
Abstract
Objective:
To compare the safety and regression rates of conservative treatments for complex atypical hyperplasia (CAH) between pre- and postmenopausal women.
Methods:
Historical cohort study of pre- and postmenopausal women with CAH managed conservatively at one center (Royal Women’s Hospital, Melbourne, Australia) between September 1999 to June 2012.
Results:
Of the 153 women with CAH, 92 (60%) underwent hysterectomy and the remaining 61 were managed conservatively with oral or intrauterine progestogen: 42 were premenopausal and 19 were postmenopausal. Within 12 months, 32 (76%) premenopausal women demonstrated regression of CAH and none developed endometrial cancer. In contrast, only 4 (21%) postmenopausal women showed disease regression and 4 (21%) progressed to endometrial cancer. Over a median of 24 months, 3 premenopausal women relapsed with CAH and 2 developed endometrial cancer. Four premenopausal women had successful pregnancies.
Conclusion:
Conservative treatment with progestogen in premenopausal women with CAH leads to high regression rates within the first 12 months. In contrast, postmenopausal women have high rates of ongoing disease and cancer progression and conservative therapy should be avoided.
Introduction
Endometrial hyperplasia is a common condition found in 5% to 10% of all women presenting with abnormal uterine bleeding. 1 It is usually thought to arise due to unopposed estrogen stimulation. 1 -5 The degree of endometrial hyperplasia is determined by the degree of architectural abnormality and cytological atypia and ranges from simple hyperplasia to complex atypical hyperplasia (CAH). 6 It is a precursor to endometrial cancer and while the risk is minimal in those diagnosed with simple hyperplasia, the risk of progression or of concomitant endometrial cancer is markedly increased in those with CAH. 7,8 As a result, the standard treatment of CAH has been hysterectomy, which is curative for noninvasive disease. 7,9,10
Progestogens have both antiestrogenic and direct antiproliferative effect on the endometrium. They can induce endometrial regression and thus may prevent progression to cancer. 1,11 -14 Currently, there are no evidence-based guidelines for the conservative (nonsurgical) treatment of CAH; however, there are a number of reports of progestogens being used successfully as an option for those who decline hysterectomy. 14
A recent meta-analysis suggests that 86% of patients will regress when CAH is treated conservatively and one-quarter of these women will conceive and deliver without complication. 15 Unfortunately, rates of relapse with median follow-up between studies of 11 and 76.5 months are high at 26%, suggesting patients treated conservatively require intensive follow-up. 15 Mode of progestogen delivery seems to influence regression rates, with the levonorgestrel-releasing intrauterine system (LNG-IUS) being more effective than oral progestogen treatment at 90% and 69%, respectively. 16 Caution must be taken when interpreting these results as all studies reported very modest numbers of patients.
In the clinic, there are 2 distinct groups of women who present with CAH. The first are premenopausal women who may be opting for conservative therapy primarily to preserve fertility. The second are postmenopausal women who may choose conservative treatment because they wish to avoid hysterectomy or are unfit for surgery. Given the physiology of these 2 groups are potentially very different, it is conceivable that their response to hormonal progestogens may differ. Surprisingly, however, there are no published reports of how these groups differ in their response to conservative therapy. This information is likely to influence practice and hence is of significant clinical value.
In this cohort study, we report outcomes of women with CAH who have been treated conservatively and grouped them according to their menopausal status. The primary outcome was the rate of regression of CAH in the first 12 months. Secondary outcomes were subsequent relapse of CAH during follow-up, whether the type of progestogens affected the rate of regression and fertility rates in the premenopausal group.
Materials and Methods
A retrospective cohort study was conducted at the Royal Women’s Hospital, Melbourne, Australia, and was approved by the hospital’s research and ethics committee. The hospital’s histopathological database was searched for “CAH” and “complex hyperplasia with atypia” to identify patients diagnosed between September 1999 and June 2012. Pathologists with a special interest in gynecological cancers reached the diagnosis of CAH using World Health Organization criteria. 6
All patients with CAH are referred to the gynecology oncology unit, where they are discussed at a multidisciplinary meeting and a management plan recommended. The standard recommended management is hysterectomy but if conservative treatment is requested this is with either oral medroxyprogesterone acetate (MPA) or a levonorgestrel intrauterine device (LNG-IUS). These women are followed up at 6-month intervals in the gynecology oncology clinic and with hysteroscopy and endometrial biopsy at 6-month intervals.
Data were obtained from the electronic oncology database and supplemented by the written patient history up until the end of April 2013. Women were studied in pre- and postmenopausal groups. The treating clinician determined menopausal status, which was 12 months since last menstruation. Baseline characteristics including age, body mass index (BMI), and use of hormonal medication prior to diagnosis were recorded. The type of treatment for all the patients was established and, if this was conservative, indicated. The incidence of endometrial cancer on histopathology following hysterectomy as primary treatment was recorded.
In those treated conservatively, type of therapy, duration of therapy, time to response, time to relapse, and whether hysterectomy was subsequently performed were recorded in pre- and postmenopausal groups. Treatment outcomes were categorized as (1) regression (normal endometrium or progestogen modified endometrium without evidence of ongoing CAH), (2) no change/stable disease (CAH), and (3) progression (endometrial cancer). Women’s desire to achieve a pregnancy and subsequent success were recorded as well as the need for assisted reproductive treatment.
The baseline characteristics and outcomes for oral progesterone or LNG-IUS were analyzed using the Mann-Whitney U tests for nonparametric data and the Pearson chi-square test for categorical data. All analysis were performed using Graphpad Prism (version 6) (GraphPad Software, La Jolla). A value of P < .05 was considered significant and standard deviation (SD) was displayed.
Results
Patient Characteristics
A total of 153 women with CAH were identified from September 1999 to June 2012. In all, 71 were premenopausal of whom 29 (41%) proceeded directly to hysterectomy. Concurrent endometrial cancer was diagnosed in 6 (21% n = 6 of 29) women at the time of hysterectomy. In all, 82 were postmenopausal, and 63 (77%, n = 63 of 82) proceeded directly to hysterectomy. Concurrent endometrial cancer was diagnosed in 15 (24%, n = 15 of 63) women on histopathology. The remaining 61 (40%, n = 61 of 153) women had conservative management and formed the study population (Figure 1). Of these, the majority (69% n = 42 of 61) were premenopausal with the remainder (31% n = 19 of 61) postmenopausal.
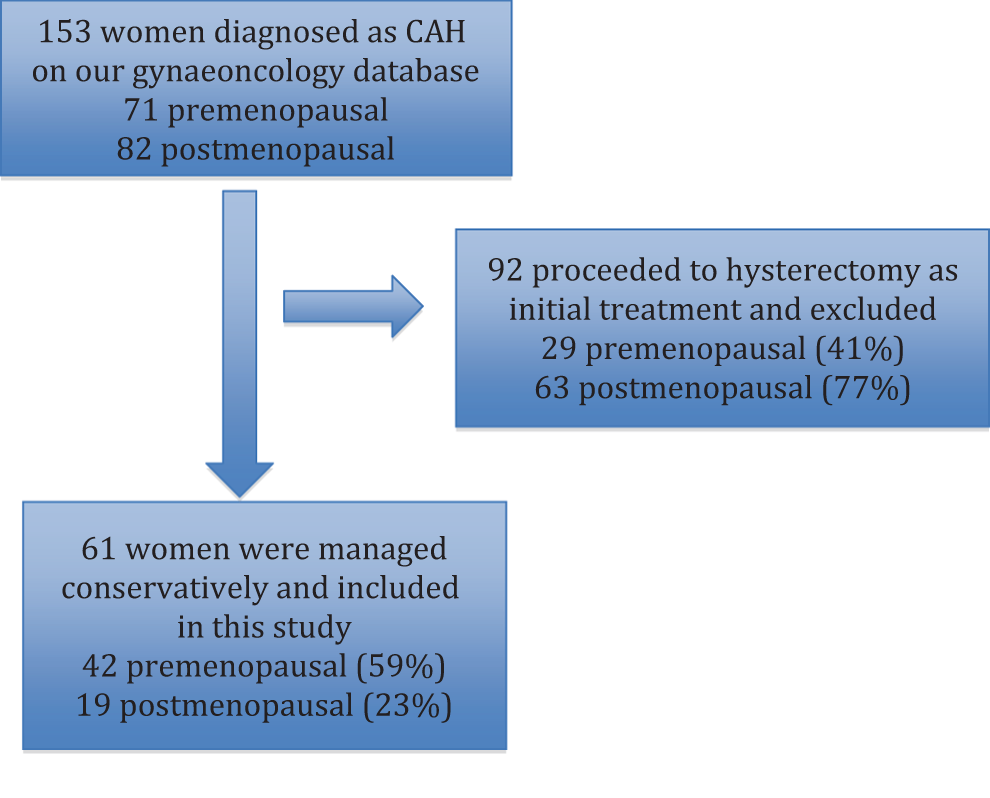
Patient selection process.
Baseline characteristics are shown in Table 1. The mean age of premenopausal women was 37 (SD ±7.6) and postmenopausal women was 61 (SD ±11.4). Both groups were obese with mean BMI of 35 (SD ±12.6) for premenopausal women and BMI of 37 (SD ±6.4) for postmenopausal women. Premenopausal women generally presented with menstrual bleeding abnormalities at 74% (n = 31 of 42); however, 19% (n = 8 of 42) were diagnosed incidentally during investigation for infertility. All postmenopausal women presented with postmenopausal bleeding. Of those who elected for conservative therapy, the indication was to preserve fertility in most of the premenopausal (71%, n = 30 of 42) and to avoid surgery in most of the postmenopausal women 79% (n = 15 of 19) while 21% (n = 4 of 19) were too unfit for surgery.
Baseline Characteristics.
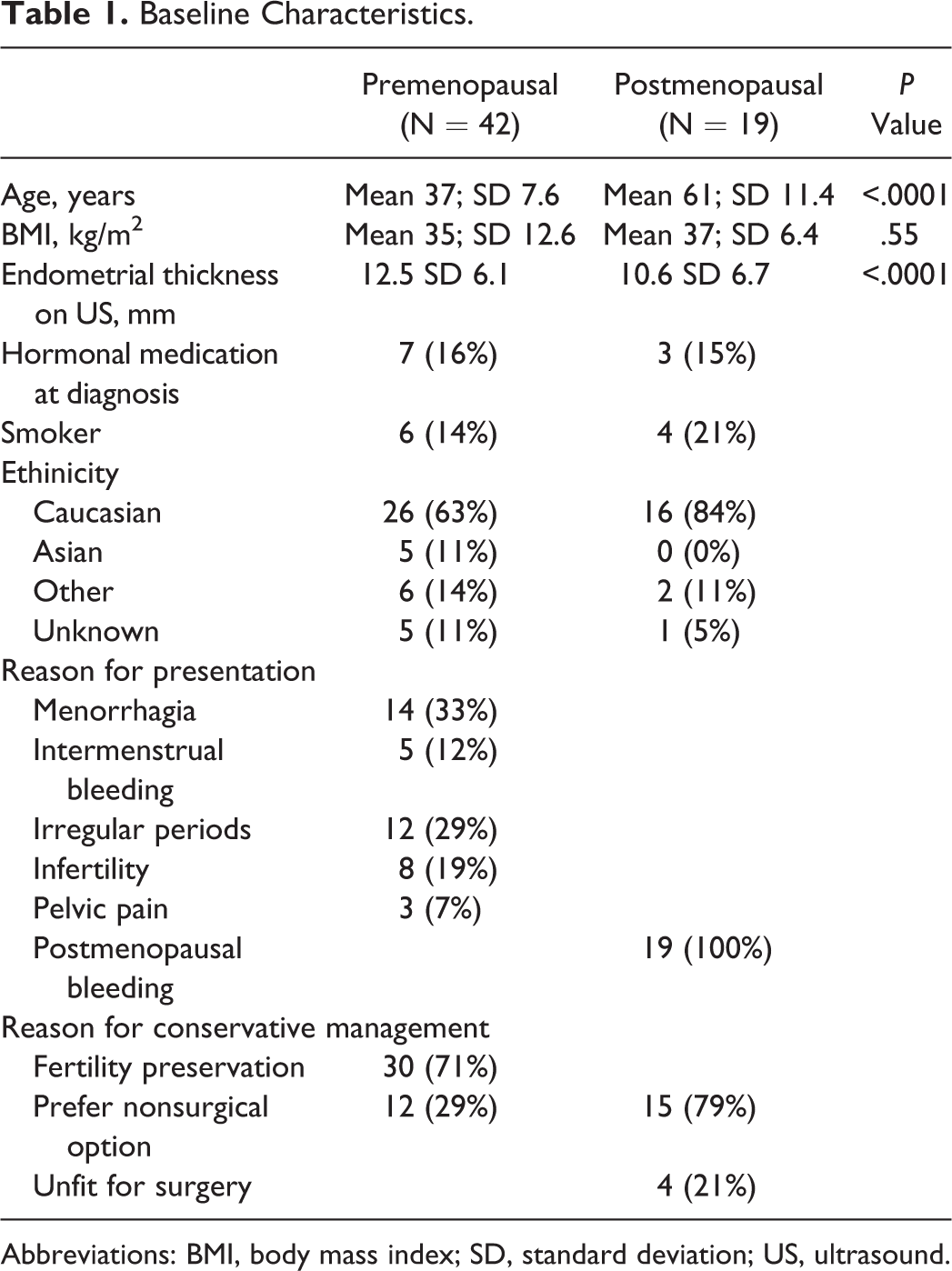
Abbreviations: BMI, body mass index; SD, standard deviation; US, ultrasound.
Regression Rates in the First 12 Months
Regression of disease was seen in 32 (76% n = 32 of 42) premenopausal women at follow-up hysteroscopy and endometrial biopsy after 12 months of conservative treatment (Table 2). Regression rates were significantly less in postmenopausal women with only 4 (21% n = 4 of 19) responses after 12 months of conservative management (P < 0.0001). This generally occurred after 6 months of medical treatment (Figure 2). There were no cases of progression to cancer in the first 12 months of treatment in the premenopausal group; however, 4 (21% n = 4 of 19) women in the postmenopausal group had endometrial cancer at first follow-up hysteroscopy dilation and curettage (P = 0.002).
Histology at First Hysteroscopy and Endometrial Biopsy Following Medical Treatment.
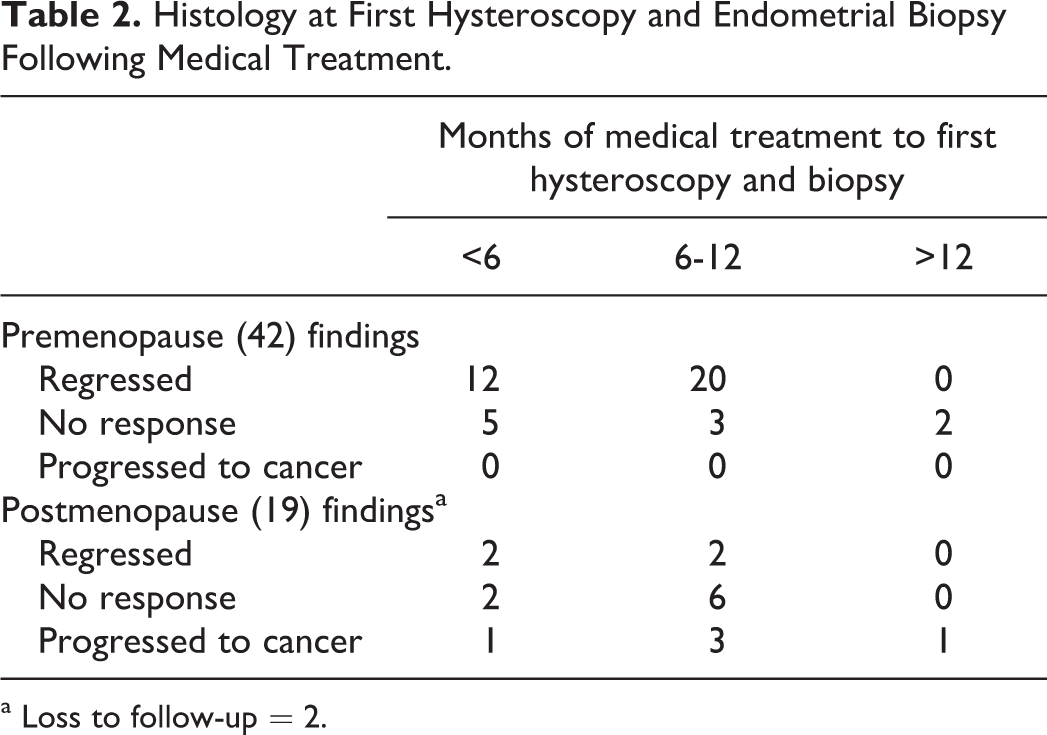
a Loss to follow-up = 2.
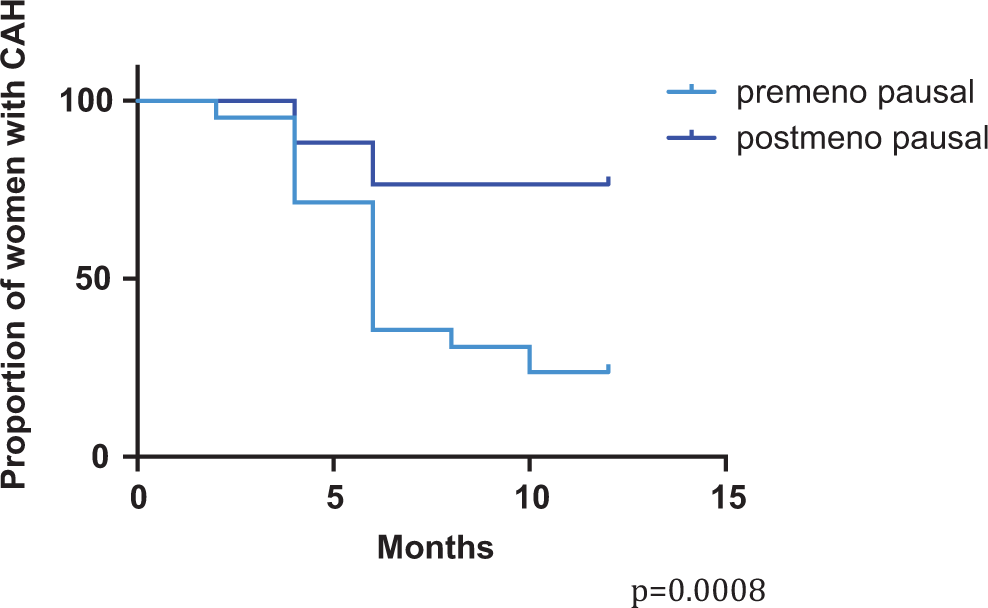
Proportion of patients with ongoing complex atypical hyperplasia (CAH) or progression of disease following conservative treatment at first hysteroscopy and endometrial biopsy.
All premenopausal women with persistent CAH despite intrauterine progestogen and 4 of the 6 of those with persistent CAH on oral progestogen proceeded to hysterectomy and histology was concordant. The remaining 2 women with persistent CAH after oral progestogen underwent disease regression with LNG-IUS. All postmenopausal women with persistent CAH or progression to endometrial cancer underwent hysterectomy and histology was concordant with the most recent curette in all except 1 where CAH was diagnosed at hysterectomy despite a preoperative diagnosis of endometrial cancer from endometrial biopsy.
We next examined treatments used and the effects they had on regression of disease. Progestogens comprised oral therapy MPA or intrauterine therapy LNG-IUS (Mirena). The rates of regression in premenopausal women were similar whether treatment was with the LNG-IUS (80% n = 8 of 10) or MPA (75% n = 24 of 32), P = .74. Regression occurred in only 3 (38% n = 3 of 8) postmenopausal women treated with the LNG-IUS and in only 1 (9% 1 of 11) postmenopausal woman treated with oral MPA. In both premenopausal and postmenopausal women, treatment was continued indefinitely or until hysterectomy.
Longer Term Follow-Up and Recurrence of Disease
Thirty-two premenopausal women continued conservative management after the initial 12-month period with a median follow-up of 24 months (interquartile range 16-50, range 10-120 months). Four postmenopausal women continued conservative management with a median follow-up of 35 months (interquartile range 17-41, range 12-43 months).
Of the 32 premenopausal women that experienced regression, 5 were found to have recurrence or developed endometrial cancer during the follow-up period at a median of 30 months (interquartile range 24-53, range 21-63 months). Three were diagnosed with recurrence of CAH and 2 progressed to endometrial cancer. Four had no treatment for 6 to 24 months prior to the time of diagnosis as 2 were undergoing fertility treatment and 2 were noncompliant with the treatment after regression was diagnosed. All except 1 proceeded to hysterectomy and histopathology was concordant at surgery. One patient with CAH recurrence was treated with a LNG-IUS and experienced regression after 6 months of treatment.
Of the 4 postmenopausal women who initially responded to treatment, 2 developed endometrial cancer and this occurred at 33 and 43 months, respectively, postinitial diagnosis. One of these women had ceased therapy for 6 months prior and the other continued with LNG-IUS. Both of these women had stage 1 adenocarcinoma that was completely resected at total abdominal hysterectomy bilateral salpingo-oophorectomy.
Only 12 of the 30 women who chose conservative management in order to preserve fertility wanted to conceive immediately. Of the 12 women, 4 successfully conceived, 2 spontaneously, and 2 with assisted reproduction. These pregnancies were carried to term without complication.
Discussion
This is one of the first studies to report differences in response to conservative treatment with progestogens for CAH comparing pre- and postmenopausal women. 17 This is a clinically important distinction since the main indication for conservative therapy, fertility preservation, should only be considered in premenopausal women with CAH. Our findings suggest that disease physiology differs according to menopausal status and that their response to progestogens may differ.
We observed that regression rates for premenopausal women with CAH are encouraging at 76% after 12 months of treatment with either a high-dose oral therapy or a LNG-IUS. Importantly, of those that did not respond, none progressed to endometrial cancer. In contrast, only 21% of postmenopausal women treated conservatively experienced endometrial regression. Alarmingly, 21% of the postmenopausal women at first follow-up hysteroscopy and endometrial biopsy had progression to endometrial cancer. These results are in agreement with the Gallos et al meta-analysis 15 that showed regression rates of 85.6% for fertility-sparing conservative treatment with progestogens for CAH. Importantly, our data highlight the significant risk of disease progression in postmenopausal women with CAH managed conservatively.
Close follow-up and continuing treatment are essential for conservative therapy. We observed that 16% (n = 5 of 32) of premenopausal women will relapse or progress over a median follow-up of 24 months (interquartile range 16-50, range 10-120 months). Half (50% n = 2 of 4) of the postmenopausal cohort that initially responded developed endometrial cancer 33 and 43 months later. Similarly, high rates of relapse have also been reported in the Gallos cohort study at 35%. This is likely due to the ongoing estrogen stimulation often resulting from obesity. 18
Pregnancy rates for those who attempted to conceive was 33% (n = 4 of 12) and all resulted in live births at term, which is similar to other reported studies at 26%. 15 This suggests that although pregnancy can be achieved, fecundity rates are reduced compared with the general population. Women considering conservative therapy to achieve pregnancy should be advised that only around one-third will successfully achieve pregnancy even with reproductive assistance.
The Royal Women’s Hospital is a large tertiary referral center. As a result, we have studied one of the largest cohorts from a single center with conservative management of CAH. We have been able to further define the risks involved in 2 important and distinctly different patient cohorts. As management practices for conservative therapy of CAH are largely consistent and unchanged over the time period studied, the results are relevant to the current management of CAH.
Although we were careful to account for potential biases, we recognize some limitations to our study. We were not able to make direct comparisons against drug efficiency and despite ensuring that scripts had been written, we could not further assess compliance. Furthermore, the number of observations with regard to future fertility was somewhat modest meaning some caution is required in interpreting this data. We have tried to account for potential bias and confounders; however, due to the nature of observational studies this is difficult. Despite the drawbacks, the cohort remains one of the largest studied with this condition at this time.
We believe that oral MPA or a LNG-IUS is appropriate hormonal treatment for informed premenopausal women with CAH having a strong desire to preserve their fertility. However, they should be advised that the risk of concurrent endometrial cancer with CAH is approximately 20% and this cannot be diagnosed without hysterectomy. They should also accept the need for follow-up at 6-month intervals with invasive testing by blind or targeted endometrial biopsy. If regression has occurred and fertility is an immediate priority, they should be referred to a fertility center for advice. If they are obese, they should be counseled about the risks that this poses to their pregnancy. Attempted pregnancy will require cessation of progestogen therapy and this may increase the risk of relapse or recurrence. They will require further treatment after they have had fertility treatment or a pregnancy and hysterectomy should be reconsidered. Hysterectomy is appropriate for those who have completed their families. Conservative management of CAH in postmenopausal women is not effective and these women should be advised to undergo hysterectomy.
Footnotes
Acknowledgment
We thank Professor Tong for intellectual input.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: