases included in the audit. The case in question was that of a 36 year-old male with a BMI of 20.9. The body was found in a decomposed state. It was unclear whether the suspension was partial or full, but the knot was positioned posteriorly. The ligature was a cable tied into a running knot, with the corresponding ligature mark lying directly over the laryngeal prominence. The cricoid fracture was present alongside fractures in the bilateral superior thyroid horns and bilateral thyroid laminae. There was no fracture to the hyoid bone. It is also likely that the laryngeal structures were also decomposed and therefore collapsed over time while the body remained suspended as it deteriorated.
Relationships Between Incidence of Laryngohyoid Fracture and Factors Related to the Body
The incidence of laryngeal fracture was 59.3%, similarly to Nikolic et al 13 However, as previously stated, there is significant variation in the reported frequency of laryngohyoid structure fractures in suicidal hangings.9–12,14–17,25 We found that there was a significant increase in fracture incidence for males when compared to females (Mann–Whitney U, P < 0.0001). A similar effect of sex on the distribution of fractures has been reported.11,12,16,27 However, several other studies have found that sex is not significantly related to the incidence of laryngohyoid fractures.9,10,15,28 Bork et al 25 even found fractures to be increased in female victims. We found that gender was not significantly related to the incidence of individual thyroid or hyoid fractures, or combinations of fractures.
Age is often stated as an important variable for predicting fracture patterns. The response of the larynx to trauma suggests that harder larynges were more likely to fracture due to the decreasing elasticity of the tissue associated with age-related ossification, with incomplete fractures becoming visible over an age of 40 years in men and 20 years in women, and complete fractures beginning to occur over the age of 40 years in both genders.29,30 We found the incidence of any laryngohyoid fracture increased with age (unpaired t-test, P < 0.0001). Several other studies have reported age as a statistically important factor contributing to the incidence of laryngohyoid fractures, however, the age at which it becomes statistically significant varies.9–17,20,25,28
Perhaps surprisingly, this audit found that there was no significant correlation between weight, BMI, and the incidence of a laryngohyoid fracture. In contrast, several sources have noted a significant increase in fractures with increasing weight and BMI.10,12,16,25 We considered whether a higher BMI could mean increased adipose tissue, thereby protecting the laryngeal skeleton from the compressive forces of a ligature. We also found increasing height to be significantly associated with increasing fracture incidence (unpaired t-test, P = 0.037), similar to Clement et al. 16 Bork et al 25 has shown an increase in the incidence of hyoid fractures with increasing height, but not with thyroid fractures.
Incidence of Laryngohyoid Fractures Relating to Ligature, Ligature Mark, and Suspension
The rates of different modalities of suspension vary between studies.17,21,27,31,32 A natural conclusion may be to think fracture incidence will increase in cases of hanging found in full suspension due to the weight of the deceased's body not being supported by external factors as it is in partial suspensions. We found that the minority of cases were fully suspended (20.4%). The proportion of those sustaining laryngohyoid fractures was higher in cases of full suspension and this was statistically significant when compared to incomplete suspension (Mann–Whitney U, P < 0.0054); this is in contrast to previous works.9,10,15,16,28 However, Clement et al did find that fracture incidence significantly increased in those over the age of 40 years who were completely suspended. 16 We found no significant link between individual fracture patterns and the type of suspension.
With regard to petechial haemorrhages, we found were that there was a significant increase in fracture incidence in cases with no oral haemorrhages in comparison to cases with multiple conjunctival haemorrhages, and that there was a significant decrease in fracture incidence in cases with multiple facial haemorrhages when compared to those with no facial haemorrhages. We hypothesise this may be related to relationship between petechial haemorrhages and suspension types, whereby cases of partial suspension typically demonstrate the presence of more florid petechial haemorrhages. However, when considering the presence of any petechial haemorrhage (oral, facial, conjunctival), we found their presence was significantly associated with increased incidence of any fracture. We also found the presence of any petechiae to be significantly more likely in those who were partially suspended.
When considering ligatures, most studies either record limited information surrounding the ligature, or those that do include ligature information do not assess the incidence of laryngohyoid fracture. Both hard versus soft ligatures and wide versus narrow ligatures are reported in the literature or noted as areas of further study12,13,16,20,27,31; however, no conclusions can be drawn given the paucity of data. Wilson et al 9 note that meta-analysis of ligature width could not be performed due to variations in reporting information between studies.
We identified rope as the most common ligature type followed by dressing-gown cords. Several other studies also found rope to be the most common form of ligature used.14,17,24,31,33 Often a wide array of ligatures is reported and this was commensurate with our data.17,24,27,31,33,34 When observing ligature types, it was found that the following materials were associated with a significant increase in fracture incidence compared to all other ligature types: cables, dog leads and ropes. Scarves were also associated with an increase in fracture incidence but only in comparison to the ligature types other than cables, dog leads and ropes. James and Silcock found that fractures were less likely to occur with a soft ligature. 14
When used as a ligature, rope was less likely to injure the hyoid in isolation. Indeed, it either predicted no injury at all, or either an isolated thyroid, or combined laryngohyoid fractures; this was statistically significant (P = 0.0042). When comparing individual fracture pattern incidence, a dressing-gown cord was significantly less likely to result in fracture (P = 0.0042).
We found the majority of knot positions to be in ‘typical’ posterior placement; similarly, several other studies demonstrate the same trend.10,16,20 However, this is not always the case, with both Ambade et al 31 and Sharma et al 27 reporting posterior knot/suspension points in a minority of their cases. We chose to evaluate the point of suspension, hypothesising opposite this point the ligature would exert greater compressive forces over the neck. We found that there was a significant decrease in any fracture incidence for suspension points which were located anterolaterally on the right side when compared to all other suspension points. We also found that any fractures were less likely to occur alongside left lateral suspension points compared to the right lateral side; and when the suspension point was on the right anterolateral aspect of the neck, fractures did not occur. No other statistically significant relationships were found when observing suspension points, either for any or individual laryngohyoid fracture patterns. Kurtulus et al 15 found that a posterior knot position was significantly associated with incidence of fracture. Zatopkova et al 10 found that the incidence of any fracture was significantly associated with knot position, but did not find this significant when looking at individual thyroid or hyoid fractures. Bork et al 25 found there was no significant impact on fracture incidence in ‘typical’ or other types of hanging. Thyroid horn fractures have been shown to have some potential in determining lateralisation of knot position; the same authors also noted that an anterior knot position was associated with an absence of fracture in those aged above 30 years. 13 However, this study only included cases of full suspension. It is also worth noting we used eight possible points to classify knot position, while the literature commonly only categorises knot location as posterior, lateral, or anterior10,15,16,20,23; this, alongside the ambiguity as to whether a knot position is the same as a point of suspension, makes it difficult to compare our findings.
We found a fracture was significantly more likely to occur in suspensions with a rising ligature mark as opposed to those with a flat mark. Fractures were significantly less likely to occur in hangings where the ligature mark was located inferiorly to the laryngeal prominence in comparison with marks located superiorly; there was no significant relationship for marks which lay directly over the laryngeal prominence.
There was no statistical significance with regard to any fracture incidence for the following factors: width of the ligature mark, circumferential ligature marks versus those with gaps (which we used as a surrogate for tightness of the ligature), type of knot, whether or not there were other marks on the neck; and the presence of internal cervical bruising upon dissection. Clement et al 16 also found no association between fracture incidence and the width of the ligature, while Sharma et al 27 could not confirm whether or not it impacted on fracture incidence at all.
Areas for Future Research
It has been reported that the force required to break the hyoid and thyroid complex is >3.11 kg 35 and >3 kg, 30 respectively. Khoklov formulated a method of calculating load in partial suspension; even when the deceased is suspended prone, 9.7–18.3% of the body weight is exerted as tension on the ligature. 36 In most people, this is likely to exceed the force required to fracture the laryngohyoid structures, suggesting that suspension (either full or partial) may not be of much importance in predicting laryngeal fractures. Much of the significant results were associated with the ligature; this suggests further research, ideally prospective, should focus on recording greater detail about the nature of the ligature and its material properties.
Limitations
The study is not without its limitations. Firstly, the retrospective nature of this study impacts on the information with can be ascertained. It is beyond the remit of this audit to collect detailed information about the circumstances in which individuals were found, beyond that reported in the autopsy report. For instance, it was not possible to discern whether or not there may have been a drop at the commencement of hanging in cases partially suspended. Furthermore, while autopsies mentioned some detail regarding the ligatures, a wide range of descriptions were reported and only some cases included measurements of ligatures or any estimation of possible material properties of the ligatures. We did not collect data on whether cardio-pulmonary resuscitation (CPR) had been performed and there is the possibility that this may have influenced the presence of internal neck injuries in some cases. A further limitation is the use of the presence of a circumferential mark as a surrogate for the tightness of the ligature; many factors such as the degree of suspension or the relationship of the deceased to the object used to support the ligature are likely to exert significant impact on visible marks left by the ligature. As mentioned above, there is often variation in terminology used to describe hangings and this can cause ambiguity in the literature.
Conclusion
The suggestion from this audit is that rather than focusing on factors relating to the deceased or the interaction of the ligature with the body, more research is needed concerning the nature of the ligature material being used. Perhaps inherent material properties, such as elasticity, are more important in predicting the absence or presence of laryngohyoid fractures in cases of suicidal hanging. Further prospective studies adhering to a standardised autopsy protocol are needed to overcome the heterogeneity in data across the current body of literature regarding the incidence of laryngohyoid fracture in suicidal hangings. Such studies should aim to collect greater information regarding material properties of the ligature to correlate with both external and internal examinations at autopsy. Finally, the use of histological examination following decalcification of the laryngeal skeleton could be a useful step in further exploring fracture incidence, and their distribution in suicidal hangings; with particular reference to the detection of cartilaginous and bony injuries that are not visible at gross examination.
Supplemental Material
sj-docx-1-afp-10.1177_19253621261457530 - Supplemental material for An Audit Into the Incidence of Laryngohyoid Fractures in Suicidal Hangings
Supplemental material, sj-docx-1-afp-10.1177_19253621261457530 for An Audit Into the Incidence of Laryngohyoid Fractures in Suicidal Hangings by Edward J. Willcocks, BDS (Hons), MBChB, Ellie Mercala, BSc, MBChB, Vijay Sharma, BScHons, MBChB, PhD, FRCPath, Aaron Borbora, BM BCh, MA, MRCS, FRCPath, and Matthew S. Lyall, MBChB, FRCPath, DMJ in Academic Forensic Pathology
Footnotes
AUTHOR CONTRIBUTIONS
Edward J. Willcocks: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, writing – original draft and writing – review and editing. Ellie Mercala: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, writing – original draft and writing – review and editing. Vijay Sharma: conceptualisation, data curation, formal analysis, methodology, writing – original draft and writing – review and editing. Aaron Borbora: conceptualisation, methodology and writing – review and editing. Matthew S. Lyall: conceptualisation, methodology, project administration, supervision and writing – review and editing.
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
ETHICAL APPROVAL AND INFORMED CONSENT STATEMENT
This study was conducted as an audit and as such ethical approval is waived, ethical approval was not, therefore, expressly sought.
The authors received no financial support for the research, authorship and/or publication of this article.
SUPPLEMENTAL MATERIAL
Supplemental material for this article is available online.
AUTHORS
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.