
Abstract
Late-onset vitamin K deficiency bleeding (VKDB) remains a preventable cause of catastrophic intracranial hemorrhage in early infancy, yet continues to present complex medicolegal challenges where parental refusal of prophylactic vitamin K persists. We present four infant deaths evaluated within the Turkish medico-legal system, each lacking prophylactic vitamin K at birth, in which autopsy played a critical role in excluding alternative causes and supporting findings most consistent with VKDB. Comprehensive review of clinical records and full forensic autopsies, including neuropathologic examination, demonstrated extensive multi-compartment intracranial hemorrhage with no findings sufficient to support inflicted trauma, skull fractures, vascular malformations, metabolic disease, congenital coagulopathy, or sepsis. Coagulation studies, when available, showed markedly prolonged prothrombin time/international normalized ratio and activated partial thromboplastin time, supporting acquired coagulopathy consistent with vitamin K deficiency. In all cases, postmortem findings aligned with clinical deterioration characterized by rapidly progressive neurologic decline. The circumstances surrounding refusal of prophylaxis, delayed medical presentation, and progression to fatal hemorrhage were evaluated in the context of medicolegal responsibilities regarding caregiver decision-making and cause-of-death certification. These cases underscore the critical role of forensic pathology in differentiating VKDB from non-accidental trauma and other causes of infant intracranial hemorrhage, ensuring accurate death investigation, and informing medicolegal evaluation in preventable infant deaths.
INTRODUCTION
Vitamin K deficiency bleeding (VKDB), formerly termed hemorrhagic disease of the newborn, remains a preventable but potentially fatal coagulopathy of early infancy. Its pathophysiology reflects insufficient activity of vitamin-K–dependent coagulation factors (II, VII, IX, X), a consequence of low transplacental vitamin K transfer, immature hepatic synthesis, and absence of intestinal microbiota in newborns (1–3). In the absence of prophylaxis, neonatal plasma levels of these clotting factors remain only 30%–60% of adult values, predisposing exclusively breastfed infants to severe hemorrhage (2,4,5). VKDB is traditionally classified into early, classic, and late forms; late-onset VKDB—occurring between 2 weeks and 6 months—carries the greatest risk for catastrophic intracranial bleeding and permanent neurologic injury (3,5,6).
Before universal prophylaxis programs, the incidence of late VKDB ranged from 4.4 to 10.5 per 100,000 live births and up to 80 per 100,000 among exclusively breastfed infants (6–8). The introduction of routine intramuscular (IM) vitamin K administration at birth has dramatically reduced the incidence, with countries adhering to prophylaxis protocols reporting rates as low as 0.1 to 1 per 100,000 live births (8,9). Professional bodies such as the American Academy of Pediatrics (AAP), the World Health Organization (WHO), and the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) recommend a single IM dose of vitamin K (0.5–1 mg) to all neonates shortly after birth to effectively prevent VKDB (2,9–11).
Despite longstanding recommendations, a concerning resurgence of VKDB has been noted in recent years, largely attributed to increasing parental refusal of vitamin K prophylaxis. Studies conducted in various countries, including the United States, Canada, and Australia, reveal a growing trend of refusal, driven by fears of potential side effects, a preference for “natural” childbirth approaches, and a general distrust of conventional medical interventions (12–14). Alarmingly, refusal of vitamin K administration has been closely linked with broader vaccine hesitancy patterns, raising further concerns for infant health and public health safety (13,15,16). This pattern echoes broader mistrust observed in other areas of neonatal care, particularly surrounding routine immunizations. Parental refusal is often influenced by misinformation, fear of potential side effects, and philosophical objections. Hamrick et al emphasized that these factors highlight the urgent need for structured educational interventions tailored to address these specific concerns (17).
Recent hospital-based surveillance in high-income countries has also demonstrated a measurable increase in IM vitamin K refusals among term neonates, suggesting a resurgence even in medically equipped settings (13). Vitamin K plays a crucial role in activating clotting factors II, VII, IX, and X, and its deficiency may manifest in three clinical forms: early, classic, and late VKDB. In clinical settings, the consequences of missed vitamin K prophylaxis may not manifest immediately, complicating early diagnosis and delaying appropriate interventions. In such contexts, medicolegal autopsies are indispensable for establishing the etiology of unexplained neonatal deaths. Forensic pathology plays a critical role when VKDB presents with unexpected collapse or sudden unexplained death. In these settings, autopsy findings—particularly non-traumatic intracranial hemorrhage in the absence of external injury—provide essential diagnostic confirmation and help differentiate VKDB from inflicted trauma, birth-related injury, metabolic disorders, infection-associated disseminated intravascular coagulation, and congenital coagulopathies (18–21). Given that late VKDB frequently manifests as an isolated intracranial hemorrhage without external signs of trauma, thorough neuropathologic evaluation remains indispensable in medicolegal determination of cause and manner of death.
MATERIALS AND METHODS
Study Design and Setting
This study was designed as a retrospective forensic case series based on medico-legal autopsies performed in Türkiye. All cases were identified through a systematic search of the National Judiciary Informatics System (UYAP), which provides centralized access to forensic autopsy data, hospital records, toxicology results, radiological imaging, and the official board opinions rendered by the First Specialization Board, Council of Forensic Medicine. The search was conducted within the archive of the First Specialization Board, covering the period January 01, 2009, through April 05, 2024.
Case Identification
Cases were retrieved by searching the National Judiciary Informatics System (UYAP) for key terms and phrases commonly used in medico-legal opinions concerning neonatal hemorrhagic conditions, including “K vitamini eksikliği” (vitamin K deficiency), “yenidoğanın hemorajik hastalığı” (hemorrhagic disease of the newborn), “geç hemorajik hastalık” (late hemorrhagic disease), “beyin kanaması” (intracranial hemorrhage), and “K vitamini eksikliğine bağlı yenidoğan hemorajik hastalığı.” This search yielded the complete medico-legal files for four neonatal deaths in which vitamin K deficiency was considered in the differential diagnosis. All retrieved files were reviewed in full to determine eligibility. Cases were included if (1) a complete forensic autopsy had been performed, (2) the board opinion considered VKDB to be the most likely cause of death after exclusion of alternative etiologies, and (3) relevant clinical, radiological, laboratory, and histopathological data were available. Cases in which trauma, congenital malformation, metabolic disease, or infectious etiologies could not be sufficiently evaluated due to missing data were excluded.
Data Sources and Extraction
Data were extracted from the complete medico-legal case files available in the National Judiciary Informatics System (UYAP). Each file contained comprehensive forensic autopsy reports prepared by regional morgue departments, detailed histopathological examinations of the brain and visceral organs, toxicological analyses, emergency department and hospitalization records, radiological imaging and interpretations, neonatal intensive care unit (NICU) documentation, and witness statements obtained during the legal investigation. Importantly, each case file also included the official board opinion issued by the First Specialization Board, which provided the final medicolegal assessment of cause and manner of death. All available data were reviewed by the authors to ensure accurate reconstruction of the clinical course, autopsy findings, and medicolegal conclusions.
Definitions and Classification
Cases were classified as most consistent with VKDB based on established international criteria, including the presence of intracranial or gastrointestinal hemorrhage, markedly prolonged coagulation parameters, absence of vitamin K prophylaxis at birth, correction of coagulation abnormalities following vitamin K administration (when applicable), and systematic assessment and exclusion of alternative traumatic, vascular, infectious, metabolic, and congenital causes. Late-onset VKDB was defined as hemorrhagic presentation occurring between 2 weeks and 6 months of age, consistent with international guidelines. Differential diagnoses—including non-accidental trauma, congenital coagulopathies, disseminated intravascular coagulation secondary to infection, metabolic disease, and vascular malformation—were evaluated through integration of clinical documentation, imaging studies, autopsy findings, and histopathology.
Ethical Considerations
Approval for the study was obtained from the Educational and Scientific Research Commission of the Council of Forensic Medicine (Decision No. 21589509/2024/1452; dated 03 December 2024). As the research involved deceased infants, and all analyses were performed on retrospective anonymized forensic records, the requirement for informed consent was waived. All images used in this article are derived from anonymized forensic autopsy documentation and contain no identifiable features; therefore, in accordance with institutional policy, additional parental consent for publication of figures was not required.
RESULTS
Case 1
A preterm male infant, measured 54 cm in length and weighed 4100 g, born at 30 weeks of gestation via cesarean section as the second twin of a dichorionic diamniotic pregnancy, required immediate admission to the NICU for respiratory distress management. Birth weight was 1540 g, with APGAR scores of 3 at 1 min, 4 at 5 min, and 6 at 10 min. During his NICU stay, blood cultures were positive for methicillin-resistant Staphylococcus species, prompting antibiotic therapy including vancomycin and cefotaxime. Following a 43-day hospitalization with gradual clinical improvement, the infant was discharged at a corrected gestational age of approximately 37 weeks and a discharge weight of 1890 g. Despite prematurity-related vulnerabilities, no IM vitamin K administration was documented at birth. Approximately two and a half months later, on the 56th postnatal day, the infant was presented to the hospital with swelling over the scalp and repeated vomiting after feeding. The parents stated that the facial injuries had occurred while the child was playing with their co-twin. Laboratory tests revealed a hemoglobin level of 7.0 g/dL, hematocrit of 19.3%, platelet count of 420 × 103/μL, and an unmeasurable prothrombin time (PT), indicating severe coagulopathy. Management included the administration of two 10 cc/kg doses of fresh frozen plasma (FFP) and 3 mg of IM vitamin K. Chest radiography showed pleuroparenchymal consolidation in the right lung, suggestive of pneumonia. Despite being informed of the medical risks, the parents insisted on discharge against medical advice, signing a written refusal form on the 62nd postnatal day. Later that evening, the infant was brought back to the emergency department and was declared dead on arrival. Postmortem external examination revealed a 10 cm subcutaneous hematoma over the right temporo-occipital region; a 3 cm ecchymosis over the right temporoparietal area; a 1 × 0.2 cm fresh ecchymosis beneath the right lower eyelid; a 1 cm ecchymosis located 3 cm anterior to the right ear; and a 0.5 cm lacerated wound with surrounding ecchymosis on the left lower eyelid. Although superficial abrasions were noted during external examination, the overall evaluation did not identify skull fracture, patterned soft-tissue injury, retinal hemorrhage, visceral trauma, or other findings sufficient to support inflicted injury or abusive head trauma. The facial ecchymoses and focal neck soft-tissue hemorrhages were therefore interpreted cautiously and in the context of the markedly abnormal coagulation profile, absence of skeletal injury, absence of retinal hemorrhage, and lack of internal traumatic lesions.
Internal examination revealed significant hemorrhages involving the right temporal muscle group and a large subdural hematoma measuring 8 × 6 cm in the left occipital region with a maximum depth of 0.6 cm, hemorrhage in the right temporal muscle group, and ecchymoses measuring 0.5 cm in diameter on both posterior aspects of the thyroid cartilage and a 1 cm ecchymosis on the anterior surface of the left thyroid cartilage. No retinal hemorrhage was identified during postmortem examination, and the optic nerves appeared unremarkable. Brain histology confirmed dural hemorrhage with fibroblast proliferation and fibrin deposition, indicative of a 48-h-old hemorrhagic process. Pulmonary histology showed features of acute and chronic bronchopneumonia, while thymic samples revealed parenchymal and perithymic hemorrhages. Active chronic tracheitis was also noted. Toxicological analysis was negative for common poisons and drugs. Bacterial cultures grew Enterobacter spp., Klebsiella spp., and Enterococcus spp., suggestive of secondary bacterial infection. No blood sample for vitamin K concentration measurement was available in this case due to the advanced postmortem interval and lack of ante-mortem laboratory evaluation. Following a comprehensive medicolegal evaluation, the findings were considered most consistent with fatal intracranial hemorrhage associated with late-onset VKDB, after exclusion of traumatic, vascular, congenital, and metabolic causes. Although prematurity-related germinal-matrix or intraventricular hemorrhage was considered, the localization, organization stage, and absence of typical intraventricular extension were not compatible with the classic patterns of prematurity-associated intracranial hemorrhage.
Case 2
A term male neonate, body length of 50 cm and a weight of 3300 g, solely breastfed and without administration of IM vitamin K prophylaxis at birth, presented around two months of age with nonspecific symptoms, including fever. Initially evaluated at a local healthcare facility, the infant was prescribed symptomatic treatment and discharged. Later that day, clinical deterioration ensued, marked by convulsions and respiratory distress, prompting emergency referral to a tertiary hospital via ambulance. Upon arrival, the infant exhibited shallow and rapid breathing, subsequently progressing to respiratory arrest, requiring immediate intubation. Brain computed tomography (CT) imaging revealed compression of the fourth ventricle, a 1.5 cm subdural hematoma along the right tentorial surface, extensive subdural hemorrhages over the right frontal and parietal lobes, hyperdense areas consistent with subarachnoid hemorrhages, and pronounced subfalcine herniation. Pupillary examination showed fixed and dilated pupils, and no response to painful stimuli was noted. Laboratory evaluation revealed a profoundly prolonged activated partial thromboplastin time (APTT) (>120 s) and PT (>120 s). Management included administration of two transfusions of 10 mL/kg FFP and 1 mg IM vitamin K. Prior to the administration of vitamin K during hospitalization, no serum sample was obtained for the measurement of vitamin K levels. Therefore, laboratory confirmation of deficiency was not available. Following vitamin K administration, APTT and PT values normalized, supporting findings most consistent with late-onset VKDB. A critically low hemoglobin level (5.4 g/dL) prompted erythrocyte suspension transfusion. Therapeutic measures also included initiation of phenytoin for seizure control, dexamethasone for cerebral edema management, and cefotaxime for suspected bacterial infection. During PICU follow-up, the patient developed marked polyuria, with elevated serum sodium (Na: 165 mEq/L) and increased serum osmolality (320 mOsm/kg), findings consistent with diabetes insipidus. Despite aggressive supportive management, the clinical condition progressively worsened, culminating in death on the 68th postnatal day. External postmortem examination revealed multiple needle puncture marks over the scalp, wrists, elbows, knees, and dorsum of the feet, along with generalized abdominal distension.
Internal examination revealed no soft-tissue contusions or skull fractures of the scalp and calvarium, nor was there any hemorrhage in the thoracic or abdominal organs to suggest blunt-force trauma. Despite the absence of traumatic findings, examination of the central nervous system demonstrated diffuse softening and reddish-blue discoloration of the brain, cerebellum, and brainstem. Widespread subdural and subarachnoid hemorrhages were present. No prominent coagulation was observed within the hemorrhagic collections during autopsy, and the blood was largely uncoagulated and diffusely distributed. Limited areas of soft clot formation were identified. Although these gross findings are non-specific, they were considered supportive when interpreted together with the markedly prolonged PT/APTT, clinical response after vitamin K administration, absence of skull fracture or visceral trauma, and lack of other structural causes of hemorrhage. Histopathological examination confirmed diffuse subarachnoid hemorrhage, fresh cortical hemorrhages in the superficial cortex, bronchopneumonia, and hyaline membrane formation within the lungs, indicative of acute respiratory distress syndrome (ARDS). Following comprehensive medicolegal evaluation, the findings were considered most consistent with fatal intracranial hemorrhage associated with late-onset VKDB.
Case 3
A 40-day-old male infant, length was 57 cm and body weight was 5300 g, exclusively breastfed and born at term, presented to a healthcare facility with complaints of vomiting. The family history revealed a refusal of neonatal vaccinations and vitamin K administration at birth. No laboratory analysis was conducted to assess serum vitamin K levels either prior to or after death. Notably, no heel-prick screening test had been performed. Upon admission, laboratory studies revealed severe anemia (hemoglobin: 4.4 g/dL), a markedly prolonged PT (27.60 s; reference: 7.07-10.93 s), an elevated international normalized ratio (INR: 2.77; reference: 0.8–1.2), and a prolonged APTT (60.4 s; reference: 22–38 s). Fibrinogen levels were within normal limits (368 mg/dL). Although blood transfusion was initially recommended, the family refused consent. Management included administration of intravenous saline solution and IM vitamin K. During hospitalization, anisocoria was observed, raising clinical suspicion of intracranial hemorrhage. Subsequent neuroimaging identified a large subdural hematoma with midline shift. The infant was urgently admitted to the pediatric intensive care unit (PICU) and underwent a blood transfusion following family consent. Neurosurgical consultation was obtained, and the infant was taken to emergency craniotomy. During the surgical procedure, the patient experienced cardiopulmonary arrest. Despite prolonged resuscitation efforts, no return of spontaneous circulation was achieved, and death was declared intraoperatively. External postmortem examination revealed multiple ecchymotic needle puncture marks over the dorsum of both hands, antecubital fossae, right foot, and left side of the neck. A C-shaped 24 cm-long surgical staple line was noted over the left parietal region (Figure 1). Internal examination demonstrated subgaleal hemorrhage beneath the scalp over the left parietal area, a surgically created cranial bone window in the left parietal bone, operative interventions over the dura mater, and extensive subdural hemorrhages (Figure 2). Apart from surgically induced changes, no skull fractures, scalp contusions beyond the operative field, or injuries to thoracic or abdominal organs were identified, arguing against non-accidental trauma. Histopathological analysis confirmed extensive subarachnoid hemorrhage with erythrocyte extravasation, focal fresh hemorrhages within the subcortical glial tissue, mild mixed inflammatory infiltration over the arachnoid surface, and the presence of amorphous basophilic foreign material suggestive of surgical intervention artifacts. After a comprehensive medicolegal evaluation, the findings were considered most consistent with fatal intracranial hemorrhage associated with VKDB after exclusion of traumatic and congenital causes.

Postmortem external view of the scalp showing a C-shaped surgical closure with metallic staples following emergency craniotomy.
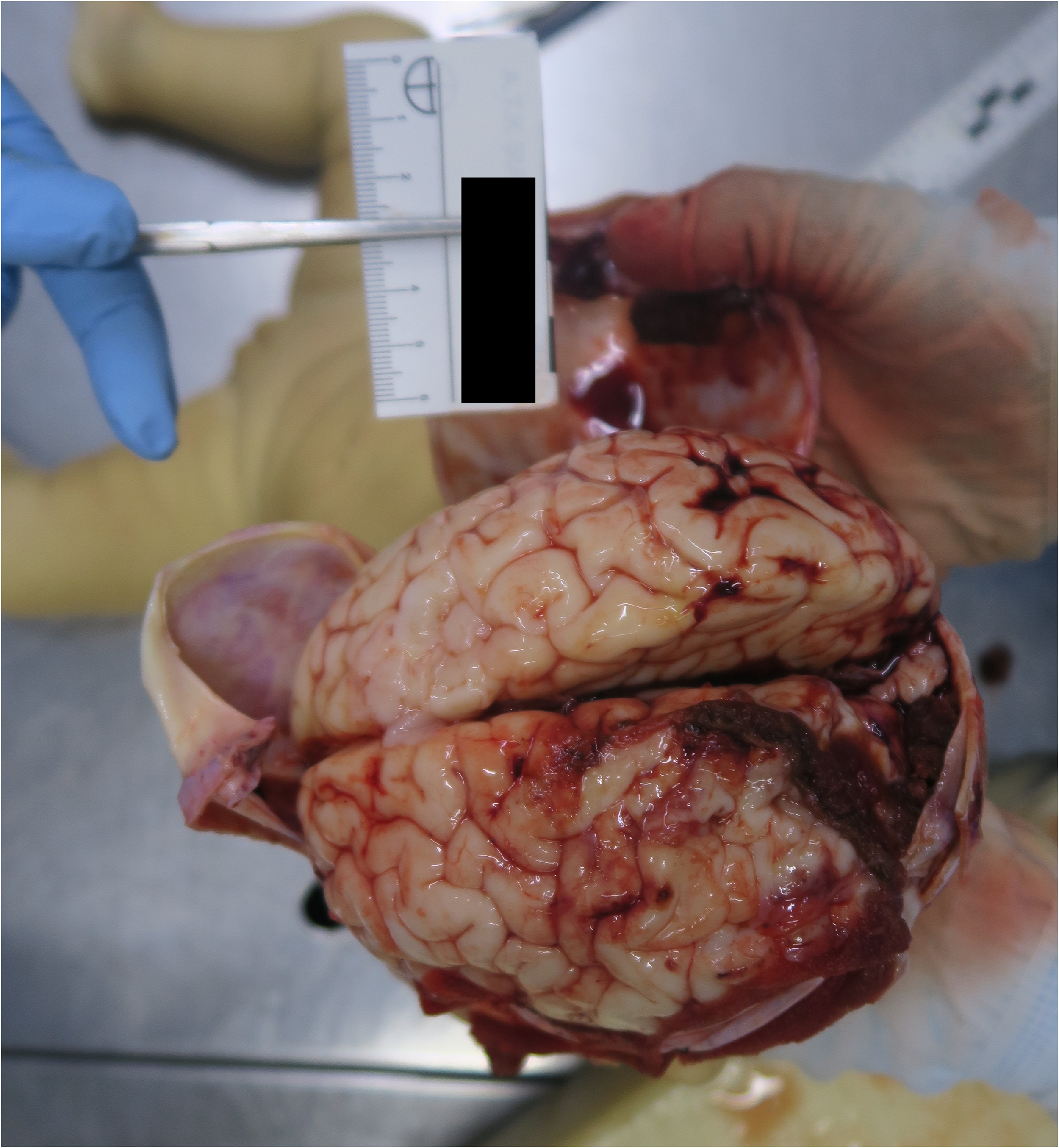
Gross examination of the brain demonstrating extensive subarachnoid hemorrhage and patchy cortical congestion, most prominent in the occipital lobes.
Case 4
A male infant, measurements showed a length of 58 cm and a weight of 4260 g, born at term via normal spontaneous vaginal delivery, was reportedly in good health until the 14th day of life. According to hospital records, he was brought to the emergency department with complaints of restlessness and seizures. The family had declined IM vitamin K prophylaxis at birth, and the infant had not received any vaccinations or routine postnatal screenings. Clinical assessment revealed poor general condition, irritability, and decreased responsiveness. Laboratory investigations showed hemoglobin of 8.2 g/dL, hematocrit 24.2%, white blood cell count of 18.5 × 103/μL, and platelet count of 200 × 103/μL. Coagulation studies indicated markedly prolonged PT (28.3 s; normal range: 10–14 s), elevated INR (2.6; normal range: 0.8–1.2), and prolonged APTT (70.2 s; normal range: 25–40 s), suggesting a severe coagulation disorder. Cranial radiography revealed bilateral subdural hematomas and midline shift (Figure 3). The patient was intubated and admitted to the NICU, where IM vitamin K (1 mg) and FFP were administered. Despite aggressive supportive care, the infant's neurological status progressively worsened. On the 15th day of life, he was declared deceased. External postmortem examination documented puncture marks over the dorsum of the hands and feet, consistent with intensive care interventions. A 15 cm linear surgical incision with metallic staples was observed over the midline scalp. Internal examination revealed bilateral subdural hematomas over the cerebral hemispheres (Figure 4), a craniotomy site over the parietal bone, and evidence of operative hemostatic materials in situ. The brain appeared markedly edematous with signs of transtentorial herniation. Histopathological analysis demonstrated diffuse subarachnoid hemorrhage, erythrocyte extravasation within subcortical white matter, and acute inflammatory infiltrates along the meningeal surfaces. There were no findings suggestive of trauma or congenital malformation. Based on the clinical history, laboratory findings, and autopsy results, the findings were considered most consistent with late-onset VKDB presenting with fatal intracranial hemorrhage after exclusion of alternative etiologies. Similar to Case 3, no blood vitamin K level was measured. The diagnosis was supported by the characteristic pattern of hemorrhage, the absence of trauma, and the lack of prophylactic vitamin K administration.
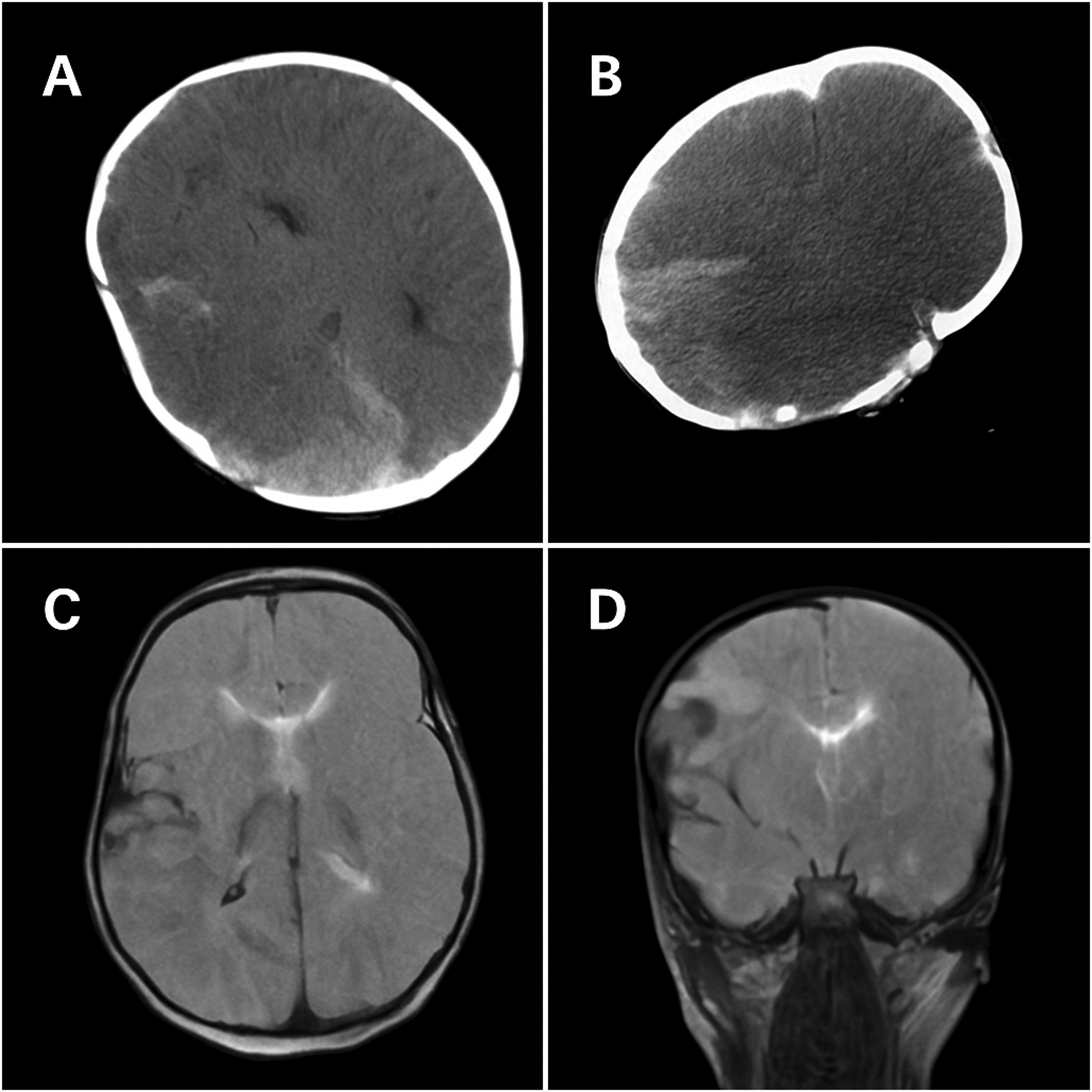
Preoperative neuroimaging findings of Case 4. (A) Axial non-contrast CT scan showing hyperdense foci consistent with parenchymal hemorrhages in the right hemisphere (on the first day of hospitalization). (B) Axial non-contrast CT scan demonstrating a large right-sided subdural hematoma causing midline shift(on the second day of hospitalization). (C) Axial T2-weighted MRI revealing extensive parenchymal hemorrhage with surrounding edema in the right cerebral hemisphere (on the eighth day of hospitalization). (D) Coronal T2-weighted MRI image depicting mass effect due to hemorrhage and compression of adjacent structures (on the eighth day of hospitalization).

Internal cranial view following calvarial removal, revealing severe subdural and subarachnoid hemorrhages with compressed cerebral gyri and effacement of cortical sulci.
DISCUSSION
VKDB remains a globally recognized, yet entirely preventable, cause of neonatal morbidity and mortality, particularly in settings with inconsistent prophylaxis practices. Despite long-standing prophylaxis protocols, the persistence of late-onset VKDB underscores critical gaps in neonatal care and parental compliance (22). This autopsy-based case series offers rare yet invaluable insights into the forensic, pathological, and public health dimensions of VKDB-related neonatal fatalities, reinforcing VKDB's continued significance as both a forensic concern and a target for public health intervention. While late-onset VKDB, typically occurring between 2 and 12 weeks of age, is considered the most severe form, Case 4 in our series developed on the 14th postnatal day—highlighting a potential overlap with the classic form and emphasizing the importance of early clinical vigilance (23,24). The observed clinical heterogeneity—including differences in gestational age, disease progression, onset timing, and rare complications such as central diabetes insipidus—underscores the multifactorial nature of VKDB and suggests the need for a more refined classification framework in forensic reporting.
Numerous studies have reported that exclusively breastfed infants are at higher risk due to low vitamin K concentrations in breast milk compared to formula (25–27). Furthermore, delayed or missed administration of vitamin K prophylaxis exponentially increases this risk (28). The susceptibility of preterm neonates, as illustrated in Case 1, may amplify the hemorrhagic outcomes of VKDB. This is primarily due to immature hepatic synthesis of clotting factors and delayed intestinal colonization, which impair endogenous vitamin K production. The global epidemiology of VKDB reveals varying incidence rates, often reflective of the effectiveness of national prophylaxis programs. In our series, the timing of onset ranged from the second week to beyond the sixth week of life, demonstrating this variability. Countries with routine IM vitamin K administration report incidences below 1 per 100,000 live births (11,29), whereas nations with less stringent policies report higher rates, sometimes reaching 80 per 100,000 among solely breastfed infants (6,30). Alarmingly, a resurgence in VKDB cases has been noted even in developed countries, largely attributed to parental refusal of prophylaxis due to misconceptions about vaccine safety and natural parenting philosophies (9,12). Similarly, Türkiye has also witnessed similar patterns of prophylaxis refusal culminating in VKDB-related deaths, emphasizing an urgent need for culturally adapted, evidence-based educational outreach initiatives (31). According to a Cochrane review by Puckett and Offringa, IM vitamin K prophylaxis significantly reduces the risk of both classic and late VKDB, establishing it as the most effective preventive measure available to date (27).
Detailed postmortem examinations are essential for supporting a diagnosis of VKDB and excluding competing causes of intracranial hemorrhage. In all four cases, neither neuroimaging nor autopsy revealed arteriovenous malformations, aneurysms, cavernous malformations, or venous sinus thrombosis that could account for the intracranial hemorrhages. In our series, key postmortem findings included extensive subdural and subarachnoid hematomas—particularly involving the parietal and occipital lobes—as well as the absence of external trauma in three cases. In Cases 3 and 4, meningeal inflammation was also present, with histopathology demonstrating mixed inflammatory infiltrates over the arachnoid surfaces (1,32). Although histopathological evaluations did not directly diagnose VKDB, they were crucial in excluding trauma, vascular malformations, congenital coagulopathies, and infection-related disseminated intravascular coagulation, thereby indirectly strengthening the diagnostic impression. In all four cases, severely prolonged PT and APTT values (up to >120 s in Case 2) were consistent with coagulation factor deficiencies secondary to vitamin K absence, reinforcing the value of laboratory findings as critical forensic indicators in suspected VKDB. Additional findings—such as fibroblastic proliferation along the dura and perithymic hemorrhages—further supported the diagnosis. In Case 1, extrinsic factors including reported co-twin bites during playing, together with extensive facial ecchymoses, underscored the importance of meticulous differential diagnosis to distinguish VKDB from inflicted trauma. Such atypical presentations highlight the added value of histopathological correlation and comprehensive medicolegal autopsy. The prominence of subdural and subarachnoid hemorrhages, particularly in the parietal and occipital regions in this case series, is consistent with previous autopsy-based studies and underscores the tendency of VKDB to cause life-threatening cerebral bleeding even in the absence of trauma. Although fibrin deposition was identified in the dura mater in Case 1, this finding does not contradict a diagnosis of vitamin K deficiency. On the contrary, the associated fibroblast proliferation and fibrin layering reflect a reparative response to ongoing hemorrhage, supporting the subacute nature of VKDB-related bleeding.
The implications of missed prophylaxis extend beyond individual outcomes. At the population level, these cases highlight systemic failures in parental education, healthcare accessibility, and policy adherence (17,33). Studies show that refusal of vitamin K correlates strongly with refusal of other neonatal interventions, including vaccinations (31,34). This observed clustering of health refusals—including vitamin K, heel-prick testing, and vaccination—necessitates a multifaceted public health strategy to address misinformation and build trust in medical recommendations. This concern is echoed by Burke, who provided a comprehensive overview of the clinical spectrum of VKDB, reinforcing the critical need for both early recognition and timely prophylaxis to prevent fatal complications (32).
Approaches to handling parental refusal of vitamin K prophylaxis differ significantly across legal systems. Some jurisdictions mandate prophylaxis, whereas others respect parental autonomy, even at the risk of adverse outcomes (35,36). The medicolegal implications of these policies are profound, particularly when preventable deaths trigger legal investigations or malpractice claims (37). In an effort to improve compliance, several alternative prophylactic strategies have been explored. Oral vitamin K regimens, although more acceptable to some parents, are less effective than IM administration and require multiple doses to achieve comparable protection (38,39). Recent studies have proposed new formulations with improved bioavailability, but consensus on their efficacy remains elusive (40). The oral regimen requires multiple doses and strict adherence to schedule, which introduces the risk of non-compliance. In contrast, a single IM dose at birth provides long-term protection and is supported by a stronger evidence base. Therefore, while oral prophylaxis can be considered when IM administration is refused, it should be accompanied by robust education and follow-up to ensure compliance. Strikingly, all four cases shared a single critical feature: documented parental refusal of vitamin K prophylaxis by caregivers, reinforcing the pivotal role of parental decision-making in the etiology of late-onset VKDB.
These cases also carry important medicolegal implications. Parental refusal of neonatal vitamin K prophylaxis raises questions regarding the boundaries between parental autonomy and medical neglect, particularly when a well-established, low-risk intervention could have prevented a fatal outcome. Forensic pathologists must clearly document the absence of traumatic findings, the presence of coagulopathy, and the lack of prophylaxis when formulating cause- and manner-of-death opinions. Such documentation informs legal authorities in determining whether deaths should be regarded as natural consequences of disease or as preventable outcomes associated with deviations from standard neonatal care.
Interestingly, the resurgence of VKDB mirrors the resurgence of vaccine-preventable diseases in populations exhibiting vaccine hesitancy. Sociocultural factors, mistrust of pharmaceutical industries, and misinformation via social media have been implicated as drivers of this phenomenon (41,42). Public health campaigns aimed at enhancing vaccine confidence—now recognized as a multidimensional phenomenon involving access, beliefs, and exposure to misinformation—could also improve the acceptance of vitamin K prophylaxis (33). To this end, educational interventions targeted at parents have demonstrated varying degrees of success. Prenatal counseling sessions, standardized informational brochures, and healthcare provider training programs have all been associated with increased acceptance of vitamin K administration (43,44). Nevertheless, combating deeply entrenched beliefs requires multifaceted strategies beyond mere information dissemination. Economic analyses have reinforced the cost-effectiveness of universal vitamin K prophylaxis compared to the healthcare costs associated with treating VKDB-related complications (45,46). From an ethical standpoint, preventing a devastating yet easily avoidable condition—particularly when safe and cost-effective measures exist—supports continued efforts to improve adherence to neonatal prophylaxis programs (47).
In the present series, VKDB was not treated as a diagnosis established by direct biochemical confirmation alone. Rather, the medicolegal conclusion was based on an integrated assessment of clinical history, coagulation studies, neuroimaging, autopsy findings, histopathology, and exclusion of competing explanations. Relevant findings included extensive multicompartment intracranial hemorrhage (subdural, subarachnoid, and intraparenchymal), markedly abnormal coagulation parameters, absence of traumatic findings typically associated with abusive head trauma, and the clinical history of absent vitamin K prophylaxis. In particular, no skull fractures, retinal hemorrhages, visceral organ injuries, healing skeletal injuries, or focal impact lesions sufficient to explain the hemorrhages were identified. In Case 1, facial ecchymoses and focal neck soft-tissue hemorrhages were carefully considered in the differential diagnosis; however, these findings were interpreted in conjunction with the severe coagulopathy and absence of corroborating traumatic injuries. Furthermore, laboratory indicators of coagulopathy, when available, and the absence of underlying vascular anomalies supported the diagnosis. This integrative assessment, coupled with the exclusion of alternative etiologies, reinforced the conclusion of fatal VKDB. In forensic settings, the diagnosis of VKDB poses unique challenges. Differentiating between accidental, inflicted, and spontaneous hemorrhages is critical in the medicolegal investigation of infant deaths (48). Multidisciplinary collaboration between forensic pathologists, pediatricians, and hematologists is essential to ensure accurate determination of the cause of death and to guide legal proceedings appropriately. Taken together, our findings highlight the critical role of autopsies in clarifying the cause of death in neonates with unexplained hemorrhagic events. These results are consistent with prior autopsy-based studies that underscore the value of postmortem examinations in neonatal deaths, particularly when clinical histories are incomplete or ambiguous (49,50). In Case 1, the presence of bronchopneumonia and positive cultures for Enterobacter, Klebsiella, and Enterococcus species suggests a secondary infectious contribution, which may have exacerbated the hemorrhagic diathesis and contributed to the rapid clinical decline. The development of complications such as central diabetes insipidus in Case 2 was confirmed by polyuria with hypernatremia (Na: 165 mEq/L) and high serum osmolality (320 mOsm/kg). In Case 3, intraoperative cardiac arrest occurred during emergency neurosurgery, further complicating the clinical course. Given the preventable nature of VKDB, each case—including those occurring as early as the second postnatal week—represents not only a clinical failure but also a missed opportunity for public health intervention. The occurrence of complications such as central diabetes insipidus and intraoperative cardiac arrest in our cases highlights the rapid clinical deterioration and diagnostic uncertainty inherent in managing unrecognized VKDB in critical care settings. Given that non-accidental trauma is a leading cause of intracranial hemorrhage in infancy, all cases were systematically evaluated for abusive head trauma. This included careful assessment for skull fractures, subgaleal hematomas, bridging vein tears, retinal hemorrhages, rib or metaphyseal fractures, abdominal organ lacerations, and patterned bruises. None of these hallmark features were identified in our series, and the hemorrhage pattern was more consistent with diffuse coagulopathy than with focal impact trauma.
In Türkiye, refusal of neonatal vitamin K administration is often influenced by a complex interplay of cultural, religious, and misinformation-driven beliefs. Some parents mistakenly associate vitamin K injection with unnecessary medical intervention or vaccine-related conspiracy theories, particularly when it is administered simultaneously with hepatitis B vaccination. Additionally, online misinformation and anecdotal accounts shared via social media platforms have further fueled skepticism toward routine neonatal prophylaxis. These deeply entrenched beliefs are often reinforced within communities with limited access to accurate medical guidance, and in some cases, refusal may stem from a general distrust of institutional healthcare. While these behaviors may verge on medical neglect, they are frequently rooted in misinformation rather than malicious intent.
CONCLUSION
VKDB remains a largely preventable but still encountered cause of fatal infant intracranial hemorrhage. Despite the global availability of effective prophylactic strategies, the continued emergence of fatal VKDB cases, as highlighted in this autopsy-based series from Türkiye, underscores enduring gaps in healthcare delivery, parental education, and public trust in medical interventions. The present findings reaffirm the catastrophic potential of late-onset VKDB when prophylaxis is omitted, especially among solely breastfed infants. The devastating intracranial hemorrhages documented in our cases highlight the necessity for consistent implementation of neonatal prophylaxis protocols. Furthermore, the medicolegal evaluations reveal that forensic autopsies offer both diagnostic clarity and public health insight.
To be truly effective, efforts to address VKDB must transcend traditional clinical boundaries. Public health strategies must integrate prenatal counseling, culturally sensitive education campaigns, and robust policy frameworks that encourage adherence to prophylaxis without alienating parents. Given the demonstrated association between vitamin K refusal and broader healthcare skepticism, public health initiatives must be aligned with trust-building efforts. From a forensic perspective, our study highlights the essential role of autopsies in supporting medicolegal assessment of suspected VKDB, as demonstrated by extensive intracranial hemorrhages and non-traumatic subdural hematomas across our four cases—findings consistent with previously published autopsy series. Future research should aim to refine strategies for early detection of VKDB, explore innovative prophylaxis delivery methods to accommodate parental concerns, and evaluate the long-term outcomes of various policy approaches globally. This refusal pattern is increasingly recognized as part of broader vaccine hesitancy, as recent studies have shown overlapping parental concerns about safety, necessity, and mistrust in healthcare providers (15). This behavioral pattern may also serve as an early indicator of subsequent refusal of other essential neonatal preventive services, including metabolic screening and immunizations (16).
Ultimately, the prevention of VKDB-related mortality depends not only on clinical availability of prophylaxis but also on effective counseling, documentation, and parental engagement. Routine implementation of vitamin K prophylaxis at birth represents a simple yet impactful public health measure, capable of eliminating preventable neonatal deaths associated with coagulopathies. From a forensic perspective, these cases emphasize the importance of careful clinicopathologic correlation, structured exclusion of inflicted trauma, and precise cause-of-death formulation in suspected VKDB-related infant deaths.
LIMITATIONS
Limitations of our study include its retrospective design and the relatively small sample size inherent to forensic case series. In addition, direct measurement of blood vitamin K concentrations and specific coagulation factor assays were not performed, as these tests are not routinely available in our setting; this represents an important limitation and requires cautious interpretation of VKDB as the most consistent diagnosis rather than as a directly biochemically confirmed diagnosis in every case.
Footnotes
ACKNOWLEDGMENTS
We would like to express our gratitude to the Council of Forensic Medicine, Ministry of Justice, Republic of Türkiye, for their support during this research.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ETHICAL CONSIDERATIONS
The approval of the Educational and Scientific Research Commission of the Council of Forensic Medicine, dated December 03, 2024, and numbered 21589509/2024/1452, was obtained for the study. As the research involved deceased infants, and all analyses were performed on retrospective anonymized forensic records, the requirement for informed consent was waived. All images used in this article are derived from anonymized forensic autopsy documentation and contain no identifiable features; therefore, in accordance with institutional policy, additional parental consent for publication of figures was not required.
FUNDING
The authors received no financial support for the research, authorship, and/or publication of this article.