
Abstract
Based on a one-month online survey that was announced to 640 subscribers of the National Association of Medical Examiners’ NAME-L listserv, perceived strengths, limitations, and needs of death investigations systems were obtained for the 25 states that lack a state medical examiner. Forty-one persons responded to the survey and at least one response was obtained from each of the 25 states. Overall, strengths could be summarized into categories that include the local nature of death investigation (e.g., items related to coroners, medical examiners, forensic pathologists, and accreditation and certification) and issues related to finances, organization, and system oversight. Perceived limitations fell into similar general categories but the largest group of comments consisted of coroner-related concerns. Needs could be categorized into issues which relate to facilities and death investigation system features; finances; coroners, forensic pathologists, and accreditation and certification; standards, training, and education; and research and technology. Specific strengths, limitations, and perceived needs are summarized in tables showing the states citing those features. We hope these data will be useful to those who wish to further study death investigation systems in the various states.
Introduction
A separate article in this issue of Academic Forensic Pathology reports the strengths, limitations, and needs of death investigation systems in those states with a state medical examiner or state agency head with a similar title (1). This article describes the perceptions of persons who work in states that have county, district, or regional based death investigation systems but which lack a state medical examiner regarding the perceived death investigation system strengths, limitations, and needs in those states.
Methods
On November 25, 2013, a message was posted on the NAME-L Listserv soliciting input from persons (primarily forensic pathologists or other NAME members) who work in the 25 states that lack a state medical examiner system. Responders were asked to indicate their perceptions about the strengths, weaknesses/limitations, and needs for improving the death investigation system in their state. The survey was open for a four-week period until December 25, 2013. During the four-week period, two additional reminder emails were sent to NAME-L subscribers (N=640). Comments from persons in each state with a response were summarized in general terms and tabulated for each state.
Results
Responses were received from 41 persons with at least one response from each of the 25 states (
States Included in This Study, With Type of Responder(s) From Each State
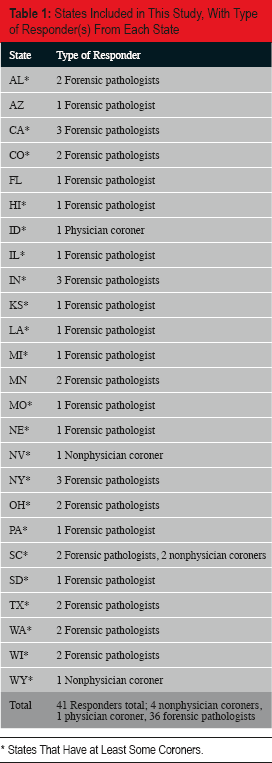
States That Have at Least Some Coroners.
Overall, strengths could be summarized into categories that include the local nature of death investigation; items related to coroners, medical examiners, forensic pathologists, and accreditation and certification; and issues related to finances, organization, and system oversight (
Summary of Perceived Strengths of Death Investigation Systems
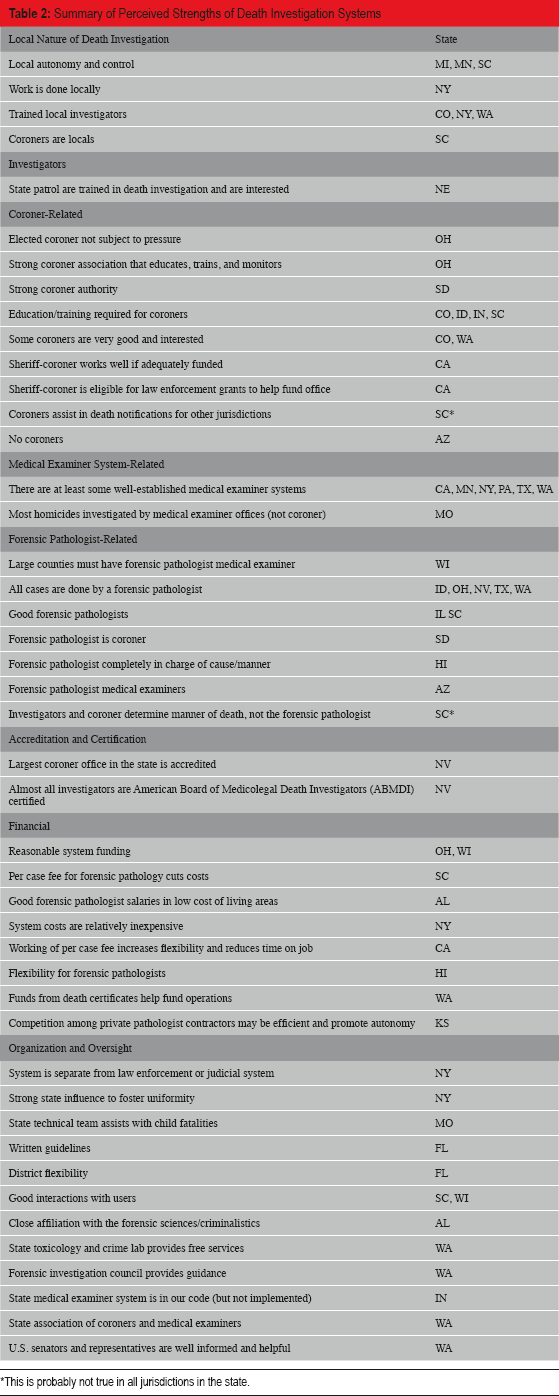
This is probably not true in all jurisdictions in the state.
Perceived limitations were diverse in scope and fell into general categories similar to those of system strengths (
Summary of Perceived Limitations of Death Investigation Systems
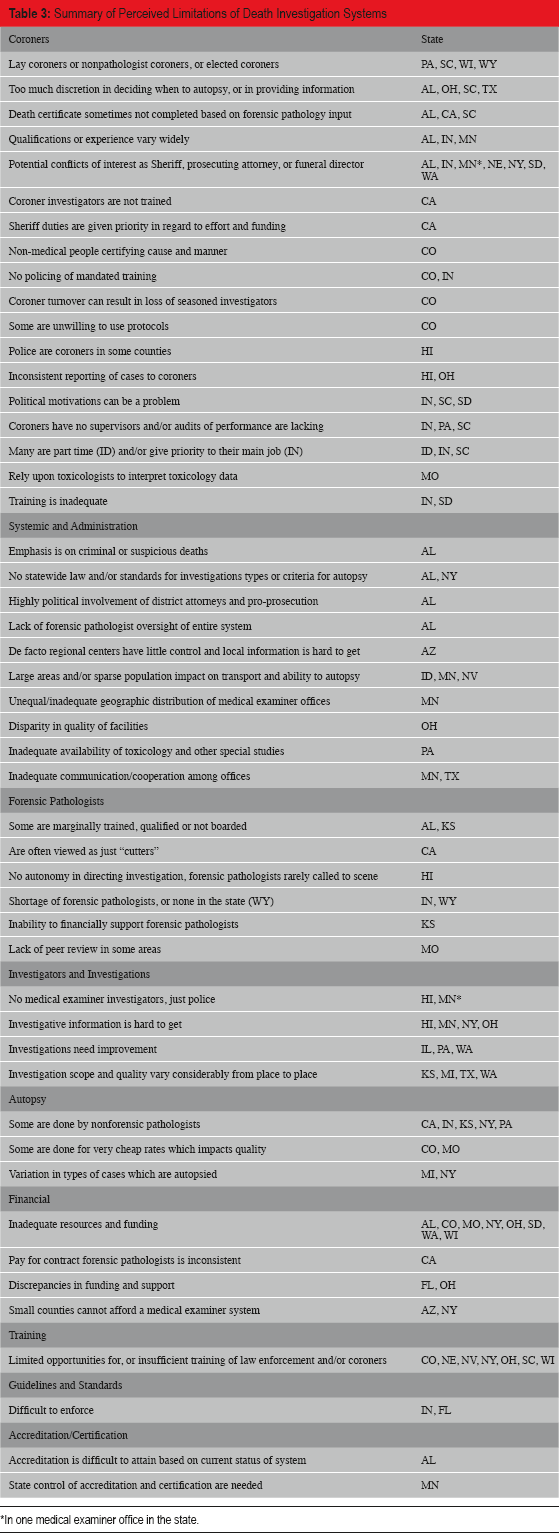
In one medical examiner office in the state.
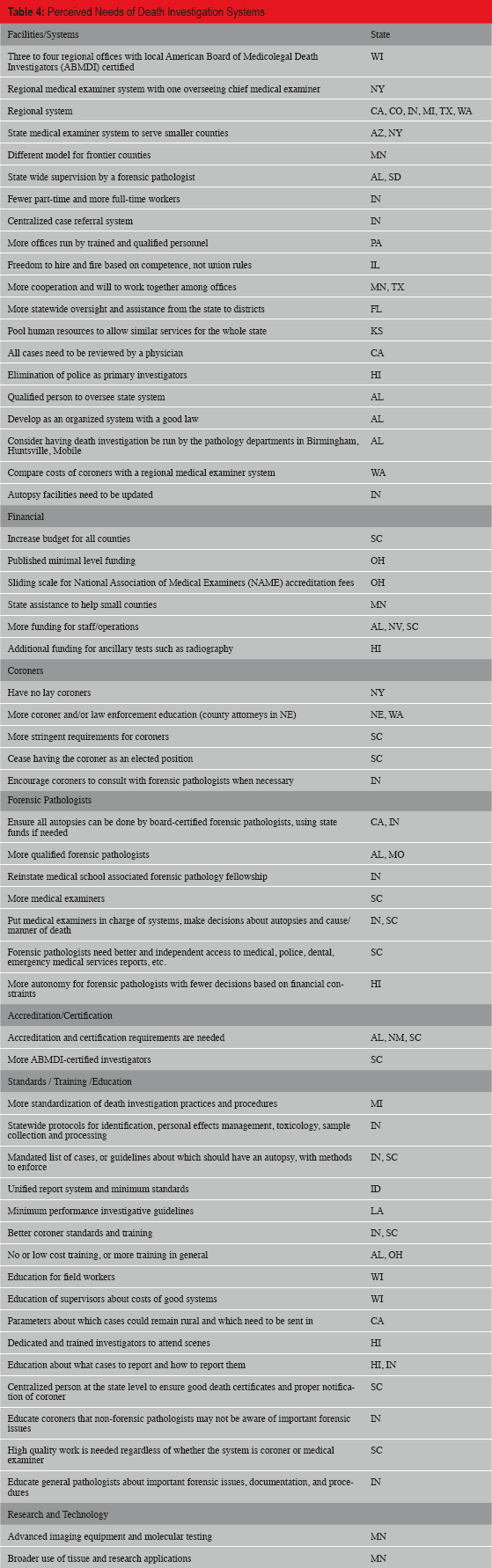
Needs could be categorized into issues which relate to facilities and death investigation system features; finances; coroners, forensic pathologists, and accreditation and certification; standards, training, and education; and research and technology (
Perceived Needs of Death Investigation Systems
Discussion
A limitation to this study is that in states lacking a state medical examiner, no single person can provide a first-hand overview of administrative, managerial, and operational aspects of death investigation for the entire state. Further, as shown in
Although
In addition to the coroner-related deficiencies, other distinguished limitations followed generally applicable themes. Those cited by the most states had to do with inadequate resources and funding, insufficient training of law enforcement scene investigators or coroners, autopsies being performed by nonforensic pathologists, variation in quality and scope of investigation from place to place, and difficulty in obtaining needed investigative information from other agencies.
Among the perceived needs, some common themes deserve mention. The development of regional centers, more cooperation among offices, centralized reporting systems, more state oversight, and conversion from part-time to more full-time personnel were noted by multiple responders. The need for more funding and operational support was noted, as was the need for more forensic pathologists, medical examiners, accreditation, certification, standards, training, and education. It should be noted that these are all needs identified in the National Research Council report regarding death investigation systems (2).
Of the 25 states in this study, 22 have coroners in at least some counties. A perceived need to abolish lay coroners or elected coroners was mentioned by only two responders (NY, SC) and the lack of coroners was cited as a strength by just one responder (AZ), although the need for improved coroner education and training was a common theme. This is an interesting observation in the context of the National Research Council's report, which recommends that coroner systems eventually be replaced with medical examiner systems (2). However, the data in our study seems to indicate a feeling that coroner systems can be functional with adequate funding, training, education, and medical input, and that the replacement of coroner systems is not a pressing issue among those who responded to the survey. Rather, the emphasis seems to be on needs to improve those systems. Of the states from which comments about coroners were received, only Ohio requires the coroner to be a physician, and in nearly all, the coroner is elected. Thus, in general, comments about coroners should be regarded as being directed at nonphysician (sometimes called “lay”) coroner systems in which the coroner is elected. It is also important to realize that some systems that retain the word “coroner” in the system leader's title actually operate as a medical examiner system, such as the medical examiner/coroner office in Denver.
In one state (SC), there was an obvious difference of opinion among responders, which included both medical examiners and coroners. While the strengths of coroners and weaknesses of medical examiners were cited, sentiments that the coroner system needs to be replaced and more authority and records access needs to be provided to forensic pathologist/medical examiners was indicated. In light of the aforementioned bias in this survey toward forensic pathologist respondents, such a divergent viewpoint likely exists in other states as well, such that more focused study is probably advisable in any state considering implementing major changes.
Not unexpectedly, the scope of comments reported in this study was larger or more diverse in nature compared with comments received from state medical examiner states, as reported elsewhere (1).
Conclusions
Recognizing that the opinions about strengths, limitations, and needs for death investigation systems in a given state may reflect the views of only one person working in that state, we have documented viewpoints about 25 states that lack a state medical examiner. The data may be useful for specific individual states to review and critically analyze to verify or identify additional needs in the state. Such reviews should be conducted by state associations of medical examiners, coroners, and death investigators where such organizations exist. Collectively, these data may also be useful as they include a wide scope of strengths, limitations, and needs that can guide further study.
Authors
Randy Hanzlick MD - Chair
Christopher Boden BS
Steven Clark PhD
Joseph Prahlow MD
Kathryn Haden-Pinneri MD
Karen Gunson MD
Tracey Corey MD
Erin Presnell MD
Footnotes
Acknowledgements
The authors wish to thank all of those who responded to the survey. Participants were told that data would be reported anonymously, so we cannot thank them by name here.
The comments in this article are those of the National Association of Medical Examiners ad hoc Data Committee authors and do not necessarily reflect the opinions, viewpoints, or position of the National Association of Medical Examiners.
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest.